anthogyr in-house data · interim clinical evaluation of the axiom® implant (dia. 4x10mm) : tissue...
TRANSCRIPT

Interim clinical evaluation of the axiom® implant (dia. 4x10mm) : tissue stabilisation and maintenance of bone level
ANTHOGYR IN-HOUSE DATA
Interim report on the axiom® clinical studyJanuary 2010

2
Introduction
The axiom® implant system is a new system designed to offer high bone crest stability in the neck (maintaining the papillae) and to improve stabilisation of soft and hard tissue around the implant. According to the Buser success criteria, the axiom® implant of diameter 4 x 10 mm offered survival and success rates of 100%.
Description of the study
> Objectives
Key times:- Length of study: one year- Inclusion period: September 2008 to March 2009- End of study: First quarter of 2010
The objective of this study is to confirm the clinical reliability of the implant and assess the system’s simplicity and ergonomics criteria. The implants were positioned according to their indications and using a specific protocol for this assessment. The information collected was centralized and organised in order to provide an overview of the clinical results quality. The ergonomics of the system (different technical features) were assessed using a clinical questionnaire.
A team of nine French and Swiss practitioners was formed to conduct the entire study:
Dr A. Adan, Dr F. Azam, Dr JP. Bernard, Dr H. Berdugo, Dr G. Durif, Dr C. Durif, Dr P. Eysseric, Dr P. Marin, Dr J. Vermeulen.
> Primary objectives: To confirm the clinical and functional reliability of the axiom® implant of diameter 4 x 10 mm (survival and success rate) 1 year post-implantation, according to the Buser success criteria.
> Secondary objectives:To evaluate bone behaviour over a year (radiographic analysis).
> Inclusion criteria - Patients without medical contraindications and with posterior mandibular premolar/molar tooth loss (34-37, 44-47).- Minimum period of 3 months (12 weeks) post-extraction.- Sufficient bone volume to enable the implants to be positioned, sufficient height and width to leave a minimum of 1 mm of bone wall on each
side of the implant.- Prosthetic rehabilitation with single units.
> Exclusion criteria - General contraindications to dental implants.- Patients who smoke > 10 cigarettes per day.- Patients with occlusal para functions.- Patients with active periodontal disease.

3
axiom® CLINICAL ASSESSMENT – JANUARY 2010
> Study Plan
The axiom® implants have been manufactured from medical grade V titanium alloy with BCP surface treatment.A 4 mm diameter and 10 mm length were used for the study.Two abutments suitable for two gum heights (1 and 3 mm) were proposed.
The study included 5 key phases:
1. Positioning the implant in a single stage (preoperative, antibiotic premedication 1h before the procedure).2. Removal of sutures 1 week post-operatively and checking hygiene quality 3 weeks post-operatively.3. Positioning the fi nal abutment at 12 weeks, capped with a protective cap.4. Fashioning and positioning the fi nal prosthesis within 10 days after positioning the fi nal abutment.5. Checks at 4, 6 and 12 months.
> Design of axiom® implant and tissue preservation Through its design, axiom® brings together different features, all intended to promote peri-implant tissue stability.
> Stable hermetically-sealed Morse cone connectionThis has two key advantages from the perspective of tissue preservation:- Absence of micro-movements between the prosthetic parts of the implant.- Hermetic sealing of the interface from bacterial infi ltration.
Numerous studies 2,5 have shown that these features appear to be essential in maintaining the bone crest and avoiding bone resorption within one year, as can be seen with the implants equipped with a so-called “fl at” connection. The absence of movement and the hermetic seal should avoid apicalisation of the epithelium and stabilise the formation of the biological space alongside the abutment rather than the implant side. The formation of a biological space at this level should therefore prevent the bone from subsequently resorbing.
> Stability of the connection over timeBecause of the Dual Cône effects of the axiom®parts, assembly of the prosthesis does not concentrate mechanical forces. This specifi c design protects the implant holder restorations against unintentional unscrewing causing rupture of the paradontal pseudo-attachment which would, in turn, predispose to apicalisation of the epithelium, the consequences of which have been described above.7,9,11,12
Dual Cone AssemblyHermann et al. (2001)

4
> Integral « Platform switching »This is a horizontal shoulder on the prosthetic interface. The breach in continuity of the prosthesis is believed to have a dual advantage as concerns bone stability3,4,8,10. Firstly, it enables back positioning of the prosthesis interface against the bone crest, reducing its impact on remodelling of alveolar bone. Secondly, it is believed to enable a circular area of gum to develop which, because of the horizontal organisation of peri-implant fibres, acts like an “O ring” joint.This latter is believed, in turn, to contribute to vertical stability at the gum and, therefore, to the preservation of the biological space alongside the base of the prosthesis.
> The sanded threads neck of the implantThere is no precise consensus to date as to the ideal neck. On the other hand, studies 1,6 agree that the presence of a smooth surface in the alveolar bone promotes its resorption. The axiom® implant neck is therefore entirely sanded, as is part of the shoulder, in order to promote bone attachment at this level. The macro-threads only has the purpose of optimising primary retention of short implants.
> Immediate definitive connection componentBeyond the design of restoration parts, the axiom® system offers protocol stages which also promote tissue preservation. The prosthetic components provided are positioned immediately and definitely to minimise manipulation of the prosthesis.The abutments used are delivered sterile and are used immediately and definitively after the healing screw has been removed.
> Constant emergence profileThese components have a constant emergence profile, i.e. their prosthetic profile is entirely consistent with that of a healing screw in order to avoid them placing any tension on the soft tissue against the gingival cuff which has been preformed.
> Description of the protocol
> Surgical protocol
The axiom® implant is positioned 0.5 mm beneath the crest. The drilling depth is planned to enable storage of bone fragments from the self tapping of the implant and avoids any over-compression in the apical part. Rotation speeds of cutting instruments are provided for information purposes for a type D2-D3 bone and can be reduced for very dense bone.The drilling and implant positioning procedures are performed under irrigation.
Dia 2.7 mm
Stabilisation ofsoft tissue
«Platform-switching»Rupture of prosthetic profile(min. 0.35 mm – max 1.25 mm)

5
axiom® CLINICAL ASSESSMENT – JANUARY 2010
> axiom® positioning protocol
DESCRIPTION OF PROCEDURES
Drilling sequence
- Mark the bone with the ø 2 mm ball drill. Rotation speed 1250 rotations per minute with abundant irrigation.- Drill with the ø 2 mm drill bit corresponding to the length of the implant.- At this stage, the drilling guide may be used. This shows the minimum distance between two 4.0 mm diameter implants.- Bore the bone, moving in succession through increasing drill diameters.- Observe the corresponding depth marker for the 10 mm long implant.- Tapping with abundant irrigation at between 40 and 50 rotations per minute.- Screw the implant using the procedure described below.- Position the healing screw with the screwdriver.
Procedure for positioning the implant and closing the implant
- Screw the implant with the contra angle to -0.5 mm under bone level, irrigating constantly at 25-30 rpm depending on bonedensity. Ideally, the implant should be screwed at a force torque of between 25 and 60 N.cm.
- 1 stage surgery: Select a screw whose narrow-part height reaches the planned gum limit. Suture the gum around thehealing screw so that the gum rests on the screw narrowing without tension.
- Screw the healing screw manually with the screwdriver and 15 N.cm ratchet wrench.- Leave the implant to heal for a period of 12 weeks.
If it is preferable to choose closed healing (for example, implantation to a grafted site), it is recommended that the cover screw designed for this purpose be used.
> Prosthetic protocol
The prosthesis is fashioned after an average healing period of 12 weeks. This period may be adjusted by the practitioner depending on individual circumstances. In some cases, the prosthesis may be fashioned by initially using a temporary prosthesis under subocclusion in order to enable the implant to gradually take on its function.
Theoretical crest marginSub crestal position
Drill Borer Gauge Tap0.00.5
7.5
9.0
11.0
13.0
15.0
Ø 4
.0 x
10
mm
Drilling Depth
6
CLINICALCASES
PRE-OPERATIVE EXAMINATION
POSITIONING THE IMPLANT
(DAY D)
IMPLANT LOADING AT 12 WEEKS
CONTROL AT 6 MONTHS
CONTROL AT12 MONTHS
CASE 1H50
35 AND 36
CAS 2H5046
CASE 3H4036
CASE 4H4046
CASE 5F6036
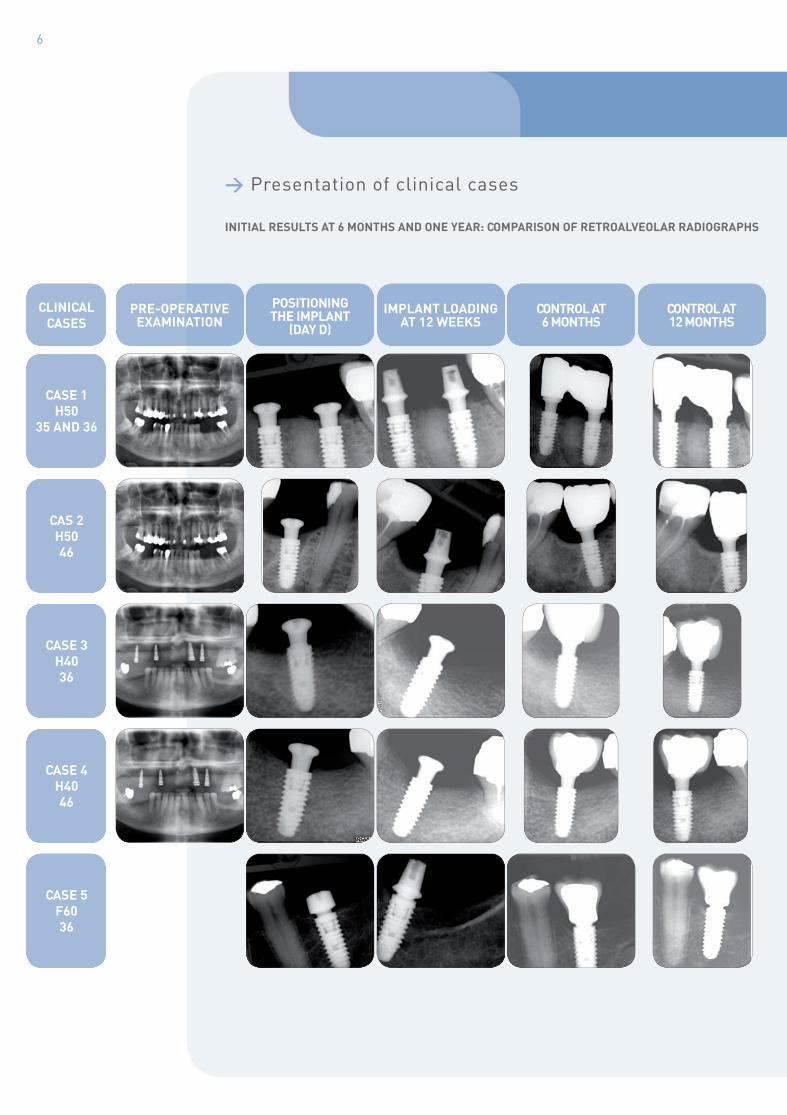
> Presentation of clinical cases
INITIAL RESULTS AT 6 MONTHS AND ONE YEAR: COMPARISON OF RETROALVEOLAR RADIOGRAPHS

7
axiom® CLINICAL ASSESSMENT – JANUARY 2010
Clinical follow-up ongoing
Clinical follow-up ongoing
Clinical follow-up ongoing
CLINICALCASES
PRE-OPERATIVE EXAMINATION
POSITIONING THE IMPLANT
(DAY D)IMPLANT LOADING
AT 12 WEEKSCONTROL AT 6 MONTHS
CONTROL AT12 MONTHS
CASE 6F5546
CASE 7H75
36-37
CASE 8H4546
CASE 9H4046
CASE 10H50
36-37
INITIAL RESULTS AT 6 MONTHS AND ONE YEAR: COMPARISON OF RETROALVEOLAR RADIOGRAPHS

8
The data obtained from this series of cases from the radiographic images show almost non-existent bone loss.According to the Buser success criteria, the axiom® implant of diameter 4 x 10 mm currently offers a survival and success rate of 100%.Following the concept of the axiom® implant and the associated prosthesis implantation protocol, overall, the crest bone exhibits stable behaviour.
* Clinical follow-up in the axiom® diameter 4 x 10 mm study is still ongoing.
> Conclusion*
> Bibliography
> 1.Alomrani AN, Hermann JS, Jones AA, Buser D, Schoolfield J, Cochran DL. The effect of a machined collar on coronalhard tissue around titanium implants: a radiographic study in the canine mandible. Int J Oral Maxillofac Implants. 2005 Sep-Oct;20(5):677-86.
> 2.Broggini N, McManus LM, Hermann JS, Medina RU, Oates TW, Schenk RK, Buser D, Mellonig JT, Cochran DL.Persistent acute inflammation at the implant-abutment interface. J Dent Res. 2003 Mar;82(3):232-7.
> 3.Canullo L, Rasperini G. Preservation of peri-implant soft and hard tissues using platform switching of implantsplaced in immediate extraction sockets: a proof-of-concept study with 12- to 36-month follow-up. Int J Oral Maxillofac Implants. 2007 Nov-Dec;22(6):995-1000.
> 4.Cappiello M, Luongo R, Di Iorio D, Bugea C, Cocchetto R, Celletti R. Evaluation of peri-implant bone loss aroundplatform-switched implants. Int J Periodontics Restorative Dent. 2008 Aug;28(4):347-55.
> 5.Dibart S, Warbington M, Su MF, Skobe Z. In vitro evaluation of the implant-abutment bacterial seal: the locking tapersystem. Int J Oral Maxillofac Implants. 2005 Sep-Oct;20(5):732-7.
> 6.Hansson S. Implant-abutment interface: biomechanical study of flat top versus conical. Clin Implant Dent Relat Res.2000;2(1):33-41.
> 7.Hermann JS, Schoolfield JD, Schenk RK, Buser D, Cochran DL. Influence of the size of the microgap on crestal bonechanges around titanium implants. A histometric evaluation of unloaded non-submerged implants in the canine mandible. J Periodontol. 2001 Oct;72(10):1372-83.
> 8.Hürzeler M, Fickl S, Zuhr O, Wachtel HC. Peri-implant bone level around implants with platform-switched abutments:preliminary data from a prospective study. J Oral Maxillofac Surg. 2007 Jul;65(7 Suppl 1):33-9. Erratum in: J Oral Maxillofac Surg. 2008 Oct;66(10):2195-6.
> 9.King GN, Hermann JS, Schoolfield JD, Buser D, Cochran DL. Influence of the size of the microgap on crestal bone levels innon-submerged dental implants: a radiographic study in the canine mandible. J Periodontol. 2002 Oct;73(10):1111-7.
> 10.Lazzara RJ, Porter SS. Platform switching: a new concept in implant dentistry for controlling postrestorative crestalbone levels. Int J Periodontics Restorative Dent. 2006 Feb;26(1):9-17.
> 11.Stanford CM. Achieving and maintaining predictable implant esthetics through the maintenance of bone arounddental implants. Compend Contin Educ Dent. 2002 Sep;23(9 Suppl 2):13-20.
> 12.Weng D, Jacobson Z, Tarnow D, Hürzeler MB, Faehn O, Sanavi F, Barkvoll P, Stach RM. A prospective multicenterclinical trial of 3i machined-surface implants: results after 6 years of follow-up. Int J Oral Maxillofac Implants. 2003 May-Jun;18(3):417-23.
2 237 avenue André-Lasquin74700 Sallanches - FranceTél. +33 (0)4 50 58 02 37Fax +33 (0)4 50 93 78 60
www.anthogyr.com
Cré
dits
pho
tos:
Ant
hogy
r -
Dr.
And
ré A
dan
- D
r. Fr
anck
Aza
m -
Dr.
Jacq
ues
Verm
eule
n -
Tous
dro
its r
éser
vés
© Anthogyr - DCIA-0110