antepartum (prenatal)mscqw.org/wp-content/uploads/preceptor-guide-for-ld-externs-2019.pdf ·...
TRANSCRIPT

1 | P a g e S T U D E N T N A M E :
MKF, 2019
MATERNITY AND WOMEN’S HEALTH CARE CLINICAL MODULE
ANTEPARTUM (PRENATAL)
Antepartum: pregnancy, prenatal period, before the baby is born
Corpus luteum: a temporary endocrine structure involved in ovulation and early pregnancy. Supports the early pregnancy by producing progesterone until the placenta matures.
Pelvis: The bony pelvis protects the pelvic structures, accommodates the growing fetus in pregnancy and anchors the pelvic support structures. The true pelvis is the lower, curved bony canal and the size and shape are vital to the progress of the fetus during birth. The false pelvis is the upper portion of the pelvis.
Pelvic types: see table
Cotyledons: Retained placental tissue is associated with postpartum hemorrhage and infection. The maternal surface of the placenta should be inspected to be certain that all cotyledons are present. Then the fetal membranes should be inspected past the edges of the placenta.
Birth Plan: a document that lets the medical team know the patient’s preferences for things such as how to manage labor pain.
Certified Nurse Midwife (CNM): a registered nurse with additional training as a midwife who is certified to deliver infants and provide prenatal and postpartum care, newborn care, and some routine care (as gynecological exams) of women.
2 | P a g e S T U D E N T N A M E :
MKF, 2019
Doula: also known as a birth companion, birth coach or post-birth supporter, is a non-medical person who assists a woman before, during, or after childbirth, to provide emotional support and physical help if needed. They also may provide support to the mother's partner and family. They CAN NOT deliver a baby.
Rh negative factor: Rh sensitization can occur during pregnancy if you are Rh-negative and pregnant with a developing baby (fetus) who has Rh-positive blood. ... But if you get pregnant again with an Rh-positive baby, the antibodies already in your blood could attack the baby's red blood cells. Teaching is VITAL!
Abortion: termination of a pregnancy before 20 weeks gestation
Spontaneous (SAB): the natural death of an embryo or fetus before it is able to survive independently. Some use the cutoff of 20 weeks of gestation, after which fetal death is known as a stillbirth.
Missed: a type of early pregnancy loss in which the dead embryo or fetus is retained in the womb for a period of time, during which the usual symptoms of miscarriage may not occur.
Elective (ETOP): elective termination of pregnancy.
Gestation: the process of carrying or being carried in the womb between conception and birth.
Preterm labor (PTL): A normal pregnancy lasts about 40 weeks. Occasionally, labor begins prematurely, before the 37th week (36 6/7weeks) of pregnancy. This happens because uterine contractions cause the cervix to open earlier than normal. Consequently, the baby is born premature and can be at risk for health problems.
Gravida: describes the total number of confirmed pregnancies that a woman has had, regardless of the outcome.
Nulligravida: a woman who has never been pregnant
Primigravida: a woman who is pregnant for the first time.
Multigravida: woman who is or has been pregnant for at least a second time.
Para: the number of births that a woman has had after 20 weeks gestation
3 | P a g e S T U D E N T N A M E :
MKF, 2019
Nullipara: a woman that is pregnant but has never given birth.
Primipara: a woman who is giving birth for the first time.:
Multipara: a woman who has had more than one pregnancy resulting in viable offspring.
Stillbirth: the birth of an infant that has died in the womb (strictly, after having survived through at least the first 28 weeks of pregnancy, earlier instances being regarded as abortion or miscarriage).
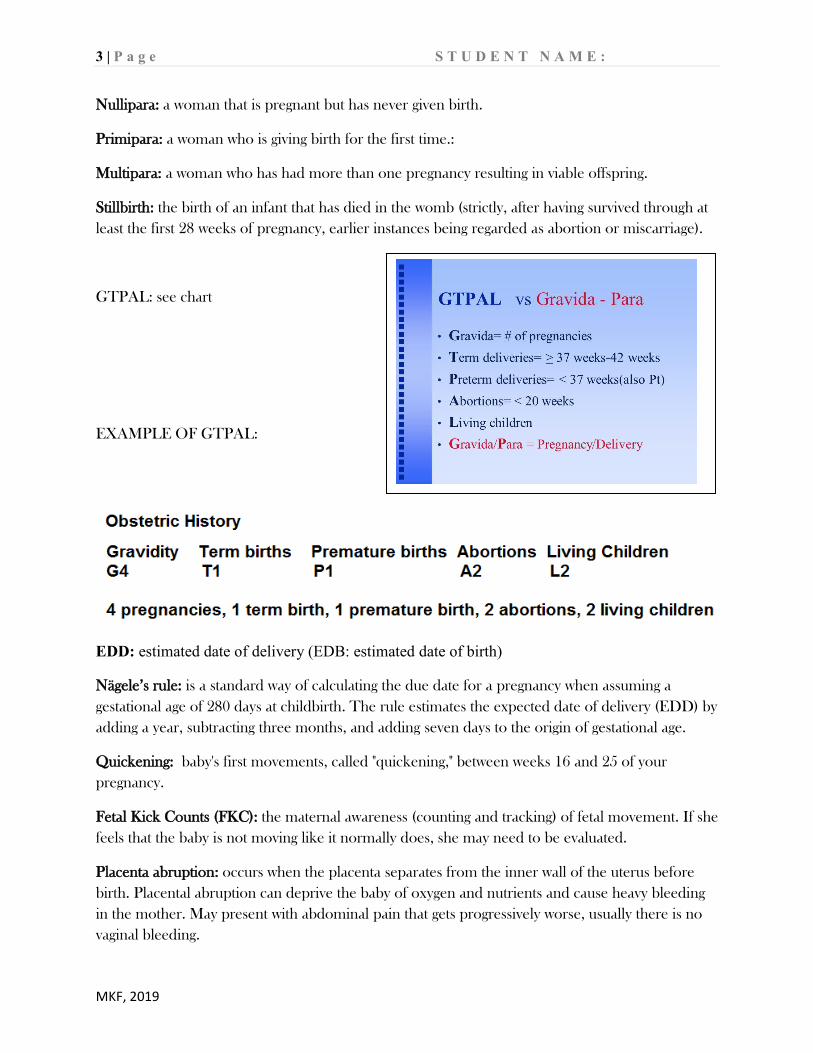
GTPAL: see chart
EXAMPLE OF GTPAL:
EDD: estimated date of delivery (EDB: estimated date of birth)
Nägele’s rule: is a standard way of calculating the due date for a pregnancy when assuming a gestational age of 280 days at childbirth. The rule estimates the expected date of delivery (EDD) by adding a year, subtracting three months, and adding seven days to the origin of gestational age.
Quickening: baby's first movements, called "quickening," between weeks 16 and 25 of your pregnancy.
Fetal Kick Counts (FKC): the maternal awareness (counting and tracking) of fetal movement. If she feels that the baby is not moving like it normally does, she may need to be evaluated.
Placenta abruption: occurs when the placenta separates from the inner wall of the uterus before birth. Placental abruption can deprive the baby of oxygen and nutrients and cause heavy bleeding in the mother. May present with abdominal pain that gets progressively worse, usually there is no vaginal bleeding.

4 | P a g e S T U D E N T N A M E :
MKF, 2019
Placenta Previa: a condition where the placenta lies low in the uterus and partially or completely covers the cervix. The placenta may separate from the uterine wall as the cervix begins to dilate (open) during labor. May present with painless vaginal bleeding. DO NOT perform a vaginal exam on a patient with placenta previa.
Group B Streptococcus (GBS): is a type of bacterial infection that can be found in a pregnant woman's vagina or rectum. This bacteria is normally found in the vagina and/or rectum of about 25% of all healthy, adult women. Women who test positive for GBS are said to be colonized. Patients who are positive for GBS, need antibiotics begun on admission.
Treatment with antibiotics during labor to help prevent GBS from being passed to the baby. The antibiotics work only if they are given during labor. If treatment is given earlier in pregnancy, the bacteria may regrow and be present during labor. Penicillin is the antibiotic that is most often given to prevent early-onset GBS infection in newborns.
INTRAPARTUM (LABOR & BIRTH) Intrapartum: period during labor and birth
Placenta: vascularized disk-shaped organ that implants in the thick muscular wall of the upper uterine segment. Organ for maternal-fetal gas and nutrient exchange. After the birth of the fetus, the placenta is expelled.
Umbilical cord: connecting stalk between the fetus and placenta that carries maternal nutrients and oxygen to the fetus. The umbilical cord is a spiral stalk with 2 arteries and 1 vein surrounded by connective tissue called Wharton’s jelly preventing compression of the blood vessels.
Amniotic fluid: fluid that fills the amniotic sac that serves many functions that protect the fetus:
• Maintain a constant body temperature • Assists in maintenance of fluid and electrolyte homeostasis • Allows the fetus freedom of movement for musculoskeletal development and
symmetric growth • Cushions the fetus • Acts as a barrier for infection • Allows fetal lung development
SVD: spontaneous vaginal delivery

5 | P a g e S T U D E N T N A M E :
MKF, 2019
FHR: fetal heart rate. Normal FHR is 110-160 bpm
IUPC: intrauterine pressure catheter
ISE: internal scalp electrode
PTL: preterm labor. Labor prior to 36 weeks gestation
Bag of waters: amniotic sac that surrounds the fetus and is filled with amniotic fluid. When the bag of water ruptures (rupture of membranes or ROM), the amniotic fluid escapes. It is important to note the following: COAT
Color Odor Amount Time ROM: rupture of membranes
SROM: spontaneous rupture of membranes
AROM: artificial rupture of membranes
PROM: premature rupture of membranes (BOW ruptured but no uterine contractions to signal labor)
PPROM: preterm (less than 36 weeks gestation) premature (not in labor) rupture of membranes
VBAC: vaginal birth after cesarean section (C/S). May also see TOLC (trial of labor after C/S)
Oligohydramnios: having less than 300 ml of fluid and is associated with renal abnormalities. May also compromise fetal oxygenation if the umbilical cord is compressed.
Polyhydramnios: having more than 2L of fluid and is associated with gastrointestinal and other malformations. Is also risk factor for postpartum hemorrhage.
Labor: process by which the fetus is expelled from the uterus
True labor: regular uterine contractions that are progressive and make cervical change
False labor: contractions are irregular, becoming regular but are temporary and do not significantly change the cervix.

6 | P a g e S T U D E N T N A M E :
MKF, 2019
FIRST STAGE OF LABOR
NOTE: these are approximate times as each labor is different.
CRITERION LATENT PHASE: 0-5 CM
ACTIVE PHASE: 6-8 CM
TRANSITION: 8-10 CM
Duration 6-8 hours 3-6 hours 20-40 minutes Contractions: Strength mild to moderate moderate to strong strong to very strong Rhythm irregular more regular regular Frequency 5-30 minutes apart 3-5 minutes apart 2-3 minutes apart duration 30-45 seconds 40-70 seconds 45-90 seconds Descent Station of presenting part
-2 to 0 station +1 to +2 station +2 to +3 station
Show Color brownish to pale pink pink to bloody mucus bloody mucus amount scant scant to moderate large amount Behavior and appearance
excited, calm or tense, pain controlled fairly well, follows directions easily, open to instructions
becomes more serious, desires companionship and encouragement, beginning fatigue, some difficulty following directions
pain described as severe, fear of loss of control, expresses doubt about ability to continue, nausea/vomiting, feeling of need to have a bowel movement, pressure on anus
Cervical dilation is the measure of how dilated the cervix is in centimeters. ... Fifty percent effaced means the cervix is at half of the expected length. If the cervix is 100% effaced, it is paper thin. The station is the position of the fetal head relative to the ischial spines of the maternal pelvis

7 | P a g e S T U D E N T N A M E :
MKF, 2019
https://www.youtube.com/watch?v=dYu-0rOnLpA
SECOND STAGE OF LABOR: Begins when cervix is completely effaced and dilated to 10cm. This is the stage where the mother will push and ends with the baby’s birth. The duration is different for each birth. The normal range is 30 min to the upper limit of 2 hours (3 hours if mother received an epidural).
THIRD STAGE OF LABOR: Begins after the baby’s birth until the placenta is born. Normally this occurs in 30 minutes. Strong uterine contractions, immediately after the baby is born, cause the placenta to separate from the uterine wall. Once the placenta is expelled, it is VITAL to assess the fundus of the uterus to be sure that the uterus is contracted, thus controlling maternal bleeding.
FOURTH STAGE OF LABOR: The first 1-2 hours after birth. This is a crucial time for both mother and baby as they transition from the physical process of birth and begin maternal/infant bonding. Skin-to-skin is encouraged during this time and breastfeeding should be initiated.
Uterine tachysystole is defined as 6 contractions in a 10-minute period.
Uterine hypertonus is described as a single contraction lasting longer than 2 minutes.
Uterine hyperstimulation is when either condition leads to a non-reassuring fetal heart rate pattern.
The term "fetal macrosomia" is used to describe a newborn who's significantly larger than average. A baby diagnosed with fetal macrosomia has a birth weight of more than 8 pounds, 13 ounces (4,000 grams), regardless of his or her gestational age. Mothers who deliver a macrosomic infant are at an increased risk for postpartum hemorrhage.
Skin to skin: placing the newborn infant directly on the mother’s chest immediately after birth. It is still considered skin to skin if the baby has on a hat and diaper. If the mother is unable to hold the baby skin-to-skin, another family member can practice skin-to-skin.

8 | P a g e S T U D E N T N A M E :
MKF, 2019
10 leading benefits of skin-to-skin care
1. Improvement in heart and lung function: Babies go through a dramatic transition after birth as they prepare to take their first breaths of air outside the uterus. Those held skin-to-skin by their mothers tend to adapt sooner than those who are not.
2. Stabilization of body temperature. 3. Regulation of blood sugar 4. Initiation of breastfeeding 5. Transfer of good bacteria 6. Reduction in infant crying 7. Relief from pain 8. Enhancement of mother-baby communication 9. Easier transition from the womb: Babies who are held skin-to-skin are more stable,
physiologically, than their peers who are placed in a warmer after birth. They also demonstrate better neurobehavioral outcomes, as indicated by many of the factors that have been noted, including less crying, lower pain response, and better breastfeeding. In short, these babies experience less stress following birth as they begin to navigate the new world around them.
10. Boost in maternal-child bonding.
Where should you palpate the mother’s abdomen to assess contractions? Why? Uterine contractions originate in the upper uterine segment or fundus of the uterus. Here is where you can palpate the intensity, duration and frequency of uterine contractions. When placing the transducers of the electronic fetal monitor, you would place the toco on the area of the upper uterine segment and the doppler over the fetal heart.
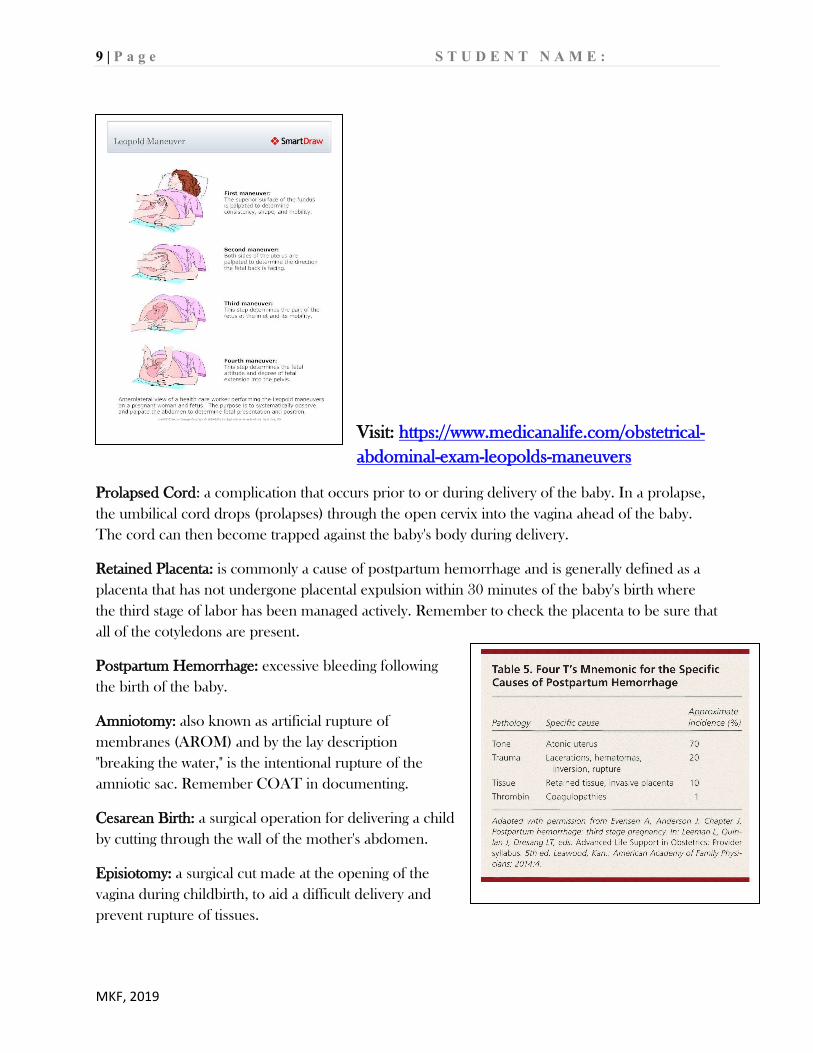
Describe the 4 maneuvers that are collectively referred to Leopold’s maneuvers and discuss what each maneuver is assessing.
9 | P a g e S T U D E N T N A M E :
MKF, 2019
Visit: https://www.medicanalife.com/obstetrical-abdominal-exam-leopolds-maneuvers
Prolapsed Cord: a complication that occurs prior to or during delivery of the baby. In a prolapse, the umbilical cord drops (prolapses) through the open cervix into the vagina ahead of the baby. The cord can then become trapped against the baby's body during delivery.
Retained Placenta: is commonly a cause of postpartum hemorrhage and is generally defined as a placenta that has not undergone placental expulsion within 30 minutes of the baby's birth where the third stage of labor has been managed actively. Remember to check the placenta to be sure that all of the cotyledons are present.
Postpartum Hemorrhage: excessive bleeding following the birth of the baby.
Amniotomy: also known as artificial rupture of membranes (AROM) and by the lay description "breaking the water," is the intentional rupture of the amniotic sac. Remember COAT in documenting.
Cesarean Birth: a surgical operation for delivering a child by cutting through the wall of the mother's abdomen.
Episiotomy: a surgical cut made at the opening of the vagina during childbirth, to aid a difficult delivery and prevent rupture of tissues.

10 | P a g e S T U D E N T N A M E :
MKF, 2019
Vacuum assisted birth: a method to assist delivery of a baby using a vacuum device. It is used in the second stage of labor if it has not progressed adequately. It may be an alternative to a forceps delivery and caesarean section.
Meconium: the dark green substance forming the first feces of a newborn infant.
Fetal Scalp Electrode (FSE): internal monitor connected directly to the fetal skin. A wire electrode is attached to the fetal scalp or other body part through the cervical opening and is connected to the monitor. This type of electrode is sometimes called a spiral or scalp electrode.
Intrauterine Pressure Catheter (IUPC): is a device placed into the amniotic space during labor in order to measure the strength of uterine contractions. External tocos are used to measure tension across the abdominal wall and detect only contraction frequency and duration.

11 | P a g e S T U D E N T N A M E :
MKF, 2019
Discuss the 3 characteristics of a contraction.
a. Frequency: beginning of one contraction to the beginning of the next contraction
b. Duration: beginning of one contraction to the end of that same contraction
c. Intensity: strength of a contraction. Subjective to each woman. Can gauge intensity by palpating fundus of uterus during a contraction or can accurately measure with the placement of an IUPC
What is a major complication of epidural anesthesia?
Hypotension is the major complication of epidural anesthesia. To avoid this, the patient is hydrated with a liter of IV fluids (Ringer’s lactate or Normal saline) prior to the epidural.
Other complications include: dizziness, tinnitus (ringing in the ears), fever, urinary retention (evaluate bladder q2h if Foley not placed), pruritus (itching), limited movement, increased use of oxytocin, longer second stage of labor.
What are nursing interventions (list 3) in caring for women desiring epidural anesthesia?
1. Change maternal position 2. Increase IV fluids 3. Stop Pitocin (if infusing) 4. Notify provider
5. Some facilities still place O2 via face mask
FETAL HEART RATE (FHR) EVALUATION:
Accelerations: abrupt increase in fetal heart rate by 15 beats/min (bpm) for 15 seconds (15X15) with return to baseline within 2 minutes.
Variability: fluctuations in the baseline fetal heart rate. Reassuring feature of the baseline FHR. Is described as absent, minimal, moderate, and marked.
Tachycardia: fetal heart rate of greater than 160 bpm for 10 minutes or longer

12 | P a g e S T U D E N T N A M E :
MKF, 2019
Bradycardia: fetal heart rate of less than 110 bpm for 10 minutes or longer
Discuss the 4 types of fetal heart decelerations and list interventions for each.
Change position Prepare for delivery
Change position Increase IV fluids Stop Pitocin Call provider What is the criteria of

13 | P a g e S T U D E N T N A M E :
MKF, 2019

14 | P a g e S T U D E N T N A M E :
MKF, 2019
Newborn Assessment
List the four ways newborns can lose heat?
The average weight loss within the first 3-4 days of life for a full-term newborn is 5-6% of body weight.
The appropriate dose for Vitamin K is __0.5 mg____. This injection is placed where? IM in the thigh.
Why must Vit. K (aquaMEPHYTON) be given to all newborns?
Vitamin K is synthesized by intestinal flora, which is not present at birth. IM vitamin K is to prevent hemorrhagic disease of the newborn.
The prophylactic eye ointment is? _Erythromycin 0.5% ophthalmic ointment is installed in all neonates to prevent ophthalmia neonatorum, an infection caused by Neisseria gonorrhea that if untreated, can lead to blindness.
In order to prevent infant abduction, what should be done before and after every parent-infant interaction? Check the baby bands with the mothers arm band.
VOCABULARY
Vernix caseosa: protective substance of cheesy consistency covering the fetal skin
Lanugo: downy, fine hair most noticeable over the shoulder, forehead and eyebrows
Caput: the occiput of the fetal head appearing at the vaginal opening (introitus) preceding birth of the head.
Cephalohematoma: blood from ruptured blood vessels between a skull bone and the skin.

15 | P a g e S T U D E N T N A M E :
MKF, 2019
Molding: overlapping of the fetal sutures and fontanels during labor that allows the fetal head to mold to the maternal pelvis. Molding can be extensive (cone head) but assumes the normal shape within 3 days after birth.
Circumcision: removal of the foreskin (prepuce) of the penis
Acrocyanosis: blue color of hands and feet in most infants at birth that may persist for 7-10 days.
Physiologic jaundice: Occurs in about 60% of newborns after 24 hours of age and usually resolves without treatment.
Bilirubin: results from the breakdown of RBCs. Jaundice occurs by elevated serum levels of unconjugated bilirubin and is visible as yellowish coloring of the skin & sclera.
Strawberry hemangioma: (nevus vascularis) is an elevated lesion of immature capillaries and endothelial cells that usually resolve over the years.
Mongolian spot: bluish gray or dark pigmented area usually found over the lower back and buttocks; present at birth in some infants, primarily non-white infants. The spot usually fades over time. Important to document to avoid misinterpretation as child abuse.
Milia: “baby acne” unopened sebaceous glands appearing as tiny, white pinpoint papules on the forehead, nose, cheeks, and chin of a neonate that disappear spontaneously over time.
Fontanelles: membrane filled spaces located where the sutures intersect. The two most important fontanelles are the anterior and posterior. If the fontanelles are depressed, the infant is dehydrated.

16 | P a g e S T U D E N T N A M E :
MKF, 2019
INTRODUCTION TO POST-PARTUM
Vocabulary:
Post-partum: period following birth
Involution: a reduction in size of the uterus after birth and its return to its nonpregnant state.
Fundus: The fundus of the uterus is the top portion, opposite from the cervix. Fundal height, measured from the top of the pubic bone, is routinely measured in pregnancy to determine growth rates.
Lochia (rubra, serosa, alba): see chart
Afterpains: contractions after birth that promote involution
Lactation: the secretion of milk by the mammary glands.
Postpartum depression (PPD): mood disorder that can affect women after childbirth. Mothers with postpartum depression experience feelings of extreme sadness, anxiety, and exhaustion that may make it difficult for them to complete daily care activities for themselves or for others.
Breast engorgement: Breast engorgement means your breasts are painfully overfull of milk. This usually occurs when a mother makes more milk than her baby uses. Your breasts may become firm and swollen, which can make it hard for your baby to breastfeed. Engorged breasts can be treated at home. For women who bottle feed, ice compresses, breast binder and cabbage leaves can help with engorgement.
Mastitis: inflammation of the mammary gland in the breast, typically due to bacterial infection transmitted from the baby via a damaged nipple. Breastfeeding should continue to help empty the breast. Antibiotics are prescribed for the mother.
17 | P a g e S T U D E N T N A M E :
MKF, 2019
Postpartum Assessment:
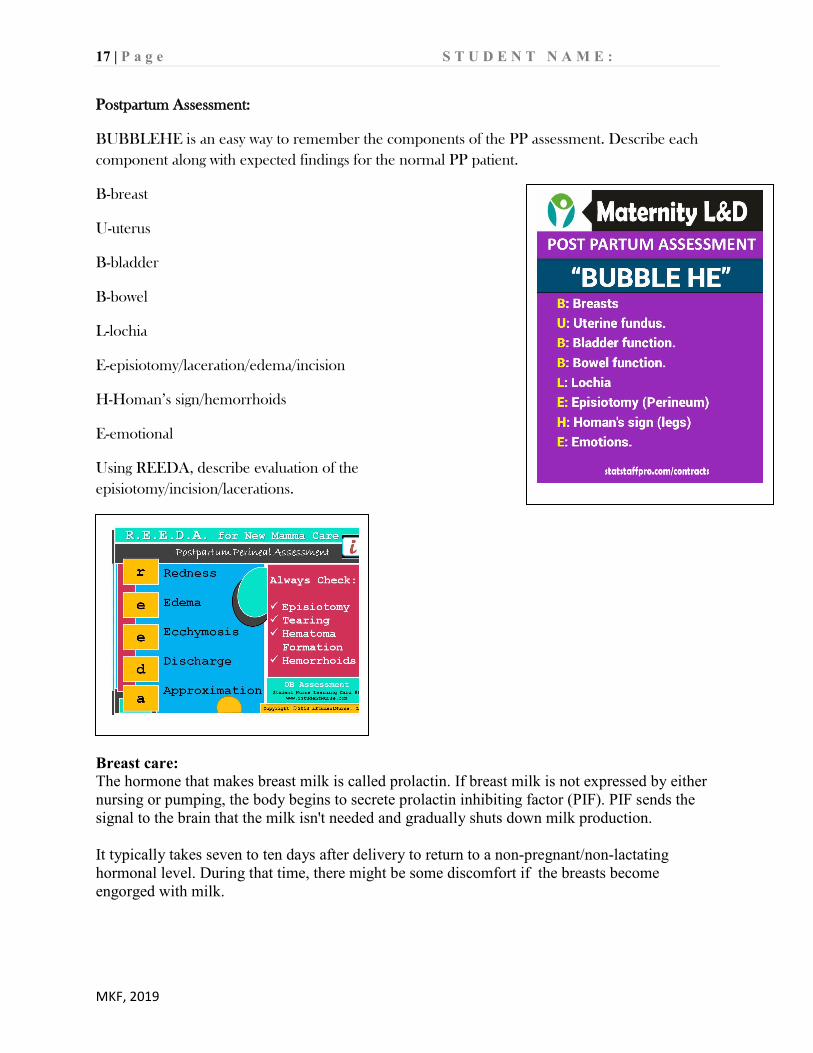
BUBBLEHE is an easy way to remember the components of the PP assessment. Describe each component along with expected findings for the normal PP patient.
B-breast
U-uterus
B-bladder
B-bowel
L-lochia
E-episiotomy/laceration/edema/incision
H-Homan’s sign/hemorrhoids
E-emotional
Using REEDA, describe evaluation of the episiotomy/incision/lacerations.
Breast care: The hormone that makes breast milk is called prolactin. If breast milk is not expressed by either nursing or pumping, the body begins to secrete prolactin inhibiting factor (PIF). PIF sends the signal to the brain that the milk isn't needed and gradually shuts down milk production. It typically takes seven to ten days after delivery to return to a non-pregnant/non-lactating hormonal level. During that time, there might be some discomfort if the breasts become engorged with milk.

18 | P a g e S T U D E N T N A M E :
MKF, 2019
Tips for the non-breastfeeding client: • Avoid stimulating the breasts. This is important for the partner to understand too.
• wearing a supportive bra is more comfortable, but don't bind the breasts. Binding can
lead to problems like mastitis and plugged ducts. At the very least, it will add to general discomfort.
• applying cool compresses or ice packs (a bag of frozen vegetables works nicely) and
taking nonsteroidal anti-inflammatory medication such as ibuprofen may help the client be more comfortable.
• If the client is really uncomfortable, it's okay to express a small amount of milk to ease
the engorgement. But keep in mind that expressing regularly signals the body to make more milk and delays how long it takes for milk production to stop.
• stand with the breasts away from the warm water in the shower, as this can stimulate milk
production.
• applying raw cabbage (green, not purple which will stain the skin) to the breasts helps ease discomfort and reduce milk production. First get the cabbage leaves nice and cold in the refrigerator or freezer. It's safe and worth a try.
Tips for the breastfeeding client:
• In the first few days after delivery, a small amount of thick yellowish milk called colostrum is produced. Colostrum is rich in nutrients and provides all the calories a baby needs for the first few days.
• Infants are born with an excess of fluid and sugar stores that they are able to use until their mom’s milk supply increases. A larger amount of milk will be produced within three to five days
• Breast fed babies generally eat every 1-2 hours, this is normal. In the first one to two weeks, most infants will breastfeed 8 to 12 times per day. Some infants will want to nurse frequently, as often as every 30 to 60 minutes, while others will have to be awakened and encouraged to nurse. A baby may be awakened by changing the diaper or tickling the feet. During the first week of life, most clinicians encourage parents to wake a sleeping infant to nurse if four hours have passed since the beginning of the previous feeding. Some babies will cluster feed, meaning that they feed very frequently for a number of feedings and then sleep for a longer period.
• You know your baby is getting enough by monitoring their wet diapers and their bowel movements. Normally, by the fourth to fifth day after birth, an infant should have at least six wet diapers per day with clear or pale yellow urine. Fewer than six wet diapers, or dark yellow or orange urine in the diaper are signs of inadequate intake and should be reported to the child's clinician. An infant's stool should become mustard yellow to light brown, often with visible milk curds, by the fourth to fifth day. Most infants have four or more stools per day by day four.

19 | P a g e S T U D E N T N A M E :
MKF, 2019
• If the breasts become engorged, try: o Wear a bra with good support 24 hours a day. o Take a warm shower or apply a warm face cloth to the breasts. ... o Pump or hand express milk before nursing to soften the breast if the baby is
having trouble latching on because the breasts are engorged.
Latching on refers to the infant's formation of a tight seal around the nipple and most of the areola with his or her mouth. A correct latch-on allows the infant to obtain an adequate amount of milk and helps to prevent nipple soreness and trauma.
Signs of a good latch-on include:
●The top and bottom lips should be open to at least 120° ●The lower lip (and, to a lesser extent, the upper lip) should be turned outward against the breast ●The chin should be touching the breast, while the nose should be close to the breast ●The cheeks should be full ●The tongue should extend over the lower lip during latch-on and remain below the areola during nursing (visible if the lower lip is pulled away)
When an infant is latched correctly, the woman may feel discomfort for the first 30 to 60 seconds, which should then decrease. Continued discomfort may be a sign of a poor latch-on. To prevent further pain or nipple trauma, the woman should insert her clean finger into the infant's mouth to break the seal. She can then reposition the infant and assist with latch-on again. Information about painful or sore nipples is available separately
Signs of poor latch-on include: ●The upper and lower lip are touching at the corners of the mouth ●The cheeks are sunken ●Clicking sounds are heard, corresponding to breaking suction ●The tongue is not visible below the nipple (if the lower lip is pulled down) ●The nipple is creased after nursing
Resource for patients: https://www.uptodate.com/contents/breastfeeding-guide-beyond-the-basics

20 | P a g e S T U D E N T N A M E :
MKF, 2019
https://www.google.com/search?q=postpartum+breastfeeding+instructions+for+nursing+mothers&client=firefox-b-1-d&source=lnms&tbm=isch&sa=X&ved=0ahUKEwjvnLD-2v_gAhWhl-AKHYL_A2EQ_AUIDygC&biw=1599&bih=903#imgrc=EalhSXPQgfODwM: