ankara, february 2007. clinical management of invasive fungal infections: an evidence-based approach
TRANSCRIPT
ANKARA, FEBRUARY 2007
ANKARA, FEBRUARY 2007

Clinical Management of Invasive Fungal Infections:
An Evidence-Based Approach
Clinical Management of Invasive Fungal Infections:
An Evidence-Based Approach

According to Odds
INCREASE IN FUNGAL INFECTIONSINCREASE IN FUNGAL INFECTIONS
• less mortality from other causesless mortality from other causes
-underlying disease-underlying disease
-better antibacterial therapy-better antibacterial therapy• higher agehigher age• better diagnostic toolsbetter diagnostic tools• more complex interventionsmore complex interventions

MORTALITY DUE TO INVASIVE MYCOSESMORTALITY DUE TO INVASIVE MYCOSESMcNeil et al. Clin Infect Dis 2001;33:641-7McNeil et al. Clin Infect Dis 2001;33:641-7
MORTALITY DUE TO INVASIVE MYCOSESMORTALITY DUE TO INVASIVE MYCOSESMcNeil et al. Clin Infect Dis 2001;33:641-7McNeil et al. Clin Infect Dis 2001;33:641-7
00
0,20,2
0,40,4
0,60,6
1980
1980
1981
1981
1982
1982
1983
1983
1984
1984
1985
1985
1986
1986
1987
1987
1988
1988
1989
1989
1990
1990
1991
1991
1992
1992
1993
1993
1994
1994
1995
1995
1996
1996
1997
1997
Rate
per
100,0
00 p
op
ula
tion
Rate
per
100,0
00 p
op
ula
tion
United States, 1980-1997United States, 1980-1997
Mycoses other than Candida albicans
19991999 20002000 20012001 20022002 20032003
00
0,50,5
11
1,51,5
22
2,52,5
33
3,53,5
Incid
en
ce (
%)
Incid
en
ce (
%)
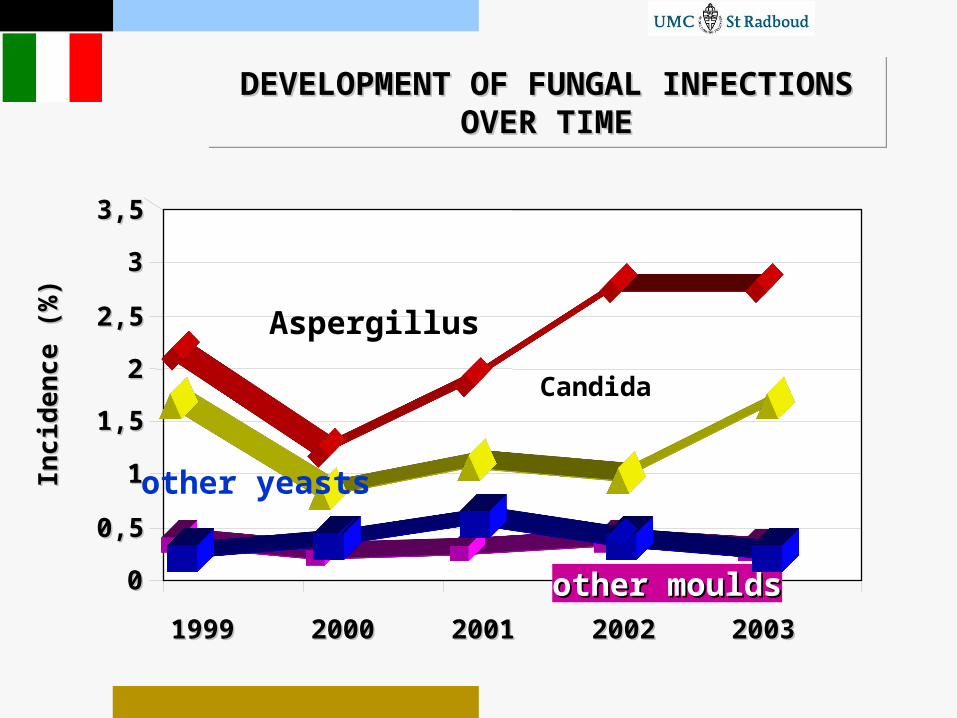
DEVELOPMENT OF FUNGAL INFECTIONS DEVELOPMENT OF FUNGAL INFECTIONS OVER TIMEOVER TIME
DEVELOPMENT OF FUNGAL INFECTIONS DEVELOPMENT OF FUNGAL INFECTIONS OVER TIMEOVER TIME
other mouldsother moulds
Aspergillus
Candida
other yeasts
nu
mb
er
of
cases
Asper
gillu
s
Zygo
myc
etes
Fusa
rium
Cand
ida
Cryp
toco
ccus
Tricho
spor
on0
100200
300400
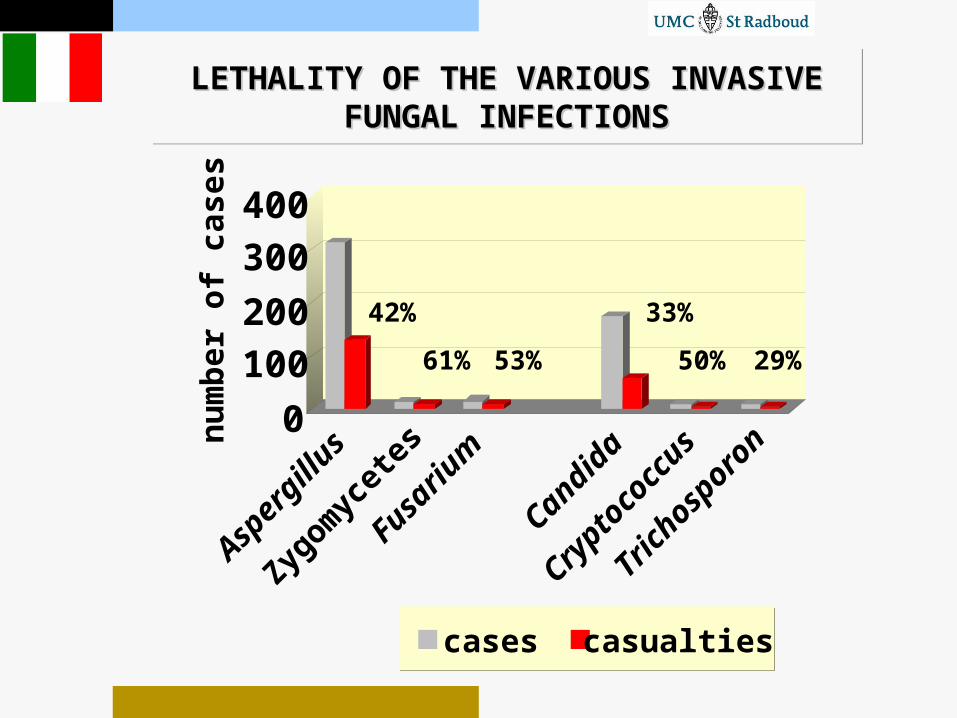
LETHALITY OF THE VARIOUS INVASIVE LETHALITY OF THE VARIOUS INVASIVE FUNGAL INFECTIONSFUNGAL INFECTIONS
LETHALITY OF THE VARIOUS INVASIVE LETHALITY OF THE VARIOUS INVASIVE FUNGAL INFECTIONSFUNGAL INFECTIONS
cases casualties
42%
61% 53%
33%
50% 29%

BASIC RISK FACTORS FOR FUNGAL INFECTIONSBASIC RISK FACTORS FOR FUNGAL INFECTIONS
immuno-
suppressionepidemiologic
exposure
technical /technical /anatomic anatomic factorsfactors
Adapted from RH Rubin, Boston
OPPORTUNISTS!OPPORTUNISTS!
MucosaMucosa
GranulocytesGranulocytes
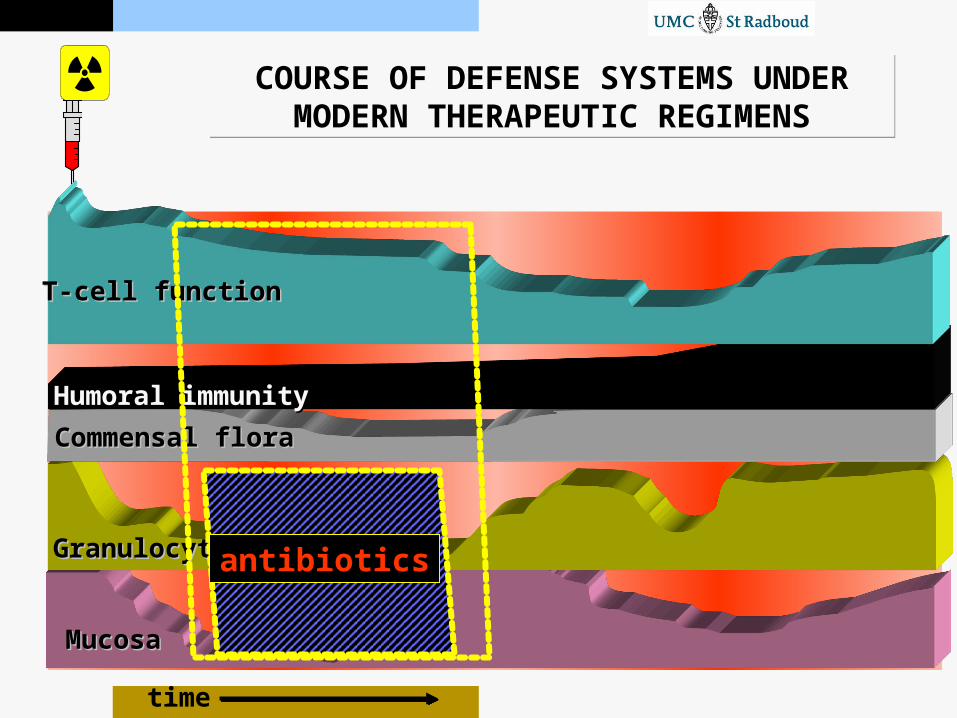
COURSE OF DEFENSE SYSTEMS UNDER MODERN THERAPEUTIC REGIMENS
COURSE OF DEFENSE SYSTEMS UNDER MODERN THERAPEUTIC REGIMENS
time
Commensal floraCommensal flora
Humoral immunityHumoral immunity
T-cell functionT-cell function
antibiotics
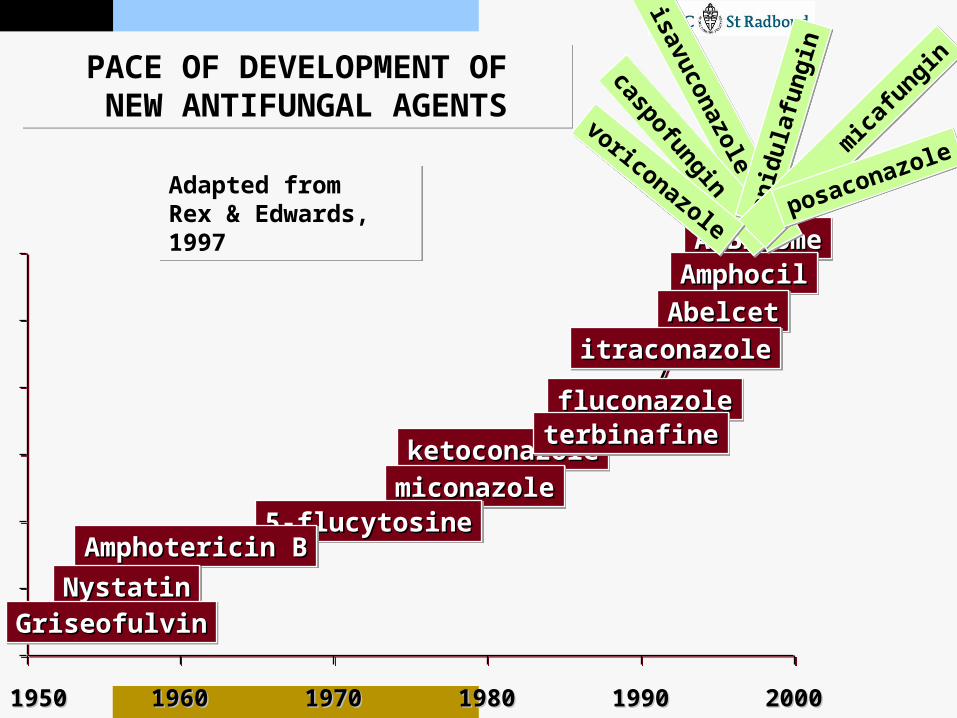
PACE OF DEVELOPMENT OF NEW ANTIFUNGAL AGENTSPACE OF DEVELOPMENT OF NEW ANTIFUNGAL AGENTS
19501950 19601960 19701970 19801980 19901990 20002000
Adapted from Rex & Edwards, 1997Adapted from Rex & Edwards, 1997
AmBisomeAmBisomeAmBisomeAmBisome
fluconazolefluconazolefluconazolefluconazole
AmphocilAmphocilAmphocilAmphocil
AbelcetAbelcetAbelcetAbelcet
itraconazoleitraconazoleitraconazoleitraconazole
ketoconazoleketoconazoleketoconazoleketoconazole
miconazolemiconazolemiconazolemiconazole
5-flucytosine5-flucytosine5-flucytosine5-flucytosine
terbinafineterbinafineterbinafineterbinafine
Amphotericin BAmphotericin BAmphotericin BAmphotericin B
NystatinNystatinNystatinNystatin
GriseofulvinGriseofulvinGriseofulvinGriseofulvin
isavuconazole
isavuconazole
caspofungin
caspofungin
anid
ulaf
ungi
n
anid
ulaf
ungi
n
mica
fungin
mica
fungin
voriconazole
voriconazole posaconazole
posaconazole

WHAT’S NEW?WHAT’S NEW?
voriconazole caspofungin
micafungin
anidulafungin
amphotericin B flucytosine fluconazole itraconazole
posaconazole
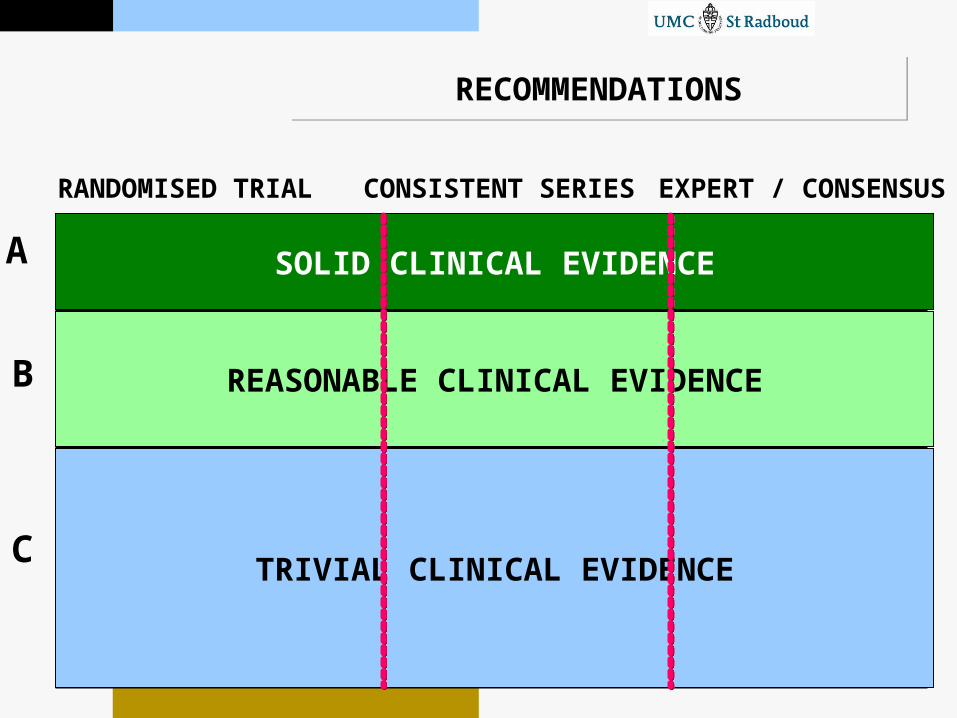
RECOMMENDATIONSRECOMMENDATIONS
A
B
C
I II IIIRANDOMISED TRIAL CONSISTENT SERIES EXPERT / CONSENSUS
SOLID CLINICAL EVIDENCE
REASONABLE CLINICAL EVIDENCE
TRIVIAL CLINICAL EVIDENCE

RECOMMENDATIONSRECOMMENDATIONS
A
B
C
I II III
lipid ampho B for primary treatment
ampho B followed by itraconazole
biological response modifiers // surgery
early start of antifungal treatment
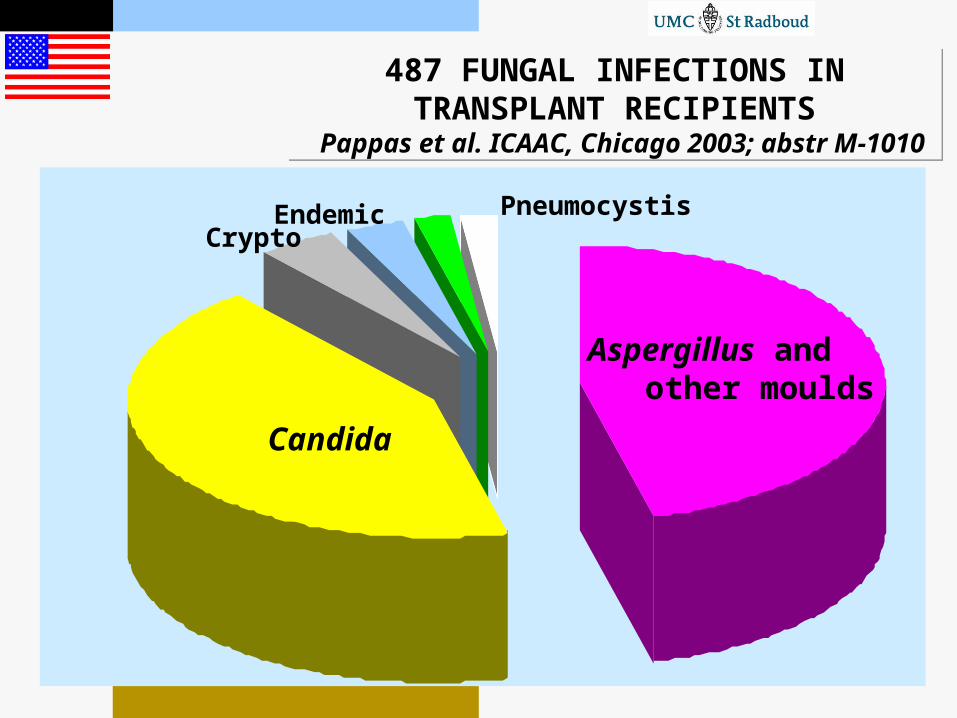
487 FUNGAL INFECTIONS IN TRANSPLANT RECIPIENTS
Pappas et al. ICAAC, Chicago 2003; abstr M-1010
487 FUNGAL INFECTIONS IN TRANSPLANT RECIPIENTS
Pappas et al. ICAAC, Chicago 2003; abstr M-1010
Candida
Aspergillus and other moulds
CryptoEndemic Pneumocystis

FUNGAL INFECTIONS IN TRANSPLANT RECIPIENTS
Pappas et al. ICAAC, Chicago 2003; abstr M-1010
FUNGAL INFECTIONS IN TRANSPLANT RECIPIENTS
Pappas et al. ICAAC, Chicago 2003; abstr M-1010
Candida species
POPULATION WITH INVASIVE CANDIDIASISPOPULATION WITH INVASIVE CANDIDIASIS
Invasive candidasis Diagnosed while aliveeligible for clinical trial

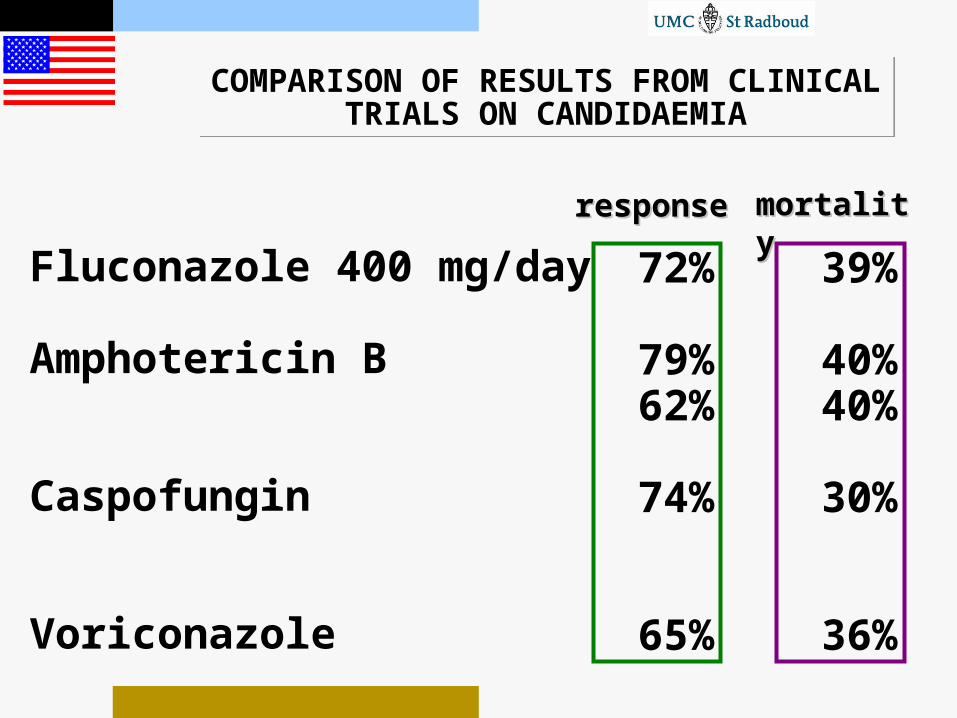
COMPARISON OF RESULTS FROM CLINICAL TRIALS ON CANDIDAEMIA
COMPARISON OF RESULTS FROM CLINICAL TRIALS ON CANDIDAEMIA
Fluconazole 400 mg/day
Amphotericin B
CaspofunginMicafunginAnidulafunginVoriconazole
72%
79%62%
74%74%76%65%
39%
40%40%
30%
23%36%
responsresponsee
mortalitmortalityy

MICAFUNGIN versus AMBISOME IN CHILDREN WITH INVASIVE CANDIDOSIS
Arrieta et al. ICAAC, San Francisco 2006; Abstract M-1308b
MICAFUNGIN versus AMBISOME IN CHILDREN WITH INVASIVE CANDIDOSIS
Arrieta et al. ICAAC, San Francisco 2006; Abstract M-1308b
Double-blind comparison, n = 98
Rate of Favorabl
e Respons
e
2mg/kg/d
(n=48)
AmBisome3 mg/day(n=50)
micafungin
7373%% 7766%%
0
20
40
60
80
100premature
7070%% 6767%%
premature
COMPARISON OF RESULTS FROM CLINICAL TRIALS ON CANDIDAEMIA
COMPARISON OF RESULTS FROM CLINICAL TRIALS ON CANDIDAEMIA
Fluconazole 400 mg/day
Amphotericin B
CaspofunginMicafunginAnidulafunginVoriconazole
72%
79%62%
74%74%76%65%
39%
40%40%
30%
23%36%
responsresponsee
mortalitmortalityy

COMPARISON OF RESULTS FROM CLINICAL TRIALS ON CANDIDAEMIA
COMPARISON OF RESULTS FROM CLINICAL TRIALS ON CANDIDAEMIA
Fluconazole 400 mg/day
Amphotericin B
CaspofunginMicafunginAnidulafunginVoriconazole
72%
79%62%
74%74%76%65%
39%
40%40%
30%
23%36%
responsresponsee
mortalitmortalityy
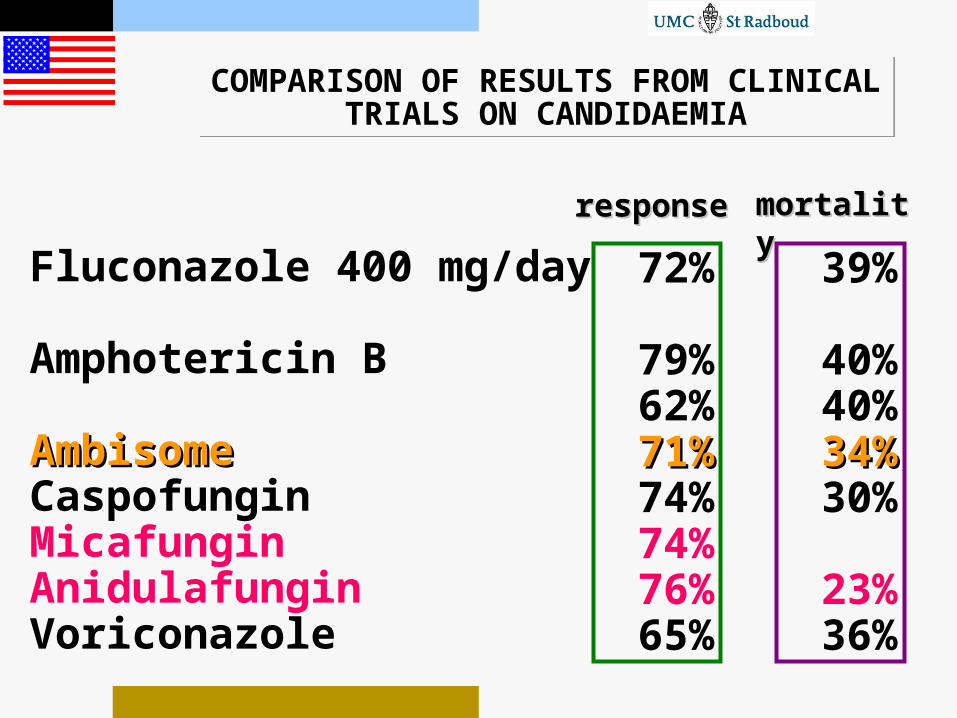
COMPARISON OF RESULTS FROM CLINICAL TRIALS ON CANDIDAEMIA
COMPARISON OF RESULTS FROM CLINICAL TRIALS ON CANDIDAEMIA
Fluconazole 400 mg/day
Amphotericin B
AmbisomeAmbisomeCaspofunginMicafunginAnidulafunginVoriconazole
72%
79%62%71%71%74%74%76%65%
39%
40%40%3434%%30%
23%36%
responsresponsee
mortalitmortalityy

RELATION INITIATION FLUCONAZOLE THERAPY AND OUTCOME OF CANDIDAEMIA
Garey et al. Clin Infect Dis 2006; 43:25-31
RELATION INITIATION FLUCONAZOLE THERAPY AND OUTCOME OF CANDIDAEMIA
Garey et al. Clin Infect Dis 2006; 43:25-31
230 cases of candidaemia
start fluconazoleday 0 day 2 day 3 day 4

RELATION INITIATION FLUCONAZOLE THERAPY AND OUTCOME OF CANDIDAEMIA
Garey et al. Clin Infect Dis 2006; 43:25-31
RELATION INITIATION FLUCONAZOLE THERAPY AND OUTCOME OF CANDIDAEMIA
Garey et al. Clin Infect Dis 2006; 43:25-31
230 cases of candidaemia
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
mortality
start fluconazoleday 0 day 2 day 3 day 4
A
B
C
I II III
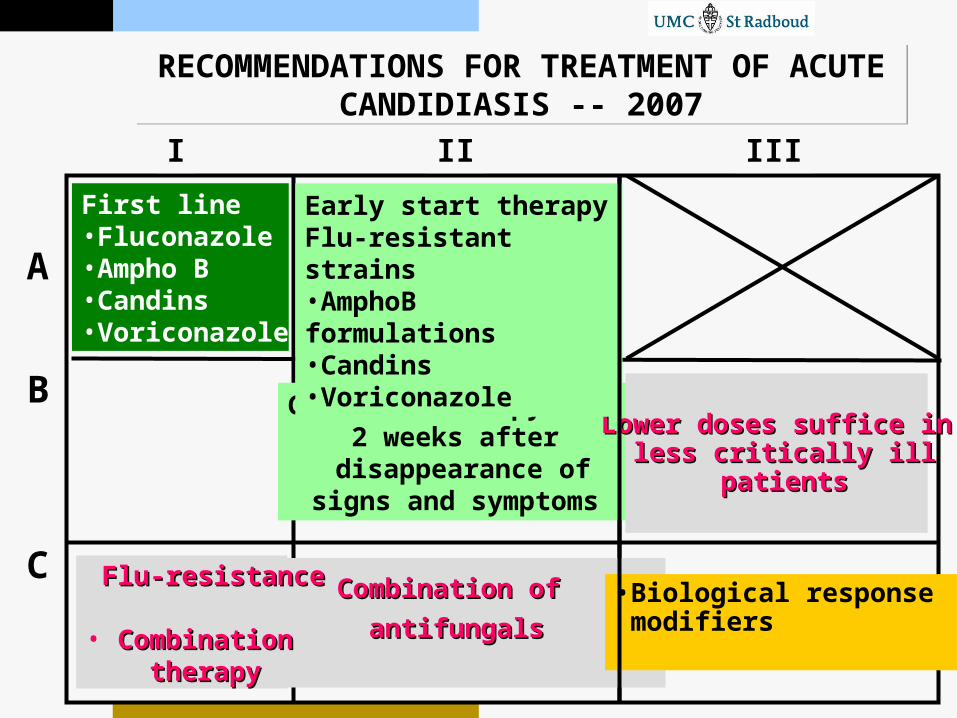
Continue therapy for 2 weeks after
disappearance of signs and symptoms
Lower doses suffice inLower doses suffice in less critically illless critically ill
patientspatients
First line•Fluconazole•Ampho B•Candins•Voriconazole
Combination of Combination of
antifungals antifungals •Biological response modifiers
FFlu-resistancelu-resistance
• CCombinationombination therapytherapy
RECOMMENDATIONS FOR TREATMENT OF ACUTE CANDIDIASIS -- 2007
RECOMMENDATIONS FOR TREATMENT OF ACUTE CANDIDIASIS -- 2007
Early start therapyFlu-resistant strains •AmphoB formulations•Candins•Voriconazole
FROM TREATMENT OF CHOICE TO CHOICES
OF TREATMENT
FROM TREATMENT OF CHOICE TO CHOICES
OF TREATMENT

FROM TREATMENT OF CHOICE TO CHOICES
OF TREATMENT
FROM TREATMENT OF CHOICE TO CHOICES
OF TREATMENT
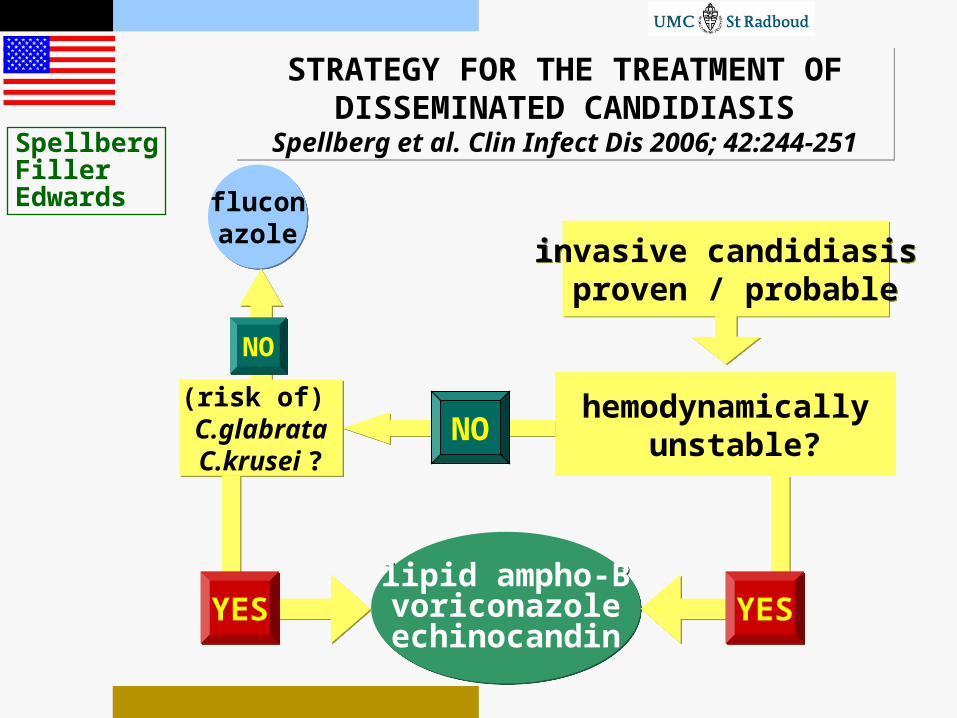
STRATEGY FOR THE TREATMENT OF DISSEMINATED CANDIDIASIS
Spellberg et al. Clin Infect Dis 2006; 42:244-251
STRATEGY FOR THE TREATMENT OF DISSEMINATED CANDIDIASIS
Spellberg et al. Clin Infect Dis 2006; 42:244-251
invasive candidiasis proven / probable
invasive candidiasis proven / probable
NO
fluconazolefluconazole
lipid ampho-Bvoriconazoleechinocandin
lipid ampho-Bvoriconazoleechinocandin
SpellbergFillerEdwards
(risk of) C.glabrataC.krusei ?
(risk of) C.glabrataC.krusei ?
NONO
hemodynamically unstable?
YESYES YESYES

FUNGAL INFECTIONS IN TRANSPLANT RECIPIENTS
Pappas et al. ICAAC, Chicago 2003; abstr M-1010
FUNGAL INFECTIONS IN TRANSPLANT RECIPIENTS
Pappas et al. ICAAC, Chicago 2003; abstr M-1010
Aspergillus species

QUESTIONS REGARDING INVASIVE ASPERGILLOSIS
QUESTIONS REGARDING INVASIVE ASPERGILLOSIS
Why is there an increase?When will it occur?Where will it strike?
When should we treat?What is the best therapy?
Treatment
Treatment
checklistchecklist
azolesazoles
polyenespolyenes
lipid formulations
lipid formulations
candinscandins
combinations
combinations
diagnostics
a plan
I FD
Treatment
Treatment
checklistchecklist
azolesazoles
polyenespolyenes
lipid formulations
lipid formulations
candinscandins
combinations
combinations
diagnostics
diagnostics
a plana plan
I FD
STRATEGY vs DRUG SELECTIONSTRATEGY vs DRUG SELECTION
When?
What?
Treatment
Treatment
checklistchecklist
azolesazoles
polyenespolyenes
lipid formulations
lipid formulations
candinscandins
combinations
combinations
diagnostics
diagnostics
a plana plan
I FD
STRATEGY vs DRUG-EFFICACYSTRATEGY vs DRUG-EFFICACY
When?
What?
Treatment
Treatment
checklistchecklist
azolesazoles
polyenespolyenes
lipid formulations
lipid formulations
candinscandins
combinations
combinations
diagnostics
diagnostics
a plana plan
I FD
STRATEGY vs DRUG-EFFICACYSTRATEGY vs DRUG-EFFICACY
When?
RELATION OUTCOME AND STATE OF FUNGAL INFECTION
RELATION OUTCOME AND STATE OF FUNGAL INFECTION
evolution of the infectionevolution of the infection evolution of the infectionevolution of the infection
odds to control the infectionodds to control the infection odds to control the infectionodds to control the infection
timetime timetime

IMPORTANCE OF EARLY TREATMENT OF INVASIVE ASPERGILLOSIS
Patterson et al. Medicine 2000
IMPORTANCE OF EARLY TREATMENT OF INVASIVE ASPERGILLOSIS
Patterson et al. Medicine 2000
Type of infection
Pulmonary only
Disseminated
Survival
40% (n=330)
18% (n=144)

RECOMMENDATIONS IDSA 2000Stevens et al. Clin Infect Dis 2000; 30:696-709RECOMMENDATIONS IDSA 2000Stevens et al. Clin Infect Dis 2000; 30:696-709
A
B
C
I II III
Early start of antifungal treatment

PROBABILITY OF DEVELOPING PULMONARY ASPERGILLUS
Gerson et al. Ann Intern Med 1984
PROBABILITY OF DEVELOPING PULMONARY ASPERGILLUS
Gerson et al. Ann Intern Med 1984
0 0
2020
4040
6060
8080
100100
PER
CEN
TA
GE
PER
CEN
TA
GE
INFEC
TED
INFEC
TED
DAYS WITH NEUTROPENIADAYS WITH NEUTROPENIA
0 10 20 30 40 50 60 70 80 90 100
Empirical therapy incidence aspergillosis 4-6%
DIAGNOSTIC TOOLS ANNO 2007DIAGNOSTIC TOOLS ANNO 2007
Sandwich-ELISA galactomannanHigh-resolution CT-scanUltrasoundBronchoalveolar lavagesBiopsy techniques
Glucan-testPCRPET-scanning
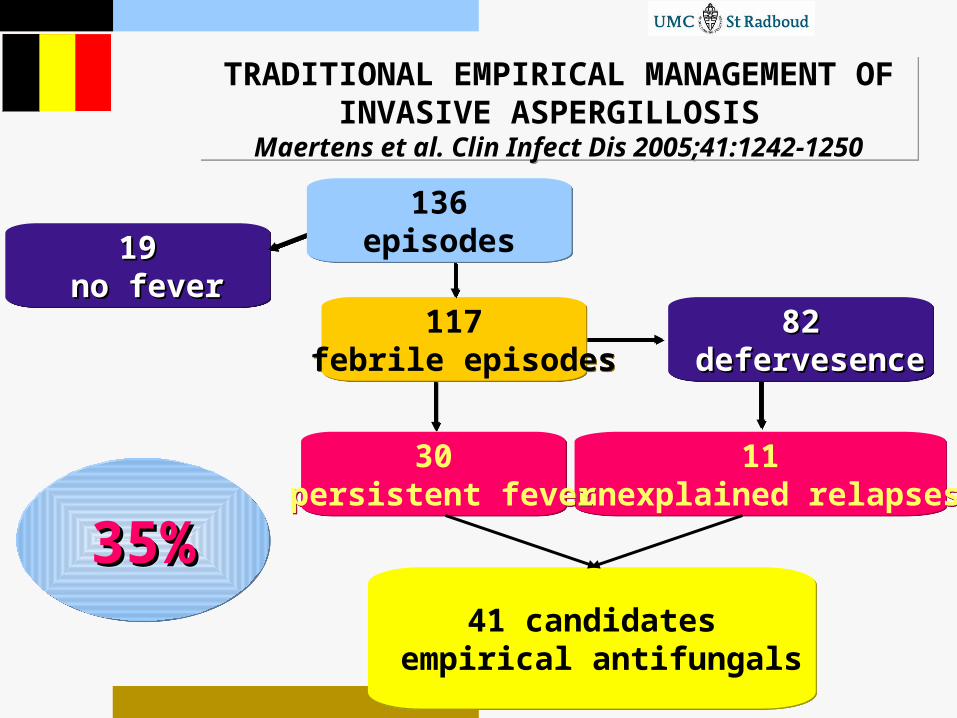
TRADITIONAL EMPIRICAL MANAGEMENT OF INVASIVE ASPERGILLOSIS
Maertens et al. Clin Infect Dis 2005;41:1242-1250
TRADITIONAL EMPIRICAL MANAGEMENT OF INVASIVE ASPERGILLOSIS
Maertens et al. Clin Infect Dis 2005;41:1242-1250
11 unexplained relapses
11 unexplained relapses
30 persistent fever
30 persistent fever
8282 defervesencedefervesence
8282 defervesencedefervesence
41 candidates empirical antifungals
41 candidates empirical antifungals
35%35%35%35%
1919 no feverno fever
1919 no feverno fever
117 febrile episodes
117 febrile episodes
136episodes
136episodes
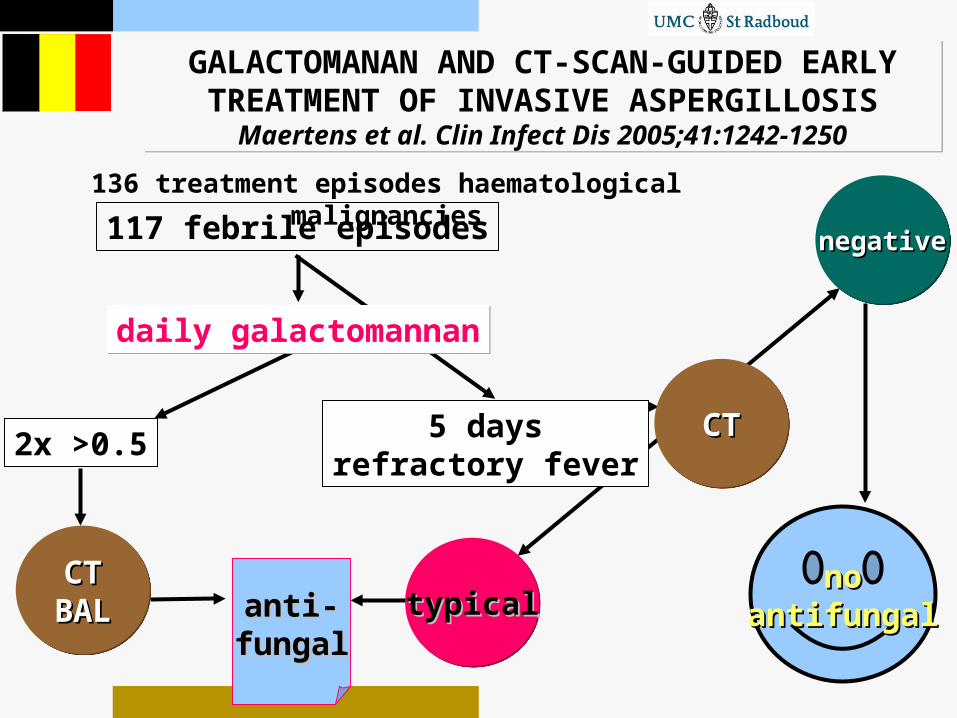
GALACTOMANAN AND CT-SCAN-GUIDED EARLY TREATMENT OF INVASIVE ASPERGILLOSIS
Maertens et al. Clin Infect Dis 2005;41:1242-1250
GALACTOMANAN AND CT-SCAN-GUIDED EARLY TREATMENT OF INVASIVE ASPERGILLOSIS
Maertens et al. Clin Infect Dis 2005;41:1242-1250
117 febrile episodes
nonoantifungalantifungalanti-anti-
fungalfungal
2x >0.5
CTCTBALBALCTCT
BALBAL
136 treatment episodes haematological malignancies
typicaltypicaltypicaltypical
negativenegativenegativenegative
CTCTCTCT5 daysrefractory fever
daily galactomannandaily galactomannan

PRE-EMPTIVE MANAGEMENT OF INVASIVE ASPERGILLOSIS
Maertens et al. Clin Infect Dis 2005;41:1242-1250
PRE-EMPTIVE MANAGEMENT OF INVASIVE ASPERGILLOSIS
Maertens et al. Clin Infect Dis 2005;41:1242-1250
136episodes
136episodes
10 seropositive
10 seropositive
9 cases suspicious CT
9 cases suspicious CT
8282 defervesencedefervesence
8282 defervesencedefervesence
19 cases for pre-emptive antifungals
19 cases for pre-emptive antifungals
16%16%16%16%
1919 no feverno fever
1919 no feverno fever
117 febrile episodes
117 febrile episodes
++

PRE-EMPTIVE MANAGEMENT OF INVASIVE ASPERGILLOSIS: MORTALITY
Maertens et al. Clin Infect Dis 2005;41:1242-1250
PRE-EMPTIVE MANAGEMENT OF INVASIVE ASPERGILLOSIS: MORTALITY
Maertens et al. Clin Infect Dis 2005;41:1242-1250
88patients
88patients
fungalfungalmortalitymortality
8%8%
fungalfungalmortalitymortality
8%8%
Fungal mortality
Walsh I 7%Walsh II 8%Walsh III 8%Boogaerts 11%

ESTIMATING TIME FOR INTERVENTIONESTIMATING TIME FOR INTERVENTION
AspergillusAspergillus
day 1 5 7 12 // 28 > 42day 1 5 7 12 // 28 > 42
infiltrateinfiltrateinfiltrateinfiltrateantigenantigenantigenantigen
Persisting fever +
• very high risk or• a suggestive symptom or• a suspected sign or• any positive test

HOW TO PROCEED?HOW TO PROCEED?

Treatment
Treatment
checklistchecklist
azolesazoles
polyenespolyenes
lipid formulations
lipid formulations
candinscandins
combinations
combinations
diagnostics
diagnostics
a plana plan
I FD
STRATEGY vs DRUG-EFFICACYSTRATEGY vs DRUG-EFFICACY
When?
What?

Treatment
Treatment
checklistchecklist
azolesazoles
polyenespolyenes
lipid formulations
lipid formulations
candinscandins
combinations
combinations
I FD
STRATEGY vs DRUG-EFFICACYSTRATEGY vs DRUG-EFFICACY
What?
WHAT IS THE BEST ANTIFUNGAL DRUG?WHAT IS THE BEST ANTIFUNGAL DRUG?
For prophylaxis?
For empirical purposes?
For treatment of established disease?

PROPHYLAXIS EMPIRICAL (PRE-EMPTIVE) THERAPY
PROPHYLAXIS EMPIRICAL (PRE-EMPTIVE) THERAPY
invasivefungal
infectionNOT
PRESENT
invasivefungal
infectionNOT
PRESENT
invasivefungal
infectionNOT
EXCLUDED
invasivefungal
infectionNOT
EXCLUDED
invasivefungal
infectionINCIPIENT
invasivefungal
infectionINCIPIENT

INTERRELATIONSINTERRELATIONS
BUG
BUG
efficacy DRUG
DRUG
PROBABLE & PROVEN FUNGAL DISEASE
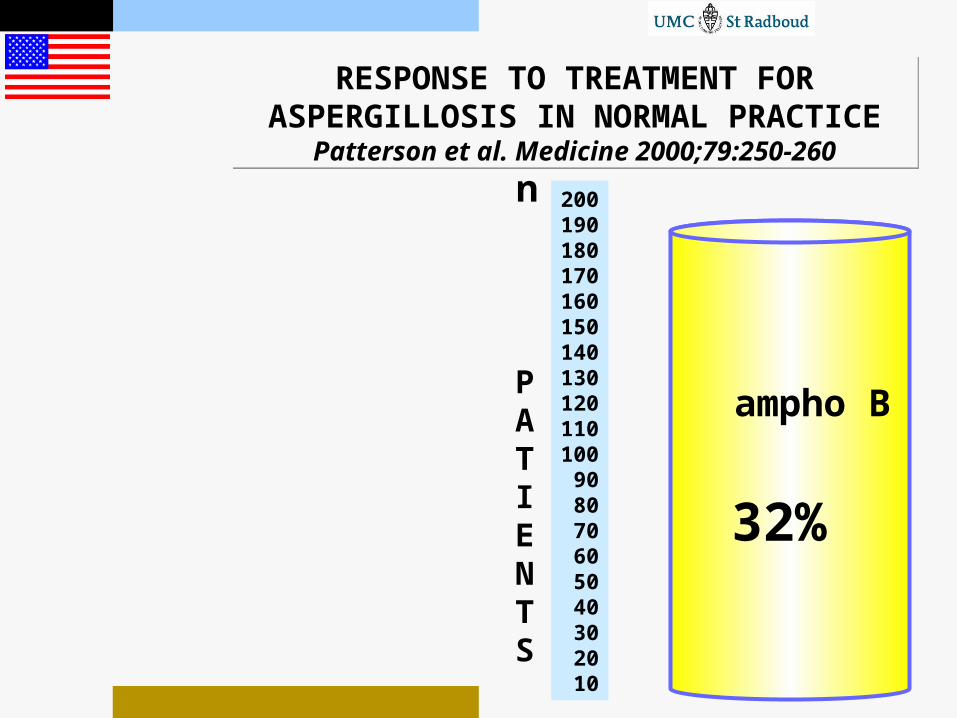
RESPONSE TO TREATMENT FOR ASPERGILLOSIS IN NORMAL PRACTICE
Patterson et al. Medicine 2000;79:250-260
RESPONSE TO TREATMENT FOR ASPERGILLOSIS IN NORMAL PRACTICE
Patterson et al. Medicine 2000;79:250-260
200190180170160150140130120110100
908070605040302010
ampho B
32%
PATIENTS
n

RECOMMENDATIONS IDSA 2000Stevens et al. Clin Infect Dis 2000; 30:696-709RECOMMENDATIONS IDSA 2000Stevens et al. Clin Infect Dis 2000; 30:696-709
A
B
C
I II III
Lipid ampho B in compromised kidneys
Ampho B and itraconazole for primary treatment
Lipid ampho B for primary treatment
Ampho B followed by itraconazole
Biological response modifiers // surgery
Early start of antifungal treatment
REFERENCE POPULATIONREFERENCE POPULATION
Invasive aspergillosis Diagnosed while alive ineligible ineligible
REPRESENTATIVE !REPRESENTATIVE !??
4% in trials !!
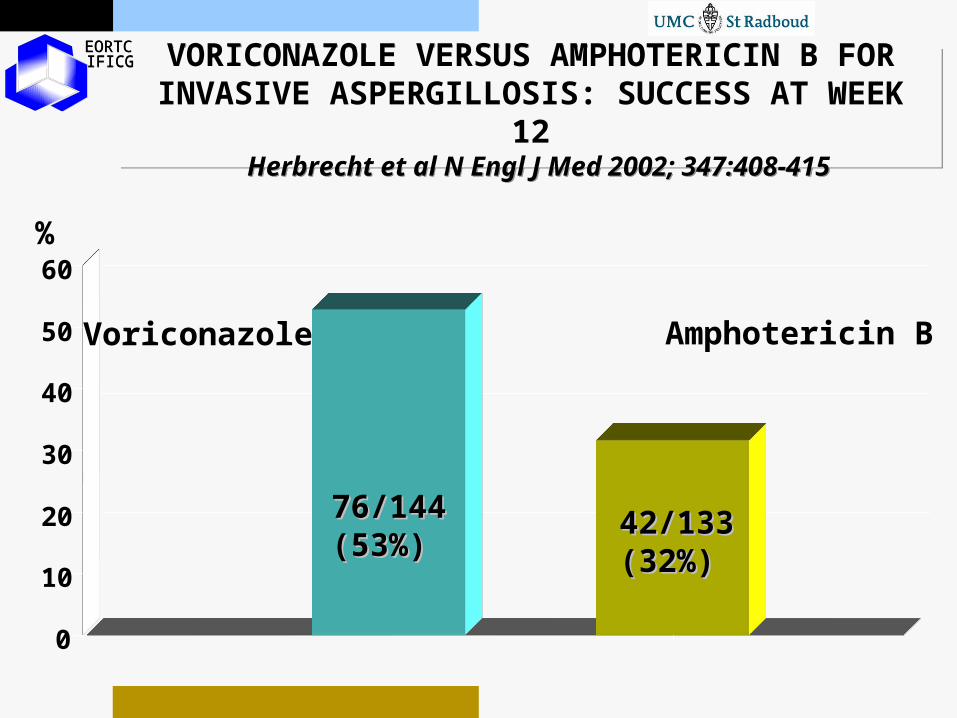
VORICONAZOLE VERSUS AMPHOTERICIN B FORINVASIVE ASPERGILLOSIS: SUCCESS AT WEEK 12
Herbrecht et al N Engl J Med 2002; 347:408-415
VORICONAZOLE VERSUS AMPHOTERICIN B FORINVASIVE ASPERGILLOSIS: SUCCESS AT WEEK 12
Herbrecht et al N Engl J Med 2002; 347:408-415
EORTC EORTC IFICGIFICG
0
10
20
30
40
50
60
Voriconazole Amphotericin B
76/14476/144(53%)(53%)
42/13342/133(32%)(32%)
%
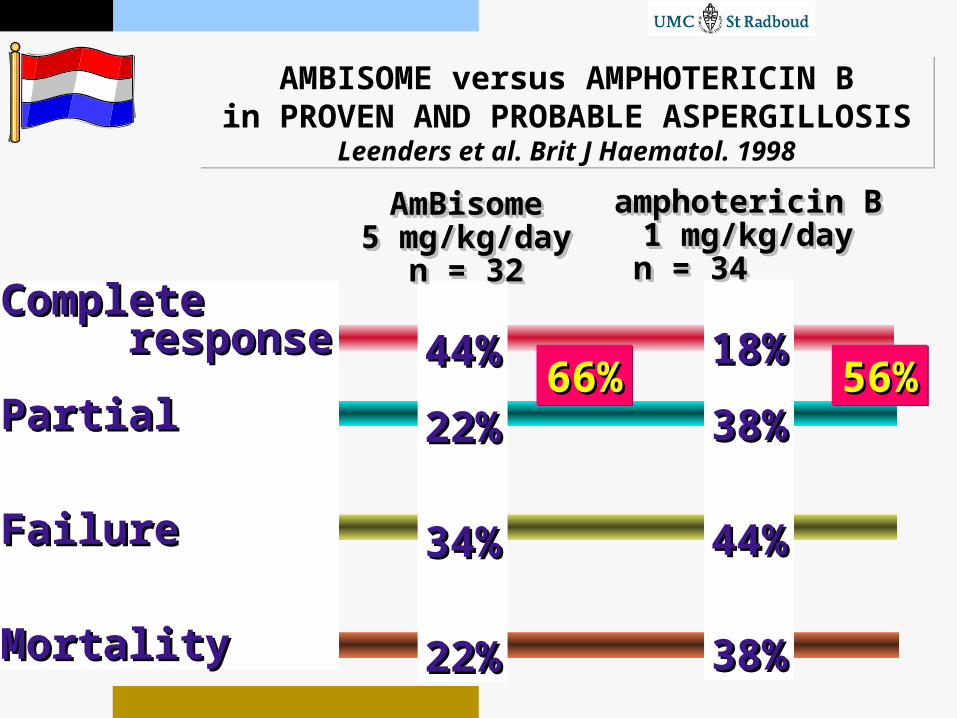
AMBISOME versus AMPHOTERICIN Bin PROVEN AND PROBABLE ASPERGILLOSIS
Leenders et al. Brit J Haematol. 1998
AMBISOME versus AMPHOTERICIN Bin PROVEN AND PROBABLE ASPERGILLOSIS
Leenders et al. Brit J Haematol. 1998
CompleteComplete responseresponse
PartialPartial
FailureFailure
MortalityMortality
44%44%
22%22%
34%34%
22%22%
18%18%
38%38%
44%44%
38%38%
66%66%66%66% 56%56%56%56%
AmBisomeAmBisome5 mg/kg/day5 mg/kg/day
n = 32n = 32
AmBisomeAmBisome5 mg/kg/day5 mg/kg/day
n = 32n = 32
amphotericin Bamphotericin B1 mg/kg/day1 mg/kg/dayn = 34 n = 34
amphotericin Bamphotericin B1 mg/kg/day1 mg/kg/dayn = 34 n = 34

HIGH VERSUS STANDARD DOSE AMBISOME FOR INVASIVE MOULD INFECTIONS Cornely et al. Blood 2005; 106:900a, Abstract 3222
HIGH VERSUS STANDARD DOSE AMBISOME FOR INVASIVE MOULD INFECTIONS Cornely et al. Blood 2005; 106:900a, Abstract 3222
16%30%30%
14%31%31%
9494 107107
46% 50%
59%59% 72%72%
End of treatmentFavorable response
Survivors 12 weeks
End of treatmentFavorable response
Survivors 12 weeks
AmBisomeAmBisome10 mg/kg x 1410 mg/kg x 14
followed byfollowed by3 mg/kg/day3 mg/kg/day
AmBisomeAmBisome10 mg/kg x 1410 mg/kg x 14
followed byfollowed by3 mg/kg/day3 mg/kg/day
AmBisomeAmBisome3 mg3 mg//kgkg//dayday
AmBisomeAmBisome3 mg3 mg//kgkg//dayday
201proven & probable
Invasive mould infections
nephrotoxicity
hypokalaemia

FIRST-LINE THERAPY WITH CASPOFUNGIN FOR PULMONARY ASPERGILLOSIS Candoni et al. Eur J Haematol 2005; 75:227-233
FIRST-LINE THERAPY WITH CASPOFUNGIN FOR PULMONARY ASPERGILLOSIS Candoni et al. Eur J Haematol 2005; 75:227-233
7 proven / 25 probable cases
31 neutropenic at start
n=32
overall
18 (
56%
) f
avora
ble
resp
on
ses
G-CSF +caspofungin
70 50 mg/d
G-CSF +caspofungin
70 50 mg/d
hem
ato
log
ical
malig
nan
cie
s
ASSESSMENT OF EFFICACYASSESSMENT OF EFFICACY
BUG
BUG
efficacy DRUG
DRUG
PROBABLE & PROVEN FUNGAL DISEASE
patients failing antifungal therapy
untreatedpatients

treatment refractory
intolerance
toxicity
PANDORRA’S BOX OF SALVAGE CASESPANDORRA’S BOX OF SALVAGE CASES
a single shiver hyperpyrexiahyperpyrexia
creatinine increase
renalfailure
3 days stable
life-threateningprogression
!subjective criteria!
treatment refractory
intolerance
toxicity
PANDORRA’S BOX OF SALVAGE CASESPANDORRA’S BOX OF SALVAGE CASES
treatedwith what?
how much??
treatedwith what?
how much??
evolvementunderlyingdisease??
evolvementunderlyingdisease??
co-medication?
co-medication?

SALVAGE FOR INVASIVE ASPERGILLOSIS SALVAGE FOR INVASIVE ASPERGILLOSIS
caspofungin n=146
Refractory / intolerant amphotericin B
posaconazole
n=107
ampho B lipid
complex
resp
on
se
40%
40% 40% 40%
voriconazol
e n=144

C.L.E.A.R. PROGRAM ON ABLCBETTER THAN NOTHING?
Clin Infect Dis 2005; 40:Supplement 6
C.L.E.A.R. PROGRAM ON ABLCBETTER THAN NOTHING?
Clin Infect Dis 2005; 40:Supplement 6
•Retrospective
•Collection of data on a voluntary basis
•Mix of superficial and disseminated infections
•No discrimination “proven-probable-possible”
•Own definitions for response / success
•Variations in dosing regimens
APPRECIATIONAPPRECIATION
Response rate improved from 30 to 60%!
Failure rate still 50%……

survival 3 months after diagnosis
VORICONAZOLE WITH CASPOFUNGIN AS RESCUE FOR INVASIVE ASPERGILLOSIS
Marr et al. Clin Infect Dis 2004; 39:797-802
VORICONAZOLE WITH CASPOFUNGIN AS RESCUE FOR INVASIVE ASPERGILLOSIS
Marr et al. Clin Infect Dis 2004; 39:797-802
Observational study with historical controls in 47 BMT recipients
Proven/probableProven/probable
invasive aspergillosisinvasive aspergillosis
ampho B 1 mg/kgampho B 1 mg/kg
kidney: lipid 5 mg/kgkidney: lipid 5 mg/kg
progression (time?)progression (time?)
intoleranceintolerance
nephrotoxicitynephrotoxicity
progression (time?)progression (time?)
intoleranceintolerance
nephrotoxicitynephrotoxicity
1997-20011997-2001 2001-2001-voriconazole
n=31
voriconazole+
caspofunginn=16
difference in survival
survival 3 months after diagnosis
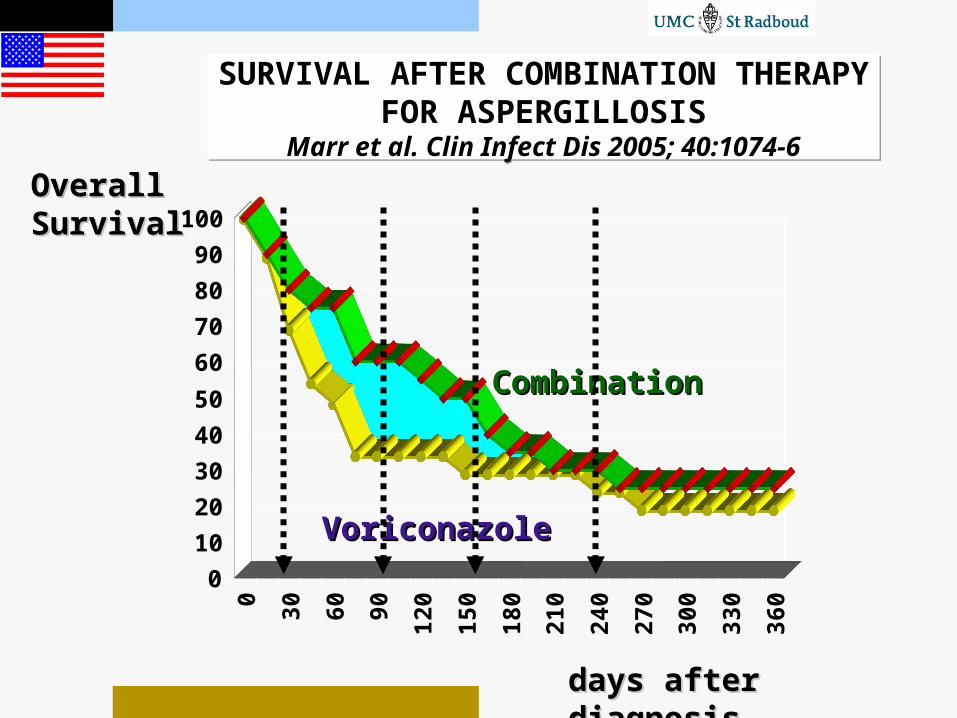
SURVIVAL AFTER COMBINATION THERAPY FOR ASPERGILLOSISMarr et al. Clin Infect Dis 2005; 40:1074-6
SURVIVAL AFTER COMBINATION THERAPY FOR ASPERGILLOSISMarr et al. Clin Infect Dis 2005; 40:1074-6
Overall Overall SurvivalSurvival
0
10
20
30
40
50
60
70
80
90
1000
30
60
90
120
150
180
210
240
270
300
330
360
days after days after diagnosisdiagnosis
CombinationCombination
VoriconazoleVoriconazole

VORICONAZOLE PLUS CASPOFUNGIN FOR ASPERGILLUS IN SOLID ORGAN TRANSPLANTS
Singh et al. Transplantation 2006; 81:320-325
VORICONAZOLE PLUS CASPOFUNGIN FOR ASPERGILLUS IN SOLID ORGAN TRANSPLANTS
Singh et al. Transplantation 2006; 81:320-325
3434 3838comparecompare
VORICONAZOLE +
CASPOFUNGIN
VORICONAZOLE +
CASPOFUNGIN
LIPID AMPHO B
HISTORICALCONTROLS
LIPID AMPHO B
HISTORICALCONTROLS
2003-20052003-2005 multicentermulticenter
mortality day 90mortality day 9026% 50%
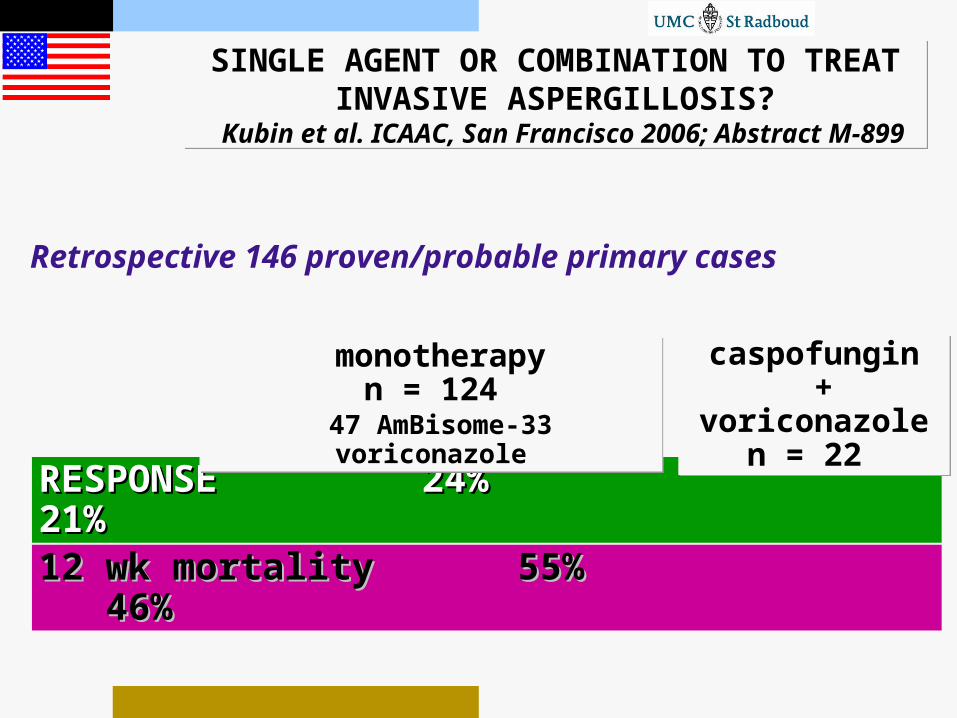
SINGLE AGENT OR COMBINATION TO TREAT INVASIVE ASPERGILLOSIS?
Kubin et al. ICAAC, San Francisco 2006; Abstract M-899
SINGLE AGENT OR COMBINATION TO TREAT INVASIVE ASPERGILLOSIS?
Kubin et al. ICAAC, San Francisco 2006; Abstract M-899
RESPONSE RESPONSE 24%24% 21% 21%
monotherapyn = 124
47 AmBisome-33 voriconazole
monotherapyn = 124
47 AmBisome-33 voriconazole
Retrospective 146 proven/probable primary cases
caspofungin +
voriconazolen = 22
caspofungin +
voriconazolen = 22
12 wk mortality 12 wk mortality 55%55% 46% 46%
HISTORICAL CONTROLSHISTORICAL CONTROLS
Unreliable due to:
•improved diagnostic tools
•over-representation of autopsy cases•changes in therapy underlying disease•changes in doctors!


QUESTIONS REGARDING INVASIVE ASPERGILLOSIS
QUESTIONS REGARDING INVASIVE ASPERGILLOSIS
Why is there an increase?When will it occur?Where will it strike?
When should we treat?What is the best therapy?Which factors dictate outcome?

QUESTIONS REGARDING INVASIVE ASPERGILLOSIS
QUESTIONS REGARDING INVASIVE ASPERGILLOSIS
Why is there an increase?When will it occur?Where will it strike?
When should we treat?What is the best therapy?Which factors dictate outcome?
ELEMENTS TO
SUCCESS
ELEMENTS TO
SUCCESS
repair repair organorgan
damagedamage
recovery recovery hosthost
defensedefense
suppression suppression of fungalof fungal growthgrowth

CORTICOSTEROIDS AND SURVIVAL OF ASPERGILLOSIS IN HSCT
Cordonnier et al. Clin Infect Dis 2006;42:955-963
CORTICOSTEROIDS AND SURVIVAL OF ASPERGILLOSIS IN HSCT
Cordonnier et al. Clin Infect Dis 2006;42:955-963
0
10
20
30
40
50
60
70
80
90
100
0 2 4 6 8 10 12 14 16 18weeks
low dose corticosteroidslow dose corticosteroids
high dosehigh dose
S
U
R
V
I
V
A
L
S
U
R
V
I
V
A
L
51 patients with aspergillosis 41 allo HSCT 10 auto
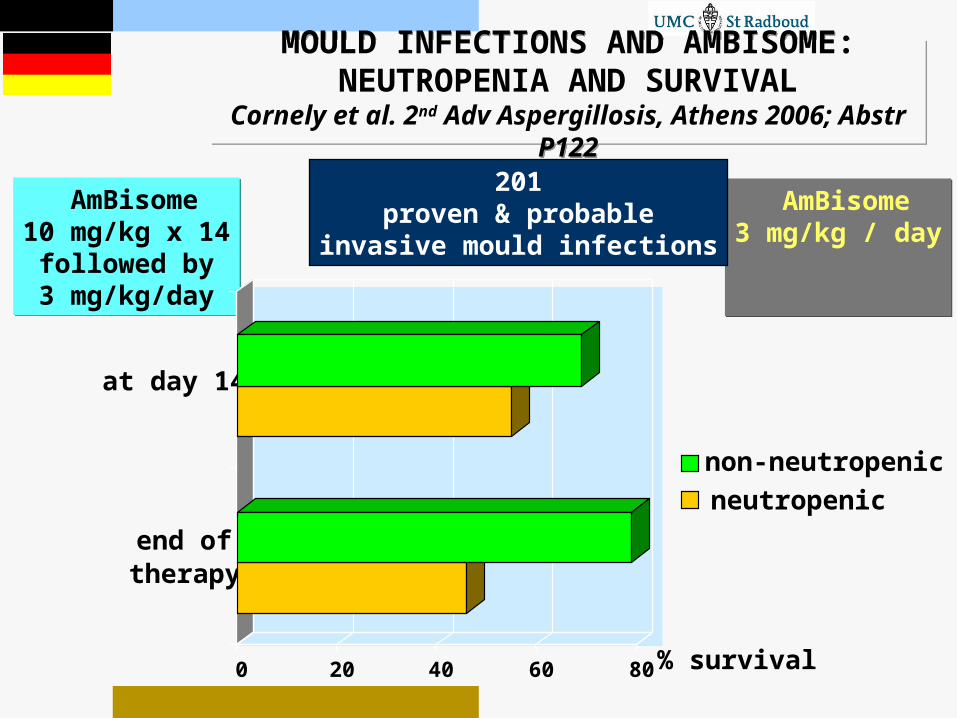
MOULD INFECTIONS AND AMBISOME: NEUTROPENIA AND SURVIVAL
Cornely et al. 2nd Adv Aspergillosis, Athens 2006; Abstr P122
MOULD INFECTIONS AND AMBISOME: NEUTROPENIA AND SURVIVAL
Cornely et al. 2nd Adv Aspergillosis, Athens 2006; Abstr P122
AmBisome10 mg/kg x 14
followed by3 mg/kg/day
AmBisome10 mg/kg x 14
followed by3 mg/kg/day
AmBisome3 mg/kg / day
AmBisome3 mg/kg / day
201proven & probable
invasive mould infections
0 20 40 60 80
end oftherapy
at day 14
neutropenicnon-neutropenic
% survival
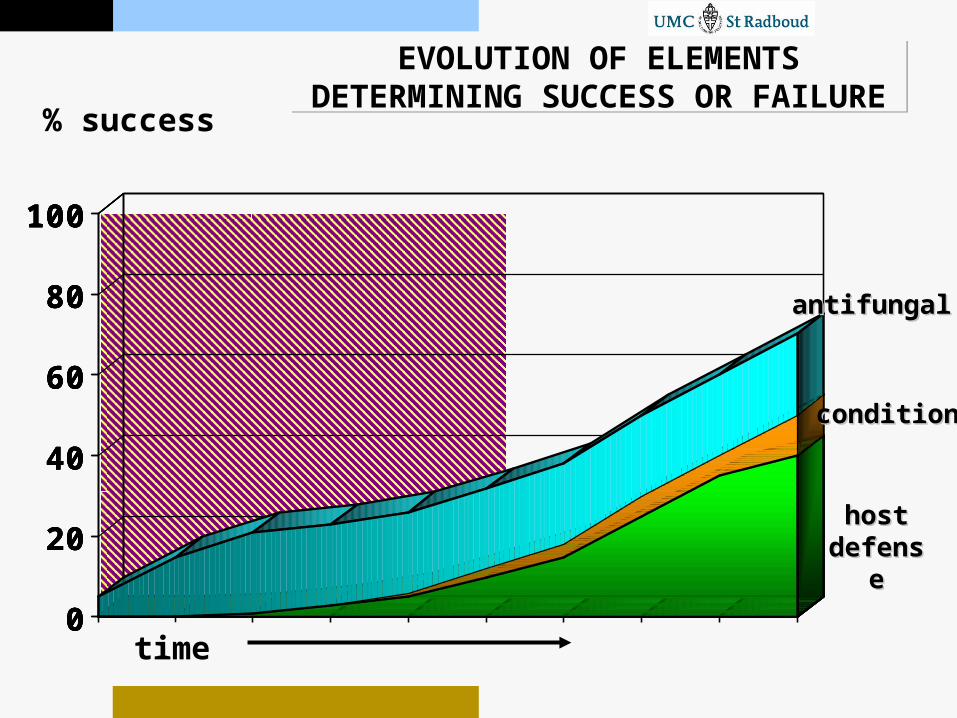
EVOLUTION OF ELEMENTS DETERMINING SUCCESS OR FAILURE
EVOLUTION OF ELEMENTS DETERMINING SUCCESS OR FAILURE
0
20
40
60
80
100
1 2 3 4 5 6 7 8 9 10
% success
0
20
40
60
80
100
1 2 3 4 5 6 7 8 9 100
20
40
60
80
100
1 2 3 4 5 6 7 8 9 100
20
40
60
80
100
1 2 3 4 5 6 7 8 9 10 time
antifungalantifungal
conditioncondition
hosthostdefensdefens
ee

A
B
C
I II III
RECOMMENDATIONS FOR ASPERGILLOSIS 2007
RECOMMENDATIONS FOR ASPERGILLOSIS 2007
•Lipid ampho B’s in compromised kidneys
•Caspofungin rescue
•Other ampho B’s, itrafor primary treatment•Pre-emptive works•Early intervention is important
•Ampho B followed by itraconazole
•Surgery in selected cases
•Voriconazole for first line•Liposomal minimal dose 3mg/kg /day
•Posaconazole (oral) for rescue
•Liposomal ampho B for first line•Posaconazole as prophylaxis
•Biological response modifiers•Combination therapy

STRANGE DUCKS IN THE STRANGE DUCKS IN THE IMMUNOSUPPRESSED PONDIMMUNOSUPPRESSED POND
STRANGE DUCKS IN THE STRANGE DUCKS IN THE IMMUNOSUPPRESSED PONDIMMUNOSUPPRESSED POND
Fusarium
Mucor/Rhizopus
Alternaria
Pseudallescheria boydii
Scedosporium
INVASIVE FUNGAL INFECTIONS IN RELATION TO IMMUNE DEFENSE
INVASIVE FUNGAL INFECTIONS IN RELATION TO IMMUNE DEFENSE
compromised compromised defensedefense
severelyseverely compromisedcompromised
external fungal external fungal populationpopulation
our body
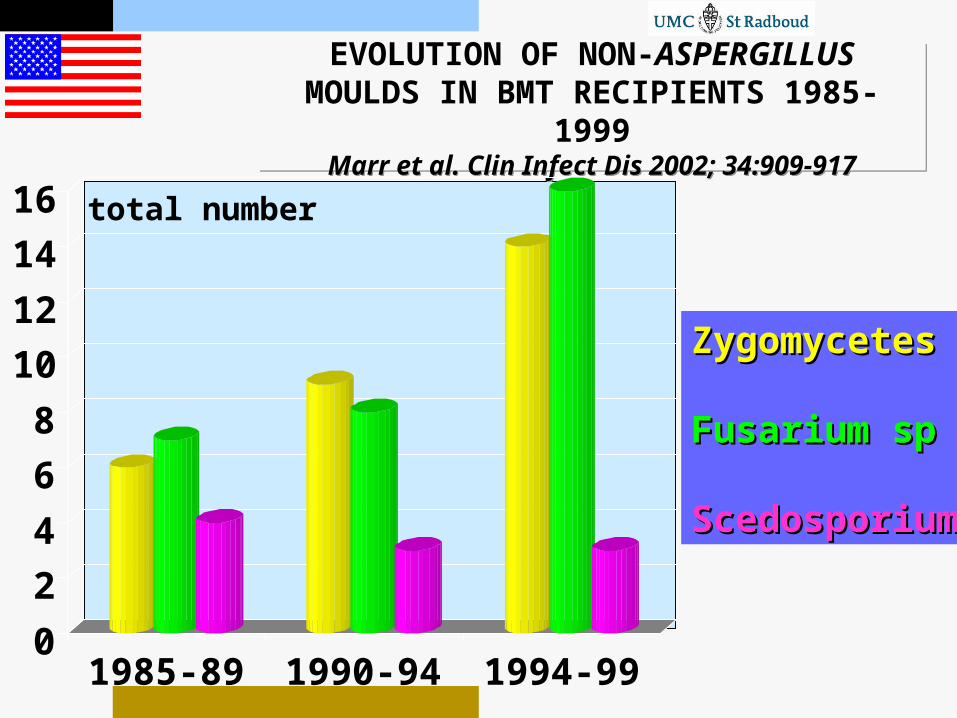
EVOLUTION OF NON-ASPERGILLUS MOULDS IN BMT RECIPIENTS 1985-1999
Marr et al. Clin Infect Dis 2002; 34:909-917
EVOLUTION OF NON-ASPERGILLUS MOULDS IN BMT RECIPIENTS 1985-1999
Marr et al. Clin Infect Dis 2002; 34:909-917
0
2
4
6
8
10
12
14
16
1985-89 1990-94 1994-99
ZygomycetesZygomycetes
Fusarium spFusarium sp
ScedosporiumScedosporium
total number
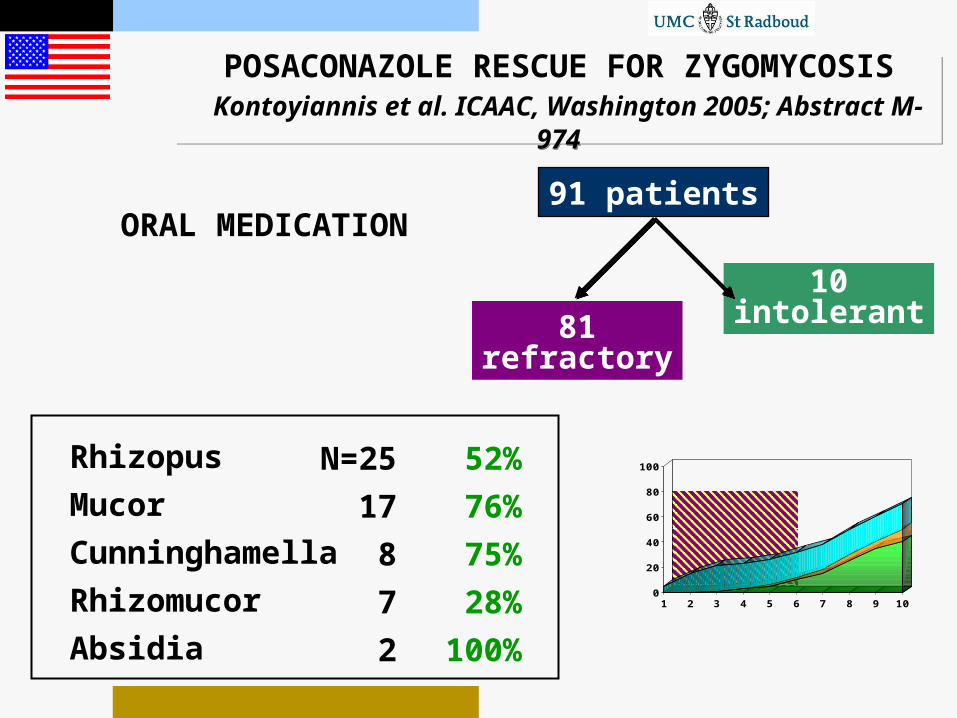
POSACONAZOLE RESCUE FOR ZYGOMYCOSIS Kontoyiannis et al. ICAAC, Washington 2005; Abstract M-974
POSACONAZOLE RESCUE FOR ZYGOMYCOSIS Kontoyiannis et al. ICAAC, Washington 2005; Abstract M-974
91 patients
81refractory
10intolerant
Rhizopus
Mucor
Cunninghamella
Rhizomucor
Absidia
N=25
17
8
7
2
52%
76%
75%
28%
100%
0
20
40
60
80
100
1 2 3 4 5 6 7 8 9 10
ORAL MEDICATION

MUCORMYCOSIS IN HAEMATOLOGIC PATIENTS: TREATMENT RESULTSPagano et al. Haematologica 2004; 89:207-214
MUCORMYCOSIS IN HAEMATOLOGIC PATIENTS: TREATMENT RESULTSPagano et al. Haematologica 2004; 89:207-214
59 cases 49 empirical antifungals
39 amphotericin B4 liposomal amphotericin B
30 failures 9 successes – 23%23%
7 successes – 44% 4 surgery
12 liposomal amphotericin B
8 switches
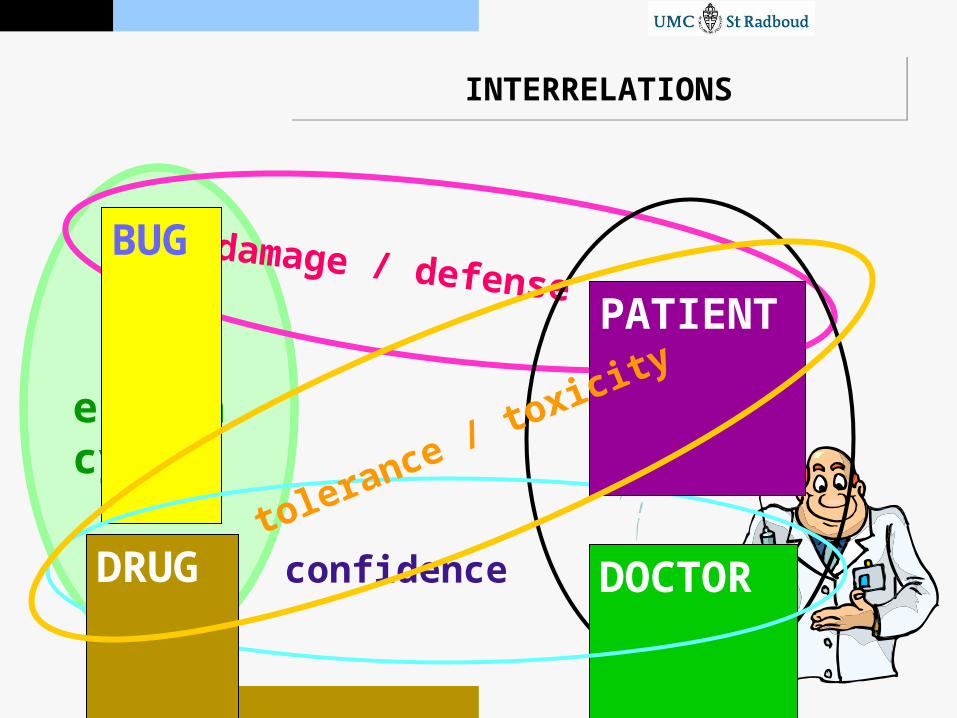
INTERRELATIONSINTERRELATIONS
BUG
efficacy DRUG
BUG
DOCTOR
damage / defense PATIENT
BUG
DOCTOR
PATIENT concern
DRUG
DOCTOR
confidence
PATIENT
DRUG
PATIENT
DRUG
DRUG
PATIENT
tolerance / toxicity

BASIS FOR LOCAL ALGORITMSBASIS FOR LOCAL ALGORITMS
STRATEGY SELECTION
DEPENDS ON:
-physician confidence/experience
-diagnostic tools available
-patient population

amphotericin B
WHAT’S NEW?WHAT’S NEW?
voriconazole caspofungin
micafungin
anidulafungin
posaconazole
liposomalamphotericin B

EVIDENCE LEADS PRACTICEEVIDENCE LEADS PRACTICE
PRACTICE
EVIDENCE
THIS AND FUTURE GENERATIONSTHIS AND FUTURE GENERATIONS