annual results and impact evaluation workshop for rbf - day eight - learning from experience -...
TRANSCRIPT

Operational Lessons from RBF
H E A LT H R E S U LT S I N N O VAT I O N T R U S T F U N D
Learning from Implementation
Petra Vergeer & Hadia Samaha

The Why and How of Operational Lessons
• Review of ongoing PBF operations suggests some useful lessons
• Focusing on the most important lessons will facilitate enhanced design and implementation
2

Lesson “Math-Phobes of the World Unite!”
– Use your data
• Data is vital but under-utilized, despite a lot of effort invested into collecting, verifying and putting payment data on the web
17

Coverage of full vaccination among children under 1
0 10 20 30 40 50 60 70 80 90
100
4 1 2 3 4 1 2 3
Benin Burkina Faso Cameroon Kenya Nigeria Zambia Zimbabwe
%

Total quality score in health facilities
0
20
40
60
80
100
Burkina Faso
Benin Cameroon Kenya Nigeria Zambia Zimbabwe
%
Scores are averages of health centers and hospitals, technical and subjective where applicable Each bar represents a quarter of implementation

Internet applications with public front-end displaying performance & financial information
18
Burundi
Benin
Nigeria

3 services absorbing largest share of payment
7
OP >5 11%
OP <=5 15%
Inst. Delive
ries 17%
Others
57% Burundi
Zambia
Cameroon
Zimbabwe
OP contac
t 6% Inst.
Deliveries 35% FP
40%
Others 19%
OP contact
35%
Inst. Deliveri
es 15%
FP 21%
Others 29%
OPC 21%
Hosp. days 15%
VCT 12%
Others 52%
Figures reported are averages of all quarters to date

Strengthening work on administrative data 1. Regularly monitoring program progress to identify candidates for
adjustment (indicators and tools) 2. Taking advantage of HMIS data to compare with control facilities
and assess performance on non-incentivized services 3. Developing online dashboard to facilitate use of data and
promote transparency 4. Developing automated data analysis software to lessen burden
of data analysis for teams and encourage focus on results (ADEPT RBF)
8

Lesson “Keep moving the goalposts!”
Continuous Quality Improvement (CQI) implies Changing the Quality
Indicators
• Many facilities make rapid improvements in quality and then plateau
6

At different levels: • Facility Staff (managers, providers, staff -hospitals and clinics):
Need quality measures to assess and continuously improve services. Is care improving?
• Regional/District & Program Managers: Need measures to assess and continuously strengthen essential system functions (e.g. competent workforce). Are essential system functions performing to standard?
--------
Understanding what different stakeholders want: Clients (users of care) National Policy-makers (value, policy) Global Stakeholders (leadership, advocacy, accountability)
Integrating Quality into RBF Projects: Prioritizing Health Conditions/Services for Improvement

Consider phasing improvement priorities: “impossible to improve everything at once”
Involve local and international experts to: • Review country standards against global evidence: evidence is constantly changing • Distill standards into minimum “intervention bundles”: focus attention on essential
high-impact interventions • Illustrative quality of care process measures based on minimum standards:
o % cases adherent with standards – “all or nothing adherence” (e.g. % PPH cases managed per minimum standard; % cases pediatric pneumonia treated per standard)
o Average % adherence with minimum standards (e.g. average % adherence with newborn sepsis case-management standards; N=30 cases)
Integrating Quality into RBF Projects: Selecting standards and Defining Quality of Care Measures
Illustrative quality measure: Quality of Partogram Completion (not so simple!)
Quality Measure Opera/onal Defini/on
% partograms in last quarter completed per standard
NUMERATOR: Number partograms documen/ng cervical dila/on, maternal BP, pulse, temperature at admission and at least every 4 hours un/l delivery
DENOMINATOR: Total number of partograms reviewed

Lesson No commodities : No program
Worry about supply chains and drug availability !!!!!!
6

Improving Medicine supply chains to debottleneck RBF Programs
• A useful first step is to diagnose the root causes of poor availability using an appropriate diagnostic tool. Poor quantification/requisitions, lack of transport, and procurement delays are common reasons.
• Range of options for RBF programs to tackle these challenges. E.g., better requisitioning tools, contracted transport for obtaining supplies from district or regional stores, negotiated prices with private sector supply sources etc.

Lesson Seeing is Believing !!!!!
Verify and Counter Verify to Ensure You pay for real outputs !!!!
6
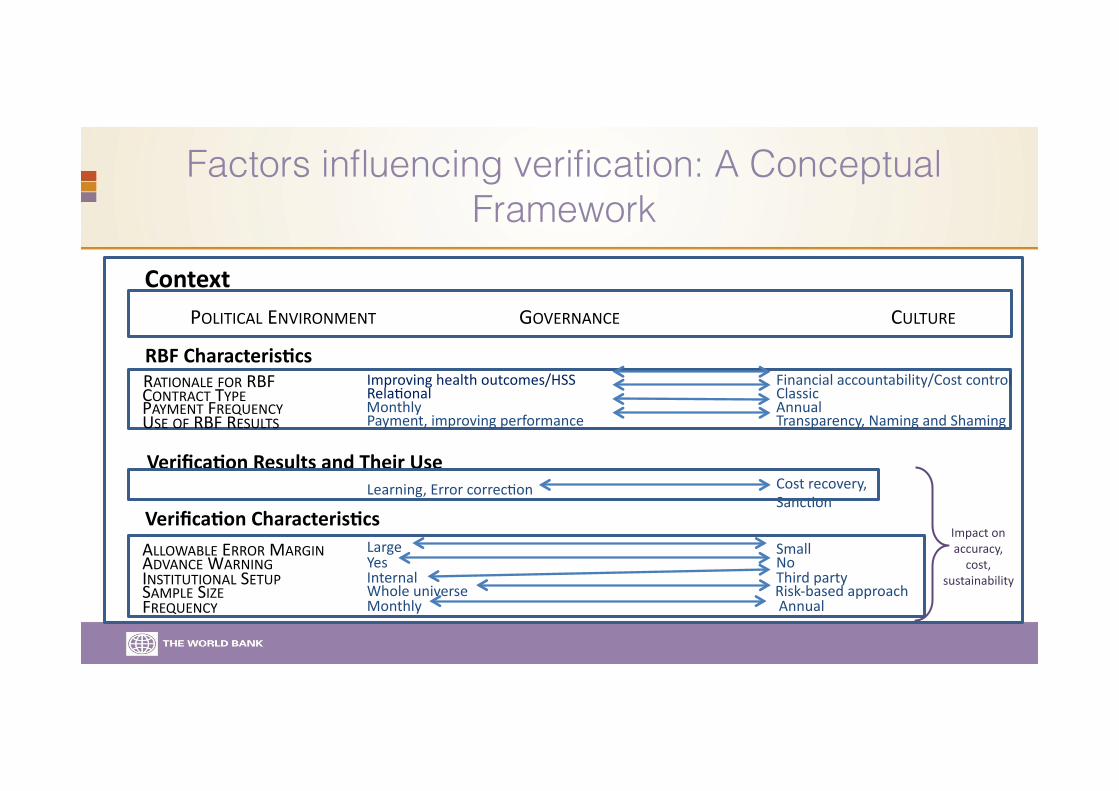
Factors influencing verification: A Conceptual Framework
Context
Verifica/on Characteris/cs Impact on accuracy, cost,
sustainability
RBF Characteris/cs RATIONALE FOR RBF CONTRACT TYPE
USE OF RBF RESULTS
Improving health outcomes/HSS RelaFonal
Payment, improving performance
Financial accountability/Cost control Classic
Transparency, Naming and Shaming
Monthly Annual
Yes Large
Whole universe Risk-‐based approach Internal
Verifica/on Results and Their Use
FREQUENCY
ALLOWABLE ERROR MARGIN
SAMPLE SIZE INSTITUTIONAL SETUP ADVANCE WARNING No
Small
Third party
Learning, Error correcFon Cost recovery, SancFon
PAYMENT FREQUENCY Monthly Annual
POLITICAL ENVIRONMENT GOVERNANCE CULTURE

Key Recommendations Verification 1. Consider context to determine whether merging
functions is appropriate (be mindful of conflict of interest)
2. Analyze and use data available from verification and counter-verification
3. Verification strategies should be dynamic, not static, and use a risk-based approach

Lesson Capable People Matter !!!!!
Invest in Your RBF Institutions & Teams
6

Scaling up capacity building and human resources for RBF and its sustainability
• South-South TA with appropriate backstopping can lead to a successful home bred PBF pilot experience
• Faculty members in Medical Schools are keen to embrace PBF, teach PBF and spread its principles and success stories, provided that they got the opportunity to be exposed to PBF in theory and in practice
• Creating local contract management and verification capacity by selecting local non-governmental organizations and training and coaching them in PBF can be an attractive strategy in some countries.
• Use of locals has made it possible to increase knowledge and capacity on RBF, research, and MNCH in-country. Ensure there is no bias and missing out on other international experiences

Lesson Let RBF Leave its Mark !!!
Think beyond tomorrow
6

RBF Institutional Set up and Ensuring Buy in
• There are 3 main stages in the integration of RBF into a national health system
Adoption: to move from PILOT to SCHEME Institutional: to move from SCHEME to POLICY PERPETUATION: to move from POLICY to SYSTEM
• Key issues are in terms of: Actors, Resources (including $$$$), RBF design, and Process
• Context shapes the trajectory