annual report and accounts - enfield ccg about enfield ccg ... welcome to our annual report and...
TRANSCRIPT


Enfield CCG Annual Report 2014/15
Contents STATEMENT OF LEGISLATIVE REQUIREMENTS ...................................................... 2
ANNUAL REPORT ............................................................................................................... 3
1. Welcome from the Chair and Chief Officer ................................................................. 3
2. Member Practices Report ........................................................................................... 5
3.0 Strategic Report ........................................................................................................... 7
3.1 About Enfield CCG ................................................................................................... 7
3.2 Our local population and their health needs ............................................................. 7
3.3 Working with partners .............................................................................................. 9
3.4 How we met our corporate objectives this year ...................................................... 10
3.5 Developing our strategic plans ............................................................................... 17
How we engage with our local stakeholders ................................................................. 19
3.7 Performance of the Clinical Commissioning Group for the Period Under Review and in the Future ................................................................................................................. 23
3.8 The Resources, Principal Risks, Uncertainties and Relationships that may affect the Clinical Commissioning Group’s Long-term Performance ............................................ 25
4.0 Corporate Report ....................................................................................................... 27
4.1 Details of Members of the Membership Body and Governing Body ........................ 27
4.2 CCG Staff .............................................................................................................. 28
4.3 Pension Liabilities .................................................................................................. 28
4.4 Sickness Absence Data ......................................................................................... 28
4.5 External Audit Remuneration ................................................................................. 29
4.6 Disclosure of Serious Untoward Incidents (SUIs) ................................................... 29
4.7 Health and Safety .................................................................................................. 29
4.8 Cost Allocation and Setting of Charges for Information .......................................... 29
4.9 Principles for Remedy ............................................................................................ 29
4.10 Employee Consultation ........................................................................................ 30
4.11 Disabled Employees ............................................................................................ 31
4.12 Equality and Diversity Report ............................................................................... 31
4.13 Equality Information ............................................................................................. 32
4.14 Equality Objectives ............................................................................................... 32
4.15 Equality Analysis .................................................................................................. 32
4.16 Equality Delivery System (EDS2) ......................................................................... 32
4.17 Workforce Race Equality Standard ...................................................................... 33
4.18 Fraud ................................................................................................................... 33
4.19 Emergency Preparedness, Resilience and Response Planning ........................... 34
Local clinicians working with local people for a healthier future Page 1 of 68

Enfield CCG Annual Report 2014/15
4.20 Training and Exercises ......................................................................................... 34
4.21 Sustainability Report ............................................................................................ 35
5. Statement as to Disclosure to Auditors ........................................................................ 35
6. Remuneration Report .................................................................................................. 36
6.1 Membership of the Remuneration and Nomination Committee............................... 36
6.2 Policy on Remuneration of Senior Managers ......................................................... 38
6.3 Senior Managers Performance Related Pay .......................................................... 38
6.4 Policy on Senior Managers Contracts .................................................................... 38
6.5 Senior Managers Service Contracts ....................................................................... 39
6.7 Salaries and Allowances 2014/15 .......................................................................... 41
6.8 Payments for Loss of Office ................................................................................... 42
6.9 Payments to Past Senior Managers ....................................................................... 42
6.11 Pension Benefits .................................................................................................. 43
6.12 Pensions .............................................................................................................. 43
6.13 Member Contribution Rates before tax relief (gross) ............................................ 43
6.14 The relationship between the highest paid director and median remuneration ..... 44
6.15 Off-payroll Engagements ...................................................................................... 44
STATEMENTS BY THE ACCOUNTABLE OFFICER .......................................................... 46
7. Statement of Accountable Officer’s Responsibilities ................................................. 46
8. Governance Statement ............................................................................................. 47
ANNUAL ACCOUNTS ........................................................................................................ 65
9. Introduction: Financial Review of the year and forward look ..................................... 65
STATEMENT OF LEGISLATIVE REQUIREMENTS
The Annual Report and Accounts have been prepared under a Direction issued by the NHS Commissioning Board under the National Health Service Act 2006 (as amended).
We certify that the Enfield CCG has complied with the statutory duties laid down in the National Health Service Act 2006 (as amended).
Local clinicians working with local people for a healthier future Page 2 of 68

Enfield CCG Annual Report 2014/15
ANNUAL REPORT
1. Welcome from the Chair and Chief OfficerWelcome to our Annual Report and Accounts for 2014-15
This report describes how our organisation works, what we achieved and the challenges we faced during our second year as a Clinical Commissioning Group (CCG). Since we were established as an organisation on 1 April 2013 we have been working hard with local partners and stakeholders to improve and develop local health services that better meet the needs of our diverse community. We believe that this year we have made a very positive impact on improving the health of people living in Enfield.
CCGs are membership organisations and GP practices work together to plan, buy and monitor most of the health services that their patients are referred on to. We are a clinically-led organisation, with eight elected GPs representing four localities on our Governing Body. During this year we have had some important changes to the membership of our Governing Body. As our previous Chair, Dr Alpesh Patel had served a three year term; our Constitution stated that we needed to elect a new Chair. Dr Mo Abedi was appointed as the new Chair. We are pleased to retain Dr Alpesh Patel’s knowledge and experience as he took up the post of Clinical Vice Chair. New members were also elected for the North East and South East Localities. The changes to the Governing Body membership are explained later in this report.
We serve a London borough that has a growing population with diverse health needs. Our member practices are committed to working together to invest in the very best quality services for patients within our programme allocation of £337m. This year NHS England launched the NHS Five Year Forward View, which describes the key challenges facing the NHS, including a growing population, rising demand and a funding gap. As local commissioners, we are facing many of these challenges already. Our financial position has proved challenging this year, and we recorded a deficit of £18.9m. We overspent on our main contracts, especially on emergency care where increasing numbers of patients are using these services.
We are committed to commissioning high quality health services and ensuring that the local health care system is sustainable moving forwards. We have worked with Royal Free London NHS Foundation Trust closely as part of their transformation work following the acquisition of Barnet and Chase Farm Hospital and this continues with the redevelopment of the Chase Farm Hospital. The changes following the implementation of the Barnet Enfield and Haringey Clinical Strategy have been embedded across emergency care and maternity. There continues to be challenges for both A&E departments and we have extended the opening hours of the Urgent Care Centre at Chase Farm Hospital to ensure good levels of access prior to our urgent care review in 2015/16.
Local clinicians working with local people for a healthier future Page 3 of 68

Enfield CCG Annual Report 2014/15
Our Transformation Programme focuses on improving community and hospital services and this year we have undertaken key projects including improving the pathways for diabetes and Chronic Obstructive Pulmonary Disease (COPD). We are investing in more Integrated Care services and are working closely with Enfield Council on rehabilitation and enablement projects to ensure. The Transformation and Integrated Care programmes are all about enabling patients to better manage their health at home and providing access to alternatives to hospital services wherever possible.
Looking forward to 2015/16, our aspiration to develop better local health services continues. We are working with the other CCGs across north central London to develop our strategic plans for transformation, planning improvements to services together when there are benefits across a bigger population. We have taken key steps towards co-commissioning primary care plans with the other CCGs in partnership with NHS England which will be further developed during 2015/16. By becoming co-commissioners we can build on the success of our North Central London Primary Care Strategy investment programme which ended in March 2015 and have more influence in the long-term over the development and delivery of local primary care services.
We will continue to work collaboratively with the London Borough of Enfield, as well as our stakeholders, to further develop our Integrated Care programmes as part of the Better Care Fund. Moving forwards, we will continue to commission primarily for quality and always put patients first. As a CCG, we strive to empower people to take a bigger role in their care plans. This enables them to make positive and informed choices about the services that they use and to be active participants in their own health. We look forward to working with our providers in 2015/16 to deliver more personalised care plans. We have continued to involve patients in our transformation projects as well as undertaking regular events and giving feedback opportunities to understand from a user perspective how we can improve local health services.
In the next section we will present our achievements for 2014-2015 from the perspective of our elected GPs who lead our commissioning plans.
We are pleased to present our Annual Report and Accounts for 2014/15 to you.
Dr Mo Abedi Liz Wise Chair Accountable Officer
Local clinicians working with local people for a healthier future Page 4 of 68
Enfield CCG Annual Report 2014/15
2. Member Practices ReportThis year the 49 member practices of Enfield CCG have continued to work together under the Constitution to improve local health services for our patients. Our Constitution explains the principles of how we work together in a democratic and transparent way to plan, buy and monitor services on behalf of people in Enfield. The CCG Constitution continues to evolve. During this year a key change to the Constitution was approved by members which will enable the CCG to jointly commission services with NHS England and other local CCGs.
According to our Constitution, our Governing Body has eight elected GP members, two for each of our four localities. Our elected GPs provide clinical leadership and work alongside NHS managers, a clinical director, lay members, a secondary care doctor, a nurse member representative, the London Borough of Enfield, Healthwatch Enfield and patient representatives to ensure that decisions taken by the Governing Body are focused on the health needs of local patients.
During this year, we held Governing Body elections and two new GPs were elected to the Governing Body: for the North East – Dr Mo Abedi and for the South East – Dr Hardeep Bhupal. Dr Alpesh Patel stepped down from his position as Chair of the Governing Body having served his three year term. A new Chair of the Governing Body, Dr Mo Abedi was subsequently elected for a three year term of office. The CCG is very fortunate to have Dr Patel as the new Clinical Vice-Chair of the Governing Body.
The Governing Body’s work is supported by a system of two-way accountability with the member practices. As a clinically-led organisation our member practices are involved in decision making through regular locality group meetings led by their elected GP Governing Body members. The planning and development of local services is discussed at these locality meetings and feeds back through the locality leads into the CCG’s commissioning priorities. The locality group meetings are also supported by regular engagement with locality and clinical networks across Enfield which includes protected learning time sessions, pan-Enfield GP seminars and questionnaires. The membership is also kept informed through our GP e-bulletin, GP intranet, GP membership events and CCG website.
Developing our Patient Participation Groups This year staff at member practices worked hard to support the development of Patient Participation Groups and we are pleased to say that by September 2014, all member practices had an active PPG.
We have extended the concept of membership from the GPs in Enfield to our patients on whose behalf we commission the services. We welcome the election of a PPG representative and we look forward to our practices supporting the successful candidate in delivering the views of patients when they take up their position on our Governing Body in June 2015.
Local clinicians working with local people for a healthier future Page 5 of 68

Enfield CCG Annual Report 2014/15
Looking forward to 2015/16 Member Practices are committed to continuing to provide high quality care for our patients and ensuring that the services we commission meet their needs and provide value for money. The financial challenge we face in 2014/15, which continues into 2015/16 means that we must work closely with our partners to transform services into systems that are able to deliver affordable coordinated, responsive and high quality care. We are excited to take on this challenge but are fully aware of the continuing quality and productivity challenge (QIPP) that faces the NHS nationally and locally in Enfield. We know that the scale of the challenge in 2015-16 will be significant.
Our vision for transformation is to co-create sustainable systems designed around the outcomes for our populations. We believe that is it critical to those systems that our providers are able to work together to provide care and case management to our populations based around our localities.
We know we need to be able to deliver a technical and information infrastructure to enable health services to operate as a single system and to enable our patients and our commissioned services to become efficient at consulting with each other. We also need to invest in systems that are able to consistently support delivery around self-care and self-management so that patients and carers become part of our care and case management model.
We would like to thank all our partners including local NHS England, our local NHS provider organisations, the London Borough of Enfield, local voluntary sector groups and many others that have supported us this year and continue to help us to build a healthier future for patients in Enfield. We would also like to thank the staff of Enfield CCG who work to support the member practices and Governing Body members, providing operational and management support to local clinical leaders.
Finally, we would like to thank our patients, particularly the volunteers who work in partnership with practices on our PPGs to help us to improve our services. We are passionate about having the patient voice at every level within our organisation providing clinical leaders and managers with their experience as a patient and their ideas for how we can improve local services.
As members of Enfield CCG we commend this Annual Report to you and we look forward to continuing to build on our achievements described in this report.
Local clinicians working with local people for a healthier future Page 6 of 68
Enfield CCG Annual Report 2014/15
3.0 Strategic Report
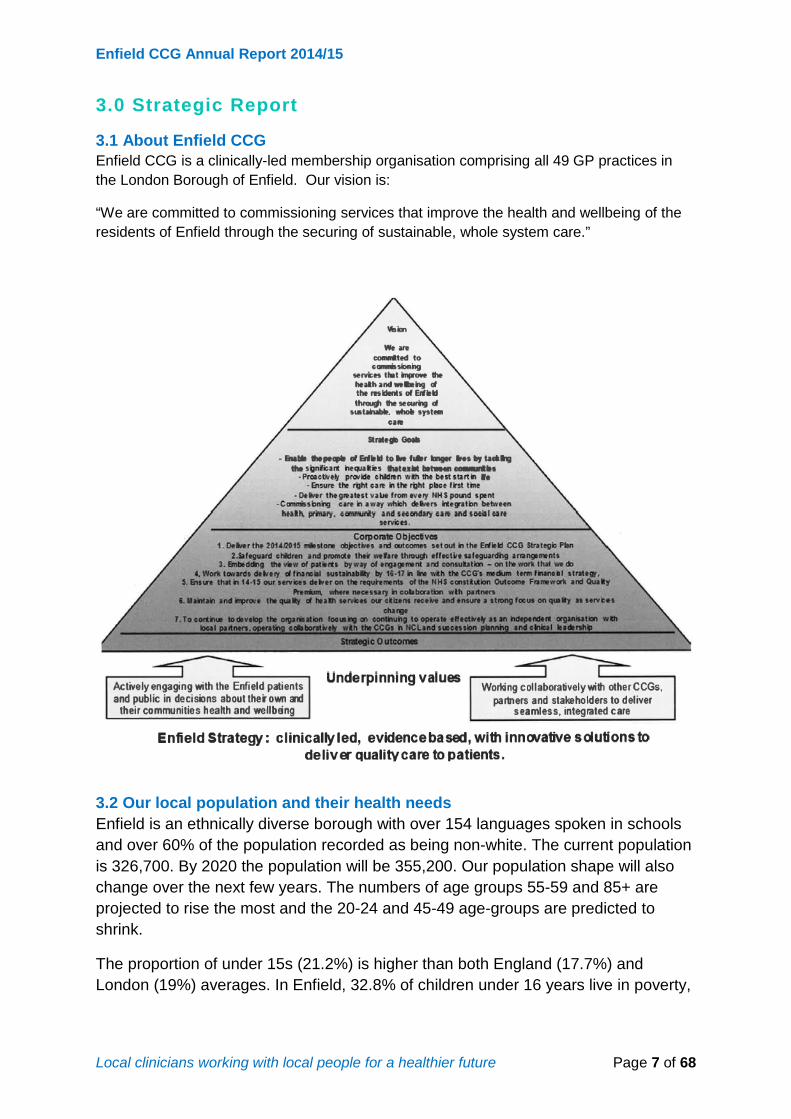
3.1 About Enfield CCG Enfield CCG is a clinically-led membership organisation comprising all 49 GP practices in the London Borough of Enfield. Our vision is:
“We are committed to commissioning services that improve the health and wellbeing of the residents of Enfield through the securing of sustainable, whole system care.”
3.2 Our local population and their health needs Enfield is an ethnically diverse borough with over 154 languages spoken in schools and over 60% of the population recorded as being non-white. The current population is 326,700. By 2020 the population will be 355,200. Our population shape will also change over the next few years. The numbers of age groups 55-59 and 85+ are projected to rise the most and the 20-24 and 45-49 age-groups are predicted to shrink.
The proportion of under 15s (21.2%) is higher than both England (17.7%) and London (19%) averages. In Enfield, 32.8% of children under 16 years live in poverty,
Local clinicians working with local people for a healthier future Page 7 of 68

Enfield CCG Annual Report 2014/15
ranking 6th worst in London and 10th worst nationally. Enfield has the highest number (23,210) of children living in poverty within London.
Enfield is a borough with a significant level of high deprivation. It is the 14th most deprived of the 32 London boroughs and the 64th most deprived local authority district in England out of 326. The three Edmonton wards, in the South East, are all within the most deprived 10% of wards in England, whilst 12 of Enfield’s twenty-one wards are in the most deprived 25% of wards in England.
The map below shows the location of areas of deprivation in Enfield, using national quintiles. The more deprived areas tend to be in the east of the borough, with the south-east of the borough being particularly deprived.
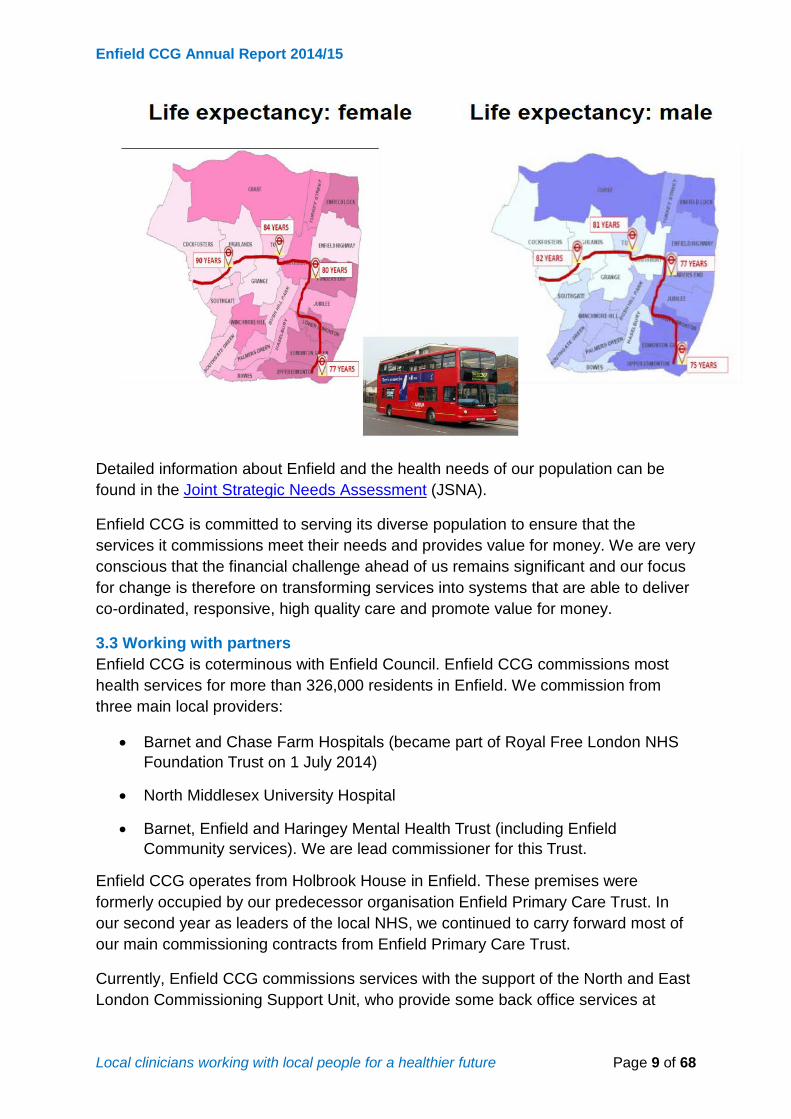
Life Expectancy
There are differences in life expectancy between different areas of Enfield. In areas of higher deprivation, men live 8.7 years less, and women live 8.6 years less.
There is a large gap in life expectancy in Enfield, greater for women than men. Life expectancy at birth in Enfield is 80.5 years for males and 84.0 years for females (above the London average).
These pictures show the gap in life expectancy in the east and west of the borough, illustrated by a journey on the 307 bus which travels through Enfield.
Local clinicians working with local people for a healthier future Page 8 of 68
Enfield CCG Annual Report 2014/15
Detailed information about Enfield and the health needs of our population can be found in the Joint Strategic Needs Assessment (JSNA).
Enfield CCG is committed to serving its diverse population to ensure that the services it commissions meet their needs and provides value for money. We are very conscious that the financial challenge ahead of us remains significant and our focus for change is therefore on transforming services into systems that are able to deliver co-ordinated, responsive, high quality care and promote value for money.
3.3 Working with partners Enfield CCG is coterminous with Enfield Council. Enfield CCG commissions most health services for more than 326,000 residents in Enfield. We commission from three main local providers:
• Barnet and Chase Farm Hospitals (became part of Royal Free London NHSFoundation Trust on 1 July 2014)
• North Middlesex University Hospital
• Barnet, Enfield and Haringey Mental Health Trust (including EnfieldCommunity services). We are lead commissioner for this Trust.
Enfield CCG operates from Holbrook House in Enfield. These premises were formerly occupied by our predecessor organisation Enfield Primary Care Trust. In our second year as leaders of the local NHS, we continued to carry forward most of our main commissioning contracts from Enfield Primary Care Trust.
Currently, Enfield CCG commissions services with the support of the North and East London Commissioning Support Unit, who provide some back office services at
Local clinicians working with local people for a healthier future Page 9 of 68

Enfield CCG Annual Report 2014/15
scale to CCGs. However we also work together with five other CCGs as part of the North Central London Strategic Planning Unit along with Barnet, Camden, Haringey and Islington CCGs. We will continue to work in partnership in north central London and respond to issues affecting our local health economy through the approach of collaborating where it adds value and localising where necessary to deliver the transformational change required.
3.4 Our corporate objectives for 2014/15 In 2014/15 our corporate objectives were:
1. Deliver the 2014/2015 milestone objectives and outcomes set out in theEnfield CCG Strategic Plan
2. Safeguard children and promote their welfare through effective safeguardingarrangements
3. Embedding the view of patients by way of engagement and consultation – onthe work that we do
4. Work towards delivery of financial sustainability by 16-17 in line with theCCG’s medium term financial strategy
5. Ensure that in 14-15 our services deliver on the requirements of the NHSconstitution Outcome Framework and Quality Premium, where necessary incollaboration with partners
6. Maintain and improve the quality of health services our citizens receive andensure a strong focus on quality as services charge
7. To continue to develop the organisation focusing on: continuing to operateeffectively as an independent organisation with local partners, operatingcollaboratively with the CCGs in NCL and succession planning and clinicalleadership.
3.5 How we met our corporate objectives for 2014/15 We are a clinically-led organisation and each of our Governing Body GPs has a leadership role in helping us to deliver our corporate vision and objectives. Our Transformation programme has six programmes of work aligned with our corporate objectives which also support the Joint Health and Wellbeing Strategy:
1. Prevention and primary care2. Integrated care3. Planned care and long term conditions4. Children, young people and maternity5. Mental health, learning disability and continuing healthcare6. Unscheduled care
In addition to the above, we have some cross-cutting programmes aligned to our six main programmes which include:
• Transformation of community services• Value based commissioning• Procedures of limited clinical effectiveness• Acute productivity
Local clinicians working with local people for a healthier future Page 10 of 68
Enfield CCG Annual Report 2014/15
As set out in our five year strategic plan, our Transformation Programme helped us to deliver the national priority objectives for 2014/15:
• Ensuring that citizens will be fully included in all aspects of service design andchange, and that patients will be fully empowered in their own care
• Wider primary care, provided at scale• A modern model of integrated care• Access to the highest quality urgent and emergency care• A step-change in the productivity of elective care• Working with others to ensure the delivery of specialised services
concentrated in centres of excellence
Here are some examples of the developments in some of our key programmes of work during 2014/15 led by our GP commissioners.
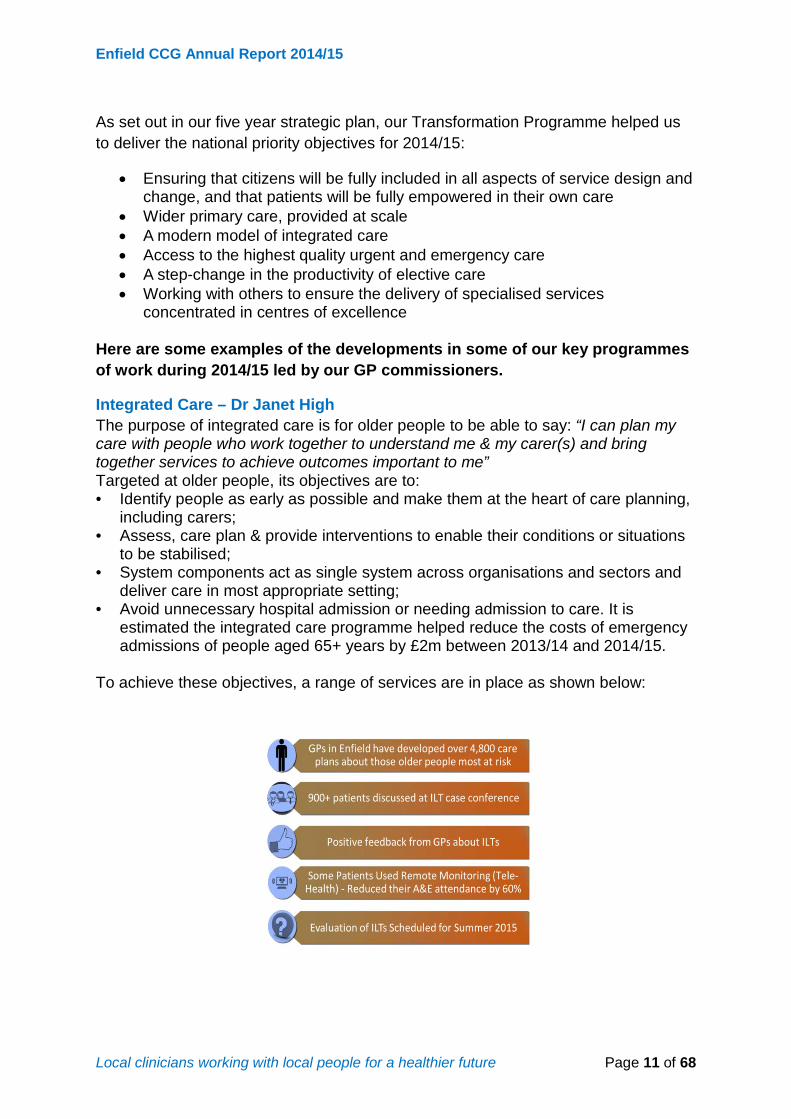
Integrated Care – Dr Janet High The purpose of integrated care is for older people to be able to say: “I can plan my care with people who work together to understand me & my carer(s) and bring together services to achieve outcomes important to me” Targeted at older people, its objectives are to: • Identify people as early as possible and make them at the heart of care planning,
including carers; • Assess, care plan & provide interventions to enable their conditions or situations
to be stabilised; • System components act as single system across organisations and sectors and
deliver care in most appropriate setting; • Avoid unnecessary hospital admission or needing admission to care. It is
estimated the integrated care programme helped reduce the costs of emergency admissions of people aged 65+ years by £2m between 2013/14 and 2014/15.
To achieve these objectives, a range of services are in place as shown below:
Local clinicians working with local people for a healthier future Page 11 of 68

Enfield CCG Annual Report 2014/15
Mental Health and Continuing Care – Dr Anshu Bhagat As lead commissioner for Barnet, Enfield and Haringey Mental Health Trust, Enfield CCG has continued to work closely with the provider to monitor the contract. The implementation of the Enfield Joint Mental Health Strategy has continued.
This year Barnet, Enfield and Haringey CCGs signed the London Crisis Concordat declaration. The declaration commits the signatories to working together to put in place the principles of the national Mental Health Crisis Concordat which aims to improve the system of care and support so that people in crisis because of a mental health condition are kept safe. A tri-borough crisis concordat action plan has been developed with Enfield as the commissioner lead. Working jointly with Barnet and Haringey CCG’s, Enfield was successful in securing additional crisis concordat fund during this financial year. Joint initiatives were commissioned by the three CCGs to:
• Review and map the mental health crisis pathways for adults and 14-18year olds.
• Identify chaotic service users who repeatedly present to services in crisisand propose alternative interventions to meet their needs
Local clinicians working with local people for a healthier future Page 12 of 68

Enfield CCG Annual Report 2014/15
• Review the Early Intervention Service against the NICE model• Reduce the Early Intervention Service waiting lists to enable newly
referred service users to receive treatment within 6 weeks of referral fromApril 2016
• Enable BEH-MHT to establish strong links with localindependent/voluntary sector and commission that sector to provideadditional contacts/ services/ activity opportunities for people experiencinga mental health crisis
Planned Care and Long-Term Conditions- Angela Dempsey • 14 GP practices in south East Enfield have signed up to provide a locally
commissioned diabetes service.• 15 practices in South East Enfield have signed up to provide a community
cardiology service aimed at reducing the incidence of stroke• 100 patients benefited from a pulmonary programme to help them better
manage their COPD
Unscheduled Care – Dr Hardeep Bhupal • CCGs across North Central London are working together to commission the
111 and OOH service under a single contract. The service will commenceApril 2016 when the current contracts expire. This is a clinically ledcommissioning collaboration across the North Central London CCGs and hasmany benefits including a streamlined pathway, strengthened clinicalassessment and enhanced patient experience. Lessons learned from NHSLondon Learning Programme pilots will be used to inform and enhance thenew service.
• We have reviewed and extended the opening hours of the popular andsuccessful Urgent Care Centre at Chase Farm Hospital.
Learning Disabilities and Adult Safeguarding – Dr Ujjal Sarkar Enfield CCG has been working closely with Enfield Council to implement its Transforming Care for people with learning disabilities programme (Winterbourne View) this year. Together the partnership has:
• Established a Community Intervention Service as a pilot (March – September2014) for people with learning disabilities as a risk of being admitted toassessment and treatment services
• Reduced admissions to learning disabilities specific assessment andtreatment services from on average 9 down to 1
• Ensured that meaningful discharge and “moving on” plans are in place forindividuals with learning disabilities who are in long stay secure hospitalplacements and that these individuals where possible, are supported to live inthe community where they can lead rich and fulfilling lives.
• Reviewed psychiatry services for people with learning disabilities• Increased the number of patients and carers accessing health checks, helping
to improve health inequalities and provide preventative treatment• Completed a review of day opportunities services for people with learning
disabilities to establish value for money in terms of quality, safety andefficiency of services
Local clinicians working with local people for a healthier future Page 13 of 68

Enfield CCG Annual Report 2014/15
• Applied to take part in NHS England’s Integrated Personal Commissioningpilot.
Additional Safeguarding achievements:
• In September 2014, NHS England circulated a guide to all ClinicalCommissioning Groups and gave advice on what assurances the CCG shouldbe looking for from their providers regarding the Mental Capacity Act (2005)(MCA) and Deprivation of Liberty Safeguards (DoLs). Based on the guidance,an audit and information collection tool was developed by Enfield CCG. Theaudit has been project managed as part of the MCA programme work beingundertaken by Enfield and funded by NHS England.
• A number of nurse practitioners have been identified as requiring the BestInterest Assessors training (MCA & DoLs). Enfield CCG has ring-fencedfunding for 6 practitioners.
• The Assistant Director for Safeguarding has undertaken and passed the BestInterest Assessors Course and is now assessing the Mental Capacity ofpatients in Enfield.
• Enfield CCG hosted a MCA & DoLS Conference in October 2014. Theconference aimed to deliver a learning and awareness opportunity toproviders across the borough of Enfield. Initially targeted at nursing homesand domiciliary care providers, the event was broadened to include healthprofessionals from Primary Care mental health and the acute sector providingan opportunity for networking across the care pathway.
• Following the conference, workshops were developed by the CCG and theMCA and DOLS lead for the local authority to facilitate care home managersto attend to continue increasing awareness and training on this issue.
• The CCG has secured some further funding to promote training of MCA &DOLS amongst GPs and other primary care staff. Training will take place in2015-16.
• NHS Enfield designed and piloted a Patient Engagement Questionnaire inEnfield nursing homes. Analysis of findings will be included in the CCGAnnual Report and reported at the Safeguarding Adults Board.
• The borough-wide Pressure Ulcer Protocol was facilitated and completed byEnfield CCG safeguarding staff.
• As part of the roll out programme for the Pressure Ulcer Protocol, the CCGhave arranged workshops to be held locally to facilitate increased awarenessand training on this issue for care homes and residential home staff. Theworkshops are open and available to staff at all levels in the care home. Theworkshops have been positively evaluated.
• Enfield CCG nursing Staff has produced a number of investigator reports onnursing homes and the Coroners’ office.
• The safeguarding adults team have trained CCG staff in safeguarding adultsand PREVENT
Primary Care Strategy – Dr Mo Abedi The 31 March 2015 marked the end of a three year programme of primary care investment across North Central London. The Primary Care Strategy, originally developed by NHS North Central London in 2012, was designed to improve primary
Local clinicians working with local people for a healthier future Page 14 of 68

Enfield CCG Annual Report 2014/15
care premises and services across the five boroughs. Some projects were implemented across North Central London, particularly improvements around GP IT systems and others were bespoke to each borough. Here is what the programme achieved in Enfield.
• Initiatives to improve access included the commissioning of an Access LocallyEnhanced Service (LES) providing support from the Primary Care Foundationto match capacity to demand. An additional 600 GP appointments per weekare offered as a result of access initiatives introduced
• Telephone triage training of GP staff. 110 GPs now offer telephoneappointments since completing training
• 152 Medical Receptionists completed customer care training• Access Pilots with 18 practices to enhance and improve access. 60% of
patients report an improvement in obtaining an appointment with theirpractice
• Patient satisfaction measured by the roll out of handheld patient experiencetracker devices in practices
• We worked on a project with University College London to bring fourpostgraduate Principal Clinical Teaching Fellows to Enfield. They will deliveran additional 17,000 GP appointments in their host practices
• Roll out of minor ailments scheme. 7,000 Minor Ailment Schemeappointments delivered by Enfield Community Pharmacies, resulting in thesame number of freed up GP appointments
• Improved self-care monitoring of weight and blood pressure through waitingroom Health Kiosks. 126,000 patients monitored their weight and bloodpressure via Health Kiosks
• Significant improvements in GP IT systems• Improvement of GP Premises environment and compliance with CQC
requirements via Improvement Grant allocation• Development of new health centre at Ordnance Road with London Borough of
Enfield relocation and re-tender of practice from old building not fit forpurpose
• Two GP Networks were been established. Once fully assured, both GPNetworks will be able to deliver services at scale to their locality populations
• 1,200 patients are now receiving their anti-coagulation care from communityhubs closer to their homes.
Children’s Safeguarding and Maternity Services – Dr Fahim Chowdhury • Perinatal mental health training has commenced• The number of caesareans has been reduced at Barnet Hospital
Children’s safeguarding
• The Enfield Safeguarding Children Board (ESCB) was subject to aninspection as part of the Ofsted inspection framework for the first time in
Local clinicians working with local people for a healthier future Page 15 of 68
Enfield CCG Annual Report 2014/15
January 2015. As a Board partner, Enfield CCG played an integral role in this inspection. The arrangements in place to evaluate the effectiveness of what is being done by the Local Authority and board partners to safeguard and promote the welfare of children were judged good by the team of inspectors.
• The inspectors found there were strong and effective partnerships meaningthat partners are holding each other to account for the delivery of good multi-agency services to children. The judgement included a review of the governance of the ESCB and demonstrated the commitment of Board partners on attendance, communication and links with the Health and Wellbeing board along with the Safeguarding Adults Board.
• The inspectors highlighted as good the ESCB’s scrutiny and challenge in theform of their annual Section 11 audits. The safeguarding team at the CCG co-ordinate the health responses to Section 11 and the Designated Nurse is a member of the multi-agency challenge panel. The inspectors noted the effectiveness of this challenge panel in providing additional oversight and scrutiny.
Identification, Referral to Improve Safety (IRIS) project
• The project aids the identification of women experiencing domestic violenceand gives a framework for the GP practice staff to manage patients who areexperiencing domestic violence. This project continues to be successful in theidentification of Domestic Violence and abuse. A total number of 90 referralshave been made to the service from GP practices since the initial training inNovember 2013 to March 2015.
• The IRIS project fits with the National Institute of Clinical Excellence (NICE)guidance published in February 2014 on Domestic Violence and Abuse. Theguidance advocates that all GP practices should have training and have areferral pathway for domestic violence and abuse.
Child Sexual Exploitation
• A profile of Child Sexual Exploitation (CSE) in Enfield has been created usingdata gathered from various agencies including health between December2013 and 5 January 2015. Having deepened the understanding of theprevalence and trends of CSE in Enfield, the Enfield Safeguarding ChildrenBoard formed a Task and Finish Group which includes the Designated Nursefor the CCG to develop a multi-agency action plan for the borough.
• The multi-agency action plan incorporated a number of recommendationsfrom recent local and national reports such as the Rotherham report. Theaction plan has been progressed to include current multi-agency practice andagency developments shared during the meetings of the Task and FinishGroup.
• The involvement of health services in the action plan has been key,particularly to the area of support, such as ensuring appropriate clinical sexualhealth services for victims as well as ensuring therapeutic interventions areavailable.
Local clinicians working with local people for a healthier future Page 16 of 68

Enfield CCG Annual Report 2014/15
• The Designated Nurse invited the author of the problem profile and theBusiness Manager for Enfield Safeguarding Children Board to the EnfieldCCG Strategic safeguarding children committee to present the multi-agencyaction plan and ensure the Named leads in the provider organisations werecognisant with the action plan.
Female Genital Mutilation
• A health needs assessment on Female Genital Mutilation (FGM) has beencompleted and presented to the Enfield Safeguarding Children Board. Theassessment highlighted there are an estimated 2823 girls and young womenat risk of FGM in Enfield.
• Enfield Safeguarding Children Board has established a Task and Finish Groupto co-ordinate the Borough’s response to Female Genital Mutilation. Eachhealthcare provider is represented at this subgroup. The Designated Nurse isa member of the Task and Finish Group.
Safeguarding Lead GP Forum
• The CCG Safeguarding team have established a Safeguarding lead GP forumfor the Safeguarding lead at each practice to attend. Each forum has a focussession on adults at risk and on child safeguarding.
• Sessions have included an update on the Adult Multi-Agency SafeguardingHub, Adults with Learning Disabilities, substance misuse, child sexualexploitation, sexual health, referrals process for adults at risk and link healthvisitors.
3.6 Developing our strategic plans Enfield CCG continues to have an ambition that aim to improve the outcomes that are important to our patients. We continue to develop an approach to commissioning that is based on populations including older people, adults with long term conditions, adults with mental health issues, children with universal needs and children with additional needs. Most of our work is with our main providers to bring about collaborative approaches that are able to deliver outcomes that patients tell us are important. We continue to focus on our key national and local outcomes as described in our operating plan including the NHS Constituent and the Quality Premium. Whilst we have been able to put in place some of the building blocks for change to secure safe, resilient and sustainable systems, we must now begin to accelerate the transformation of services and systematically improve the standards of care and outcomes our population experiences.
The CCG is committed to serving its population to ensure that the services it commissions meet their needs and provide value for money. We are very conscious that the financial challenge ahead of us remains significant and our focus for change is therefore on transforming services into systems that are able to deliver affordable coordinated, responsive and high quality care.
Our key priorities over the next five years include: • The development of locality infrastructures managing locality populations.
Local clinicians working with local people for a healthier future Page 17 of 68

Enfield CCG Annual Report 2014/15
• Shifting resources from activity based contracting to commissioning based onoutcomes for patients through our value based commissioning approach.
• Supporting the redevelopment of Chase Farm Hospital• Continuing to move forward our integration agenda through our model of
integrated care and implementation of the Better Care Fund.• Implementing a stepped up recovery programme for those in our population
with mental ill-health.• Reducing inequalities through the implementation of our Joint Health and
Wellbeing Strategy and other partnership work.
Our Transformation Programme is continuously informed by detailed analysis of borough and CCG wide performance based on a range of data sources including the Joint Strategic Needs Assessment, NHS England CCG value pack and comparator benchmarking exercises. This has enabled us to further identify more population specific groups and areas for improvement.
Our Transformation Programmes, collaborative work across our North Central London Strategic Planning Unit as well as some of the other initiatives and key enablers set out in our strategic plan will help drive forward the changes to improve health and healthcare in Enfield. Our local priorities are also linked to our shared responsibility to deliver our Joint Health and Wellbeing Strategy.
We have worked and will continue to work closely with the Health and Wellbeing Board on the development of the Joint Health and Wellbeing Strategy, Better Care Fund plans and our CCG’s five year strategic and two year operational plans.
Integration continues to be a key area for Enfield CCG moving forwards. We have worked with Enfield Council to produce a Better Care Fund plan based on accelerating our progress to deliver the priorities and outcomes agreed by our Health and Wellbeing Board. We are home to a larger than average population of young people, but our older population is also set to increase dramatically to over 16.6% of our population from 2032. For these reasons, and because of our particular demographic pressures, our plan is targeted at improving outcomes across four population groups. These are the population groups around which our NHS and local authority planning is based, and we have used these groups in order to provide a framework across our commissioning intentions.
The population groups are:
1. Older people – focussed on those experiencing frailty and/or disability
2. Working age adults – focussed on those with long-term conditions
3. Adults experiencing mental health issues
4. Children with health needs
We have agreed a common pathway approach across all of our population groups which span the full range of our ambition from prevention and early intervention right
Local clinicians working with local people for a healthier future Page 18 of 68

Enfield CCG Annual Report 2014/15
through to integrated pathways and support for people at home. Our common pathway is backed up by the locality structure we have already developed with our Health and Wellbeing Board, providers and partners in response to the priorities they have helped us to shape. In doing so, we will address multiple issues, including accelerating our existing programme for integrating care for older people, investing in safeguarding and quality, supporting carers, maximising the contribution of the third sector and building our infrastructure to support more integrated ways of working.
Within those programmes, through assessment and prioritisation, we will continue to aim to deliver efficiencies and savings through:
• Prevention and early intervention
• Single points of contact and joint assessments
• Rapid response and re-enablement
• Rapid access and integrated discharges for all populations groups
• Seven day discharge planning
• Step up step down
• Care co-ordination and case management
• Integrated care teams
We are committed to ensuring that service users contribute to decisions that are important to them, for example Enfield CCG continues to work with the London Borough of Enfield to utilise existing direct payment infrastructure to ensure a single process across direct payments and personal health budgets. Self-management is a crucial part of our service delivery models and we are investing in supporting self-management programmes for people with long-term conditions through the Better Care Fund.
3.7 How we engage with our local stakeholders Patients are at the heart of everything we do and we are committed to involving them in our commissioning decisions. In 2014 we revised our corporate Communications and Engagement Strategy which describes how we involve our stakeholders in our work. Some examples of how we did this in 2014/15 are below.
• We have worked in partnership with other public sector organisations to co-ordinate the planning and delivery of local health services and will continue toinvolve service users in redesigning patient pathways wherever possible.
• We hold three public events a year around the commissioning cycle. Wepublish the feedback from these events on ourwebsite http://www.enfieldccg.nhs.uk/Listening-to-you.htm
• We also present to voluntary and community groups on request e.g. CarersForum; Over 50s Forum; Enfield Vision, BME Health Seminar organised byEnfield Racial Equality Council.
Local clinicians working with local people for a healthier future Page 19 of 68

Enfield CCG Annual Report 2014/15
• We attended summer festivals e.g. Edmonton Summer fair and Enfield TownShow.
• Our Patient and Public Engagement (PPE) Committee reviews the delivery ofour communications and engagement and our equality and diversitystrategies.
• We continued to use our website to publish information about the CCG andlocal services. The website is inclusive and use technologies that will help usengage and communicate with people with disabilities.
• We regularly published materials electronically, as hard copies and whereverpossible produced plain English summaries of our key documents.
• We continued to promote the Choose Well marketing campaign and ChooseWell North London App in partnership with Barnet and Haringey CCGs whichexplains the range of local NHS services available.
• We continued to support the development of local Patient ParticipationGroups (PPGs) in all our GP practices. We also supported the development ofan Enfield Patient Participation Group network which meets quarterly.
• Our interim PPG representatives continued to sit on our Governing Body in2014/15 as we worked towards delivering an elected representative by May2015. The successful candidate will be elected by the PPGs and be theirvoice on the Governing Body.
3.8 Commissioning for quality
Our patients tell us that the quality and safety of services is critical and we have to make sure that this is maintained. To put patients at the heart of everything we do, we use three key domains to evaluate quality as set out in our Governing Body approved Quality Strategy.
Our agreed quality assurance framework is monitored through the provider clinical quality review and contract monitoring meetings as well as the CCG’s own internal governance process through our Quality and Safety Committee.
Provider clinical quality groups and contract monitoring meetings provide a forum for detailed oversight and scrutiny of provider performance against service quality
1. Safe service (Patient Safety)The right staff, correctly trained, learning from experience
2. Effective service (Clinical Effectiveness)Evidence based, right care, right place, first time
3. Good experience (Patient Experience)Service users feel valued and cared for
Local clinicians working with local people for a healthier future Page 20 of 68

Enfield CCG Annual Report 2014/15
schedules and Commissioning for Quality and Innovation Payments (CQUIN) frameworks.
Quality schedules and CQUINs which form part of the contract between the CCG and its provider contain a range of key performance indicators and stretch targets relating to patient experience, patient safety and clinical outcomes. Each provider’s quality schedule contains a range of measurable quality metrics relating to patient experience, patient safety and clinical outcomes. Progress against the quality schedules and CQUINs is reported to the Quality and Safety Committee. With smaller contracts, where a clinical quality review meeting is not viable, a contract manager leads this dialogue through contract monitoring meetings.
Where performance issues arise, plans are put in place to achieve compliance and unresolved issues are escalated to the CCG Quality and Safety Committee and Governing Body as appropriate.
Enfield is the lead CCG commissioner for Barnet, Enfield and Haringey Mental Health Trust. Enfield CCG also works collaboratively with other CCGs, particularly in managing quality in our acute and mental health providers, and has also signed a collaboration agreement with the CCGs in north central London (Barnet, Camden, Haringey, and Islington) to achieve this. Monthly meetings are held with providers for the purpose of assurance across the quality agenda.
Enfield CCG has commissioned the North and East London Commissioning Support Unit under a service level agreement, to monitor aspects of quality and safety on our behalf. An integrated provider quality and performance report is reviewed by the CCG Quality and Safety Committee to ensure continuous quality improvements.
Our quality outcomes in 2014/15
We are committed to ensuring the quality of local health services. Here are some examples of Enfield CCG’s 2014/2015 quality outcomes and in response to Francis, Berwick, Keogh and the Winterbourne Report recommendations:
• The CCG expects all commissioned services to use feedback to improve theirservices and work alongside the CCG to regularly inform, consult and involvepatients, their families, carers and the public in the planning and review ofservices. During 2014 the CCG refreshed its Communication andEngagement Strategy which supports this approach by describing how we ascommissioners will also collect views from our patients and feed these in toour commissioning work.
• In July 2014 the CCG’s Quality Strategy was reviewed and approved by theGoverning Body. This strategy supports the CCG in keeping quality at theheart of all the CCG does. It communicates the vision, key drivers andambitions for quality and it explains how the CCG will deliver this vision. Itdescribes the CCG’s commitment to continuous improvement of qualityoutcomes and encourages the development of robust quality assurance
Local clinicians working with local people for a healthier future Page 21 of 68

Enfield CCG Annual Report 2014/15
mechanisms, in order to provide assurance to the Governing Body about the standard of quality and patient safety in commissioned services.
• The CCG is constantly seeking ways to actively identify quality issues through innovative means. In 2014, the CCG refreshed its quality alerts system introduced in 2013 to enable GPs to raise concerns on behalf of their patients. Our system has already been adopted by many other CCGs. The quality alerts system identifies opportunities to improve the care patients receive, particularly around communication and discharge processes. In 2015-16, the quality alert system will be rolled out more widely to other providers like care homes.
• We have conducted a table top review of Enfield Community Services on quality reporting through the contract. The report noted that there were no areas of concern identified that were not already reported or subject to improvement monitoring. The review has informed the strengthening of the contract quality schedule for 2015/16.
• We participate in the local Quality Surveillance Group (QSAG). This group is chaired by NHS England and works with health and social care colleagues to identify system wide issues through intelligence sharing as well as the triangulation of soft intelligence. Membership of the QSAG includes Monitor, Trust Development Authority & the Care Quality Commission.
• Locally developed ‘key performance indicators’ (KPIs) are included in acute and community 2015-16 contracts to drive performance in key areas such as complaint handling, mandatory training and incident reporting.
• We work with local acute providers to ensure strong arrangements are in place to manage and learn from complaints in a systematic way and to communicate how services are responding and changing in response to patient feedback. We have also been working closely with our hospitals to ensure they minimise the risk to patients of infections such as MRSA and Clostridium Difficile, and that patients do not suffer avoidable harm, such as pressure ulcers and falls.
• We have revised our Quality Impact Assessment (QIA) tool to support QIPP project managers in assessing quality impacts associated with service redesign and to identify appropriate metrics to inform service specifications and monitor risks. These assessments are discussed alongside scoping papers or draft service specifications to support decision-making by the CCG. In 2015/2016, the CCG will ensure QIAs continue to be embedded in project governance; owned and reported to the project steering groups.
• The Francis Report makes specific recommendations in relation to elderly people with frailty. It is clear from this report along with other inquiries such as Winterbourne View that the most vulnerable patients are at the most risk from harm. Enfield CCG and Enfield Council prioritise the care of older people and have placed particular emphasis on the quality of care provided in local nursing homes during 2014-15
• We have hosted Four Mental Capacity Act (MCA) and Deprivation of Liberty Safeguard (DOLS) surgeries to provide advice and information available to care home staff in Enfield. The events have led to an agreement to co-develop a shared policy for care homes with the borough. As part of the funds received jointly by Enfield, Barnet and Haringey CCGs from NHS England, work continues to raise awareness of the Act among patient and carers, three engagement events were held across the boroughs. A suite of patient
Local clinicians working with local people for a healthier future Page 22 of 68

Enfield CCG Annual Report 2014/15
information leaflets on advance care planning is in the final stages of completion. The leaflets will be circulated to all GP practices, voluntary organisations and providers for use from April 2015. A conference to share the learning and challenges faced by providers over the last twelve months will take place in May 2015. 240 training places have already been made available to GPs across the three CCGs.
• A MCA DOLS Champion Training model is being introduced following thesuccess of the Haringey project earlier in the year. Key ward and unitmanagers from acute, mental health and community providers have beennominated to undertake intensive training with additional learning support.
• Commissioners, the CCG Continuing Healthcare Team and the IntegratedLearning Disabilities Service have all worked in partnership to identify peoplewho meet the Winterbourne View Concordat criteria. The Winterbourne ViewProject Team has worked to meet the deadlines as set out in the concordatand believe that they are compliant with the June 2014 deadline. Due to thesuccess of local implementation of the Winterbourne View Concordat, NHSEngland representatives have requested to visit our Integrated LearningDisabilities Service.
• We take our responsibility seriously to ensure that systems are in place tomake sure our children and vulnerable adults are safe and protected andclose working with partner agencies for both child and adult safeguardingcontinues. We will triangulate safeguarding systems and processes with otherquality alerts, in particular the CCG’s response to the prevention of pressureulcers.
• We have designed an Enfield Pressure Ulcer Protocol which sets out how toreport concerns to the local authority and the CQC. This provides a pathwayto support consistent and appropriate referral of pressure ulcers that arecurrently reportable as serious incident to the local authority’s SafeguardingAdults service.
Some of our priorities for 2015/16 are: • We will review our Walk the Pathway Protocol in response to feedback from
providers to listen, record, triangulate, investigate, learn, act and share patientexperience. The protocol includes a programme of visits for 2015/16 forproviders for which the CCG is lead commissioner. It is hoped that theprotocol will inform and support Healthwatch’s schedule of Enter and Viewvisits in 2015-16.
• For 2015/2016, we will also strengthen learning disabilities contractualperformance and quality indicators. This will incorporate needs related tolearning disabilities elements of the vast range of services commissioned fromthe community services provider.
3.9 Performance of the Clinical Commissioning Group for the Period Under Review and in the Future Enfield CCG has made good progress this year against NHS Constitutional standards and other supporting measures set out in the CCG Operating Plan, in line with its statutory responsibilities. Barnet and Chase Farm sites of the Royal Free London NHS Trust are currently not reporting referral to treatment times (RTT) due
Local clinicians working with local people for a healthier future Page 23 of 68

Enfield CCG Annual Report 2014/15
to issues with reporting systems at the Trust. Significant progress has been made by the RTT Programme Board set up by the Trust to address the issues following their acquisition of the former Barnet and Chase Farm NHS Trust in July 2014.
Enfield CCG has delivered against the standards for a range of NHS Constitutional measure for the year as shown in the table below. As an associate commissioner to local providers contracting arrangements the CCG worked closely with lead commissioners to ensure remedial action plans are in place and monitored to address areas of underperformance.
Standard Performance Referral to Treatment waiting times for non-urgent consultant-led treatment* Admitted patients to start treatment within a maximum of 18 weeks from referral 90% 91.0%
Non-admitted patients to start treatment within a maximum of 18 weeks from referral 95% 95.0%
Patients on incomplete non-emergency pathways (yet to start treatment) should have been waiting no more than 18 weeks from referral
92% 92.1%
Diagnostic test waiting times Patients waiting for a diagnostic test should have been waiting less than 6 weeks from referral 99% 98.6%
A&E Waits Patients should be admitted, transferred or discharged within 4 hours of their arrival at an A&E department 95% 94.5%
Cancer Waits – 2 week wait Maximum two-week wait for first outpatient appointment for patients referred urgently with suspected cancer by a GP
93% 94.4%
Maximum two-week wait for first outpatient appointment for patients referred urgently with breast symptoms (where cancer was not initially suspected)
93% 93.7%
Cancer Waits – 31 days Maximum 31-day wait from diagnosis to first definitive treatment for all cancers 96% 99.2%
Maximum 31-day wait for subsequent treatment where that treatment is surgery 94% 97.6%
Maximum 31-day wait for subsequent treatment where that treatment is an anti-cancer drug regimen 98% 99.7%
Maximum 31-day wait for subsequent treatment where the treatment is a course of radiotherapy 94% 99.6%
Cancer Waits – 62 days Maximum 62-day wait from urgent GP referral to first definitive treatment for cancer 85% 81.0%
Maximum 62-day wait from referral from an NHS screening service to first definitive treatment for all cancers
90% 95.9%
Local clinicians working with local people for a healthier future Page 24 of 68

Enfield CCG Annual Report 2014/15
*Excludes data for Barnet and Chase Farm Hospital Sites of Royal Free London NHS Trust due todata reporting issues.
The CCG has continued to work in partnership with local Health and Wellbeing Board, providers and other CCGs to deliver its statutory obligations and other local priorities. As part of the CCGs Outcome Ambitions for 2014/15 a local commitment was also made to improve patient experience, safety and mental health access. As a result:
• 2.8% of people with depression entered treatment in the last quarter of2014/15 exceeding the 2.5% target
• Dementia diagnosis rates improved from 48% in March 2014 to 56% inFebruary 2015. This was below plan and CCG plans to recover the positionand improve further to 66.75 by the end of 2015/16
• Emergency readmission rates were maintained at the same level as theprevious year of 13%.
3.10 The Resources, Principal Risks, Uncertainties and Relationships that may affect the Clinical Commissioning Group’s Long-term Performance All CCGs have a duty to deliver both financial and other statutory duties. The CCG is expected to manage its business within the resources allocated to it:
• Expenditure should not exceed the revenue allocation• The CCG will manage its cash flow to target• Running costs not to exceed £25 per head of population
The CCG successfully managed its cash flow to target and kept its running costs within £25 per head of population. However it was not able to maintain expenditure within its Revenue Allocation.
Enfield is a financially challenged CCG that was under its “fair shares” allocation by £33m in 2013/14 and £24m in 2014/15. It is forecast to be £16.4m under in 2015/16. Whilst the CCG broke even in 2013/14, this was after receiving £6.3m on a one off basis through the North Central London Risk Share arrangements.
In 2014/15, a planned deficit budget of £5.6m was agreed with NHS England, reflecting a number of pressures including a specialist commissioning adjustment originating late in 2013/14. Due to the increased pressures in 2014/15 the CCG acknowledged it would not achieve its original control total, and in month 9 the CCG amended its forecast to a deficit of £19.0m. The annual accounts show a deficit of £18.9m.
A recently commissioned benchmarking review demonstrated that CCG acute activity and costs were closely aligned to our peer group. It did however highlight several areas on which we will focus in targeting future savings.
Local clinicians working with local people for a healthier future Page 25 of 68

Enfield CCG Annual Report 2014/15
• Acute activity rose significantly in 2014/15, including a headline 20% on NonElective Admissions.
• GP Referral rates increased by c12% in the same time period, causing anincrease in first outpatient appointments.
• Day case and Inpatient elective activity rose by 8.5% in 2014/15, which waslargely attributable to addressing one off waiting list reductions.
• The 2014/15 QIPP programme did not deliver savings to the level expectedfrom service redesign. The total QIPP programme savings were £10.6m ofwhich half are transactional and non-recurrent in nature. The QIPP target was£12.0m and was underachieved by £1.4m.
The CCG has undertaken a review of Project Management Office and Quality, Innovation, Productivity and Prevention (QIPP) structures, processes and documentation to support improved delivery. We have also worked extensively with external consultants to support our recovery plan and have appointed a Recovery Director reporting directly to the Chief Officer.
The CCG also jointly commissioned a Financial Governance Review with NHS England.
In summary the Report recommended that a full risk assessment should be performed as part of our 2015/16 planning, including quantification of risks presented to the appropriate committees. This has been implemented.
The CCG has already implemented many of the other more detailed practical measures recommended by the review. We will implement all of the recommendations by the 30th September 2015.
Finally the report recommended that the CCG produce a Recovery Plan and agree it with NHS England. At the time of writing this Recovery Plan, which covers a five year period, is being finalised. It will then be taken to our Governing Body for scrutiny and approval.
Enfield CCG forecast an in year deficit of £14.4m in 2015/16. This plan is a realistic view of risk and opportunity. However there is a risk that the CCG will fail to achieve the £12.5m QIPP savings target and that our Payment by Results (PbR) acute contracts will overspend our budgets.
To mitigate these risks the CCG have commissioned external help to support building a robust recovery plan. The terms of reference for this work were signed off jointly with NHS England. Whilst the remit covered contracting, monitoring and reporting the main focus is to build and implement the QIPP programme for 2015/16.
Local clinicians working with local people for a healthier future Page 26 of 68

Enfield CCG Annual Report 2014/15
4.0 Corporate Report
4.1 Details of Members of the Membership Body and Governing Body The Chair of Enfield CCG during the first third of the year has been Dr Alpesh Patel. The Chair for the second two thirds of the year has been Dr Mo Abedi. The Chief Officer is Liz Wise. Profiles of Governing Body members can be found on the CCG website here. A list of member practices can be found here and the composition and governance of our membership body can be found in our Constitution.
NAME MEMBERSHIP VOTING GENDER Elected GP members Dr Alpesh Patel
GP Member (ongoing) and Chair (to 31 July 2014) Clinical Vice Chair (from 20 August 2014)
Yes M
Dr Mo Abedi GP Member (from 1 August 2014) and Chair of the Governing Body (from 20 August 2014)
Yes M
Dr Janet High GP Member (ongoing) and Clinical Vice Chair (to 31 July 2014)
Yes F
Dr Anshumen Bhagat
GP Member Yes M
Dr Fahim Chowdhury
GP Member Yes M
Dr Raj Mazumder
GP Member (to 31 July 2014) Yes M
Dr Mike Gocman
GP Member Yes M
Dr Pavan Sardana
GP Member (to 31 July 2014) Yes M
Dr Ujjal Sarkar
GP Member Yes M
Dr Hardeep Bhupal
GP Member (from 1 August 2014) Yes M
Executive Directors Liz Wise Chief Officer Yes F Simon East Interim Chief Finance Officer (until 26 June 2014) Yes M Ian Winning Interim Chief Finance Officer (from 1 July 2014 to 14
November 2014) Yes M
Rob Whiteford
Chief Finance Officer (from 17 November 2014) Yes M
Aimee Fairbairns
Director of Quality and Integrated Governance No F
Graham MacDougall
Director of Strategy and Partnerships No M
Jane Pike Interim Director of Operations (from 7 August 2014 to 31 December 2014)
No F
Jane Pike Director of Operations (from 1 January 2015) No F Dr Mo Abedi Medical Director (until 31 July 2014) No M
Local clinicians working with local people for a healthier future Page 27 of 68

Enfield CCG Annual Report 2014/15
4.2 CCG Staff Information about CCG staff can be found in Equality Information 2015.
4.3 Pension Liabilities Past and present employees are covered by the provisions of the NHS Pensions Scheme. Details of the benefits payable under these provisions can be found on the NHS Pensions website at www.nhsbsa.nhs.uk/pensions
The scheme is an unfunded, defined benefit scheme that covers NHS employers, GP practices and other bodies, allowed under the direction of the Secretary of State, in England and Wales. The scheme is not designed to be run in a way that would enable NHS bodies to identify their share of the underlying scheme assets and liabilities. Therefore, the scheme is accounted for as if it were a defined contribution scheme: the cost to the NHS Body of participating in the scheme is taken as equal to the contributions payable to the scheme for the accounting period. Further details on pension liabilities can be found in the accounting policy note included in the financial statements and the remuneration report
4.4 Sickness Absence Data Enfield CCG generally has low levels of sickness absence and turnover amongst its staff compared with similar organisations locally, thereby showing a good level of staff motivation and retention. For 2014-2015, the average sickness absence rate was 7.9 working days lost. The average turnover rate is 1% (NHS average is 8.8%).
The CCG has a robust process for managing sickness absence and supporting employees who experience periods of ill health. The CCG through the North and
Lay members Karen Trew Lay Member for Governance and Vice Chair Yes F Teri Okoro Lay Member for Patient and Public Engagement Yes F Other Governing Body Members Angela Dempsey
Registered Nurse Member Yes F
Prof Robert Elkeles
Secondary Care Clinical Lead Yes M
Rathai Thevananth
GP Practice Manager Representative Yes F
Dr Shahed Ahmad
Director of Public Health, London Borough of Enfield No M
Ray James London Borough of Enfield (Director of Health, Housing and Adult Social Care
No M
Bill Mackay/ Litsa Worrall
Interim Patient Participation Group representatives (shared voluntary role) – Bill Mackay attended from 1 April to 31 May 2014 and Litsa Worrall attended Governing Body meetings in public from 1 June to 31 March 2015.
No M and F
Deborah Fowler
Chair, Healthwatch Enfield (from July 2013) No F
Local clinicians working with local people for a healthier future Page 28 of 68

Enfield CCG Annual Report 2014/15
East London Commissioning Support Unit purchase an occupational health and staff support service through AXA PPP Healthcare.
4.5 External Audit Remuneration Our external auditor is Grant Thornton. The cost of its external audit services in 2014-15 was £84,800, excluding VAT as stated in paragraph 47 of the Audit Commission’s guidance.
Grant Thornton were appointed by the Audit Commission as auditors to Enfield CCG. The work they are required to undertake each year is determined by the Audit Commission and includes:
• an opinion on the CCG’s financial statements• a value for money (VFM) conclusion which covers whether the CCG has
proper arrangements in place for securing financial resilience and challenginghow it secures economy, efficiency and effectiveness.
External audit fees are determined by the Audit Commission. The Audit Commission places each CCG into one of nine fee bands, depending on the size of the CCG’s commissioning budget.
4.6 Disclosure of Serious Untoward Incidents (SUIs) There were no serious untoward incidents involving data loss or confidentiality breaches in 2014-2015.
4.7 Health and Safety The CCG has complied with all relevant Health and Safety Legislation.
Risk assessment has been the main focus of safety planning during 2014/15 and the CCG all the necessary assessments in relation to Health and Safety risks to employees.
A program of annual inspections has been put in place during 2014/15 to identify requirements for any additional Health and Safety assessments or training. All staff receive appropriate Health and Safety training at induction and as part of the mandatory training program.
The legislation also requires that assessments are carried out in specific areas at the request of individual members of staff where a risk to Health and Safety is identified. There have been no specific requests for assessment during 2014/15.
4.8 Cost Allocation and Setting of Charges for Information We certify that Enfield CCG has complied with HM Treasury’s guidance on cost allocation and the setting of charges for information.
4.9 Principles for Remedy Enfield CCG has adopted the six Principles of Remedy recommended by the Parliamentary and Health Service Ombudsman when dealing with all complaints and these are included in our Governing Body approved Complaints Policy.
Local clinicians working with local people for a healthier future Page 29 of 68

Enfield CCG Annual Report 2014/15
The six Principles of Remedy are:
1. Getting it right2. Being customer focused3. Being open and accountable4. Acting fairly and proportionately5. Putting things right6. Seeking continuous improvement.
The CCG has also assured itself that local healthcare providers properly investigate, respond and learn from the complaints they receive taking into consideration the recent reports from the Parliamentary and Health Service Ombudsman, “The NHS Hospital Complaints System – A Case for Urgent Treatment” (2013) and the government report co-chaired by Clwyd and Hart (2013).
Trusts provide quarterly reports to quality meetings with the CCG. Reports identify trends and themes from complaints, and the learning identified as a result. They also provide assurance of how that learning is being disseminated and embedded through the Trusts.
The CCG also uses complaints as one aspect of its intelligence gathering about local providers and its own commissioning. This intelligence is considered at the CCG’s Quality & Risk Sub Group in conjunction with other information gathered. Where concerns are identified, further information is sought and necessary action is taken where improvements can be made.
4.10 Employee Consultation In the past year, Enfield CCG has continued to developed the GP intranet and CCG staff intranet site. These sites hold information about key policies, latest news and events. The intranet content is supported by regular emails to staff and GP member practices highlighting important information and linking to the intranet wherever possible.
In addition, the CCG holds monthly staff briefing sessions led by the Chief Officer to summarise the headline news from the CCG, including finance and performance, as well as providing an opportunity for staff to ask questions and share news from their areas of work. All directorates within the CCG hold regular meetings, and it is expected that all managers have regular one-to-one meetings with their staff. These meetings ensure that employees of the CCG have a good understanding of the CCG’s business and ownership of improving the performance of the organisation.
Enfield CCG is committed to working in partnership with trade unions and actively encourages staff to join a trade union and participate in union activities. The CCG is a member of the North Central London CCGs Joint Staffside Partnership Group a collaborative committee of management, human resources and trade union representatives from across the five CCGs in north central London. The committee meets quarterly to provide an environment where management representatives and
Local clinicians working with local people for a healthier future Page 30 of 68

Enfield CCG Annual Report 2014/15
CCG staff representatives can review and discuss changes affecting the organisation. The aim of the Joint Staffside Partnership Group is to:
• Contribute trade union and employer perspectives to the implementation ofpolicy and changes within the CCGs
• Collaborate on the implementation of policy change and local guidance• Promote effective communications throughout the organisation• Promote good practice across the CCGs• Provide a forum for meaningful consultation on any issues of interest to staff• Provide a forum for the negotiation of any appropriate changes to the terms
and conditions of staff in the CCG. This will include Agenda for Change andlocally negotiated terms and conditions
• Exchange views and ideas and promote good employee relations• Partnership working with regards to strategic developments, workforce
planning, reward and recognition strategies and organisational development
4.11 Disabled Employees The CCG has an active policy on equalities which covers the treatment of all employees with protected characteristics including disability. The CCG recognises that discrimination and victimisation is unacceptable and that it is in the interests of the organisation and its employees to utilise the skills of the total workforce. The CCG implements the ‘Two Ticks’ in recruitment and ensures ‘reasonable adjustment’ is made for candidates and employees as required.
It is the aim of the organisation to ensure that no employee or job applicant receives less favourable facilities or treatment (either directly or indirectly) in recruitment or employment on grounds of age, disability, gender / gender reassignment, marriage / civil partnership, pregnancy / maternity, race, religion or belief, sex, or sexual orientation. Please see the equality information on our website for further detail.
Please see Enfield CCG’s equality report for further details.
4.12 Equality and Diversity Report The Equality Act 2010 legally protects people from discrimination in the workplace and in wider society. It replaced previous antidiscrimination laws with a single act, making the law easier to understand and strengthening protection in some situations. It sets out the different ways in which it is unlawful to treat someone. The intention of the general equality duty is to ensure that a public authority like NHS Enfield CCG must, in the exercise of its functions as a public sector organisation, have due regard to three main aims to the need to:
• eliminate discrimination, harassment, victimisation and any other conduct thatis prohibited by or under the Act.
• advance equality of opportunity between persons who share a relevantprotected characteristic and persons who do not share it.
Local clinicians working with local people for a healthier future Page 31 of 68

Enfield CCG Annual Report 2014/15
• foster good relations between persons who share a relevant protectedcharacteristic and persons who do not share it.
4.13 Equality Information Our Equality Information is our annual performance report which we have published in January 2015 to meet the public sector equality duty (PSED). The report outlines the work we have done since April 2013 in relation to policy development, commissioning, engagement, current workforce and recruitment of staff from diverse backgrounds. It also provides further links to our main providers’ equality information about how our providers are meeting their equality duty.
4.14 Equality Objectives Our equality objectives set out what equality outcomes we intend to achieve in our organisation both in workforce and commissioning and how we plan to achieve them. We have refreshed our equality objectives in consultation with our partners, providers and the community and voluntary organisations. We have also developed an action plan to deliver equality objectives and to ensure relevance to our priorities as well as monitoring progress. The CCG is required by the public sector equality duty to develop and publish equality objectives at least once every four year. Our current equality objectives 2012-16 are revised annually through EDS2, the national best practice tool.
4.15 Equality Analysis We routinely analyse our existing and new policies to ensure there is no unintended negative or disproportionate impact on equality groups that are protected by the Equality Act. At NHS Enfield CCG no policy decision is made without an equality analysis of the policy. Our governing body report cover sheet includes a section specifically about equality impact prompting managers to carrying out an equality analysis of the policy or the function they are reporting to the governing body. We maintain a log for all our equality analyses and ensure the actions arising from the analyses are implemented and monitored. Staff receive appropriate training and support to complete equality analysis.
4.16 Equality Delivery System (EDS2) NHS Enfield CCG has adopted the Equality Delivery System (EDS2) as an equality performance management tool. We have been working with NEL Commissioning Support Unit, Healthwatch, the local authority and our providers to assess our performance against four EDS2 goals and eighteen outcomes and to determine the grades. This has helped us to identify gaps, set priorities and develop action plans. Our equality objectives and the action plan will be designed and delivered through EDS2. Our January 2015 Equality Information includes information about the CCG’s current grades and the targets for the future.
Local clinicians working with local people for a healthier future Page 32 of 68
Enfield CCG Annual Report 2014/15
4.17 Workforce Race Equality Standard The Workforce Race Equality Standard (WRES) will, for the first time, require organisations employing almost all of the 1.4 million NHS workforce, to demonstrate progress against a number of indicators of workforce equality, including a specific indicator to address the low levels of Black and Minority Ethnic (BME) Board representation. All providers, as holders of the NHS standard contract 2015/16, except ‘small providers’ will be expected to implement the WRES from April 2015. An annual report will be required to be submitted to the co-ordinating commissioner outlining progress on the WRES. The CCG is working with its providers to ensure through contract monitoring that they meet the standard.
4.18 Fraud One of the basic principles of the NHS is the proper use of public funds. It is therefore important that all staff working in the CCG are aware of the risk of fraud, corruption, theft, and other illegal acts involving dishonesty.
The CCG aims to reduce fraud to the absolute practical minimum and put in place arrangements to hold fraud at a minimum level permanently. This enables the CCG to target more resources at providing better patient care. The CCGs counter fraud approach is professional, comprehensive, fair, balanced, cost effective, specialist and inclusive.
Enfield CCG currently commissions the following services:
• Local Counter Fraud Service (LCFS) - The role of the LCFS is to prevent,detect and investigate allegations of fraud and corruption within the CCG.
• National Fraud Initiative (NFI) – NFI is an exercise that matches electronicdata within and between public and private sector bodies to prevent anddetect fraud. This includes police authorities, local probation boards, fire andrescue authorities as well as local councils and a number of private sectorbodies.
Enfield CCG has also implemented a number of robust policies to assist in our aim of reducing fraud including:
• Anti-Fraud and Bribery Policy• Standards of Business Conduct• Whistleblowing Policy• Disciplinary Policy• Gifts, Hospitality, Sponsorship & Declarations of Interest Policy• Policy for joint working with the Pharmaceutical Industry• Clinical Procurement Framework• NHS England: Managing conflicts of interests: Guidance for CCG's,• Standing Orders
Local clinicians working with local people for a healthier future Page 33 of 68

Enfield CCG Annual Report 2014/15
• Prime Financial Policies• Scheme of Reservation and Delegation• Standards of Business Conduct Policy
4.19 Emergency Preparedness, Resilience and Response Planning Enfield CCG continues to ensure that we meet the statutory obligations of a category 2 responder. These include:
• In 2014, the Governing Body of Enfield CCG approved a combined and inter-related Business Continuity Management Plan and arrangements foremergency planning resilience and response that were compliant with ISO23001 and NHS England Framework respectively. These plans have beenreviewed during 2015 and revised and updated plans will be approved by theGoverning body in 2015/16
• The Business Continuity Management Plan follows best practice in applying abusiness impact analysis and recovery plans for its critical servicedepartments to deal with IT, cold weather, fire and estates issues, whilst theemergency planning resilience and response arrangements demonstratedthat regular guidance received from NHS England and obligations set out inthe Civil Contingencies Act 2004 had been followed as a category 2responder.
• Enfield CCG has in place named Accountable Emergency Officer andEmergency Planning Liaison Officer as required by statutory guidance and toensure that emergency planning is acknowledged to be a critical managementactivity within the organisation.
• Enfield CCG has a presence on the Enfield Borough Resilience Forum andtakes part in local exercises, designed to test the resilience of the Barnet,Enfield and Haringey Clinical Strategy with acute trust emergency planners.
• We regularly attend the North East and North Central London EmergencyPlanning Resilience and Response Network meetings organised through NHSEngland and attended the NHS Emergency Planning Resilience andResponse National Conference in June 2014.
• Enfield CCG also participated in two major NHS emergency planningresilience and response ‘table top’ planning exercises in London in relation tothe Ebola outbreak.
4.20 Training and Exercises • Surge management refresher training was provided by North and East
London Commissioning Support Unit to the executive directors and seniorstaff of Enfield CCG in 2014/15.
• Emergency planning resilience and response refresher training is scheduledto be delivered to executive directors and senior managers in April 2015/16.
• NHS England led ‘Command Post’ training exercises were postponed until2015/16.
• Further NHS wide emergency planning resilience and response exercises areexpected sometime during the autumn of 2015/16.
Local clinicians working with local people for a healthier future Page 34 of 68

Enfield CCG Annual Report 2014/15
• Enfield CCG plan to run some combined local resilience tests with local acutetrusts during the course of the new financial year.
We certify that the Enfield CCG has incident response plans in place, which are fully compliant with the NHS Commissioning Board Emergency Preparedness Framework 2013. The CCG regularly reviews and makes improvements to its major incident plan and has a programme for regularly testing this plan, the results of which are reported to the Governing Body.
4.21 Sustainability Report Enfield CCG continues to support the Government’s aim to reduce overall carbon emissions in each year up to 2020 and beyond. Increasing staff awareness and improving organisational practice forms an important part of achieving this aim.
An important part of CCG strategy in 2014/15 has been to continue the implementation of plans to assess risks, enhance our performance and reduce our impact, including against carbon reduction and climate change adaption objectives. The strategy includes establishing mechanisms to embed social and environmental sustainability across policy development, business planning and in commissioning. Sustainable development principles, actions and measurements will be included as an integral part of all policies, strategies and plans, and ultimately become a normal and accepted part of the leadership and organisational culture in every team, department, and local system.
During the next 12 months, the sustainability action plan will be reviewed to ensure that Enfield CCG complies with its statutory obligations and remains as a local leader of NHS sustainability practice.
Partnership working continues to be a vital element of Enfield CCG’s approach to carbon management and therefore as a tenant at Holbrook House, positive and direct collaboration with NHS Property Services Limited and our landlord Jones Lange and LaSalle is essential. Other partners include the Department of Health, local providers and the London Borough of Enfield.
The CCG will undertake its annual energy audit which will review lighting, heating, cooling and ventilation, electrical equipment, water usage, waste management, transport, procurement and sustainability awareness raising. The audit will also include checking the CCG’s compliance with its Display Energy Certificate.
5. Statement as to Disclosure to AuditorsThe CCG’s Governing Body will make the following statement at their June 2015 meeting in public.
Each individual who is a member of the Governing Body at the time the Member’s Report is approved confirms:
Local clinicians working with local people for a healthier future Page 35 of 68

Enfield CCG Annual Report 2014/15
• So far as the member is aware, that there is no relevant audit information ofwhich the CCG’s external auditor is unaware; and
• That the member has taken all the steps they ought to have taken as amember in order to make them self-aware of any relevant audit informationand to establish that the clinical commissioning group’s auditor is aware ofthat information.
6. Remuneration ReportThe NHS has adopted the recommendations outlined in the Greenbury Report in respect of the disclosure of senior managers’ remuneration and the manner in which it is determined. This report outlines how those recommendations have been implemented by the CCG in the year to 31 March 2015.
6.1 Membership of the Remuneration and Nomination Committee Clinical Commissioning Groups are required to have a Remuneration and Nomination Committee to oversee the pay, terms and conditions of service of senior managers. The main function of the Committee is to give advice to the Governing Body on the remuneration, allowances and terms of service of other officer members to ensure they are fairly rewarded for their individual contribution to the organisation, having regard for the organisation’s circumstances and performance, and taking into account national arrangements.
Enfield CCG’s Constitution sets out that there should be two lay members on its Remuneration and Nomination Committee and that the Governing Body shall appoint the membership of this Committee in consultation with the Chair of the Committee. As of 31 March 2015 the members of the Remuneration and Nomination Committee are as follows:
• Teri Okoro (Chair of the Remuneration and Nomination Committee and Laymember for Patient and Public Engagement)
• Mrs Angela Dempsey (Governing Body Nurse Member)
Local clinicians working with local people for a healthier future Page 36 of 68

Enfield CCG Annual Report 2014/15
• Mrs Karen Trew (Governing Body Lay member for Governance and CCG ViceChair)
• Dr Mo Abedi (GP Chair of the Governing Body)
With the exception of the Dr Abedi all members have been on the Committee since April 2014. There have been seven meetings during the financial year 1 April 2014 to 31 March 2015. Dr Abedi joined the Committee as Chair of the CCG Governing Body from September 2014. From April 2014 to July 2014 Dr Alpesh Patel the previous Chair of the Governing Body was a member of the Committee.
The attendance record of meetings in 2014/15 is set out below:
Members
16 Ap
ril 2
014
8 M
ay
2014
11 J
une
2014
9 Ju
ly
2014
3 S
ept
2014
26 N
ov
2014
4 M
arch
20
15
Tota
l
Teri Okoro (Chair) Y Y Y Y Y Y Y 7/7
Angela Dempsey Y A Y Y Y A Y 5/7
Dr Alpesh Patel A A Y Y N/A N/A N/A 2/4
Dr Mo Abedi N/A N/A N/A N/A Y Y Y 3/3
Karen Trew Y Y Y Y Y Y Y 7/7
Total attendance 24/28 (86%)
During the financial year 2014/15 the Remuneration and Nomination Committee called upon specialist advice from the North and East London Commissioning Support Unit’s HR Business Partner, Ms Eleanor Davies, a service provided as part of the service level agreement between the CCG and North and East London Commissioning Support Unit. This advice covered all aspects of remuneration and terms and conditions of appointments. It also included the production of a detailed benchmarking report which reviewed the salaries of over 10 other CCGs as well as national guidance issued by NHS England which senior managers must comply with. The Committee discussed this confidential report in the context of deciding whether Enfield CCG is following best practice and if remuneration is decided in a similar and fair way in comparison to other CCGs. The Committee concluded from this exercise that the CCG was compliant with NHS England guidance and was setting remuneration and terms and conditions in a fair and comparable way to other CCGs. No fees or additional costs have been incurred from using this service.
Local clinicians working with local people for a healthier future Page 37 of 68

Enfield CCG Annual Report 2014/15
6.2 Policy on Remuneration of Senior Managers The Remuneration and Nomination Committee sets salaries and terms and conditions of service for all Governing Body Members, including clinical members, lay members and the two executive directors (Chief Officer and Chief Finance Officer) on an annual basis in accordance with the CCG’s constitution. All salaries are set with regard to the guidance laid out by NHS England’s Annex 2: Principles relating to reimbursement and remuneration for governing body members April 2012 and also to local benchmarking provided by NEL CSU. The executive directors have their pay and terms and conditions of service set in accordance with the NHS Very Senior Manager (VSM) framework and the NHS London Pay Framework for Very Senior Managers in Strategic and Special Health Authorities, Primary Care Trusts and Ambulance Trusts (June 2013). Pay and terms and conditions for other directors who do not sit on the Governing Body are governed by the national Agenda for Change regulations.
6.3 Senior Managers Performance Related Pay We operate a system of performance-related pay for those senior management posts subject to the Very Senior Managers (VSM) pay framework. There has been no payment of performance related pay during the year ending 31 March 2015.
Future performance related pay for directors will be subject to the terms and conditions of service for very senior managers and will be considered by the remuneration committee. No compensation was payable during the year and no amounts are included that are payable to third parties for the services of senior managers. In the event of redundancy standard NHS packages will apply.
The CCG has a local ‘pay progression’ policy for staff with Agenda for Change contracts, which requires senior managers with NHS contracts to meet the standards of performance set by the individual’s line manager in order to receive incremental progression increases to pay. No performance related bonuses are paid to any senior managers.
6.4 Policy on Senior Managers Contracts The Chair, GP members and lay members of the Governing Body are all engaged via a contract for services. The duration and other terms of office of these are set in accordance with the CCG’s constitution. Notice periods for Governing Body members engaged via a contract for services are set at one month. No termination payments are made on expiry of the contract.
Employed senior managers (the Executive Directors and other directors) are all directly employed on permanent contracts and have notice periods of three months, unless employed on interim contracts. No payments are made on termination except in circumstances of redundancy.
Local clinicians working with local people for a healthier future Page 38 of 68

Enfield CCG Annual Report 2014/15
6.5 Senior Managers Service Contracts Senior Managers Service Contracts
Name and Title Date of the Contract
Unexpired term Notice Period
Provision for early termination
Elected GP members Dr Mo Abedi, GP Member and Chair of the Governing Body *
1 August 2014 2 years 4 months
1 month None
Dr Alpesh Patel, GP Member and Clinical Vice Chair of the Governing Body *
1 August 2014 2 years 4 months
1 month None
Dr Janet High, GP Member *
1 August 2014 2 years 4 months
1 month None
Dr Anshumen Bhagat, GP Member
20 September 2012
6 months 1 month None
Dr Mike Gocman, GP Member
1 August 2014 2 years 4 months
1 month None
Dr Raj Mazumder, GP Member
18 July 2011 Resigned 31 July 2014
n/a None
Dr Pavan Sardana, GP Member
18 July 2011 Resigned 31 July 2014
n/a None
Dr Ujjal Sarkar, GP Member
1 August 2014 2 years 4 months
1 month None
Dr Fahim Chowdhury, GP Member
30 October 2013 1 year 7 months 1 month None
Dr Hardeep Bhupal, GP Member
1 August 2014 2 years 4 months
1 month None
Executive Directors Mrs Liz Wise, Chief Officer 1 April 2013 n/a -permanent 6 months Standard
VSM redundancy provision
Mr Robert Whiteford 17 November 2014
n/a -permanent 6 months Standard VSM redundancy provision
Ms Aimee Fairbairns, Director of Quality and Governance
1 April 2013 n/a -permanent 3 months Standard AfC redundancy provision
Mr Graham MacDougall 1 June 2014 n/a -permanent 3 months Standard AfC redundancy provision
Ms Jane Pike, Director of Operations
2 January 2015 n/a -permanent 3 months Standard AfC redundancy provision
Local clinicians working with local people for a healthier future Page 39 of 68

Enfield CCG Annual Report 2014/15
Mr Simon East, Interim Chief Finance Officer
11 December 2013 to 26 June 2014
n/a-interim 1 week n/a
Mr Ian Winning, Interim Chief Finance Officer
1 July 2014 to 14 November 2014
n/a-interim 1 week n/a
Dr Mohammad Abedi, Medical Director
1 December 2012 to 31 July 2014
n/a - resigned 1 month None
Other Governing Body Members Ms Rathai Thevananth, Practice Manager Representative
18 February 2015 2 years 10 months
1 month None
Professor Robert Elkeles, Secondary Care Doctor Representative
1 December 2012 8 months 1 month None
Ms Angela Dempsey, Registered Nurse Member
1 February 2013 10 months 1 month None
Lay members Ms Karen Trew, Lay Vice Chair
1 April 2013 12 months 1 month None
Teri Okoro, Lay Member
1 January 2013 9 months 1 month None
*Where job title has changed, the job title is correct as of 31 March 2015
6.6 Termination agreements or exit packages Termination arrangements are applied in accordance with statutory regulations as modified by national NHS conditions of service agreements (specified in Agenda for Change), and the NHS pension scheme. Specific termination arrangements will vary according to age, length of service and salary levels. The Remuneration Committee will agree any severance arrangements.
Local clinicians working with local people for a healthier future Page 40 of 68

Enfield CCG Annual Report 2014/15
6.7 Salaries and Allowances 2014/15
2014-15 Name and Title Salary Taxable Annual Long -term All Pension Total
Benefits Performance Performance Related (rounded Related Related Benefits
(bands of to the Bonuses Bonuses (Bands of (Bands of £5,000) nearest (Bands of (Bands of £2,500) £5000)
£5000) £5000) £000 £000 £000 £000 £000 £000
Executive Directors Mrs Liz Wise - Chief Officer 125 - 130 0 0 0 0 - 2.5 130 - 135
(1) Mr Simon East - Interim Chief Financial Officer 50 - 55 0 0 0 0 50 - 55 (1) Mr Ian Winning - Interim Chief Financial Officer 100 - 105 0 0 0 0 100 - 105
Mr Rob Whiteford - Chief Financial Officer 40 - 45 0 0 0 0 40 - 45 Ms Aimee Fairbairns - Director of Service Quality and Integrated Governance 100 - 105 0 0 0 12.5 - 15 110 - 115
Mr Graham MacDougall - Director of Strategy & Partnerships 90 - 95 0 0 0 15 - 17.5 105 - 110
Ms Jane Pike - Director of Operations 25 - 30 0 0 0 0 25 - 30 Medical Director
(2) Dr Mo Abedi - Medical Director 30 - 35 0 0 0 0 30 - 35 Elected GP Members
(2) Dr Mo Abedi – Chair 50 - 55 0 0 0 0 50 - 55 Dr Alpesh Patel - Chair / Clinical Vice Chair 55 - 60 0 0 0 0 55 - 60 Dr Janet High - Clinical vice chair / GP Member 30 - 35 0 0 0 0 30 - 35 Dr Anshumen Bhagat - GP Member 25 - 30 0 0 0 0 25 - 30 Dr Hardeep Bhupal - GP Member 15 - 20 0 0 0 0 15 - 20 Dr Fahim Chowdhury - GP Member 25 - 30 0 0 0 0 25 - 30 Dr Mike Gocman - GP Member 25 - 30 0 0 0 0 25 - 30 Dr Raj Mazumder - GP Member 5 - 10 0 0 0 0 5 - 10 Dr Pavan Sardana - GP Member 5 - 10 0 0 0 0 5 - 10 Dr Ujjal Sarkar - GP Member 25 - 30 0 0 0 0 25 - 30 Other Governing Body Members Mrs Rathai Thevananth - Practice Manager Member 10 - 15 0 0 0 0 10 - 15 Prof Robert Elkeles - Secondary Care Doctor Member 15 - 20 0 0 0 0 15 - 20 Mrs Angela Dempsey - Nurse Member 15 - 20 0 0 0 0 15 - 20 Lay Members Ms Karen Trew - Lay Member 20 - 25 0 0 0 0 20 - 25 Dr Teri Okoro - Lay Member 10 - 15 0 0 0 0 10 - 15
(1) Paid through agency not direct to individual.
(2) Invoices the CCG direct.
The Chair works six sessions or three days a week. The Clinical Vice Chair works three sessions or one and a half days a week. The elected Governing Body GP Members are contracted for two sessions or one day a week. The Lay Member for Governance and Chair of Audit is contracted for two sessions a week. Other Governing Body members are contracted for one session a week.
Local clinicians working with local people for a healthier future Page 41 of 68

Enfield CCG Annual Report 2014/15
Salaries and Allowances 2013/14
6.8 Payments for Loss of Office No significant awards or payments have been made during the financial year 2014/15.
6.9 Payments to Past Senior Managers No significant awards or payments have been made during the financial year 2014/15.
6.10 Salary and pension entitlements of directors and senior managers The following schedules disclose further information regarding remuneration and pension entitlements.
NAME TITLE Salary Taxable Annual Long -term All Pension TotalBenefits Performance Performance Related
(bands of (rounded Related Bonuses Related Bonuses Benefits£5,000) to the (Bands of (Bands of (Bands of (Bands of
nearest £5000) £5000) £2,500) £5000)£000 £000 £000 £000 £000 £00
VOTING MEMBERS
DirectorsMrs Liz Wise Chief Officer 125 - 130 0 0 0 12.5 - 15 135 - 140Mr Richard Quinton Interim Chief Financial Officer 85 - 90 0 0 0 0 85 - 90
(1) Mr Simon East Interim Chief Financial Officer 50 - 55 0 0 0 0 50 - 55
Ms Aimee Fairbairns Director of Service Quality and Integrated Governance
95 - 100 0 0 0 5.0 - 7.5 100 - 105
Mr Graham MacDougallDirector of Strategy & Partnerships 85 - 90 0 0 0 0 85 - 90
Medical Director(2) Dr Mo Abedi Medical Director 80 - 85 0 0 0 0 80 - 85
Elected GP Members
(a) Dr Alpesh Patel GP Member 80 - 85 0 0 0 0 80 - 85(a) Dr Janet High GP Member 40 - 45 0 0 0 0 40 - 45(a) Dr Anshumen Bhagat GP Member 25 - 30 0 0 0 0 25 - 30(a) Dr Fahim Chowdhury GP Member 10 - 15 0 0 0 0 10 - 15(2) Dr Tim Fenn GP Member 5 - 10 0 0 0 0 5 - 10(a) Dr Mike Gocman GP Member 25 - 30 0 0 0 0 25 - 30
Dr Raj Mazumder GP Member 20 - 25 0 0 0 0 20 - 25(a) Dr Pavan Sardana GP Member 25 - 30 0 0 0 0 25 - 30
Dr Ujjal Sarkar GP Member 25 - 30 0 0 0 0 25 - 30
Other Governing Body Members
Mrs Rathai Thevananth Practice Manager Member 20 - 25 0 0 0 0 20 - 25
Prof Robert Elkeles Secondary Care Doctor Member 10 - 15 0 0 0 0 10 - 15
Mrs Angela Dempsey Nurse Member 10 - 15 0 0 0 0 10 - 15
Lay Members
Ms Karen Trew Lay Member 25 - 30 0 0 0 0 25 - 30Dr Teri Okoro Lay Member 10 - 15 0 0 0 0 10 - 15
(1) Paid through agency not direct to individual.(2) Invoice the CCG direct.
(a) Restated to include employer pension contributions now a requirement in 2014/15
2013-14
Local clinicians working with local people for a healthier future Page 42 of 68

Enfield CCG Annual Report 2014/15
2014/15
2013/14
6.11 Pension Benefits Certain Members do not receive pensionable remuneration therefore there will be no entries in respect of them.
6.12 Pensions All staff, including senior managers, are eligible to join the NHS pensions scheme. The scheme has fixed the employer’s contribution at 14% of the individual’s salary as per the NHS Pension Agency regulations. Employee contribution rates for PCT officers and practice staff, and the prior year comparators, are as follows:
6.13 Member Contribution Rates before tax relief (gross)
Name Title
Real increase
/decrease in pension at age 60 (bands of £2500)
Real increase
/decrease in related lump sum at age 60 (bands of £2500)
Total accrued pension
at age 60 at 31
March 2015
(bands of £5000)
Total accrued related
lump sum at age 60
at 31 March 2015
(bands of £5000)
Cash Equivalent Transfer Value
(CETV) at 31 March
2015
Cash Equivalent Transfer Value
(CETV) at 31 March
2014
Real increase / decrease in Cash
Equivalent Transfer Value
Employers Contribution
to Partnership
Pension
£000 £000 £000 £000 £000 £000 £000 £000
Governing Body MemebersMrs Liz Wise Chief Officer 0 - 2.5 2.5 - 5 25 - 30 80 - 85 632 578 38 18
Ms Aimee FairbairnsDirector of Service Quality and Integrated Governance
0 - 2.5 2.5 - 5 20 - 25 65 - 70 438 394 33 13
Mr Graham MacDougall Director of Strategy & Partnerships 0 - 2.5 2.5 - 5 25 - 30 75 - 80 501 452 37 13
Name Title
Real increase
/decrease in pension at age 60 (bands of £2500)
Real increase
/decrease in related lump sum at age 60 (bands of £2500)
Total accrued pension
at age 60 at 31
March 2014
(bands of £5000)
Total accrued related
lump sum at age 60
at 31 March 2014
(bands of £5000)
Cash Equivalent Transfer Value
(CETV) at 31 March
2014
Cash Equivalent Transfer Value
(CETV) at 31 March
2013
Real increase / decrease in Cash
Equivalent Transfer Value
Employers Contribution
to Partnership
Pension
£000 £000 £000 £000 £000 £000 £000 £000
Governing Body MembersMrs Liz Wise Chief Officer 2.5-5.0 10-12.5 25-30 75-80 578 476 92 0
Ms Aimee FairbairnsDirector of Service Quality and Integrated Governance
0-2.5 5-7.5 20-25 60-65 394 334 53 0
Local clinicians working with local people for a healthier future Page 43 of 68

Enfield CCG Annual Report 2014/15
Scheme benefits are set by the NHS Pensions Agency and are applicable to all members.
Past and present employees are covered by the provisions of the NHS pension scheme. For full details of how pension liabilities are treated please see note 3 in the annual accounts.
6.14 The relationship between the highest paid director and median remuneration Reporting bodies are required to disclose the relationship between the remuneration of the highest-paid director in their organisation and the median remuneration of the organisation’s workforce.
The banded remuneration of the highest paid member of Enfield CCG in the financial year 2014/15 was £ 125k to 130k.
This was 3.14 times the median remuneration of the workforce, which was £ 41k. In 2014/15 No employees received remuneration in excess of the highest paid member of the Enfield Clinical Commissioning Group. Remuneration ranged from £ 2k to £128k.
Total remuneration includes: salary, non-consolidated performance-related pay, and benefits in-kind. It does not include severance payments, employer pension contributions and the cash equivalent transfer value of pensions.
The Hutton review of fair pay in the public sector guidance suggests that all staff, irrespective of any recharges, should be shown as 100% charged to Enfield CCG compared to the highest paid director as only being shown as the element of cost the CCG is charged for that director’s service
6.15 Off-payroll Engagements Following the Review of Tax Arrangements of Public Sector Appointees published by the Chief Secretary to the Treasury on 23 May 2012 clinical commissioning groups must publish information on their highly paid and/or senior off-payroll engagements. Off-payroll engagements as of 31 March 2015, for more than £220 per day and that last longer than six months are shown in the next table.
The number that have existed: Number For less than one year at the time of reporting 6 For between one and two years at the time of reporting 4 For between two and three years at the time of reporting 0 For between three and four years at the time of reporting 0 For four or more years at the time of reporting 0 Total number of existing engagements as of 31 March 2014 10
All existing off-payroll engagements outlined above have, at some point, been subject to a risk based assessment as to whether assurance is required that the individual is paying the right amount of tax and, where necessary, that assurance
Local clinicians working with local people for a healthier future Page 44 of 68

Enfield CCG Annual Report 2014/15
has been sought. All interim staff are paid by the recruitment agency they work through.
Local clinicians working with local people for a healthier future Page 45 of 68

Enfield CCG Annual Report 2014/15
STATEMENTS BY THE ACCOUNTABLE OFFICER
7. Statement of Accountable Officer ’s ResponsibilitiesThe National Health Service Act 2006 (as amended) states that each Clinical Commissioning Group shall have an Accountable Officer and that Officer shall be appointed by the NHS Commissioning Board (NHS England). NHS England has appointed the Chief Officer to be the Accountable Officer of the Clinical Commissioning Group.
The responsibilities of an Accountable Officer, including responsibilities for the propriety and regularity of the public finances for which the Accountable Officer is answerable, for keeping proper accounting records (which disclose with reasonable accuracy at any time the financial position of the Clinical Commissioning Group and enable them to ensure that the accounts comply with the requirements of the Accounts Direction) and for safeguarding the Clinical Commissioning Group’s assets (and hence for taking reasonable steps for the prevention and detection of fraud and other irregularities), are set out in the Clinical Commissioning Group Accountable Officer Appointment Letter.
Under the National Health Service Act 2006 (as amended), NHS England has directed each Clinical Commissioning Group to prepare for each financial year financial statements in the form and on the basis set out in the Accounts Direction. The financial statements are prepared on an accruals basis and must give a true and fair view of the state of affairs of the Clinical Commissioning Group and of its net expenditure, changes in taxpayers’ equity and cash flows for the financial year. In preparing the financial statements, the Accountable Officer is required to comply with the requirements of the Manual for Accounts issued by the Department of Health and in particular to:
• Observe the Accounts Direction issued by NHS England, including therelevant accounting and disclosure requirements, and apply suitableaccounting policies on a consistent basis;
• Make judgements and estimates on a reasonable basis;• State whether applicable accounting standards as set out in the Manual for
Accounts issued by the Department of Health have been followed, anddisclose and explain any material departures in the financial statements; and,
• Prepare the financial statements on a going concern basis.
To the best of my knowledge and belief, I have properly discharged the responsibilities set out in my Clinical Commissioning Group Accountable Officer Appointment Letter.
Liz Wise Accountable Officer 29th May 2015
Local clinicians working with local people for a healthier future Page 46 of 68

Enfield CCG Annual Report 2014/15
8. Governance StatementIntroduction & Context
Enfield CCG was authorised from 1 April 2013 under provisions enacted in the Health and Social Care Act 2012, which amended the National Health Service Act 2006.
The CCG operated in shadow form prior to 1 April 2013, to allow for the completion of the authorisation process and the establishment of function, systems and processes prior to the clinical commission group taking on its full powers.
As at 1 April 2013, the CCG was licensed with conditions.
The seven conditions were:
3.1.1.B – Further information is required to show the targets for the commissioning intentions to achieve end state and the process that will ensure this happens. Clarity is required regarding its priorities, 2013-2014 commissioning intentions and longer term strategic aims.
3.1.1 C – The CCG needs to clearly set out how it will achieve financial balance and manage within its management allowance and other required constraints.
4.2.1B - More evidence is required that patient feedback is being used
systematically as part of the process to identify early quality and safety issues;
and that the Quality Strategy, which does address patient feedback, is
translated into practice.
4.2.1G - Further evidence is required to demonstrate that the risk-sharing arrangements have been agreed with neighbouring CCGs.
4.2.3D - Further evidence of effective child safeguarding arrangements (other than the role and responsibility being mentioned in the Safeguarding Children Structure Chart contained within the policy).
5.1 A – Evidence is required to demonstrate that all CCGs have agreed to the collaboration arrangements.
6.4 G - Further support is needed to ensure that the capacity of the senior leadership team is developed to sufficiently address the CCG's strategic issues,
The legal direction was applied to the condition regarding the CCG’s capacity to maintain strategic oversight over a large and complex public health, service and financial change agenda with available resources. These were lifted in October 2013.
Local clinicians working with local people for a healthier future Page 47 of 68

Enfield CCG Annual Report 2014/15
Scope of Responsibility As Accountable Officer, I have responsibility for maintaining a sound system of internal control that supports the achievement of Enfield CCG’s policies, aims and objectives, whilst safeguarding the public funds and assets for which I am personally responsible, in accordance with the responsibilities assigned to me in Managing Public Money. I also acknowledge my responsibilities as set out in my Clinical Commissioning Group Accountable Officer Appointment Letter.
I am responsible for ensuring that Enfield CCG is administered prudently and economically and that resources are applied efficiently and effectively, safeguarding financial propriety and regularity.
Compliance with the UK Corporate Governance Code The aforementioned Financial Governance Review recommended changes to the Terms of Reference and timing of key committees which the CCG has already actioned.
Whilst compliance with the UK Corporate Governance Code is not mandatory for public sector bodies, Enfield CCG’s Corporate Governance arrangements are set out in its Constitution authorised by NHS England. Our constitution draws upon best practice available, including those aspects of the UK Corporate Governance Code we consider to be relevant to the CCG and best practice. The Constitution includes the organisation’s Standing Orders, Standing Financial Instructions, Schemes of Reservation and Delegation and Codes of Accountability and Conduct. These arrangements have been drawn up in line with Department of Health Guidance.
The Clinical Commissioning Group Governance Framework Enfield CCG was established under the Health and Social Care Act as a statutory body responsible for health services as set out in section 3 of the Act and the regulations made under that provision. Enfield CCG is a clinically led membership organisation made up of local general practices. The members of CCG are responsible for determining the governing arrangements for their organisation, as set out in Enfield CCG’s Constitution.
Governing Body Membership The Chair of Enfield CCG during 2014-2015 was Dr Mo Abedi (from 20 August 2014). Prior to this, Dr Alpesh Patel was the Chair. The Chief Officer is Liz Wise. A list of Governing Body members during 2014/15 can be found on page 27 of this report.
Committees In line with statutory requirements and guidance, the Governing Body established the following Committees:
• Audit Committee
Local clinicians working with local people for a healthier future Page 48 of 68

Enfield CCG Annual Report 2014/15
• Remuneration and Nomination Committee• Quality and Safety Committee• Financial Recovery and Quality, Innovation, Productivity and Prevention
(QIPP) Committee (FR&Q)• Patient and Public Engagement Committee• Procurement Committee (established in 2014/2015)• Executive Committee (established in 2014/2015)
The last two additional committees were established and submitted to NHS England as part of its June 2014 window for constitutional changes. Highlights of the work of all the above committees – “the effectiveness of Governing Body Committees” can be found on page 58 of this report.
A summary of the responsibilities of these committees, their membership and delegated responsibilities can be found in our Constitution
The Terms of Reference of each Committee are available on the CCG website.
The CCG’s Committee accountability is set out below:
The Financial Governance Review This recommended changes to the timing and terms of reference of committees. The FR&Q Committee timing has been changed to allow for the most recent information to be available to it. Terms of reference for the FR&Q Committee have been also been changed to provide greater clarity of purpose.
The Effectiveness of the Governing Body Committees As part of the Audit Committee work plan, all Governing Body Committee Chairs are required to attend the Audit Committee to report on their effectiveness. Committee chairs also formally report to every CCG Governing Body meeting. A meeting self-
Local clinicians working with local people for a healthier future Page 49 of 68

Enfield CCG Annual Report 2014/15
evaluation form is also completed following every Committee meeting to evaluate effectiveness.
In 2014, the CCG Governing approved a set of Key Performance Indicators (KPIs) for monitoring the effectiveness of the Governing Body and its Committees annually. The KPIs were developed using Monitor’s Code of Governance and Intelligent Board guidance together with the Healthcare Financial Management Association (HFMA) Audit Committee Handbook guidance.
The KPIs have been used to produce a questionnaire to be completed by members of the committees annually to ensure their views are obtained with a desktop review of the cycle of business and Terms of Reference of each Committee undertaken by the Board Secretary. An annual report on Committee effectiveness will be presented to the Governing Body which will include the outcome of the effectiveness review, membership of these committees, attendance records and coverage of their work with recommendations as appropriate.
Highlights of Governing Body and its Committees’ reports
Governing Body The Governing Body met six times in public during the financial year. Highlights of the year include:
• Approval of co-commissioning arrangements with NCL CCGs and NHSEngland to deliver Primary Care.
• Closer working and partnership with NCL CCGs around managing providercontracts, procurement of services e.g. NHS 111 and Out of Hours
• Working with NCL colleagues to support acquisition of Barnet and ChaseFarm Hospitals by Royal Free London and subsequently support plans byRFH to redevelop the Chase Farm Site
Other highlights include: • Review of procurement matters including, Musculoskeletal Services and
Community Services• Adult and Children’s Section 75 Agreement• Review of Financial matters including the QIPP and managing the CCG
Financial Recovery Plan• Managing the performance of providers and the increase in activity levels at
providers due to A&E attendances, RTT, Mental Health etc.• Review of Corporate Objectives and the BAF level risks• Reviewed and monitor activity via the Integrated Performance Report• NHSE Quality Assurance
Local clinicians working with local people for a healthier future Page 50 of 68

Enfield CCG Annual Report 2014/15
Audit Committee The committee met seven times during the financial year. The Committee have, in the course of the year, reviewed and responded to the following:
• Scrutiny of the Financial Governance Review and monitoring progress onrecommendations
• The Internal Audit Plan. In addition, all twelve CCGs worked with North EastLondon Commissioning Support Unit to gain assurance on the process of thissignificant outsourcing operation that Enfield CCG (along with the other 11CCGs) relies on.
• The Counter Fraud Plan, which has reviewed CCG’s systems as well assupported by proactive awareness work as part of the agreed Plan
• The External Audit Plan, which has included the review of the Annual Reportand Accounts from which an evaluation of the process and value for moneyreview take place
• Review of the effectiveness of Governing Body Committees• Considered and agreed an anti-fraud and bribery policy• Delegated limits and financial process arrangements, which had been
approved by the Governing Body• The management of service provider contracts with the Commissioning
Support Unit, seeking assurance as to the way these had been monitored andprogressed as well as acknowledging the complexities when several CCGswere party to the contract with the provider
• Developing a policy on procurement• Business continuity and emergency response arrangements• Approval of the Gifts & Hospitality Policy and review of the Gifts & Hospitality
Register• Approval of the Policy for working in conjunction with the pharmaceutical
industry• Review of the Committee’s own Terms of Reference• Evaluation Checklist completed at the end of every meeting
Quality and Safety Committee The Committee met six times during the financial year and assured itself about issues relating to quality and safety in Enfield by means of an Integrated Provider Quality and Performance Report using quality and performance indicators, risk registers, Clinical Quality and Review Groups update report and minutes of sub-groups including the Quality and Risk Sub Group and Clinical Reference Group.
The Committee monitored and provided assurance to the Enfield CCG Governing Body regarding the performance of safeguarding, medicines management and governance. The following areas had been discussed amongst others:
• Monthly quality and performance integrated report• Serious incident trend report• Safeguarding and safety assurance• Quality improvement• CCG quality governance• Committee terms of reference and workplan• Annual Committee Effectiveness review• Evaluation Checklist completed at the end of every meeting
Local clinicians working with local people for a healthier future Page 51 of 68
Enfield CCG Annual Report 2014/15
Financial Recovery and Quality, Innovation, Productivity and Prevention (QIPP) Committee (FR&Q) The Committee met monthly during the year and highlights from the year include:
• Scrutiny of the Financial Governance Review and recommended actions• Completion of an alignment process to ensure leadership and ownership of
finance and Quality, Innovation, Productivity and Prevention plans• Increased focus on underlying recurrent positions of the Enfield CCG• Review of plans for performance management and future reporting
The following areas were discussed amongst others: • The monthly finance report• The key contracting variances• QIPP performance including transformation programme updates• Development of the Financial Recovery Plan• Authorisation of investments• Forward planner• Annual Committee Effectiveness review• Evaluation Checklist completed periodically
Remuneration and Nomination Committee The Committee met seven times during the year. Highlights from the year include:
• Assessing and recommending remuneration mechanisms and rates forGoverning Body members
• Governing Body elections and detailed consideration on the selection andappointment process for a Chair and Governing Body GPs and PracticeManager
• Annual Committee Effectiveness review• Evaluation Checklist completed periodically
Patient and Public Engagement (PPE) Committee The Committee met six times during the year. Highlights from the year include:
• Approval of the Equality Delivery Scheme 2• Patient Participation Group representatives election process agreed and
started• Increase in number of PPGs so that every practice has a PPG• Development of the PPG network• Delivery of Patient and Public Engagement events in 2014/2015• Overview of engagement across the organisation as well as wider NHS &
partner agency engagement and consultation work.• Development of the annual patient and public engagement report• Evaluation Checklist completed periodically
Executive Committee Highlights from the year include:
• Review of locality commissioning• Review of Better Care Fund
Local clinicians working with local people for a healthier future Page 52 of 68

Enfield CCG Annual Report 2014/15
• Consider Mental Health Strategy, Value Based Commissioning, commissioning intentions
• Review of Organisational Development, EPRR • Approval of HR policies • Review CSU Improvement Plan • Review of NHS England Conflicts of Interest Statutory Guidance & CCG
Action Plan • Review of Policy for Working in conjunction with Pharmaceutical Industries
The following areas had been discussed amongst others:
• Monthly Performance Report setting out performance of provider trusts • Reports from Locality Commissioning Business meetings • A review of the Committee’s effectiveness • A review of Corporate Objectives • A review and approval of Constitutional issues • Evaluation Checklist completed periodically
Procurement Committee The committee was established in June 2014 and met six times. Highlights from the year include:
• Assurance of GP Provider Networks • Community Health Services Procurement Strategy • MSK Procurement Strategy • Evaluation Checklist completed periodically • Review of NHS England Conflicts of Interest Statutory Guidance & CCG
Action Plan The Clinical Commissioning Group Risk Management Framework Enfield CCG’s Governing Body approved Risk Management Strategy outlines the organisation’s approach to risk management, including:
• Identifying committees and groups which have responsibility for risk management
• Roles and responsibilities of staff with regards to risk management • The process for identification, assessment and management of including risk
to data security • The process for managing, and Board review of, the Risk Register and Board
Assurance Framework • The risk appetite of the organisation which sets out the thresholds for
tolerating, managing and reporting different orders of risk • The CCG Risk Assessment Framework is based on the National Patient
Safety Agency (NPSA) guidance and the Australia/New Zealand standard AZ/NZS 4360:1999. This provides guidance on identifying, evaluating and controlling risks. This is a generic method applied in many contexts to assess risks in a consistent manner.
Local clinicians working with local people for a healthier future Page 53 of 68

Enfield CCG Annual Report 2014/15
Risk Identification Methods for identifying risk in the CCG include:
• Internal methods such as: quality impact assessments, quality alerts,information governance breaches, equality impact assessments, incidents,complaints, claims and serious incident reporting and identification of trends,audits, quality, innovation, productivity and prevention (QIPP) related risks,project risks based on the achievement of project objectives, patientsatisfaction surveys, risk assessments, surveys including staff surveys,whistle-blowing. Contract quality monitoring of commissioned services.
• Risks are also identified through GP locality meetings, patient engagementforums, practice feedback forms and practice managers’ meetings.
• External methods include media, national reports, new legislation, and reportsfrom assessments and inspections by external bodies and reviews ofpartnership working.
Risk Evaluation • As part of Enfield CCG’s risk management process, all risks identified are
evaluated and given a risk level rating. The higher the risk level, the greater the likelihood an opportunity or threat will occur and the greater its consequence.
• An acceptable risk may be defined as a potential hazard that is either smallenough to have an immaterial effect on the achievement of organisational objectives, or is a significant risk that has been mitigated by the establishment of effective controls to minimise the likelihood of the risk occurring, or to minimise the adverse consequences should the risk identified occur.
Management of current risks All CCG risks are managed via the Datix risk management system. Datix captures risks at all levels within the organisation from operational (directorate) to strategic level as well as project risks. These risks are be prioritised in accordance with the CCG’s Risk Management Strategy, thereby enabling its principal risks to be fed upwards onto the Assurance Framework.
The key objectives of the Datix database are to: • Develop and use an agreed coding structure to satisfy the current and
anticipated needs of the CCG and, as much as possible, to make risk gradingeasily understood by relevant managers and directors without compromisingthe CCG’s Risk Management Strategy.
• Make use of Datix system-wide codes for Risk Register (including theAssurance Framework), project and programme risk register to enable easiersharing of information and risks across different directorates and services.
• Maximise the potential benefit of having an integrated risk managementdatabase within the CCG by ensuring that a standard set of reports areaccessible across the CCG for its relevant committees and for the GoverningBody meetings.
Local clinicians working with local people for a healthier future Page 54 of 68

Enfield CCG Annual Report 2014/15
• Centralise storage of related documents and information (assurance records)onto Datix Risk Register through the use of document templates, file uploads,attached documents from the internal drives.
Reporting and Monitoring of Current Risks All risks are linked to the CCG’s strategic objectives and assigned a risk owner (i.e. lead director), and a lead committee which has oversight for the management and mitigation of the risk.
To enable successful risk management and assurance reporting and ensure that risk is embedded within the CCG, a monitoring and reporting structure has been established for both strategic and operational risk as set out below.
The Governing Body Assurance Framework and Corporate Risk Register The CCG operates a Governing Body Assurance Framework and Corporate Risk Register. The Governing Body Assurance Framework and Corporate Risk Register assess the effectiveness of systems of internal control and provide assurances that risk management processes are effective. Both are dynamic documents that capture the understanding of the risk environment at any given time.
The Governing Body Assurance Framework outlines the CCG’s principal objectives, the significant risks (12+) to achieving those objectives, key controls and assurances, and gaps in controls and assurances. The Corporate Risk Register contains a mixture of strategic and operational risks (8+) at organisational and directorate level as well as the arrangements in place to mitigate these.
The Assurance Framework is reported at every Governing Body Meeting. The Finance Recovery & QIPP Committee and Quality and Safety Committee review the Corporate Risk Register no less than four times a year and escalate significant risks to the Assurance Framework as appropriate. The Audit Committee scrutinises the Assurance Framework and Corporate Risk Register at every meeting. As part of the Audit Committee work plan, Directors also attend the Audit Committee on a rotational basis to present their risk and provide assurance on their mitigation and control measures.
The above process ensures that the highest risks appear on the Governing Body Assurance Framework with a systematic approach to lower risks. The process ensures where risks are identified, there is a requirement for action to be taken to mitigate the risk. Where risks remain at a high level, they are subject to regular scrutiny by the Governing Body relevant Committee so that they receive constant management attention.
Local clinicians working with local people for a healthier future Page 55 of 68

Enfield CCG Annual Report 2014/15
The Clinical Commissioning Group Internal Control Framework The system of internal control is designed to manage risk to a reasonable level rather than to eliminate all risk of failure to achieve policies, aims and objectives; it can therefore only provide reasonable and not absolute assurance of effectiveness. The system of internal control is based on an on-going process designed to identify and prioritise the risks to the achievement of the policies, aims and objectives of the clinical commissioning group, to evaluate the likelihood of those risks being realised and the impact should they be realised, and to manage them efficiently, effectively and economically. The system of internal control has been in place in the clinical commissioning group for the year ended 31 March 2015 and up to the date of approval of the Annual Report & Accounts.
Committee structures, Terms of Reference and timing were the subject of recommendations in the Financial Governance Review. The CCG has already implemented many of these and all recommendations will be implemented by 30 September 2015.
Information Governance The management of current risk section explains how all risks including risk to data security are being managed and controlled.
Enfield CCG’s Information Governance Framework sets the processes and procedures by which we handle information about patients and employees, in particular personal identifiable information. Our Information Governance Framework and associated policies is supported by an information governance toolkit and the annual submission process provides assurances to the Governing Body, other organisations and to the public that personal information is dealt with legally, securely, efficiently and effectively.
We place high importance on ensuring there are robust information governance systems and processes in place to help protect patient and corporate information. All staff have undertaken annual information governance training to ensure they are aware of their information governance roles and responsibilities. We have submitted a satisfactory level of compliance with the 2014/2015 information governance toolkit assessment. As part of the information governance toolkit, we have undertaken data flow mapping, information risk assessment and management procedures. There are processes in place for incident reporting and investigation of serious incidents. We have developed an information risk assessment and management procedures and a programme has been established to fully embed an information risk culture throughout the organisation.
Local clinicians working with local people for a healthier future Page 56 of 68

Enfield CCG Annual Report 2014/15
Risk Assessment in Relation to Governance, Risk Management & Internal Control
Risk Assessment All identified risks are assessed using a clearly defined risk assessment matrix by determining the likelihood and consequence of the risk to calculate an overall risk rating. Risks are categorised as low, moderate, high or extreme (see risk appetite section) using a widely used NHS Risk Scoring Tool and their categorisation informs the organisation’s approach to management and monitoring of the risk
Enfield CCG’s Risk Appetite Risk appetite is a threshold – the amount of risk that an organisation is prepared to accept before it takes action.
In 2014-15, following feedback from the Audit Committee, the Board Assurance Framework (BAF) and Risk Register was overhauled with the support of the Baker Tilly. The Audit Committee recommended a moderation exercise on the number of extreme risks scores to ensure that the BAF reflects the key strategic risk facing the CCG. The Committee also felt there was a significant amount of operational risks on the BAF which required review. The CCG Executive Committee considered the Audit Committee recommendations and agreed an amendment to the Risk Management Strategy so that the BAF reflects not just strategic extreme risk graded 15 and above but strategic high risks graded 12+.
In 2014/2015, two Governing Body risk workshops were facilitated by Baker Tilly on risk management as well as a deep dive into existing risks on the BAF. The second session involved a review of our 2015/2016 objectives and associated high level strategic risks. As part of this work, the existing risks on the Enfield CCG Board Assurance Framework were reviewed and either refreshed or closed down as appropriate. Updated risks, along with any newly-identified risks, were then migrated or aligned to a new and more easily digestible template to reflect feedback from the Governing Body and staff.
The risk appetite for Enfield CCG is defined below:
Risk Score Actions Taken Amber/Red risks
High/Extreme (Score 12-25): Immediate action to reduce the risk with review within a month
The Chief Officer and the Executive Directors should be informed immediately. The consequences of such risks materialising could seriously impact on the CCG and threaten the achievement of its key objectives. A comprehensive risk assessment should be carried out with a clear action plan with prescribed timescales agreed by the Executive Committee.
Amber risks High Level (8-10): prompt action required
A risk with a ‘High Level’ scoring should be discussed at the relevant committee below)
Local clinicians working with local people for a healthier future Page 57 of 68

Enfield CCG Annual Report 2014/15
to reduce the risk within 1 to 3 months.
with clear scrutiny on mitigation.
Yellow risks Moderate risk (4-6): requires action to reduce and monitor the risk within 3 to 6 months.
Close monitoring of all ‘Yellow- Moderate risks’ should be undertaken by the relevant sub-committees of the board so that assurance can be provided that these risks are being managed comprehensively at local and operational level. It is the responsibility of relevant managers to ensure that the risk register is kept up-to-date with relevant actions in order to monitor and mitigate all moderate risks.
Green risks Low risk (1-3): These are acceptable risks which can be tolerated with sometimes little action to reduce the risk to as low as reasonably practicable within 12 months.
It should be realistically possible to reduce these risks within a reasonable timescale through reasonably practicable measures to mitigate them, such as staff training, purchase of equipment, minor department restructuring.
Risk Profile
2014-2015 has been challenging in meeting in-year delivery targets and meeting our statutory financial obligations. In that context, the most significant and enduring risks for 2014-2015 are described below.
Identified significant risks (15+) during the financial year and after the year end
Risk Mitigation or closure Risk that the CCG will not meet planned financial position for the year 2014/15
The CCG overshot its control total by £13.3m
Risk that CCG will not remain within its control total for 2015/16
-Improved Contract Negotiation -Investment Review -External assistance to build a robust recovery plan -Appointment of a Recovery Director -Implementation of the Financial Governance Review recommendations
Risk of inadequate QIPP Schemes to meet CCG's QIPP Plan
QIPP of £10.6m was achieved in 2014/15. The establishment of a Financial Recovery Group delivered £5m of savings in year.
Risk of Acute overspend: 2014/15 contracts are being negotiated as payment by result (PbR) contracts and therefore there is a risk
Acute contracts overspent by £10.4m. The majority of this was on non-elective activity at Barnet and Chase Farm Hospitals. We
Local clinicians working with local people for a healthier future Page 58 of 68

Enfield CCG Annual Report 2014/15
of over performance. will review the causes of this in 2015/16
Data quality risk to the CCG ‘s ability to report accurately and decision making including availability of RTT information
-Performance management of contracts and data quality indicators -Monitoring at FR&Q -Performance management process established focusing on Data Quality --Monitoring at NCL wide CSU Improvement Group -RTT reporting improvements
Risk of system failure in terms of A&E targets and RTT
-Increased capacity for 7 day working across the organisation and enablement wards. -Enfield participate in 2 System Resilience Groups ("SRGs") 1 centred around the Royal Free hosted by Barnet and one centred around the North Middlesex -Clear KPIs and dashboard in place to monitor additional schemes through winter. -Operational groups in place under each SRG monitoring implementation of winter schemes (meeting monthly, increasing according to need)
Review of Economy, Efficiency & Effectiveness of the Use of Resources Monthly finance reports are produced and are a standing item at the CCG’s Finance, Recovery & QIPP Committee meetings. A regular finance report is also a standing item at each CCG Governing Body meeting. The CCG is required to submit monthly financial returns to NHS England which form part of the regular Assurance Meetings between NHS England and the CCG. The CCG has contracts in place for both internal audit and the Local Counter Fraud Service (LCFS) with Baker Tilly.
The work plan for each of these contracts includes coverage of key areas of risk for the CCG. Updates from internal audit and LCFS are standing items on the Audit Committee agenda. In addition, Baker Tilly provides assurance to the Audit Committee as a result of internal audit work undertaken with the NELCSU.
The CCG has developed an Integrated Quality & Performance Report (IQPR) in collaboration with CSU colleagues during 2014-15. The IQPR provides an overarching picture of the performance of the CCG and its main providers in relation to finance, key performance indicators (KPIs) and quality metrics. The report, which is reviewed on a monthly basis by the Finance, Recovery & QIPP Committee, highlights any significant areas of concern and actions being taken to address them. The IQPR is also a standing agenda item at the Governing Body meetings.
Local clinicians working with local people for a healthier future Page 59 of 68

Enfield CCG Annual Report 2014/15
Review of the Effectiveness of Governance, Risk Management & Internal Control As Accountable Officer I have responsibility for reviewing the effectiveness of the system of internal control within Enfield CCG.
Enfield CCG has a number of key processes in place to ensure that resources are used economically, efficiently and effectively. These include a Transformation Programme Group, the Finance, Recovery and QIPP Committee and the Audit Committee. Please see the terms of reference for a full description of the roles of Committees.
Capacity to Handle Risk - Directors, Clinical Leads and Head of Services
All risks are assigned a relevant Executive Director, Clinical Lead and Head of Service who has accountability for overseeing the management of the risk by identifying the most effective means to minimise, transfer or remove it, and ensuring the quality of action plans, controls and assurances. A lead officer is also assigned with management responsibility for delivering the action plan, developing robust controls and identifying sources of assurance.
The Assistant Director of Quality, Governance & Risk and Risk Manager provide professional support and training to staff on the risk management process.
Departmental Risk Champions Each CCG department has a trained Risk Champion who:
• Proactively engages in the implementation of the monthly risk register reviewand update within their directorate.
• Work with Service Leads to ensure risk registers are quality checked withinthe time frames set out in the risk management strategy
• Input risk register information on to the Risk Module of the Datix database inan accurate and timely manner so that the Risk & Governance Team are able to supply the Executive Committee, Audit Committee, Finance & Recovery Committee, Quality & Risk Sub Group and other bodies with accurate and up to date Corporate Risk Registers and Assurance Framework.
• Keep up to date with any changes to the database by attending refreshertraining as and when appropriate.
• Report any concerns to their Director and advice directors, managers andother staff within their directorate of identified risks requiring attention
Staff training and support • A system of trained risk champions has been established in each directorate
responsible for ensuring their department risk registers are managed and updated.
• A list of named departmental risk champions and risk owners has beenshared with staff. Risk owners are members of the Executive Team and are accountable for the identification, assessment and management/ mitigation of all risks in their area.
Local clinicians working with local people for a healthier future Page 60 of 68

Enfield CCG Annual Report 2014/15
• To ensure the successful implementation and maintenance of this RiskManagement
• Strategy, committee members and staff have access to appropriate advice,guidance,
• Information and training in order to carry out their respective responsibilitiesfor risk control and risk assessment.
• All staff receive mandatory training annually in health, fire & safety, includingrisk assessment and management, via the CCG’s corporate learning anddevelopment programme.
• General awareness raising for staff is also undertaken through staff briefings,induction programmes and inclusion of relevant documents on the intranet.
• The Risk Management Strategy and guidance is accessible to all CCG staffvia the CCG intranet.
Review of Effectiveness My review of the effectiveness of the system of internal control is informed by the work of the internal auditors and the executive managers and clinical leads within the clinical commissioning group who have responsibility for the development and maintenance of the internal control framework. I have drawn on performance information available to me. My review is also informed by comments made by the external auditors in their management letter and other reports.
The Board Assurance Framework itself provides me with evidence that the effectiveness of controls that manage risks to the CCG achieving its principles objectives have been reviewed.
I have been advised on the implications of the result of my review of the effectiveness of the system of internal control by the Governing Body, the Audit Committee and Quality and Safety Committee and a plan to address weaknesses and ensure continuous improvement of the system is in place. The process that has been applied in maintaining and reviewing the effectiveness of the system of internal control, includes: a full internal audit programme.
Head of Internal Audit Opinion The purpose of my annual Head of Internal Audit Opinion is to contribute to the assurances available to the Accounting Officer and the Board which underpin the Board’s own assessment of the effectiveness of the organisation’s system of internal control. This Opinion will in turn assist the Board in the completion of its Annual Governance Statement.
The Head of Internal Audit Opinion, based on work undertaken up to 11th March 2015, is set out as follows:
“Based on the work undertaken in 2014/15, significant assurance can be given that there is a generally sound system of internal control, designed to meet the organisation’s objectives, and that controls are generally being applied consistently. However, some weaknesses have been identified.
Local clinicians working with local people for a healthier future Page 61 of 68

Enfield CCG Annual Report 2014/15
The month 9 cumulative results were showing a deficit of £13.5m against a planned deficit of £4.5m, £9.0m over target. The CCG is forecasting a deficit of £19.0m for the year, £13.4m in excess of the control total. The major factor was a worsening position on the acute contract over-performance exacerbated by the move to primarily payments by results contracts as opposed to block contracts as in 2013/14 The CCG has had external support in reviewing the financial out-turn. We are planning to audit progress on the recommendations from the Financial Governance review early in the 2015/16 financial year.
The CCG has had external support from Deloitte in reviewing the financial out-turn. We are planning to deliver a detailed Financial Governance review early in the 2015/16 financial year.
We also identified one review where we could only provide some assurance. We issued an Amber RED opinion for the Procurement review. Key issues from the review were as follows: - An absence of documentation to support some of the procurement activity undertaken by the CCG. - The CCG currently does not have in place robust guidelines to ensure that clinical expertise and other key stakeholder engagement is sought in the development of any service specifications. An Action plan has been agreed for this area and we will track the progress of implementation and report back to the Audit Committee. Internal Audit has been able to deliver substantial or reasonable assurance in all other areas reviewed
Internal Audit has been able to deliver substantial or reasonable assurance in all other areas reviewed.”
Data Quality The North East London Commissioning Support Unit provides a business intelligence service to the Clinical Commissioning Group which supports the management of contract and other data and the production of performance information. This service includes data validation and contract challenges which are then reflected in the reported positions. Data quality risk has been highlighted in the risk section of this report.
Business Critical Models The key business critical models on which the Governing Body relies are in-year financial forecasts, medium term financial planning and financial evaluation and forecasting. These models are the responsibility of the Chief Finance Officer and operated by the Finance and Contracts Team and the Programme Management Office. Operation of these models is delegated from the Governing Body to the Finance, Recovery & QIPP Committee. Quality assurance on these models has
Local clinicians working with local people for a healthier future Page 62 of 68

Enfield CCG Annual Report 2014/15
been sought, and received, by expert external review and the internal audit programme.
The supplier of our ICT and Business Intelligence functions is the NELCSU. Business critical models in use within ICT are subject to a number of quality assurance processes which link into the overall framework and management commitment to quality. There is transparency and management oversight over models and data sources used to make business critical and strategic decisions, with scrutiny within the Executive committee. Data inputs and outputs are regularly validated, with senior management responsible for an overall ‘sense check’ before decisions are approved.
Business critical models in use within Business Intelligence include processes which support the identification and maintenance of a list of all business critical models and a schedule for periodic review. These processes are subject to review by internal audit, who review management information data and process owners, and external audit whose work covers the quality assurance processes of financial models.
Data Security Please see the information governance section of this report for our Information Governance Toolkit submission.
There were no serious incidents relating to data security breaches in 2014-2015.
Discharge of Statutory Functions
During establishment, the arrangements put in place by the clinical commissioning group and explained within the Constitution were developed with extensive expert external legal input, to ensure compliance with the all relevant legislation. That legal advice also informed the matters reserved for the Membership Body, Governing Body decision and the scheme of delegation. Enfield CCG has robust arrangements in place for the discharge of its statutory duties as outlined in its constitution.
In light of the Harris Review, the CCG has reviewed all of the statutory duties and powers conferred on it by the National Health Service Act 2006 (as amended) and other associated legislative and regulations. As a result, I can confirm that the clinical commissioning group is clear about the legislative requirements associated with each of the statutory functions for which it is responsible, including any restrictions on delegation of those functions. Responsibility for each duty and power has been clearly allocated to a lead Director.
Enfield CCG’s Financial Position
Enfield CCG failed to achieve its statutory duty in regard to financial performance in 2014/15.
Local clinicians working with local people for a healthier future Page 63 of 68

Enfield CCG Annual Report 2014/15
The CCG planned for £5.6m deficit in financial year 2014-15. After a thorough external review involving objective opinion the CCG indicated a likely deficit of £19.0m at the end of the financial year and subsequently recorded a deficit of £18.9m. This was caused by increased activity in both emergency and planned care under Payment by Results contracts. Enfield CCG is currently finalising a recovery plan with the aim of returning to financial balance as soon as possible.
Robust measures are in place to support financial recovery and governance arrangements including:
• Monthly Finance Committee receiving improved and comprehensiveinformation
• Monthly Transformation Programme Group (TPG) to oversee development ofthe three year Transformation Programme as well as in between fortnightlymeetings focusing on performance.
• The appointment of a Recovery Director reporting directly to the Chief Officer• Implementation of the recommendations included in the Financial Governance
Review
Significant Control Issues The external auditors are likely to issue a report under section 19 of the Audit Commission Act 2013 to Secretary of State for Health. This is because the CCG is setting a deficit plan for 2015/16.
Conclusion With the exception of the above issue no significant internal control issues have been identified.
Liz Wise
Accountable Officer
29th May 2015
Local clinicians working with local people for a healthier future Page 64 of 68

Enfield CCG Annual Report 2014/15
ANNUAL ACCOUNTS
9. Introduction: Financial Review of the year and forwardlook
Background Enfield is a financially challenged CCG that was under its “fair shares” allocation by £33m in 2013/14 and £24m in 2014/15. It is forecast to be £16.4m under in 2015/16. Whilst the CCG broke even in 2013/14, this was after receiving £6.3m on a one off basis through the North Central London Risk Share arrangements.
Financial Performance 2014/15 In 2014/15, a planned deficit budget of £5.6m was agreed with NHS England, reflecting a number of pressures including a specialist commissioning adjustment originating late in 2013/14. Due to the increased pressures in 2014/15 the CCG acknowledged it would not achieve its original control total, and in Month 11 the CCG amended its forecast to a deficit of £19.0m. The annual accounts show a deficit of £18.9m.
Enfield CCG spend versus budget Budget Actual Variance
2014/2015 £'000 £'000 £'000
Revenue Resource Limit -349,344 -349,344 0
Acute & Integrated Care 214,564 225,013 10,448
Mental Health 41,265 43,323 2,058
Community Services 21,368 22,225 858
Primary Care - Prescribing 37,857 38,579 722
Primary Care - Other 3,841 3,349 -492
Continuing Care 15,958 17,591 1,633
Learning Disabilities 2,375 2,552 177
Other 6,195 3,884 -2,311
Strategic Investments 3,778 4,279 501
CCG Running Cost 7,742 7,420 -323
Total Expenditure 354,944 368,215 13,271
Unadjusted Deficit 5,600 18,871 13,271
A recently commissioned benchmarking review demonstrated that CCG acute activity and costs were closely aligned to our peer group. It did however highlight several areas on which we will focus in targeting future savings.
• Acute activity rose significantly in 2014/15, including a headline 20% on NonElective Admissions
• GP Referral rates increased by c12% in the same time period, causing anincrease in first outpatient appointments.
Local clinicians working with local people for a healthier future Page 65 of 68

Enfield CCG Annual Report 2014/15
• Day case and Inpatient electives rose by 8.5% in 2014/15, which was largelyattributable to addressing one off waiting list reductions.
• The 2014/15 QIPP programme did not deliver savings to the level expectedfrom service redesign, which has not generally led to reductions in acuteactivity. The total QIPP programme savings were £10.6m of which half aretransactional and non-recurrent. The QIPP target is £12.0m and hasunderachieved by £1.4m.
The CCG has undertaken a review of PMO and QIPP structures, processes and documentation to support improved delivery. The CCG also jointly commissioned a Financial Governance Review with NHS England.
In summary the Report recommended that a full risk assessment should be performed as part of our 2015/16 planning, including quantification of risks presented to the appropriate committees. This has been implemented.
The CCG has already implemented many of the other practical measures recommended by the review. We will implement all of the recommendations by the 30th September 2015.
Finally the report recommended that the CCG produce a Recovery Plan and agree it with NHS England. At the time of writing this Recovery Plan, which covers a five year period, is being finalised. It will then be taken to our Governing Body for scrutiny and approval.
Local clinicians working with local people for a healthier future Page 66 of 68

Enfield CCG Annual Report 2014/15
Financial Plan 2015/16 Enfield CCG forecast an in-year deficit of £14.4m in 2015/16. This plan is a realistic view of risk and opportunity. However there is a risk that the CCG will fail to achieve the £12.5m QIPP savings target and that our Payment by Results (PbR) acute contracts will overspend our budgets.
Enfield CCG planned spend Budget
2015/2016 £'000
Revenue Resource Limit -373,590
2014/15 Deficit Brought Forward 18,871
Acute 225,251
Mental Health 42,397
Community 23,681
Continuing Care 31,941
Primary Care 42,737
Other Programme 13,320
Running Costs 7,019
Contingency 1,774
Total Expenditure 388,119
Unadjusted Cumulative Deficit 33,400
As a result, the CCG have commissioned external help to provide support in building and implementing a robust recovery plan. The terms of reference for this work were signed off jointly with NHS England. Whilst the remit covered contracting, monitoring and reporting the main focus is on helping to build a credible and implementable QIPP programme for 2015/16.
Local clinicians working with local people for a healthier future Page 67 of 68

Enfield CCG Annual Report 2014/15
10. Annual Accounts
Local clinicians working with local people for a healthier future Page 68 of 68

Data entered below will be used throughout the workbook:
Entity name: NHS ENFIELD CLINICAL COMMISSIONING GROUPThis year 2014-15This year ended 31 March 2015This year commencing: 1 April 2014

NHS ENFIELD CLINICAL COMMISSIONING GROUP - Annual Accounts 2014-15
Page Number
The Primary Statements:
Statement of Comprehensive Net Expenditure for the year ended 31st March 2015 1Statement of Financial Position as at 31st March 2015 2Statement of Changes in Taxpayers' Equity for the year ended 31st March 2015 3Statement of Cash Flows for the year ended 31st March 2015 4
Notes to the AccountsAccounting policies 5Other operating revenue 9Revenue 10Employee benefits and staff numbers 11Operating expenses 14Better payment practice code 14Operating leases 15Trade and other receivables 15Cash and cash equivalents 16Trade and other payables 16Provisions 16Contingencies 16Financial instruments 18Pooled budgets 19Intra-government and other balances 19Related party transactions 20Events after the end of the reporting period 23Losses and special payments 23Financial performance targets 23
CONTENTS

1
NHS ENFIELD CLINICAL COMMISSIONING GROUP - Annual Accounts 2014-15
Statement of Comprehensive Net Expenditure for the year ended31 March 2015
2014-15 2013-14Note £000 £000
Total Income and ExpenditureEmployee benefits 3.1.1 6,721 6,198Operating Expenses 4.2 363,897 361,148Other operating revenue 2 (2,403) (3,494)Net operating expenditure before interest 368,215 363,852
Of which:Administration Income and ExpenditureEmployee benefits 3.1.1 3,656 2,626Operating Expenses 4.2 4,230 5,209Other operating revenue 2 (467) (286)Net administration costs before interest 7,420 7,549
Programme Income and ExpenditureEmployee benefits 3.1.1 3,065 3,572Operating Expenses 4.2 359,667 355,939Other operating revenue 2 (1,936) (3,208)Net programme expenditure before interest 360,796 356,303
The notes on pages 5 to 23 form part of this statement
Programme expenditure relates to the commissioning of healthcare and administration relates to the CCG's own running costs.

2
NHS ENFIELD CLINICAL COMMISSIONING GROUP - Annual Accounts 2014-15
Statement of Financial Position as at31 March 2015
31 March 2015
31 March 2014
Note £000 £000
Current assets:
Trade and other receivables 7 3,203 3,906Cash and cash equivalents 8 32 154Total current assets 3,235 4,060Total assets 3,235 4,060
Current liabilitiesTrade and other payables 9 (38,746) (32,411)Total current liabilities (38,746) (32,411)
Total Assets less Current Liabilities (35,511) (28,351)
Total Assets Employed (35,511) (28,351)
Financed by Taxpayers’ EquityGeneral fund SOCITE (35,511) (28,351)Total taxpayers' equity: (35,511) (28,351)
The notes on pages 5 to 23 form part of this statement
Robert WhitefordChief Finance OfficerNHS Enfield CCG
The financial statements on pages 1 to 23 were approved by the Audit Committee on behalf of the Governing Body on 27/05/2015 and signed on its behalf by:

3
NHS ENFIELD CLINICAL COMMISSIONING GROUP - Annual Accounts 2014-15
Statement of Changes In Taxpayers Equity for the year ended31 March 2015
General fund Total reserves£000 £000
Changes in taxpayers’ equity for 2014-15
Balance at 1 April 2014 (28,351) (28,351)Net operating expenditure for the financial year SOCNE (368,215) (368,215)
Net Recognised NHS Clinical Commissioning Group Expenditure for the Financial Year (368,215) (368,215)
Net funding 361,055 361,055
Balance at 31 March 2015 (35,511) (35,511)
General fund Total reserves£000 £000
Changes in taxpayers’ equity for 2013-14
Balance at 1 April 2013 0 0Net operating costs for the financial year (363,852) (363,852)Net Recognised NHS Clinical Commissioning Group Expenditure for the Financial Year (363,852) (363,852)Net funding 335,502 335,502
Balance at 31 March 2014 (28,351) (28,351)
Financial Performance:
During 2014/15 NHS Enfield CCG received RRL funds of £349,344,000 (£364,202,000 2013/14) and incurred expenditure of £368,215,000 (£363,852,000 2013/14). This resulted in a deficit for the year of £18,871,000 (£350,000 surplus 2013/14).
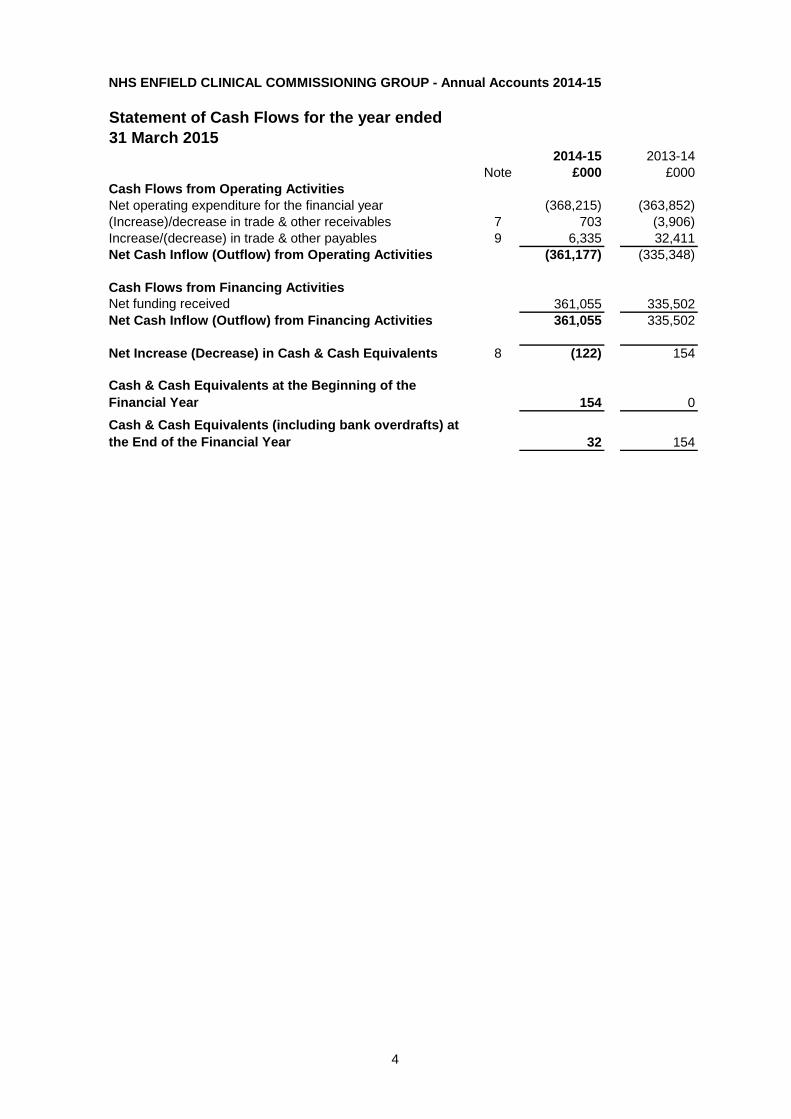
4
NHS ENFIELD CLINICAL COMMISSIONING GROUP - Annual Accounts 2014-15
Statement of Cash Flows for the year ended31 March 2015
2014-15 2013-14Note £000 £000
Cash Flows from Operating ActivitiesNet operating expenditure for the financial year (368,215) (363,852)(Increase)/decrease in trade & other receivables 7 703 (3,906)Increase/(decrease) in trade & other payables 9 6,335 32,411Net Cash Inflow (Outflow) from Operating Activities (361,177) (335,348)
Cash Flows from Financing ActivitiesNet funding received 361,055 335,502Net Cash Inflow (Outflow) from Financing Activities 361,055 335,502
Net Increase (Decrease) in Cash & Cash Equivalents 8 (122) 154
Cash & Cash Equivalents at the Beginning of the Financial Year 154 0
Cash & Cash Equivalents (including bank overdrafts) at the End of the Financial Year 32 154

5
NHS ENFIELD CLINICAL COMMISSIONING GROUP - Annual Accounts 2014-15
Notes to the financial statements
1 Accounting Policies
NHS England has directed that the financial statements of clinical commissioning groups shall meet the accounting requirements of the Manual for Accounts issued by the Department of Health. Consequently, the following financial statements have been prepared in accordance with the Manual for Accounts 2014-15 issued by the Department of Health. The accounting policies contained in the Manual for Accounts follow International Financial Reporting Standards to the extent that they are meaningful and appropriate to clinical commissioning groups, as determined by HM Treasury, which is advised by the Financial Reporting Advisory Board. Where the Manual for Accounts permits a choice of accounting policy, the accounting policy which is judged to be most appropriate to the particular circumstances of the clinical commissioning group for the purpose of giving a true and fair view has been selected. The particular policies adopted by the clinical commissioning group are described below. They have been applied consistently in dealing with items considered material in relation to the accounts.
1.1 Going ConcernThese accounts have been prepared on the going concern basis.IAS 1: Presentation of Financial Statements requires management to assess, as part of the Annual Accounts preparation process, the CCG’s ability to continue as a going concern. These accounts have been prepared on the going concern basis. Public sector bodies are assumed to be going concerns where the continuation of a service in the future is anticipated, as evidenced by inclusion of financial provision for that service in published accounts.The Department of Health Manual of Accounts 2014-15 outlines the following interpretations of Going Concern for the public sector in Section 4.13: ‘For non-trading entities in the public sector, the anticipated continuation of the provision of a service in the future, as evidenced by inclusion of financial provision of that service in published documents, is normally sufficient evidence of going concern.’
The CCG commenced with a planned deficit of £5.6m in 2014-15 and is implementing a medium term financial recovery plan to comply with statutory duties. The CCG failed to achieve its statutory duty to break-even in 2014-15 and requires a qualified audit regularity opinion to the Secretary of State. 1
The following is clear evidence that meets the requirement above in section 4.13 of the DH Manual of Accounts:
· Enfield CCG was established on 1st April 2013 as a separate statutory body;
· Enfield CCG has an agreed constitution and is operating to its constitution to govern its activities;
· Enfield CCG has been allocated funds from NHS England for the financial years 2014/15, 2015/16, 2016/17, 2017/18, 2018/19 and 2019/20;
· Enfield CCG has a 5 year financial plan from 2015/16 to 2018/19 which has been submitted to the Governing Body and NHS England.
As a result of the above evidence Enfield CCG is being treated as a Going Concern.
1As well as an opinion on the accounts, our auditors are required to give a regularity opinion on whether expenditure has been incurred 'as intended by Parliament'. Failure to meet statutory financial targets automatically results in a qualified regularity opinion.Public sector bodies are assumed to be going concerns where the continuation of the provision of a service in the future is anticipated, as evidenced by inclusion of financial provision for that service in published documents.
Where a CCG ceases to exist, it considers whether or not its services will continue to be provided (using the same assets, by another public sector entity) in determining whether to use the concept of going concern for the final set of Financial Statements. If services will continue to be provided the financial statements are prepared on the going concern basis.
1.2 Accounting ConventionThese accounts have been prepared under the historical cost convention modified to account for the revaluation of property, plant and equipment, intangible assets, inventories and certain financial assets and financial liabilities.
1.3 Acquisitions & Discontinued Operations
Activities are considered to be ‘acquired’ only if they are taken on from outside the public sector. Activities are considered to be ‘discontinued’ only if they cease entirely. They are not considered to be ‘discontinued’ if they transfer from one public sector body to another.
1.4 Movement of Assets within the Department of Health Group
Transfers as part of reorganisation fall to be accounted for by use of absorption accounting in line with the Government Financial Reporting Manual, issued by HM Treasury. The Government Financial Reporting Manual does not require retrospective adoption, so prior year transactions (which have been accounted for under merger accounting) have not been restated. Absorption accounting requires that entities account for their transactions in the period in which they took place, with no restatement of performance required when functions transfer within the public sector. Where assets and liabilities transfer, the gain or loss resulting is recognised in the Statement of Comprehensive Net Expenditure, and is disclosed separately from operating costs.Other transfers of assets and liabilities within the Department of Health Group are accounted for in line with IAS 20 and similarly give rise to income and expenditure entries.
1.5 Pooled budgets & risk share
Where a CCG has entered into a pooled budget arrangement under Section 75 of the National Health Service Act 2006 the CCG accounts for its share of the assets, liabilities, income and expenditure arising from the activities of the pooled budget, identified in accordance with the pooled budget agreement.The Section 75 partnership arrangements in the National Health Service Act 2006 have been developed to give NHS bodies and local authorities the ability to respond effectively to improve services, either by joining up existing services or developing new, co-ordinated services. One of the three ways in which Section 75 agreements can be agreed is in the establishment of a pooled fund, thus allowing the ability for partners each to contribute agreed funds to a single pot, to be spent on agreed projects for designated services.

6
NHS ENFIELD CLINICAL COMMISSIONING GROUP - Annual Accounts 2014-15
Notes to the financial statements
An agreement was reached to enter into a Section 75 Agreement between Enfield CCG and London Borough of Enfield for commissioned services for children, in line with the flexibilities outlined in the National Health Service Act 2006 for a total of £886,999 with the CCG contributing £253,021 to the fund.A second Section 75 Agreement was entered into between Enfield CCG and London Borough of Enfield to facilitate further integration of health and social care commissioning in accordance with Section 75 of the National Health Service Act 2006 for a total of £8.283 million with the CCG contributing £2.441 million to that fund.
1.6 Financial Transformation and Risk Share
All CCGs are required to budget for a contingency and to set aside a proportion of their overall resource limit for non-recurrent uses.
The purpose of this note is to provide a disclosure of the financial transformation and risk-share arrangement which is operated across the CCGs in North Central London. The financial and governance arrangements for the risk-share are overseen by the North London Joint Clinical Commissioning Committee. This Committee includes representation from each of the five CCGs in North Central London.
In 2014-15, the risk-share provided financial coverage for both the transformation of healthcare services and in-year financial risks. The governance and financial arrangements for the risk-share were approved by the CCG’s Governing Body. The financial statements for 2014-15 include relevant contributions and receipts relating to the risk-share for Enfield CCG. In particular, Note 19, which sets out the financial performance of the CCG in 2014-15, reflects income and expenditure relating to the risk-share.
The CCG contributed £1.682m to the risk share in 2014-15. The source of funding for the contribution was an element of its budgeted contingency. The overall level of funding received by the CCG from the risk-share in 2014-15 was £2.300m. This is set out in the table below:
Primary Care Strategy - £2.0m
Royal Free / Barnet & Chase Farm Transaction Costs - £0.3m
There is a firm commitment from each CCG in north central London to operate a similar transformation and risk-share arrangement for the medium term. The specific arrangements for the fund in 2015-16 will be approved by CCG Governing Bodies. The collaboration through the transformation and risk-share pool is seen by both the CCGs and NHS England as an important mechanism for both providing a necessary source of funding to facilitate the transformation of local health services and managing financial risk across the local health economy.
Historically, the former Primary Care Trusts in North Central London have operated a system of financial risk sharing. As part of the authorisation process for Clinical Commissioning Groups CCGs were advised to work collaboratively where possible and hence it was agreed to continue this practice within the five North Central London CCGs.
1.7 Critical Accounting Judgements & Key Sources of Estimation UncertaintyIn the application of the clinical commissioning group’s accounting policies, management is required to make judgements, estimates and assumptions about the carrying amounts of assets and liabilities that are not readily apparent from other sources. The estimates and associated assumptions are based on historical experience and other factors that are considered to be relevant. Actual results may differ from those estimates and the estimates and underlying assumptions are continually reviewed. Revisions to accounting estimates are recognised in the period in which the estimate is revised if the revision affects only that period or in the period of the revision and future periods if the revision affects both current and future periods.
1.7.1 Critical Judgements in Applying Accounting PoliciesThe following are the critical judgements, apart from those involving estimations (see below) that management has made in the process of applying the Clinical Commissioning Group’s accounting policies that have the most significant effect on the amounts recognised in the financial statements:
NHS Property Services/Community Health Partnerships Properties
Under IFRIC 4 the CCG recognises the need to account for payments to NHS Property Services Limited and Community Health Partnerships Limited as a lease arrangement. The indications of a lease include an arrangement comprising a transaction or a series of related transactions, that does not take the legal form of a lease but conveys a right to use an asset in return for a payment or series of payments.
Even though there is no formal contract in place, the transactions involved do convey the right of the CCG to use property assets. As such these transactions are being accounted for as an operating lease in accordance with IAS 17.
1.7.2 Key Sources of Estimation UncertaintyThe following are the key estimations that management has made in the process of applying the Clinical Commissioning Group’s accounting policies that have the most significant effect on the amounts recognised in the financial statements:
Partially completed spellsExpenditure relating to patient care spells that are part-completed at the year-end are apportioned across the financial years on the basis of length of stay at the end of the reporting period compared to expected total length of stay OR costs incurred to date compared to total expected costs. Estimate applies to a balance of £ 1,564,357 (£1,799,460 2013/14).Accruals
For goods and/or services that have been delivered but for which no invoice has been received/sent, the CCG makes an accrual based on the contractual arrangements that are in place and its legal obligation. See trade and other payables Note 9.Prescribing liabilities
7
NHS ENFIELD CLINICAL COMMISSIONING GROUP - Annual Accounts 2014-15
Notes to the financial statements
NHS England actions monthly cash charges to the CCG for prescribing contracts. These are issued approximately two months in arrears. The CCG uses a forecast based on previous in year charges (when the operating organisation was Enfield PCT) by the NHS Business Authority to estimate the full year expenditure. Estimate applies to a balance of £ 6,267,110 (£5,918,815 2013/14).
Maternity pathwaysExpenditure relating to all antenatal maternity care is made at the start of a pathway. As a result at the year-end part completed pathways at treated as a prepayment. The CCG agrees to use the figures calculated by the local Providers. Estimate applies to a balance of £1,955,805 (£1,800,169 2013/14).
1.8 RevenueRevenue in respect of services provided is recognised when, and to the extent that, performance occurs, and is measured at the fair value of the consideration receivable.Where income is received for a specific activity that is to be delivered in the following year, that income is deferred.
1.9 Employee Benefits1.9.1 Short-term Employee Benefits
Salaries, wages and employment-related payments are recognised in the period in which the service is received from employees, including bonuses earned but not yet taken.The cost of leave earned but not taken by employees at the end of the period is recognised in the financial statements to the extent that employees are permitted to carry forward leave into the following period.
1.9.2 Retirement Benefit Costs
Past and present employees are covered by the provisions of the NHS Pensions Scheme. The scheme is an unfunded, defined benefit scheme that covers NHS employers, General Practices and other bodies, allowed under the direction of the Secretary of State, in England and Wales. The scheme is not designed to be run in a way that would enable NHS bodies to identify their share of the underlying scheme assets and liabilities. Therefore, the scheme is accounted for as if it were a defined contribution scheme: the cost to the clinical commissioning group of participating in the scheme is taken as equal to the contributions payable to the scheme for the accounting period.
For early retirements other than those due to ill health the additional pension liabilities are not funded by the scheme. The full amount of the liability for the additional costs is charged to expenditure at the time the clinical commissioning group commits itself to the retirement, regardless of the method of payment.
1.10 Other Expenses
Other operating expenses are recognised when, and to the extent that, the goods or services have been received. They are measured at the fair value of the consideration payable.Expenses and liabilities in respect of grants are recognised when the clinical commissioning group has a present legal or constructive obligation, which occurs when all of the conditions attached to the payment have been met.
1.11 LeasesLeases are classified as finance leases when substantially all the risks and rewards of ownership are transferred to the lessee. All other leases are classified as operating leases.
1.11.1 The Clinical Commissioning Group as LesseeProperty, plant and equipment held under finance leases are initially recognised, at the inception of the lease, at fair value or, if lower, at the present value of the minimum lease payments, with a matching liability for the lease obligation to the lessor. Lease payments are apportioned between finance charges and reduction of the lease obligation so as to achieve a constant rate on interest on the remaining balance of the liability. Finance charges are recognised in calculating the clinical commissioning group’s surplus/deficit.Operating lease payments are recognised as an expense on a straight-line basis over the lease term. Lease incentives are recognised initially as a liability and subsequently as a reduction of rentals on a straight-line basis over the lease term.
Contingent rentals are recognised as an expense in the period in which they are incurred.
Where a lease is for land and buildings, the land and building components are separated and individually assessed as to whether they are operating or finance leases.
1.11.2 The Clinical Commissioning Group as Lessor
Amounts due from lessees under finance leases are recorded as receivables at the amount of the clinical commissioning group’s net investment in the leases. Finance lease income is allocated to accounting periods so as to reflect a constant periodic rate of return on the clinical commissioning group’s net investment outstanding in respect of the leases.
Rental income from operating leases is recognised on a straight-line basis over the term of the lease. Initial direct costs incurred in negotiating and arranging an operating lease are added to the carrying amount of the leased asset and recognised on a straight-line basis over the lease term.
1.12 Cash & Cash EquivalentsCash is cash in hand and deposits with any financial institution repayable without penalty on notice of not more than 24 hours. Cash equivalents are investments that mature in 3 months or less from the date of acquisition and that are readily convertible to known amounts of cash with insignificant risk of change in value.
In the Statement of Cash Flows, cash and cash equivalents are shown net of bank overdrafts that are repayable on demand and that form an integral part of the clinical commissioning group’s cash management.

8
NHS ENFIELD CLINICAL COMMISSIONING GROUP - Annual Accounts 2014-15
Notes to the financial statements
1.13 Clinical Negligence Costs
The NHS Litigation Authority operates a risk pooling scheme under which the clinical commissioning group pays an annual contribution to the NHS Litigation Authority which in return settles all clinical negligence claims. The contribution is charged to expenditure. Although the NHS Litigation Authority is administratively responsible for all clinical negligence cases the legal liability remains with the clinical commissioning group.
The total value of clinical negligence claims carried by the NHSLA on behalf of the CCG at 31st March 2015 is nil. (31st March 2014 was nil).
1.14 Non-clinical Risk PoolingThe clinical commissioning group participates in the Property Expenses Scheme and the Liabilities to Third Parties Scheme. Both are risk pooling schemes under which the clinical commissioning group pays an annual contribution to the NHS Litigation Authority and, in return, receives assistance with the costs of claims arising. The annual membership contributions, and any excesses payable in respect of particular claims are charged to operating expenses as and when they become due.
1.15 Continuing healthcare risk pooling
In 2014-15 a risk pool scheme has been introduced by NHS England for continuing healthcare claims, for claim periods prior to 31 March 2013. Under the scheme clinical commissioning group contribute annually to a pooled fund, which is used to settle the claims.
1.16 Contingencies
A contingent liability is a possible obligation that arises from past events and whose existence will be confirmed only by the occurrence or non-occurrence of one or more uncertain future events not wholly within the control of the clinical commissioning group, or a present obligation that is not recognised because it is not probable that a payment will be required to settle the obligation or the amount of the obligation cannot be measured sufficiently reliably. A contingent liability is disclosed unless the possibility of a payment is remote.
A contingent asset is a possible asset that arises from past events and whose existence will be confirmed by the occurrence or non-occurrence of one or more uncertain future events not wholly within the control of the clinical commissioning group. A contingent asset is disclosed where an inflow of economic benefits is probable.
Where the time value of money is material, contingencies are disclosed at their present value.
1.17 Financial Assets
Financial assets are recognised when the clinical commissioning group becomes party to the financial instrument contract or, in the case of trade receivables, when the goods or services have been delivered. Financial assets are derecognised when the contractual rights have expired or the asset has been transferred.
All Financial assets are classified as loans and receivables.The classification depends on the nature and purpose of the financial assets and is determined at the time of initial recognition.
1.18 Loans & Receivables
Loans and receivables are non-derivative financial assets with fixed or determinable payments which are not quoted in an active market. After initial recognition, they are measured at amortised cost using the effective interest method, less any impairment. Interest is recognised using the effective interest method.
The effective interest rate is the rate that exactly discounts estimated future cash receipts through the expected life of the financial asset, to the initial fair value of the financial asset.
At the end of the reporting period, the clinical commissioning group assesses whether any financial assets, other than those held at ‘fair value through profit and loss’ are impaired. Financial assets are impaired and impairment losses recognised if there is objective evidence of impairment as a result of one or more events which occurred after the initial recognition of the asset and which has an impact on the estimated future cash flows of the asset.
1.20 Financial Liabilities
Financial liabilities are recognised on the statement of financial position when the clinical commissioning group becomes party to the contractual provisions of the financial instrument or, in the case of trade payables, when the goods or services have been received. Financial liabilities are de-recognised when the liability has been discharged, that is, the liability has been paid or has expired.
Financial liabilities are initially recognised at fair value.
1.21 Value Added Tax
Most of the activities of the clinical commissioning group are outside the scope of VAT and, in general, output tax does not apply and input tax on purchases is not recoverable. Irrecoverable VAT is charged to the relevant expenditure category or included in the capitalised purchase cost of fixed assets. Where output tax is charged or input VAT is recoverable, the amounts are stated net of VAT.
1.22 Losses & Special Payments
Losses and special payments are items that Parliament would not have contemplated when it agreed funds for the health service or passed legislation. By their nature they are items that ideally should not arise. They are therefore subject to special control procedures compared with the generality of payments. They are divided into different categories, which govern the way that individual cases are handled.Losses and special payments are charged to the relevant functional headings in expenditure on an accruals basis, including losses which would have been made good through insurance cover had the clinical commissioning group not been bearing its own risks (with insurance premiums then being included as normal revenue expenditure).
1.23 Accounting Standards That Have Been Issued But Have Not Yet Been Adopted
The Government Financial Reporting Manual does not require the following Standards and Interpretations to be applied in 2014-15, all of which are subject to consultation:

9
NHS ENFIELD CLINICAL COMMISSIONING GROUP - Annual Accounts 2014-15
Notes to the financial statements
· IFRS 9: Financial Instruments· IFRS 13: Fair Value Measurement· IFRS 14: Regulatory Deferral Accounts· IFRS 15: Revenue for Contract with Customers
The application of the Standards as revised would not have a material impact on the accounts for 2014-15, were they applied in that year.

10
NHS ENFIELD CLINICAL COMMISSIONING GROUP - Annual Accounts 2014-15
2 Other Operating Revenue2014-15 2014-15 2014-15 2013-14
Total Admin Programme Total
£000 £000 £000 £000
Prescription fees and charges 83 0 83 49Education, training and research 317 317 0 35Non-patient care services to other bodies 1,761 67 1,694 3,096Income generation 0 0 0 154Other revenue 242 82 159 160Total other operating revenue 2,403 467 1,936 3,494
2.1 Revenue2014-15 2014-15 2014-15 2013-14
Total Admin Programme Total£000 £000 £000 £000
From rendering of services 2,403 467 1,936 3,494From sale of goods 0 0 0 0Total 2,403 467 1,936 3,494
Revenue in this note does not include cash received from NHS England, which is drawn down directly into the bank account of the CCG and credited to the General Fund.
Revenue is totally from the supply of services. The clinical commissioning group receives no revenue from the sale of goods.
Other revenue in this note includes a charge of £154,000 by the CCG to North East London CSU for use of CCG facilities during 2013/14. In 2013/14 there were service departments of the CSU based within Holbrook House and a recharge was made to recover establishment costs. In 2014/15 these departments were no longer based within Holbrook House as the team in question disbanded and no longer occupied the space.
Admin revenue is revenue received that is not directly attributable to the provision of healthcare or healthcare services.

11
NHS ENFIELD CLINICAL COMMISSIONING GROUP - Annual Accounts 2014-15
3. Employee benefits and staff numbers3.1.1 Employee benefits
2014-15 Total Admin Programme
TotalPermanent Employees Other Total
Permanent Employees Other Total
Permanent Employees Other
£000 £000 £000 £000 £000 £000 £000 £000 £000Employee BenefitsSalaries and wages 5,937 3,985 1,952 3,284 1,789 1,495 2,653 2,196 458Social security costs 349 349 0 171 171 0 178 178 0Employer Contributions to NHS Pension scheme 436 436 0 201 201 0 235 235 0Gross employee benefits expenditure 6,721 4,769 1,952 3,656 2,161 1,495 3,065 2,608 458
Less recoveries in respect of employee benefits (note 4.1.2) 0 0 0 0 0 0 0 0 0Total - Net admin employee benefits including capitalised costs 6,721 4,769 1,952 3,656 2,161 1,495 3,065 2,608 458
Less: Employee costs capitalised 0 0 0 0 0 0 0 0 0Net employee benefits excluding capitalised costs 6,721 4,769 1,952 3,656 2,161 1,495 3,065 2,608 458
2013/14 Total Admin ProgrammeTotal
Employees Other Total
Employees Other Total
Employees Other
£000 £000 £000 £000 £000 £000 £000 £000 £000Employee BenefitsSalaries and wages 5,270 3,464 1,806 2,257 1,591 666 3,013 1,873 1,140Social security costs 569 569 0 177 177 0 392 392 0Employer Contributions to NHS Pension scheme 359 359 0 192 192 0 167 167 0Gross employee benefits expenditure 6,198 4,392 1,806 2,626 1,960 666 3,572 2,432 1,140
Less recoveries in respect of employee benefits (note 4.1.2) 0 0 0 0 0 0 0 0 0Total - Net admin employee benefits including capitalised costs 6,198 4,392 1,806 2,626 1,960 666 3,572 2,432 1,140
Less: Employee costs capitalised 0 0 0 0 0 0 0 0 0Net employee benefits excluding capitalised costs 6,198 4,392 1,806 2,626 1,960 666 3,572 2,432 1,140
3.2 Average number of people employed 2013-14
TotalPermanently
employed Other TotalNumber Number Number Number
Total 99 74 25 85
Of the above:Number of whole time equivalent people engaged on capital projects 0 0 0 0
3.3 Staff sickness absence and ill health retirements 2014-15 2013-14Number Number
Total Days Lost 588 159Total Staff Years 74 63Average working Days Lost 7.9 2.5
2014-15 2013-14Number Number
Number of persons retired early on ill health grounds 0 0
£000 £000Total additional Pensions liabilities accrued in the year 0 0
Ill health retirement costs are met by the NHS Pension Scheme
2014-15

12
NHS ENFIELD CLINICAL COMMISSIONING GROUP - Annual Accounts 2014-15
3.4 Pension costs
Past and present employees are covered by the provisions of the NHS Pension Scheme. Details of the benefits payable under these provisions can be found on the NHS Pensions website at www.nhsbsa.nhs.uk/Pensions.
The Scheme is an unfunded, defined benefit scheme that covers NHS employers, GP practices and other bodies, allowed under the direction of the Secretary of State, in England and Wales. The Scheme is not designed to be run in a way that would enable NHS bodies to identify their share of the underlying scheme assets and liabilities.
Therefore, the Scheme is accounted for as if it were a defined contribution scheme: the cost to the Clinical Commissioning Group of participating in the Scheme is taken as equal to the contributions payable to the Scheme for the accounting period.
The Scheme is subject to a full actuarial valuation every four years (until 2004, every five years) and an accounting valuation every year. An outline of these follows:
3.4.1 Full actuarial (funding) valuation
The purpose of this valuation is to assess the level of liability in respect of the benefits due under the Scheme (taking into account its recent demographic experience), and to recommend the contribution rates to be paid by employers and scheme members. The last such valuation, which determined current contribution rates was undertaken as at 31 March 2004 and covered the period from 1 April 1999 to that date. The conclusion from the 2004 valuation was that the Scheme had accumulated a notional deficit of £3.3 billion against the notional assets as at 31 March 2004.
In order to defray the costs of benefits, employers pay contributions at 14% of Pensionable pay and most employees had up to April 2008 paid 6%, with manual staff paying 5%.
Following the full actuarial review by the Government Actuary undertaken as at 31 March 2004, and after consideration of changes to the NHS Pension Scheme taking effect from 1 April 2008, his Valuation report recommended that employer contributions could continue at the existing rate of 14% of Pensionable pay, from 1 April 2008, following the introduction of employee contributions on a tiered scale from 5% up to 8.5% of their Pensionable pay depending on total earnings. On advice from the scheme actuary, scheme contributions may be varied from time to time to reflect changes in the scheme’s liabilities.
3.4.2 Accounting valuation
A valuation of the scheme liability is carried out annually by the scheme actuary as at the end of the reporting period by updating the results of the full actuarial valuation.
Between the full actuarial valuations at a two-year midpoint, a full and detailed member data-set is provided to the scheme actuary. At this point the assumptions regarding the composition of the scheme membership are updated to allow the scheme liability to be valued.
The valuation of the scheme liability as at 31 March 2011 is based on detailed membership data as at 31 March 2008 (the latest midpoint) updated to 31 March 2011 with summary global member and accounting data.
The latest assessment of the liabilities of the Scheme is contained in the scheme actuary report, which forms part of the annual NHS Pension Scheme (England and Wales) Resource Account, published annually. These accounts can be viewed on the NHS Pensions website. Copies can also be obtained from The Stationery Office.

13
NHS ENFIELD CLINICAL COMMISSIONING GROUP - Annual Accounts 2014-15
3.4 Pension costs
3.4.3 Scheme Provisions
The NHS Pension Scheme provides defined benefits, which are summarised below. This list is an illustrative guide only, and is not intended to detail all the benefits provided by the Scheme or the specific conditions that must be met before these benefits can be obtained:
The Scheme is a “final salary” scheme. Annual pensions are normally based on 1/80th for the 1995 section and of the best of the last three years pensionable pay for each year of service, and 1/60th for the 2008 section of reckonable pay per year of membership. Members who are practitioners as defined by the Scheme Regulations have their annual pensions based upon total pensionable earnings over the relevant pensionable service;
With effect from 1 April 2008 members can choose to give up some of their annual pension for an additional tax free lump sum, up to a maximum amount permitted under HM Revenue & Customs rules. This new provision is known as “pension commutation”;
Annual increases are applied to pension payments at rates defined by the Pensions (Increase) Act 1971, and are based on changes in retail prices in the twelve months ending 30 September in the previous calendar year;
Early payment of a pension, with enhancement, is available to members of the Scheme who are permanently incapable of fulfilling their duties effectively through illness or infirmity. A death gratuity of twice final year’s pensionable pay for death in service, and five times their annual pension for death after retirement is payable;
For early retirements other than those due to ill health the additional pension liabilities are not funded by the scheme. The full amount of the liability for the additional costs is charged to the statement of comprehensive net expenditure at the time the clinical commissioning group commits itself to the retirement, regardless of the method of payment; and,
Members can purchase additional service in the Scheme and contribute to money purchase AVC’s run by the Scheme’s approved providers or by other Free Standing Additional Voluntary Contributions (FSAVC) providers.
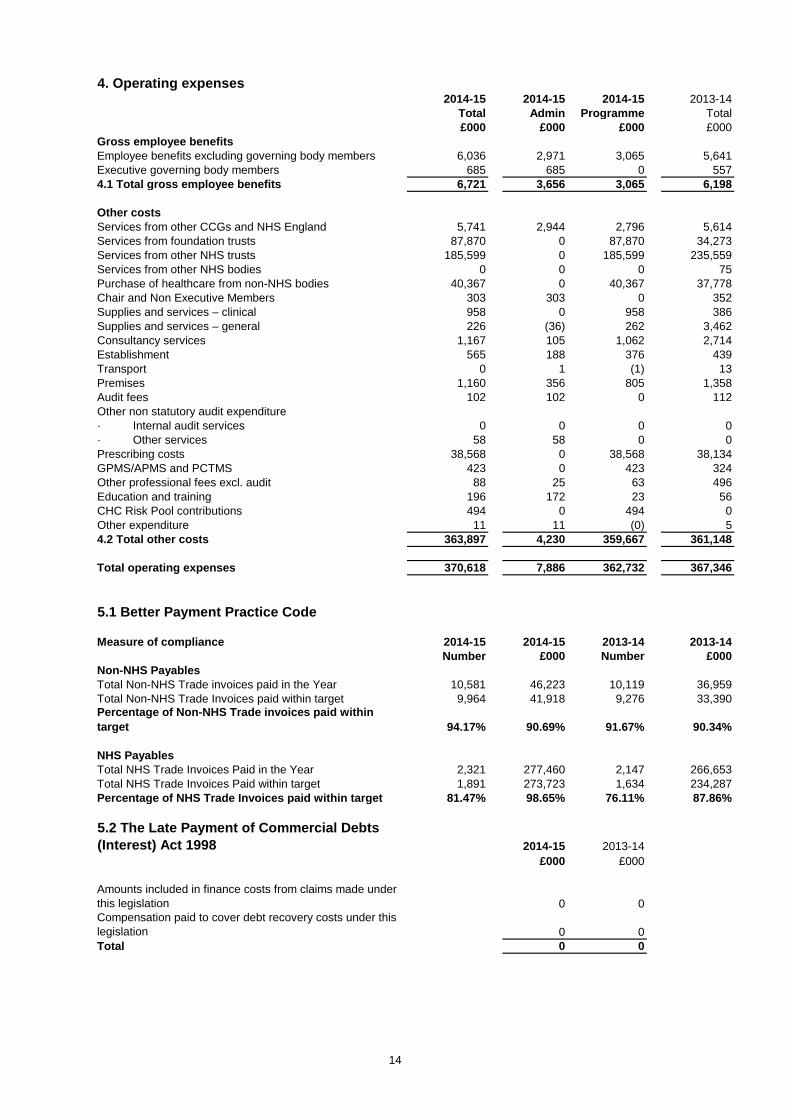
14
4. Operating expenses2014-15 2014-15 2014-15 2013-14
Total Admin Programme Total£000 £000 £000 £000
Gross employee benefitsEmployee benefits excluding governing body members 6,036 2,971 3,065 5,641Executive governing body members 685 685 0 5574.1 Total gross employee benefits 6,721 3,656 3,065 6,198
Other costsServices from other CCGs and NHS England 5,741 2,944 2,796 5,614Services from foundation trusts 87,870 0 87,870 34,273Services from other NHS trusts 185,599 0 185,599 235,559Services from other NHS bodies 0 0 0 75Purchase of healthcare from non-NHS bodies 40,367 0 40,367 37,778Chair and Non Executive Members 303 303 0 352Supplies and services – clinical 958 0 958 386Supplies and services – general 226 (36) 262 3,462Consultancy services 1,167 105 1,062 2,714Establishment 565 188 376 439Transport 0 1 (1) 13Premises 1,160 356 805 1,358Audit fees 102 102 0 112Other non statutory audit expenditure· Internal audit services 0 0 0 0· Other services 58 58 0 0Prescribing costs 38,568 0 38,568 38,134GPMS/APMS and PCTMS 423 0 423 324Other professional fees excl. audit 88 25 63 496Education and training 196 172 23 56CHC Risk Pool contributions 494 0 494 0Other expenditure 11 11 (0) 54.2 Total other costs 363,897 4,230 359,667 361,148
Total operating expenses 370,618 7,886 362,732 367,346
5.1 Better Payment Practice Code
Measure of compliance 2014-15 2014-15 2013-14 2013-14Number £000 Number £000
Non-NHS PayablesTotal Non-NHS Trade invoices paid in the Year 10,581 46,223 10,119 36,959Total Non-NHS Trade Invoices paid within target 9,964 41,918 9,276 33,390Percentage of Non-NHS Trade invoices paid within target 94.17% 90.69% 91.67% 90.34%
NHS PayablesTotal NHS Trade Invoices Paid in the Year 2,321 277,460 2,147 266,653Total NHS Trade Invoices Paid within target 1,891 273,723 1,634 234,287Percentage of NHS Trade Invoices paid within target 81.47% 98.65% 76.11% 87.86%
5.2 The Late Payment of Commercial Debts (Interest) Act 1998 2014-15 2013-14
£000 £000
Amounts included in finance costs from claims made under this legislation 0 0Compensation paid to cover debt recovery costs under this legislation 0 0Total 0 0

15
NHS ENFIELD CLINICAL COMMISSIONING GROUP - Annual Accounts 2014-15
6. Operating Leases
6.1 As lessee6.1.1 Payments recognised as an Expense 2014-15 2013-14
Buildings Other Total Total£000 £000 £000 £000
Payments recognised as an expenseMinimum lease payments 1,101 36 1,137 1285Contingent rents 0 0 0 0Sub-lease payments 0 0 0 0Total 1,101 36 1,137 1,285
7. Trade and other receivables Current Current2014-15 2013-14
£000 £000
NHS receivables: Revenue 262 428NHS prepayments and accrued income * 2,315 2,322Non-NHS receivables: Revenue 1,981 1,652Non-NHS prepayments and accrued income 960 175Provision for the impairment of receivables (2,436) (778)VAT 121 107Total Trade & other receivables 3,203 3,906
Total current and non current 3,203 3,906
Included above:Prepaid pensions contributions 0 0Prepaid NHS Maternity Pathway Funding * 1,956 1,800
7.1 Receivables past their due date but not impaired 2014-15 2013-14£000 £000
By up to three months 723 927By three to six months 135 0By more than six months 779 0Total 1,637 927
£637k of the amount above has subsequently been recovered post the statement of financial position date.
7.2 Provision for impairment of receivables 2014-15 2013-14£000 £000
Balance at 1 April 2014 (778) 0
Amounts written off during the year 0 0Amounts recovered during the year 0 0(Increase) decrease in receivables impaired (1,658) (778)Transfer (to) from other public sector body 0 0Balance at 31 March 2015 (2,436) (778)
2014-15 2013-14£000 £000
Receivables are provided against at the following rates:Invoices disputed by Local Authority 100% 100%
The CCG will continue to pursue recovery of these impaired receivables, however a provision has been deemed necessary in this instance as recovery will be extremely challenging.
The great majority of trade is with NHS England. As NHS England is funded by Government to provide funding to Clinical Commissioning Groups to commission services, no credit scoring of them is considered necessary.
The Clinical Commissioning Group occupies property owned and managed by Community Health Partnerships Ltd and /or NHS Property Services Ltd. For 2014/15, a transitional occupancy rent based on annual property cost allocations was agreed. This is reflected in note 6.1.1 above.
Whilst our arrangements with Community Health Partnerships Limited and NHS Property Services Limited fall within the definition of operating leases, rental charges for future years have not yet been agreed . Consequently this note does not include future minimum lease payments for these arrangements.
The CCG evaluates its receivables age analysis on a regular basis for potential irrecoverable debt. The clinical commissioning group assesses receivables for recoverability on an individual basis and to make provision where it is considered necessary. In assessing recoverability the CCG takes into account any indicators of impairment up until the reporting date. The overall level of credit risk is considered to be relatively low due to the proportion of the customer base which is comprised of NHS bodies and other central and local government bodies.

16
NHS ENFIELD CLINICAL COMMISSIONING GROUP - Annual Accounts 2014-15
8. Cash and cash equivalents
2014-15 2013-14£000 £000
Balance at 1 April 2014 154 0Net change in year (122) 154Balance at 31 March 2015 32 154
Made up of:Cash with the Government Banking Service 32 154Cash and cash equivalents as in statement of financial position 32 154
Current Current2014-15 2013-14
£000 £000
NHS payables: revenue 16,329 16,170NHS accruals and deferred income 3,672 1,875Non-NHS payables: revenue 9,513 4,396Non-NHS accruals and deferred income 8,606 9,695Social security costs 64 58Tax 69 57Other payables 493 160Total Trade & Other Payables 38,746 32,411
Total current and non-current 38,746 32,411
Current Current2014-15 2013-14
£000 £000
Total current and non-current 0 0
11 Contingencies
Contingent liabilities
The CCG has no contingent liabilities (2013/14 nil).
Under the Accounts Direction issued by NHS England on 12 February 2014, NHS England is responsible for accounting for liabilities relating to NHS Continuing Healthcare claims relating to periods of care before establishment of the clinical commissioning group. However, the legal liability remains with the CCG. The total value of legacy NHS Continuing Healthcare provisions accounted for by NHS England on behalf of this CCG at 31 March 2015 is £1,030,000 (£7,156,000 at 31st March 2014).
10 Provisions
9 Trade and other payables
Other payables include £71k outstanding pension contributions at 31 March 2015 (£62K 2013/14)

17
NHS ENFIELD CLINICAL COMMISSIONING GROUP - Annual Accounts 2014-15
12 Financial instruments
12.1 Financial risk management
12.1.1 Currency risk
12.1.2 Interest rate risk
12.1.3 Credit risk
12.1.3 Liquidity risk
The Clinical Commissioning Group borrows from government for capital expenditure, subject to affordability as confirmed by NHS England. The borrowings are for 1 to 25 years, in line with the life of the associated assets, and interest is charged at the National Loans Fund rate, fixed for the life of the loan. The clinical commissioning group therefore has low exposure to interest rate fluctuations.
Because the majority of the NHS Clinical Commissioning Group and revenue comes parliamentary funding, NHS Clinical Commissioning Group has low exposure to credit risk. The maximum exposures as at the end of the financial year are in receivables from customers, as disclosed in the trade and other receivables note.
NHS Clinical Commissioning Group is required to operate within revenue and capital resource limits, which are financed from resources voted annually by Parliament. The NHS Clinical Commissioning Group draws down cash to cover expenditure, as the need arises. The NHS Clinical Commissioning Group is not, therefore, exposed to significant liquidity risks.
Financial reporting standard IFRS 7 requires disclosure of the role that financial instruments have had during the period in creating or changing the risks a body faces in undertaking its activities.
Because NHS Clinical Commissioning Group is financed through parliamentary funding, it is not exposed to the degree of financial risk faced by business entities. Also, financial instruments play a much more limited role in creating or changing risk than would be typical of listed companies, to which the financial reporting standards mainly apply. The clinical commissioning group has limited powers to borrow or invest surplus funds and financial assets and liabilities are generated by day-to-day operational activities rather than being held to change the risks facing the clinical commissioning group in undertaking its activities.
Treasury management operations are carried out by the finance department, within parameters defined formally within the NHS Clinical Commissioning Group standing financial instructions and policies agreed by the Governing Body. Treasury activity is subject to review by the NHS Clinical Commissioning Group and internal auditors.
The NHS Clinical Commissioning Group is principally a domestic organisation with the great majority of transactions, assets and liabilities being in the UK and sterling based. The NHS Clinical Commissioning Group has no overseas operations. The NHS Clinical Commissioning Group and therefore has low exposure to currency rate fluctuations.

18
NHS ENFIELD CLINICAL COMMISSIONING GROUP - Annual Accounts 2014-15
12 Financial instruments cont'd
12.2 Financial assetsLoans and
Receivables Total2014-15 2014-15
£000 £000
Receivables:· NHS 262 262· Non-NHS 1,981 1,981Cash at bank and in hand 32 32Other financial assets 0 0Total at 31 March 2015 2,275 2,275
Loans and Receivables Total
2013-14 2013-14£000 £000
Receivables:· NHS 428 428· Non-NHS 1,652 1,652Cash at bank and in hand 154 154Other financial assets 0 0Total at 31 March 2014 2,234 2,234
12.3 Financial liabilitiesPayables Total
2014-15 2014-15£000 £000
Payables:· NHS 20,001 20,001· Non-NHS 18,612 18,612Total at 31 March 2015 38,613 38,613
Payables Total2013-14 2013-14
£000 £000Payables:· NHS 18,045 18,045· Non-NHS 14,091 14,091Total at 31 March 2014 32,136 32,136

19
NHS ENFIELD CLINICAL COMMISSIONING GROUP - Annual Accounts 2014-15
13 Pooled budgets
2014-15 2013-14£000 £000
Income 0 0Expenditure 2,694 2,632
2014-15 2013-14£000 £000
Expenditure - Commissioned Services for Children 253 181Expenditure - Integration of Health & Social Care Commissioning 2,441 2,451
2,694 2,63214 Risk Share
Historically, the former Primary Care Trusts in North Central London have operated a system of financial risk sharing. As part of the authorisation process for Clinical Commissioning Groups CCGswere advised to work collaboratively where possible and hence it was agreed to continue this practicewithin the five North Central London CCGs.
2014-15 2013-14
£000 £000(a) Primary Care Strategy 2,000 2,500 (b) Whittington Trust Support - 123 (c) Barnet, Enfield & Haringey Clinical Strategy - 9,700 (on behalf of Barnet CCG, Enfield CCG and Haringey CCG) (d) Barnet & Chase Farm Trust RTT 300 4,500 (on behalf of Barnet CCG and Enfield CCG)(e) Activity Pressures re SLA over-performance - 6,269
2,300 23,092
15 Intra-government and other balancesCurrent
ReceivablesCurrent
Payables2014-15 2014-15
£000 £000Balances with:· Local Authorities 393 4,075
Balances with NHS bodies:· NHS Trusts and Foundation Trusts 2,577 20,001Total of balances with NHS bodies: 2,577 20,001
· Bodies external to Government 233 14,670
Total balances at 31 March 2015 3,203 38,746
Current Receivables
Current Payables
2013-14 2013-14£000 £000
Balances with:· Local Authorities 254 0
Balances with NHS bodies:· NHS Trusts and Foundation Trusts 2,749 18,045Total of balances with NHS bodies: 2,749 18,045
· Bodies external to Government 903 14,366
Total balances at 31 March 2014 3,906 32,411
The NHS Clinical Commissioning Group shares of the income and expenditure handled by the pooled budget in the financial year were:
The five CCG Governing Bodies in North Central London approved the North London 2014/15 CCG Risk Share agreement during early summer 2014. As one of the five CCGs in North Central London Enfield CCG contributed and utilised the Risk Share. As one of the five CCGs in North Central London Enfield CCG contributed towards and utilised the Risk Share.
Enfield CCG contributed £1.682 million from its contingency fund and Headroom Reserve. It received a total of £2.300 million, which was spent in the following areas:

20
NHS ENFIELD CLINICAL COMMISSIONING GROUP - Annual Accounts 2014-15
16 Related party transactions
Payments to Related
Party
Receipts from
Related Party
Amounts owed to Related
Party
Amounts due from
Related Party
£000 £000 £000 £000Barndoc Healthcare Ltd 1,326 - 6 - Enfield GP Healthcare Network Ltd 8 - - - Enfield Health Partnership Ltd 609 - - - Enfield Healthcare Alliance Ltd 24 - - - Medicare Medical Services LLP 222 - 131 - Vision Mental Healthcare Ltd 103 - - - White Lodge Medical Services Ltd 2 - 27 -
Payments to Related
Party
Receipts from
Related Party
Amounts owed to Related
Party
Amounts due from
Related Party
£000 £000 £000 £000Abernethy House 118 - 10 (1) Angel Surgery 16 - 7 - Arnos Grove Medical Centre 8 - - - Bincote Road Surgery 45 - 5 - Bounces Road Surgery 70 - 7 - Boundary Court Surgery 34 - 7 - Boundary House Surgery 30 - - - Bowes Medical Centre 178 - 2 - Brick Lane Surgery 19 - 6 - Bush Hill Park Medical Centre 5 - - - Carlton House Surgery 103 - 12 - Chalfont Road Surgery 54 - - - Cockfosters Medical Centre 24 - - (1) Connaught Surgery 30 - 7 - Curzon Avenue Surgery 46 - 10 - Dean House Surgery 13 - 3 - Dover House GP Practice 27 - - - Eagle House Surgery Enfield 99 - 22 - East Enfield Medical Practice 8 - - - Edmonton Medical Centre 8 - 3 - Enfield Island Surgery 39 - 3 - Evergreen PCC 75 (1) 29 - Forest Group Practice 44 - 10 (2) Freezywater Primary Care Centre 162 - 12 - Gillan House Surgery 192 - 12 - Green Cedars GP Surgery 14 - - - Green Lanes Surgery 112 - - - Green Street Surgery 5 - - - Grovelands Road Medical Centre 53 - 7 - Highlands Practice 50 - 2 - Jaina House Surgery 1 - - - Keats Surgery 16 - - -
The transactions listed below are in relation to interests declared, other than those relating to member general practices.
Clinical commissioning groups are clinically led membership organisations made up of general practices. The
The members of Enfield Clinical Commissioning Group are contained within Appendix B of the constitution. Where payments have been made to these practices, these are listed below. The majority of the payments are in relation to agreed locally enhanced services and some prescribing costs.

21
NHS ENFIELD CLINICAL COMMISSIONING GROUP - Annual Accounts 2014-15
Payments to Related
Party
Receipts from
Related Party
Amounts owed to Related
Party
Amounts due from
Related Party
£000 £000 £000 £000
Latymer Road Surgery 20 - - - Lincoln Road Medical Practice 165 - 4 - Moorfield Road Health Centre 7 - 3 - Morecambe Surgery 53 - 6 - Nightingale House Surgery 53 - - - North London Health Centre 36 - 12 - Oakwood Medical Centre London 81 (1) 6 - Park Lodge Medical Centre 52 - 10 - Rainbow Practice 37 - 4 - Riley House Surgery 35 - 8 - Riverside Practice 5 - - - Southbury Surgery 27 - 4 - Southgate Surgery 36 - - - Town Surgery 17 - - - Trinity Avenue Surgery 4 - 2 - White Lodge Medical Practice 79 - 1 - Willow House Surgery 23 - - - Winchmore Practice 9 - 25 (3) Woodberry Practice 135 - 13 -
Payments to Related
Party
Receipts from
Related Party
Amounts owed to Related
Party
Amounts due from
Related Party
£000 £000 £000 £000
NHS England 494 (343) 102 (181) NHS Barnet CCG 300 (125) 507 (126) NHS Haringey CCG 387 (470) 24 (54) NHS North & East London CSU 4,865 (7) 127 - Barnet & Chase Farm Hospitals NHS Trust 16,275 - - - Barnet, Enfield & Haringey Mental Health NHS Trust 52,764 (83) 1,832 (20) Barts Health NHS Trust 3,942 - 60 - Imperial College Healthcare NHS Trust 836 - 133 - London Ambulance Service NHS Trust 10,010 - 135 - London North West Healthcare NHS Trust 303 - 105 - North Middlesex University Hospital NHS Trust 92,786 - 1,052 (1,305) North West London Hospitals NHS Trust 291 - - - Royal National Orthopaedic Hospital NHS Trust 1,886 - (4) (55) The Princess Alexandra Hospital NHS Trust 476 - 113 - The Whittington Hospital NHS Trust 3,984 - 338 (78) Camden & Islington NHS Foundation Trust 333 - 333 - Central & North West London NHS Foundation Trust 1,072 - 120 - Chelsea And Westminster Hospital NHS Foundation Trust 315 - 89 - Great Ormond Street Hospital for Children NHS Foundation Trust 731 - - (96)
Guy's & St Thomas' NHS Foundation Trust 1,302 - 188 - Homerton University Hospital NHS Foundation Trust 1,670 - 84 - King's College Hospital NHS Foundation Trust 421 - 115 - Moorfields Eye Hospital NHS Foundation Trust 3,594 - 212 - North East London NHS Foundation Trust 302 - 225 -
The Department of Health is regarded as a related party. During the year the clinical commissioning group has had a significant number of material transactions with entities for which the Department is regarded as the parent Department. A de minimis limit of £250k has ben applied in reporting these figures.

22
NHS ENFIELD CLINICAL COMMISSIONING GROUP - Annual Accounts 2014-15
Payments to Related
Party
Receipts from
Related Party
Amounts owed to Related
Party
Amounts due from
Related Party
£000 £000 £000 £000
Royal Brompton & Harefield NHS Foundation Trust 361 - 68 - Royal Free London NHS Foundation Trust 60,890 - 8,076 (436) University College London Hospitals NHS Foundation Trust 15,283 - 3,783 (136) Health Education England 7 (317) 66 (100) NHS Property Services 1,001 (4) 822 (1) National Health Service Pension Scheme 436 - - -
Payments to Related
Party
Receipts from
Related Party
Amounts owed to Related
Party
Amounts due from
Related Party
£000 £000 £000 £000
Enfield London Borough Council 8,608 (832) 4,075 (2,829) HM Revenue and Customs Trust Statement 348 - - -
In addition, the clinical commissioning group has had a number of material transactions with other government departments and other central and local government bodies. Most of these transactions have been with Local Authorities or HMRC. A de minimis limit of £250k has ben applied in reporting these figures.

23
NHS ENFIELD CLINICAL COMMISSIONING GROUP - Annual Accounts 2014-15
17 Events after the end of the reporting period
18 Losses and special payments
There are no losses or special payments to report for 2014-15 (Nil 2013/14).
19 Financial performance targets
Clinical Commissioning Groups have a number of financial duties under the NHS Act 2006 (as amended).The Clinical Commissioning Group’s performance against those duties was as follows:
2014-15 2014-15 2014-15 2014-15Target
PerformanceActual
PerformanceSurplus / (Deficit) Duty Achieved
£000 £000 £000 Yes / No
Expenditure not to exceed income 351,747 370,618 (18,871) No
Capital resource use does not exceed the amount specified in Directions
- - - Yes
Revenue resource use does not exceed the amount specified in Directions 349,344 368,215 (18,871) No
Capital resource use on specified matter(s) does not exceed the amount specified in Directions
- - - Yes
Revenue resource use on specified matter(s) does not exceed the amount specified in Directions - - - Yes
Revenue resource use does not exceed the amount specified in Directions - Administration 7,742 7,420 322 Yes
2013-14 2013-14 2013-14 2013-14Target
PerformanceActual
PerformanceSurplus / (Deficit) Duty Achieved
£000 £000 £000 Yes / No
Expenditure not to exceed income 367,696 367,346 350 YesCapital resource use does not exceed the amount specified in Directions
- - - Yes
Revenue resource use does not exceed the amount specified in Directions
364,202 363,852 350 Yes
Capital resource use on specified matter(s) does not exceed the amount specified in Directions
- - - Yes
Revenue resource use on specified matter(s) does not exceed the amount specified in Directions
- - - Yes
Revenue resource use does not exceed the amount specified in Directions - Administration
7,670 7,549 121 Yes
There are no post balance sheet events which will have a material effect on the financial statements of the Clinical Commissioning Group.
Note: Expenditure is defined as the aggregate of gross expenditure on revenue and capital in the financial year; and, income is defined as the aggregate of the notified maximum revenue resource, notified capital resource and all other amounts accounted as received in the financial year (whether under provisions of the Act or from other sources, and included here on a gross basis).
Re-stated
Due to a change in presentation requirements for 2014-15, the 2013-14 figures are restated to a comparable basis to 2014-15.