annual report for looked after children
TRANSCRIPT

LAC Annual Report 2017 - 2018
Annual Report for Looked After Children
1st
April 2017 to 31st
March 2018
Report Author:
Wendy Costello – Named Nurse for Looked After Children, City Health Care Partnership CIC
Report Contributors:
Angie Rawlings – Designated Nurse for Looked After Children, Hull Clinic Commissioning Group City
Health Care Partnership CIC
Dr. Kanika Grover – Designated Doctor for Looked After Children, City Health Care Partnership CIC
Tracy Gamble - Clinical Manager, 0 - 19 Public Health Nursing, City Health Care Partnership CIC
Endorsed by:
Tracy Vickers - Executive Nurse & Care Group Director, Care Group 2
Page 1

LAC Annual Report 2017 - 2018
CONTENTS
Glossary of terms
1. Introduction
2. National Guidance
3. Local Commissioner / Provider arrangements
4. 2017 CQC Inspection Action Outcomes
5. Integrated Looked after Children meetings (ILAC/Health & Social Care)
6. Performance
7. Initial and Review Health Assessments
8. Late notifications
9. Consent
10. Dental Health
11. Immunisations
12. Sexual Health
13. Child Sexual Exploitation
14. Emotional Health
15. Substance Misuse
16. Looked After Children and Young People’s Health Team (LACHT)
17. Service User Feedback
18. Conclusion
19. Recommendations
Appendix 1.
Action Plan 2016/17
Appendix 2.
IHA Quality Assurance data from Designated Doctor for LAC
Page 2

LAC Annual Report 2017 - 2018
GLOSSARY OF TERMS
CAMHS – Child and Adolescent Mental Health
CAYP – Children and Young People
CCG – Clinical Commissioning Group
CHCP CIC - City Health Care Partnership CIC
CLA – Child Looked After
Coram BAAF - British Association for Adoption and Fostering
CQC – Care Quality Commission
CSE – Child Sexual Exploitation
DFE – Department For Education
DFES - Department For Education and Skills
DH – Department of Health
DoH - Department of Health
ECR – Electronic Care Record
GIDS – Gender Identity Development Service
GP – General Practitioner
HDP – Health and Development Practitioner
HV – Health Visitor
ICRO – Independent Conferencing and Reviewing Officer
IHA – Initial Health Assessment
ILAC – Integrated Looked After Children Team
KPI – Key Performance Indicators
LA – Local Authority
LAC –Looked After Child
LACHT - Looked After Children Health Team
LL – Liquid Logic
MACE – Multi-Agency Child Exploitation Meetings
NICE – National Institute for Clinical Care and Excellence
OOA – Out of Area
RCPCH - Royal College of Paediatrics and Child Health
RHA – Review Health Assessment
Page 3

LAC Annual Report 2017 - 2018
RIT – Risk Indicator Tool
S1 – SystmOne (electronic health care record)
SDQ – Strength and Difficulties Questionnaire
SOP – Standard Operating Procedure
SW – Social Worker
Page 4

LAC Annual Report 2017 - 2018
1. Introduction
The Statutory Guidance for promoting the health and wellbeing of Looked After Children (2015)
requires the Designated Doctor and Designated Nurse to complete an annual report that evaluates
the delivery of health services to children and young people Looked After within the care system.
This report will provide a brief overview of the local commissioner / provider arrangements detailing
how Looked After Children’s (LAC) health services are delivered by City Health Care Partnership CIC
(CHCP CIC).
It will include an evaluation of the delivery of health services for LAC and young people within the
local care system, with reference to activity and performance outcomes against National Guidance.
The information within this report is taken from data held by CHCP CIC within the electronic care
record (ECR) known as SystmOne (S1) for children and young people who were registered as being
Looked After during the following time frame - 1st
April 2017 – 31st
March 2018.
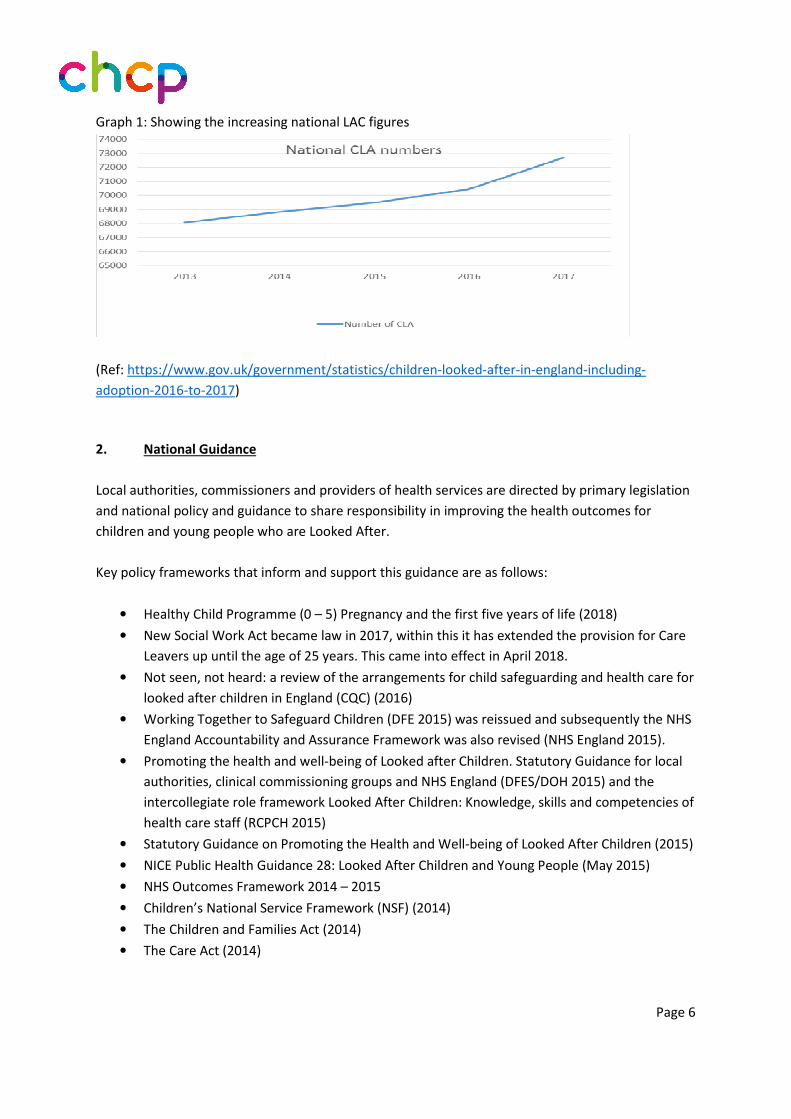
Government data for LAC is published 1 year retrospectively, therefore the national data discussed
in this report is for the year 2016 – 2017. Nationally the number of LAC has continued to rise; it has
increased steadily over the last nine years.
By 31 March 2017 there were 72,670 LAC in the UK, an increase of 3% on 2016. The number of
children starting to be Looked After has also risen in recent years and has increased by 2% over 2016
- 2017 when compared to the previous year.
Table 1: Number of LAC at 31 March 2013 to 2017
Year ending 31
March
Number of
Looked After
Children
Year on year
change
Rate per 10,000
children under 18
years
2013 68,070 60
2014 68,820 +1% 60
2015 69,500 +1% 60
2016 70,450 +1% 60
2017 72,670 +3% 62
Source: SSDA 903
The number of children ceasing to be Looked After in 2016-17 fell by 2% compared with the previous
year. In 2016 the number of adoptions fell for the first time since 2011, by 12% and in 2017 the
number of LAC adopted has fallen again by 8% to 4,350.
There was a large rise in the number of unaccompanied asylum-seeking children in 2016 and this
number continued to increase in 2017. The number of LAC at 31 March 2017 who were
unaccompanied asylum-seeking children increased by 6% up to 4,560, compared to 4,300 in 2016
and up 134% from 1,950 in 2013.
Page 5
LAC Annual Report 2017 - 2018
Graph 1: Showing the increasing national LAC figures
(Ref: https://www.gov.uk/government/statistics/children-looked-after-in-england-including-
adoption-2016-to-2017)
2. National Guidance
Local authorities, commissioners and providers of health services are directed by primary legislation
and national policy and guidance to share responsibility in improving the health outcomes for
children and young people who are Looked After.
Key policy frameworks that inform and support this guidance are as follows:
• Healthy Child Programme (0 – 5) Pregnancy and the first five years of life (2018)
• New Social Work Act became law in 2017, within this it has extended the provision for Care
Leavers up until the age of 25 years. This came into effect in April 2018.
• Not seen, not heard: a review of the arrangements for child safeguarding and health care for
looked after children in England (CQC) (2016)
• Working Together to Safeguard Children (DFE 2015) was reissued and subsequently the NHS
England Accountability and Assurance Framework was also revised (NHS England 2015).
• Promoting the health and well-being of Looked after Children. Statutory Guidance for local
authorities, clinical commissioning groups and NHS England (DFES/DOH 2015) and the
intercollegiate role framework Looked After Children: Knowledge, skills and competencies of
health care staff (RCPCH 2015)
• Statutory Guidance on Promoting the Health and Well-being of Looked After Children (2015)
• NICE Public Health Guidance 28: Looked After Children and Young People (May 2015)
• NHS Outcomes Framework 2014 – 2015
• Children’s National Service Framework (NSF) (2014)
• The Children and Families Act (2014)
• The Care Act (2014)
Page 6

LAC Annual Report 2017 - 2018
• Ofsted report: From a distance: Looked after Children living away from their home area.
(April 2014)
• Public Health Outcomes Framework for England 2013 – 2016;
• NICE Quality Standard QS31: Quality Standard for the health and well-being of Looked After
Children and Young People (April 2013)
• The Health and Social Care Act 2012
• Healthy Lives, Brighter Futures: the strategy for children and young people’s health (2009)
• DH / DCSF Strategy on the health of children in the youth justice system (2009)
• High Quality Healthcare for All and World Class Commissioning (2008)
• Children and Young People in Mind: National CAMHS Review (2008)
2020 Workforce Strategy (2008)
3. Local Commissioner / Provider arrangements
Since March 2012, City Health Care Partnership CIC (CHCP CIC) has been commissioned by the Hull
Clinical Commissioning Group (CCG) to deliver the LAC service for all children within the looked after
care system.
Until 31st
March 2018 the Designated Nurse for LAC continued to carry out a role that would
ordinarily be carried out by a Named Nurse for LAC, a role that was not separately provided in
Kingston upon Hull. The Designated Nurse for LAC has been recruited to within the CCG and the role
of the Named Nurse for LAC is temporarily recruited to within CHCP CIC. The permanent post for
Named Nurse for LAC is due to be recruited to CHCP CIC in the near future.
4. 2017 CQC Inspection Action Outcomes
The 2016 - 2017 LAC annual report on the review of health services for Safeguarding and Looked
After Children Hull focused on the experiences and outcomes for children within the geographical
boundaries of the Local Authority area and reported on the performance of health providers serving
the area including Clinical Commissioning Groups (CCGs) and NHS England Local Area Teams (LATs).
An action plan was developed with the services involved in the inspection. The actions for the
Looked After Children’s Health Team (LACHT) were:-
• Strengthen the arrangements for using the Strengths and Difficulties questionnaires (SDQs)
in health assessments of LAC.
A dip sample of 34 Review Health Assessments (RHA) undertaken in March 2018 indicate that 84.8%
evidenced reference to the SDQ. The Named Nurse for LAC will continue to undertake 6 monthly
audits of the RHA through 2018-19 in order to monitor and evidence further improvements in the
use of SDQs.
Page 7
LAC Annual Report 2017 - 2018
Joint work between CHCP CIC and the Local Authority continues to strengthen and utilise the
information gathered within SDQ responses.
• Ensure the Part C health action plan within RHAs are routinely shared with LAC and their
foster carers.
The LACHT continued to investigate acceptable options for sharing a paper copy of the RHA with
carers or young people during 2017- 2018, however all practitioners undertaking RHAs with children
and young people discuss and agree the health action plan with the foster carer and child or young
person, at the time of the assessment. This process has progressed and since May 2018 and finalised
paper copies of the RHA are sent to young people and their carers as requested.
5. Integrated Looked after Children meetings (ILAC/Health & Social Care)
The Named Nurse and the LAC Administration Team facilitated these meetings which took place in
May 2017, July 2017, November 2017 and January 2018, allowing productive discourse on issues
including the late notification of Children and Young People (CAYP) becoming LAC and its impact on
the timely completion of assessments / Key Performance Indicators (KPIs).
The Named Nurse continues to work with the CCG and LA senior management to improve
representation and the frequency of these meetings. Since May 2018 the ILAC meetings have been
successfully re-established and well attended.
6. Performance
The performance data is provided 1 month retrospectively on a monthly basis, to the CCG as per
contractual requirements. On 31st
March 2017 the total number of Hull LAC was 758, which has
decreased from 774 LAC CAYP as of 31st
March 2017.
This figure includes Hull LAC placed in Hull, Hull LAC placed out of area (OOA) and OOA LAC placed in
Hull. The table below shows that by 31st
March 2018 there were less Hull LAC placed in Hull but
more Hull LAC placed out of area, including in the East Riding, compared to previous years. The
number of LAC from out of area placed in Hull has almost doubled in the last 2 years.
So although the Hull LAC numbers having decreased, the demand on services has remained due to
the sustained total number for the LACHT to provide services to.
Page 8

LAC Annual Report 2017 - 2018
Table 2: Showing the number of LAC placed by Hull Local Authority, both in Hull and OOA. The table
also reflects the number of OOA LAC placed in Hull.
Placement Area 2016
Total
Number of
Children
2017
Total
Number of
Children
2018
Total Number
of Children
Hull LAC placed Hull 444 463 417
Hull LAC placed OOA 218 231 243
OOA area LAC placed Hull 54 80 98
Total number of LAC for LACHT caseload 716 774 758
Graph 2: Showing the number of LAC placed by Hull Local Authority, both in Hull and Out of the
Local Area. The table also reflects the number of Out of Area LAC placed in Hull.
From 2017 the completion of Part A of the Coram BAAF IHA within the Local Authority’s Liquid Logic
data system has allowed for more comprehensive figures within this report than in previous years.
Table 3: Child in Need Code for LAC in Hull
Child In Need Code (Reasons for
Becoming LAC) 2016 2017 2018 As a % National
%
Child In Need Code (Reasons for Becoming LAC)
2016 2017 2018 2018 2017
Abuse or neglect 137 180 516 68.12% 62%
Child’s disability 7 6 15 1.97% 3%
Parental illness or disability 4 8 11 1.45% 3%
Family in acute stress 21 17 41 5.4% 8%
Family dysfunction 55 72 143 18.86% 15%
Socially unacceptable behaviour 3 1 5 0.65% 2%
Low income 0 1 3 0.39% -
Absent parenting 9 20 24 3.16% 7%
Total 236 305 758 100% 100%
Page 9

LAC Annual Report 2017 - 2018
Graph 3: Child in Need Code for LAC national % compared to Hull %
The ethnic origin data provided within the Liquid Logic data system is more condensed than in
previous years.
Table 4: Ethnic origin LAC Hull
ETHNIC ORIGIN OF LOOKED AFTER CHILDREN AT
31st
MARCH 2018
2018 %
White 682 89.97%
Mixed 27 3.56%
Asian or Asian British 17 2.24%
Black or Black British 5 0.66%
Other ethnic groups 27 3.57%
Total 758 100%
Page 10

LAC Annual Report 2017 - 2018
7. Initial and Review Health Assessments
From 1st
April 2017 – 31st
March 2018 there were a total of 190 LAC Initial Health Assessments (IHA)
in Hull and 658 Review Health Assessments (RHA) completed. In comparison to the 2016-2017
figures this is a 14.7% increase in LAC IHA and a 35.3% increase in RHA completed.
This significant increase in demand has had a noticeable impact on achieving set timescales. For the
year of 2017 – 2018, 51% in total CAYP were offered an appointment for their Initial Health
Assessment within 28 days of becoming Looked After.
Of the 51% who were offered IHAs within timescales, 71% were completed within timescales,
excluding those outside the control of CHCP, for example incomplete parental consent for medical
assessments, late notification of becoming Looked After or cancellation of the appointment.
In regards to RHAs, 100% of LAC aged 0 – 4 years were offered an appointment within 6 months of
their last health assessment and 99% of LAC aged 5 – 18 years were offered an appointment within
12 months of their last health assessment.
Graph 4: Number of LAC who had an IHA per month from March 2017 – February 2018
Page 11

LAC Annual Report 2017 - 2018
Graph 5: Percentage of Initial Health Assessments offered to LAC within 28 day timescale
8. Late notifications
CHCP LACHT administration team record within the child’s electronic care record (ECR) when a child
or young person becomes Looked After. It is also recorded if the notification period is over the
agreed 5 working day notification period given by the Local Authority (LA).
The breach information is provided to the Local Authority to investigate why the notification was
sent to the LACHT outside of the agreed 5 working day notification period. The LA findings are given
to Business Intelligence to feedback to the CCG.
9. Consent
There has been a significant improvement in the receipt of the Coram BAAF consent form from the
Social Work teams. As mentioned earlier in the report, there are still some instances where
appointments have had to be cancelled due to the lack of parental consent, but these instances have
reduced from previous years.
As already discussed, consent to share Part C of the RHA has been made explicit, and the consent
form amended accordingly. Practitioners are now routinely sharing the Part C document with the
young people (if over 13 with capacity to consent).
Page 12

LAC Annual Report 2017 - 2018
10. Dental Health
In 2017 – 2018, 60.2% of CAYP were already registered with a dentist on entering the LAC system,
this increased to 86.9% at their RHA 6 or 12 months later as appropriate to age. National data states
that 58.2% of the child population were seen by an NHS dentist in the 12 months up to 30th June
2017.
Reference: ( https://digital.nhs.uk/data-and-information/publications/statistical/nhs-dental-
statistics/nhs-dental-statistics-for-england-2016-17 )
Graph 6: Dental registration for LAC in Hull
It can be seen from table 5 that although the Hull statistics are better than the reported national
statistics there remains scope for further work in promoting dental care for LAC. This will continue to
be addressed by the LACHT.
11. Immunisations
In Hull in 2017 -2018, 63.4% of LAC’s immunisation status were up-to-date when they had their IHA,
which is a drop compared to recent years. By the first RHA 88.8% of LAC’s were up to date with
immunisations, an increase compared to the 2016 – 2017 figure. Hull’s figures remain lower than
national trends.
National data shows that in 2016-17, four out of the six routine vaccinations at 1 and 2 years showed
small decreases in coverage compared to 2015-16. This includes coverage for the Measles Mumps
and Rubella (MMR) which decreased in 2016-17 for the third year in a row. Coverage for this vaccine
is now at 91.6 per cent, at a similar level to that reported in 2011-12.
Page 13

LAC Annual Report 2017 - 2018
Nationally 93.4 per cent of children reaching their first birthday were reported to have completed
their primary DTaP/IPV/Hib course (three doses). This compares with 93.6 per cent in 2015-16.
National coverage figures reported for the Diphtheria, Tetanus, Pertussis and Polio (DTaP/IPV)
booster as measured at 5 years show a decrease in 2016-17 for the fourth year in a row.
The LACHT continue to advise carers to attend the child’s GP for immunisations. All LAC
immunisation status is reported within the initial LAC review meeting health report and updates are
provided at subsequent LAC review meetings. The CHCP CIC School based immunisation team
immunise children and young people at home where required, including the residential looked after
children’s homes.
Graph 7: Immunisation status of Hull LAC
12. Sexual Health
The LACHT continue to work with Specialist Sexual Health Services for young people. A central
telephone number for both client and professional referrals is staffed Monday-Friday 9am-5pm and
an answer-machine is available for referrals at all other times.
This ensures that the referrals into Sexual Health services are dealt with swiftly and efficiently. Joint
visits between practitioners are arranged where it is felt that this will help facilitate engagement
with young people. Proactive information sharing has developed considerably between the two
teams, supported by CHCP CIC safeguarding team.
Page 14
LAC Annual Report 2017 - 2018
Referrals made by Sexual Health Services to Children’s Social Care access and assessment team are
now saved on the child’s ECR. The Specialist Sexual Health Services for young people are now invited
to child protection conferences.
A standard operating procedure (SOP) supports these processes and facilitate the timely sharing of
relevant information and early identification of risk and/or sexual health need for Hull LAC and other
vulnerable young people.
13. Child Exploitation
The Child Exploitation Team is now a permanent service within Children’s Social Care and work has
been completed on the Risk Indicator Tool (RIT) which is now firmly embedded in practice.
CHCP CIC Safeguarding Practitioners attend the MACE meetings and liaise with the LACHT in regards
to LAC where appropriate.
The Specialist Sexual Health Service practitioners have access to the ECR. This ensures that if a young
person accesses the service, relevant practitioners will be aware if they subject to the MACE process.
14. Emotional Health
The LACHT administrative staff circulate a set of SDQs for completion 3 months after a child or young
person becomes Looked After, to facilitate a baseline assessment for the Social Worker (SW) and
Independent Conference Reviewing Officer (ICRO) about the emotional health of the child or young
person entering the Looked After system.
A second set of SDQs are sent out to correspond with the first RHA to enable the Social Worker to
demonstrate the emotional health status of children as they come into care and compare this with
the relevant score after being in the Looked After system for 6 months or a year, depending on the
age of the child. The LACHT use the SDQ responses to inform a holistic health assessment for LAC. If
the SDQ is not available to inform the RHA, this is included as an outstanding action in the child /
young person’s health plan.
Where a child or young person is assessed as having an emotional health need requiring extra
support they will be offered additional contacts by the LACHT. If the assessment deems that
specialist support is required a referral to CAMHS will be made.
All referrals to CAMHS are now made electronically. The 9 pathways that have been developed by
CAMHS are embedded into the screening tools within the child or young person’s ECR. There is a
hyperlink into the electronic referral system so that CHCP can report on the number of referrals
made into CAMHS, improving the quality of information overall.
Page 15

LAC Annual Report 2017 - 2018
15. Substance Misuse
When CAYP are assessed by the LACHT as having an identified need around substance misuse they
are automatically referred to REFRESH, the adolescent substance misuse service. The LACHT
continually work with REFRESH to strengthen the existing referral and assessment pathways. Joint
visits between practitioners are arranged where it is felt that this will facilitate engagement with
young people.
16. Looked After Children and Young People’s Health Team (LACHT)
Table 5: Number of LAC within on LACHT caseload on 31st
March 2018
Hull LAC placed in Hull Boys Girls
Age 0 -1 years 39 18 21
Age 1 – 4 years 147 80 67
Age 5 – 9 years 179 95 84
Age 10 – 15 years 268 153 115
Age 16 – 17 years 125 67 58
Graph 8: Percentage of LAC on LACHT caseload on 31st March 2018
Page 16

LAC Annual Report 2017 - 2018
In August 2017 the post of Designated Nurse for LAC was reappointed. During 2017 – 2018
processes have been developed to enhance efficiency in working practice.
The LAC RHA document in use has been updated to the Coram BAAF 2017 version. The RHA
documents are now completed by the LACHT practitioners directly within the LAC ECR. This change
in process has reduced the number of administrative steps, thereby reducing the length of time the
LACHT practitioners and administrative staff need to spend on the process.
The SOP for ECRs of adopted children has been completed and ratified ensuring that when a child is
adopted their new ECR is created and the old ECR is ended securely guaranteeing there are no
familial links between each ECR.
LAC Review Meeting reports have been standardised to ensure all practitioners include essential
information for ICRO’s and SW’s. Training has been provided for new practitioners within the LACHT
in completing the RHA documents to an exemplary standard.
The Designated Nurse attended ICRO team meetings on a quarterly basis to create a better
understanding of roles, enhance communication and provide updates to the ICRO’s in regards to
changes in practice within the LACHT. The Named Nurse for LAC will continue this meeting
attendance through 2018 – 2019.
Professional links have been strengthened between the Designated Nurse for LAC and all the CAYPs
Social Care Teams as well as the ICROs. This has had a significantly positive impact on
communication pathways. Social Care Team administrators and many of the SW’s have the direct
contact details for the LACHT, including the LACHT administrative team and the Designated Nurse
for LAC. They are able to directly discuss queries or issues with regards to the health or well-being of
any LAC or foster placement and are better able to co-ordinate professional meetings. This
professional relationship has continued with the Named Nurse for LAC.
Several members of the LACHT have been trained as Foster Panel members. Their attendance at
Foster Panel has given them greater insight into the legislative requirements for foster carers and
foster placements. This knowledge and practice has enhanced their work when supporting LAC and
carers.
Several members of the LACHT attended a Foster Carer Event. This allowed the LACHT to highlight
their extensive role in supporting foster carers and LAC. The event generated new referrals into the
team for support from carers, evidencing the success in raising the team profile.
LACHT members have been invited to attend Hull foster carer support groups in both Hull and East
Yorkshire. This will allow practitioners to provide up to date health advice to carers and continue to
raise the profile of the LACHT’s role.
Links have been made with the Local Authority training team and plans are in progress to provide
foster carers with health training updates through 2018 – 2019.
Nationally the term “LAC” is being phased out in favour of the term Children Looked After (CLA). This
term is being embedded in practice by the LACHT, the ICRO’s and SW’s in the Local Authority. The
2018 -2019 LAC Annual Report will reflect this in the terminology used.
Page 17

LAC Annual Report 2017 - 2018
The 2017 CQC review of health services in Safeguarding and Looked After Children’s services in Hull
highlighted some excellent work offered within the skill mix team including:-
• A strong adolescent offer which enables effective safeguarding and provides good
opportunities for identifying and responding to additional needs.
One example of such work was engagement with a young person in foster care who had tried to
conceal an unplanned pregnancy. The LACHT practitioner was able to co-ordinate an effective
support plan for the young person ensuring appropriate professionals were kept informed as
needed.
Another example was the support given to a young person identifying themselves as transgender.
The LACHT practitioner was able to make a direct referral to the Tavistock Centre, a Gender Identity
Development Service (GIDS) and reassure the young person about the counselling and assessment
process.
• Good relationships with education, good knowledge of missing from home and home
educated children.
There remains a dedicated School Health Practitioner for home educated
CAYP. The pop-in clinics at the pupil referral unit, which are attended by a number of LAC continue,
and are an excellent forum for addressing health needs.
• Regarding the Health and Development Practitioners (HDP) the inspectors saw some good
outcomes and examples with good direct engagement with young people.
The LACHT HDPs have maintained monthly staff liaison meetings with the children’s homes within
the city. This has proven useful in partnership working and information sharing for safeguarding
purposes.
Some of the exceptional work provided by the HDPs within the LACHT team include:-
A relative carer was provided with some nutritional advice and support for her 2 grandsons, one was
under-eating and the other was over-eating. After several visits the carer was pleased with the
effectiveness of the strategies she had been given for both the young people, she was also proud to
tell us that having followed the advice she had lost 2 stone.
A HDP successfully encouraged a vulnerable young person to receive contraception. This young
person had adamantly refused to engage with the Specialist Sexual Health Services prior to this.
• An improved relationship with CAMHS. In 2017 the LACHT have held regular monthly peer
supervision meetings with the CAMHS practitioners. All practitioners within the LACHT continue to
have telephone consultations with the LAC psychologist employed within the Local Authority, in
respect of individuals they are jointly working with.
Page 18

LAC Annual Report 2017 - 2018
An example of a positive outcome would be a referral made for a young person to CAMHS being
accepted, with an expected consultation within 7 days of the referral, evidencing the LACHT
practitioners’ skill and accuracy in the assessment of emotional health and well-being of children
and young people.
• Good quality LAC health assessments. Assessments were of a high quality and focussed on
the needs of the children, they had smart outcomes, showed continuity of care, were child focussed,
with the child at the heart of the assessment.
Some examples of the effectiveness of quality assessments include:-
A LACHT practitioner identified a young person with unusual growth and referred him to the
endocrinologist. Further tests identified a significant endocrine problem.
The persistence of reappointing and rearranging a RHA for a young person for 5 months. The young
person would agree to have the assessment, but cancel at short notice. Despite this the practitioner
continued to offer support, at the LAC review meeting, the young person happily agreed to remain
after the meeting in order for the practitioner to undertake the outstanding RHA.
17. Service User Feedback
At RHAs, the Health Assessment Feedback forms are left with carers and young people aged 11 years
and over to complete and send back in a stamped addressed envelope allowing anonymous
responses. There were 244 collated feedback forms for 2017 - 2018.
Table 6: Feedback Form responses from RHAs How much do you agree with the following statements Health
Visitors
School
Nurses
Confidentiality was discussed with me 94.4% 93%
I felt I could discuss sensitive issues with the nurse 100% 89.44%
The nurse listened to me 100% 100%
The nurse was friendly 100% 100%
I would see the nurse again for support 97.76% 94.72%
I would recommend the nurse to a friend if they had
health concern
98.88% 90.76%
Page 19

LAC Annual Report 2017 - 2018
Graph 9: Feedback form response at RHA
Comments from Feedback Forms at RHA
• Very friendly and easy to talk to
• Prompt on the visit, structured questions so I feel we covered everything, I have contact
phone number if needed, and nurse contacted me to arrange appointment, very happy
child’s info. Extremely professional and offered good advice.
• Thank you come again!
• I felt totally at ease with the nurse and felt she listened and was interested in my views and
concerns, she was very professional and explained things I didn’t not understand in a way
that made sense to me. Thank you. The person I was talking to was nice.
• The nurse turned up on time, she was very friendly and professional
• Every question answered fully
• Thank you, you really took time listening to child as she does struggle at times
• Nurse is very friendly and easy to talk to about anything, she is able to put young person at
ease.
• I hope that next time I have a health meeting I have the same nurse
• Felt very comfortable, nurse was very helpful and easy to talk to and discuss life events /
problems
• She was really nice and comfortable / easy to talk to
Page 20
LAC Annual Report 2017 - 2018
18. Summary
The number of LAC within Hull for as at 31st March 2018 decreased compared to 31st March 2017,
but remains significantly higher than previous years. The upward trend in Hull mirrors an upward
trend nationally. This trend may be influenced by the national reduction in adoption figures.
During 2017 - 2018 there was a 14.7% increase in LAC IHAs and a 35.3% increase in RHAs. These
figures have had a significant impact on performance figures and work continues within the
Community Paediatric Team to meet the increase in demand.
During 2017 there continued to be significant difficulties created by late notification of LAC status
for CAYP. It has been recognised that the late notifications to LACHT by the social care teams has
had a significant impact on enabling the IHA’s to be completed in a timely manner. The issue was
escalated to Hull CCG through the contracting report and to the Local Authority through the ILAC
meetings. LACHT and the Local Authority continue to work towards solutions to this issue.
The LACHT have undergone significant changes in staffing structure during 2017 – 2018, leading to
the Designated Nurse for LAC during that time period managing a LAC caseload alongside
undertaking the role requirements. Significant effort has been made to ensure this had a minimal
impact on performance. The role of Designated Nurse for LAC was transferred to the CCG on 1st
April
2018, with the Named Nurse for LAC role remaining within the provider service as recommended by
the unpublished joint agency pilot inspection in 2014, previously referred to in the 2016 – 2017 LAC
Annual Report.
The actions for the LACHT from the 2017 CQC review of health services in Safeguarding and Looked
After Children’s services in Kingston upon Hull have been met. The excellent work provided by the
LACHT highlighted within the 2017 CQC review has been embedded into practice and can be
evidenced through client feedback and SW feedback.
Due to changes within the LA’s data systems and completion of the Coram BAAF IHA Part A
document, data for reasons for LAC entering the care system could be included in this report. It can
be seen in Table 3 of the report that abuse or neglect is by far the most common reason within Hull
at 68.12%. The next most common reason is recorded as family dysfunction at 18.86%. These figures
mirror national trends. Information from the Local Authority indicates that 89.97% of LAC in Hull on
31st
March 2018 were of white ethnic origin. The Local Authority were unable to provide a separate
figure for unaccompanied asylum seeking children within Hull for the 2017 – 2018 time period.
Dental registration statistics for Hull are similar to national statistics. Improvement in dental
registration after a child or young person has entered the care system are similar to the 2016 – 2017
level. The rise from 60% at IHA to 86.9% at RHA evidences the dental health education that is
reinforced by the LACHT.
Page 21

LAC Annual Report 2017 - 2018
Immunisations statistics for Hull are lower than the national average, but 88.8% of LAC have their
immunisations brought up to date by the first RHA, evidencing the effectiveness of the advice and
information provided to SWs, ICROs and foster carers at LAC Review meetings by the LACHT.
Effective partnership working is embedded in practice with the LACHT and can be evidenced through
the positive outcomes for LAC. The LACHT continue to work closely with the Specialist Sexual Health
Services, REFRESH, CAMHS and all the SW teams.
The LACHT ensure promotion of the health and well-being of all Looked After CAYP at every contact
made with the CAYP as well as the professionals involved in each CAYP’s life. The team is proud of
the recognition of this perseverance through the positive feedback they receive from the CAYP, SWs
and foster carers.
13. Recommendations
The appointment of the Designated Nurse for LAC within the CCG and the forthcoming permanent
appointment of the Named Nurse for LAC will facilitate a continued Improvement of the health
profiling for Looked After CAYP.
The Designated Nurse and the Named Nurse for LAC will continue to work with the Local Authority
to improve the timeliness of the notification process for Looked After Children.
The Designated Nurse and the Named Nurse for LAC will continue to work with the Local Authority
to transfer the responsibility for administration of the Strengths and Difficulties Questionnaires back
to the CAYP Social Care Teams. See Appendix one Action plan 18/19.
The LACHT will continue work with foster carers on the importance of promoting bonding and
attachment in looked after children. A formalised training package for foster carers will be
implemented jointly with the Local Authority Training Department. See Appendix one Action plan
18/19.
Page 22
LAC Annual Report 2017 - 2018
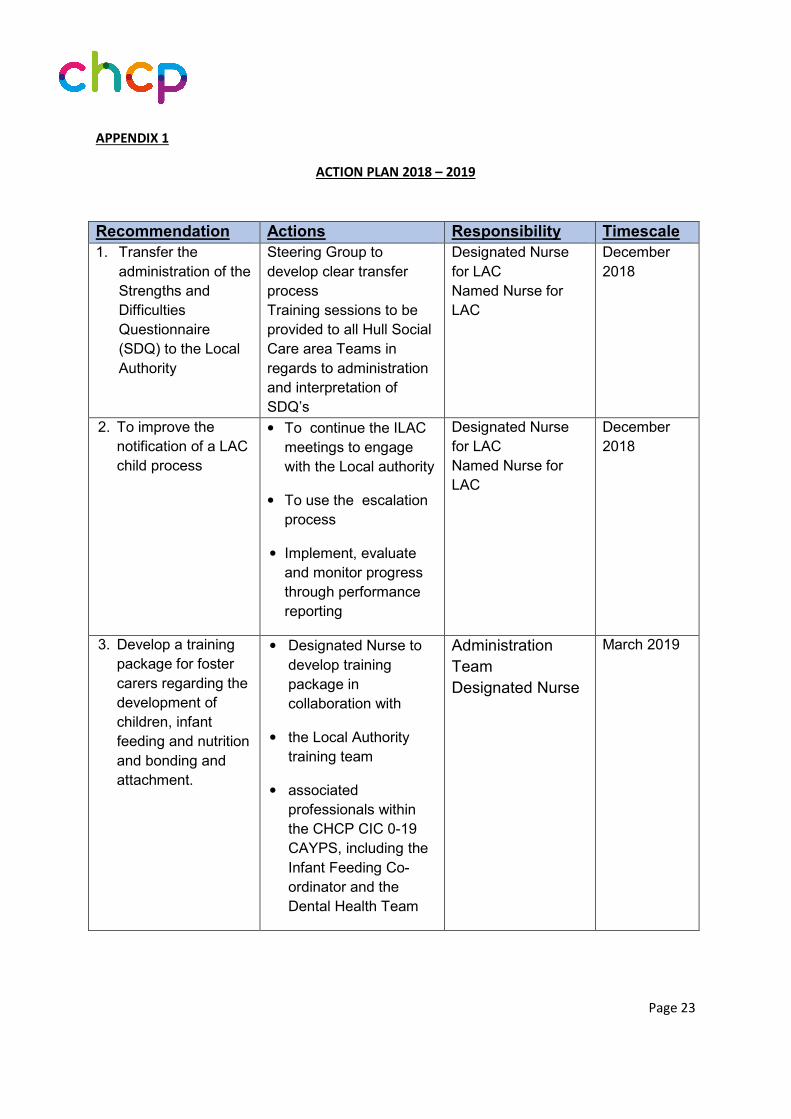
APPENDIX 1
ACTION PLAN 2018 – 2019
Page 23
Recommendation Actions Responsibility Timescale
1. Transfer the
administration of the
Strengths and
Difficulties
Questionnaire
(SDQ) to the Local
Authority
Steering Group to
develop clear transfer
process
Training sessions to be
provided to all Hull Social
Care area Teams in
regards to administration
and interpretation of
SDQ’s
Designated Nurse
for LAC
Named Nurse for
LAC
December
2018
2. To improve the
notification of a LAC
child process
• To continue the ILAC
meetings to engage
with the Local authority
• To use the escalation
process
• Implement, evaluate
and monitor progress
through performance
reporting
Designated Nurse
for LAC
Named Nurse for
LAC
December
2018
3. Develop a training
package for foster
carers regarding the
development of
children, infant
feeding and nutrition
and bonding and
attachment.
• Designated Nurse to
develop training
package in
collaboration with
• the Local Authority
training team
• associated
professionals within
the CHCP CIC 0-19
CAYPS, including the
Infant Feeding Co-
ordinator and the
Dental Health Team
Administration
Team
Designated Nurse
March 2019
LAC Annual Report 2017 - 2018
APPENDIX 2
IHA Quality Assurance data from Designated Doctor for LAC
The Designated Doctor for Hull Looked After Children undertakes an annual audit of a random
sample of Initial Health Assessments. From this audit, recommendations are shared with the
Community Paediatricians to ensure an excellent standard is maintained when completing the IHA
documents.
Dr. Grover undertook the audit in November 2017. Utilising a formatted quality assurance tool, Dr.
Grover’s analysis was as follows:-
Date; those present; sources of information; consent detail; background information; current health
and developmental status; emotions/ behaviour/mental health and lifestyle; quality of health plan;
summary and contact information.
Dr. Grover noted that the standard for adequacy of the care plan recommendations was 100%. Dr.
Grover’s recommendations from the audit of the IHA’s for age 10 -17 years were as follows:-
• Health recommendation should include a time limit for registration with GP/ dentist.
• Outstanding immunisations should be specifically identified
• The Health Care plan should address all issues uncovered in discussion including emotional
and mental health; and education
• Appropriate professional responsible for identified actions should be named
• Time targets should be specified for each task arising from issue(s) identified
Dr. Grover noted that the standard for adequacy of the Care Plan recommendations was 100%. Dr.
Grover’s recommendations from the audit of the IHA’s for age 0 - 9 years were as follows:-
• Even if the parent information is available but there is no consent to share this information,
it should be clearly stated as such on part C.
• If parent information is not available, a request for the SW to supply, within the Health Care
Plan.
• Parental health information can be directly obtained from them if present at the health
assessment. Similarly Maternity history too can be obtained directly from mother when
present.
• Neonatal screens’ reports should be included as part of birth information.
• Health recommendations should include a time limit for registration with GP/ dentist.
Page 24

LAC Annual Report 2017 - 2018
The LACHT have noted that the standard of IHA document information has improved since the last
audit with full health chronologies where appropriate and clear recommendations with specific
timescales. This ensures that information shared at LAC review meetings is precise and roles and
responsibilities are unambiguous.
Page 25