antibiotics made easy
DESCRIPTION
Lecture notes by Dr. Shuhaila ShahrilCUCMSTRANSCRIPT
Final Year CUCMS Teaching Module
Dr Nor Shuhaila Shahril

BACTERIA!!

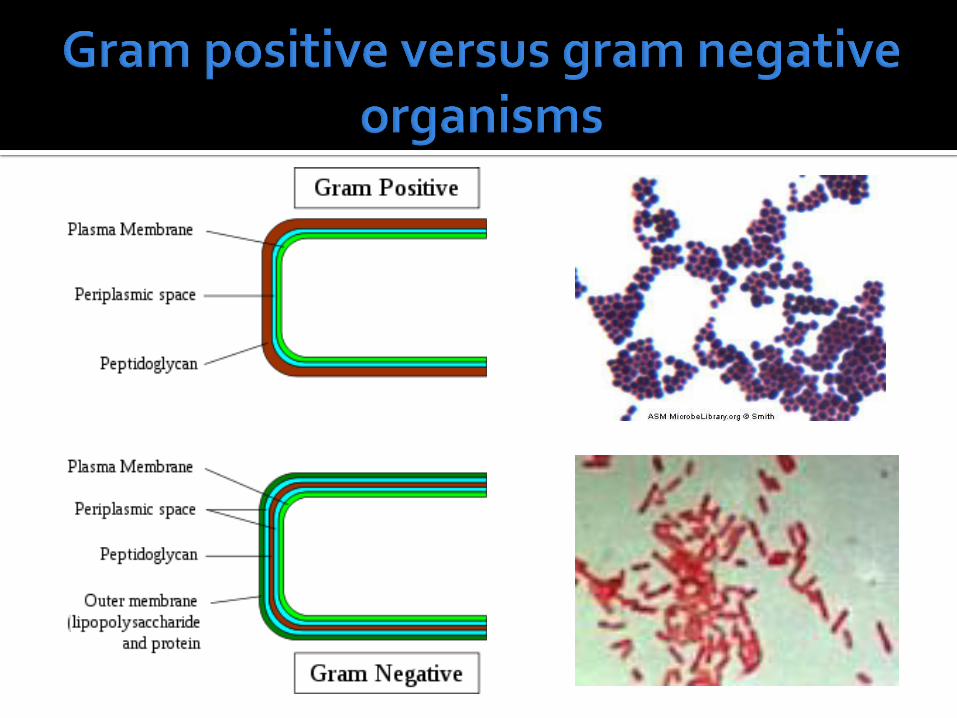
Gram staining method
If stained dark blue or violet = gram positive
Due to high amount of peptidoglycan in cell wall
If cannot retained crystal violet but takes up
counterstain (safranine or fuchsine), and appear pink or red = gram negative

coccus (sing.), cocci (pl.): are spherical (coccus = a berry),
bacillus (sing.), bacilli (pl.): are rod-shaped (bacill(um) = a little stick)
spirillum (sing.), spirilla (pl.): are spiral (spiro = spiral, coil).
Streptococcus – in chains (strepto = bent, twisted, pliable) Staphylococcus – in clusters (staphylo = a bunch of grapes Diplococcus – in sets of two (diplo = double)
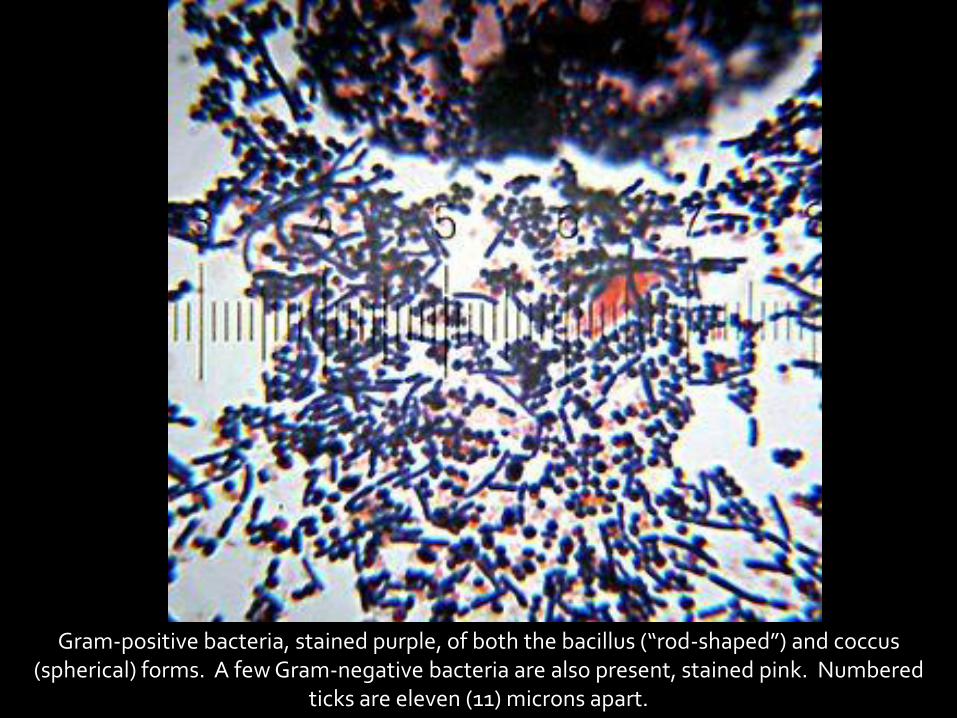
Gram-positive bacteria, stained purple, of both the bacillus (“rod-shaped”) and coccus (spherical) forms. A few Gram-negative bacteria are also present, stained pink. Numbered
ticks are eleven (11) microns apart.
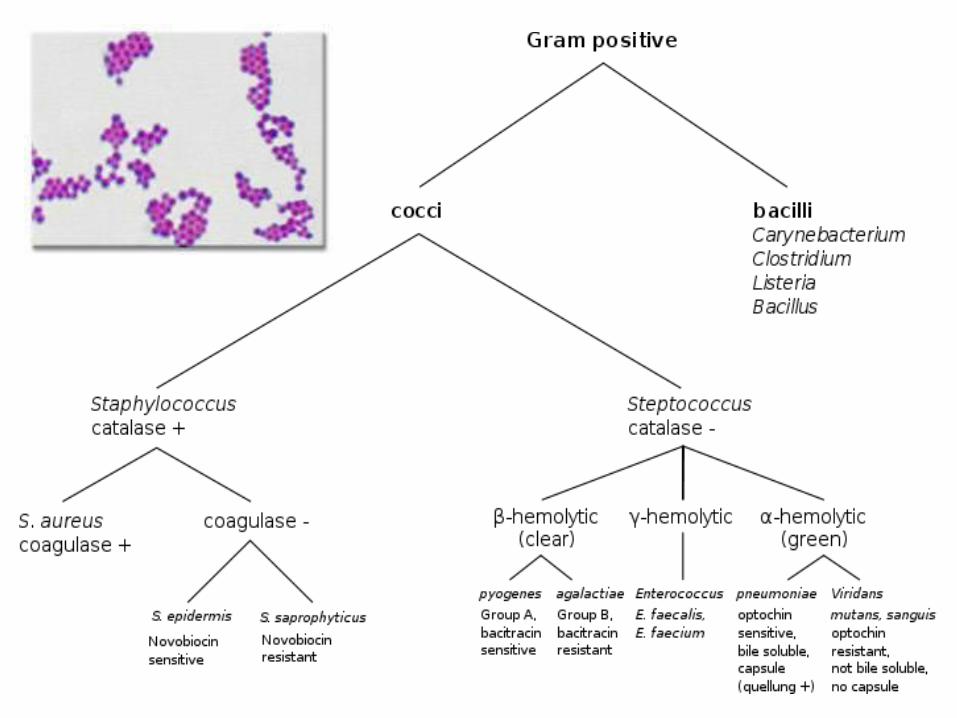

Cocci (sphere-shaped bacteria)
Streptococcus spp.
Staphylococcus spp.
Bacilli (rod-shaped bacteria)
Subdivided based on their ability to form spores:-
▪ Non-spore formers are Corynebacterium and Listeria (a coccobacillus)
▪ Spore-formers: Bacillus and Clostridium (anaerobes)

Coxiella burnetti (coccobacilli) Coccobacillus – intermediate between cocci and bacilli shape
E.coli

Enzymes produced by some bacteria Responsible for their resistance to beta
lactam antibiotics like penicillins and carbapenems.
These antibiotics have a common element in their molecular structure: a four-atom ring known as a beta-lactam.
The lactamase enzyme breaks that ring open, deactivating the molecule's antibacterial properties.
Beta-lactam antibiotics are typically used to treat a broad spectrum of Gram-negative bacteria.
Beta-lactamases produced by Gram-negative organisms are usually secreted.
Enterobacteriaceae, Pseudomonas aeruginosa, Haemophilus influenzae, and Neisseria gonorrhoeae

Cephalosporins (except for 1st generation) are relatively resistant to beta-lactamase.
cephalosporins with an oxyimino side chain, such as cefotaxime, ceftazidime, ceftriaxone, or cefepime.
Consequently, when these antibiotics were first introduced, they were effective against a broad group of otherwise resistant bacteria.

Enzyme not only chops apart penicillins, but also cephalosporin antibiotics.
Many different species of bacteria can produce the ESBL enzyme, including both gram positive and gram negative bacteria.
The most common ESBL bacteria are E. coli and Klebsiella species. Surgical site infections and blood infections, and are
commonly responsible for urinary tract infections (UTIs).
Clavulanic acid + amoxicillin = Augmentin Sulbactam+ ampicillin= Unasyn Tazobactam+ piperacillin= Tazosin
GOOD NEWS! Beta-lactamase inhibitors inhibit the beta lactamase thereby not allowing the molecule to hydrolyze the antibiotic. Most ESBLS remain susceptible to Beta-lactamase inhibitors
BAD NEWS! Some ESBL producing bacteria produce large amounts of beta-lactamase thereby overwhelming the beta-lactamase inhibitors.


Antibiotics may need dosage adjustment in patients with renal impairment.
Calculate creatinine clearance
Some antiBx do not need adjustement for
patients with renal insufficiency
e.g. amphotericin B, azithromycin, ceftriaxone, clindamycin, doxycycline, pyrimethamine, rifampicin.


A group of antibiotics derived from Penicillium fungi 1. Natural penicillins:
Pen G and V indicated against streptococci, anaerobes (above the diaphragm), syphilis, Listeria monocytogenes (high dose), dog and cat bites (Pasteurella multocida ).
Does not cover S. aureus. 2. Penicillinase-Resistant Penicillins (PRSP):
Methicillin / cloxacillin – indicated against penicillinase producing S.aureus (MSSA not MRSA) for endocarditis, osteomyelitis.
3. Aminopenicillins: Ampicillin / Amoxicillin: G(+) coverage similar to above,
covers many G(-) in GI tract (Salmonella, Shigella, E. coli, Proteus), N. meningitidis, 70% of H. influenza, Listeria, Nocardia.

Amoxicillin + clavulanate = Augmentin. Covers most G(+) except MRSA, and many G(-).
Anaerobe coverage ((B. fragilis, C. difficile )
Ampicillin + sulbactam = Unasyn. Coverage to G(+) similar to above and G(-) all
except Serratia, Enterobacter, Pseudomonas, Legionella.
Anaerobe coverage (B. fragilis, C. difficile )
Indication: GYN, GI and skin.
4. Anti-pseudomonal penicillins: CarboxyPCN e.g. ticarcillin UreidoPCN e.g. piperacillin
Cover most streptococci, and most G(-) with variable coverage for Klebsiella, M. catarrhalis, Serratia, Legionella.
NO coverage for Staphylococcus (except for Piperacillin+Tazobactam).
Good anaerobic coverage (B. fragilis, C. difficile ).
Main indication is Pseudomonas aeuroginosa. For serious Pseudomonas infections an aminoglycoside should be
added for synergism.


A class of β-lactam antibiotics originally derived from the fungus Acremonium, which was previously known as "Cephalosporium”.
First-generation cephalosporins are active predominantly against Gram-positive bacteria
Successive generations have increased activity against Gram-negative bacteria (albeit often with reduced activity against Gram-positive organisms).
Infrequent ADRs (0.1–1% of patients) include: nausea, vomiting, rash, headache, dizziness, oral and vaginal candidiasis, pseudomembranous colitis, eosinophilia, and/or fever.
The cross reactivity with penicillin (5-10%) is a concern especially if pt had anaphylaxis - cephalosporins should be completely avoided.

Cephalexin , Cefazolin.
Covers all streptococci, S. aureus (not MRSA) and S. epidermis.
Also cover G (-) bacteria: N. gonorrhea, M. catarrhalis, H. influenza , E. coli, Klebsiella.
Main indications are surgical prophylaxis and Strep. / Staph. (not MRSA)

Subdivided into:- "good for H. influenza" – cefuroxime and "good for anaerobes" –cefoxitin, cefotetan.
Similar G(+) coverage as 1ST generation and better G(-) coverage including N. meningitis (not the drug of choice for meningitis), Salmonella / Shigella / Proteus and +/- Yersenia.
Main indications are GI (colorectal surgery and appendicectomy), and Ob-Gyn procedures.

Ceftriaxone (Rocephin) & ceftazidime (Fortum) – two most commonly used.
Others: cefotaxime (Claforan), cefoperazone (Cefobid)
G(+) coverage is similar to 1ST and 2ND generation.

Bacterial meningitis Has activity against H. influenza (resistant to PCN), N.
gonorrhea and N. meningitidis
Good CSF penetration.
Dose 2g bd Pneumonia
CAP (1-2g od, together with macrolide)
Mild-to-mod health-care associated pneumonia Typhoid fever (3g od) Gonorrhoea (125mg IM stat)

Anaerobic coverage varies from one drug to the other.
G(-) are generally covered well except for atypicals (e.g. Legionella).
Cephalosporins DO NOT cover Listeria or Enterococcus.

Ceftazidime: indicated against Pseudomonas.
Older 3RD generation include cefotaxime (Claforan), similar to ceftriaxone, and cefoperazone (Cefobid), similar to ceftazidime.

Cefepime (Maxipine)
Similar to 3rd generation but with better G(-) coverage (P. aeruginosa, Enterobacter, Serratia, C. freundii) and better G(+) coverage (S. aureus ).


Erythromycin Clarithromycin Azithromycin
Clarithromycin and azithromycin have similar
antimicrobial profiles, providing enhanced activity against H. influenza as compared with erythromycin and retaining good efficacy against G+ organisms.

Cover Streptococcus, Staphylococcus (not MRSA), +/- N. gonorrhea, H. influenza, M. catarrhalis, Legionella, M. pneumonia and Chlamydia.
Cross-resistance is seen among all macrolides, particularly in Gram positive bacteria.
Because azithromycin has the best activity against Chlamydia trachomatis
1 gm PO single dose for the treatment of non-gonococcal urethritis and cervicitis.

An alternative to penicillin in allergic patients
Non-gonococcal urethritis / cervicitis
Upper respiratory tract infections
Pneumonia (atypical) secondary to Legionella or Mycoplasma.

Gastrointestinal complaints, particularly nausea, abdominal pain and diarrhea
Headache Abnormal LFT's Reversible hearing loss. Azithromycin and clarithromycin – lowest
S/E. Clarithromycin - taste disturbance, Archilles
tendon rupture
More significant with clarithromycin and erythromycin, as they both increase serum concentrations of drugs metabolized by the P-450 system in the liver.
May increase the levels of warfarin, digoxin, carbamezapine
May cause arrhythmias when used with some anti-histamines.


Most common is imipenam + cilastatin (Imipenem) given with cilastatin to inhibit renal breakdown.
Wide spectrum antibiotic
Covers most G (+) except MRSA and most G (-) except Legionella and some strains of Pseudomonas (maltophilia, cepacia ).
Also covers all anaerobes and has activity against Listeria and Nocardia.

Seizures are reported particularly in patients with history of seizures or renal failure.
Main indication is multidrug resistant bacteria and should NOT be a first choice.

Good activity against G(-) such as Proteus mirabilis and E. coli.
Good for GI pathogens such as Vibrio cholera, Campylobacter jejuni, Yersinia, Salmonella and Shigella (drug of choice for traveler's diarrhoea)
Most active fluoroquinolone against the Pseudomonas species.
Good against bacteria that depend on the production of beta lactamase for survival, thus it covers H. influenza and S. aureus
But surprisingly weak against streptococci (including S. pyogenes and S. pneumonia)

NO activity against anaerobic bacteria, including B. fragilis. (not a good choice for PID - weak against chlamydia and enterococci.
NOT used in children – impair proper growth of cartilage.

Levofloxacin
Better activity against Gram (+) cocci and perhaps less toxicity.
Main advantage: daily dose (250-500mg po qd)
Moxifloxacin (Avelox)
Main indication: community acquired pneumonia
Used as monotherapy


Gentamycin, netilmicin and amikacin are the most common.
BEWARE! All aminoglycosides have the potential to cause nephrotoxicity and ototoxicity.

They cover many G(-) including Pseudomonas aeruginosa (but not cepacia or maltophilia) and they do not cover Neisseria (gonorrhea or meningitidis).
DO NOT cover anaerobes, Legionella or atypicals.
G(+) coverage is poor, but they will cover S. aureus (MSSA only) and Listeria monocytogenes.

As volume of distribution increases (CHF, ascites, third spacing) the dosage of the drug must be increased.
NO CSF penetration. TDM: Peaks and troughs should be
measured, although other dosing alternatives are now being used, such as once-daily 7 mg/kg/day of gentamycin.
Divided dosing in endocarditis.

Gram negative sepsis, endocarditis (in combination with penicillin), and for synergism against P. aeruginosa infections.


Indicated mainly for anaerobic coverage
Good activity against C. difficile (given PO), Trichomonas, Giardia and B. fragilis.

E.g Tetracycline, doxycycline, minocycline Indication:
Infection due to Rickettsiae, Chlamydia, Nocardia, Lyme's disease (early)
Patients allergic to PCN that requires treatment for syphilis
Minocycline is more effective against staph and used for the treatment of acne.
Drugs should be taken on empty stomach since milk, Fe, Ca and antacids interfere with absorption.
Photosensitivity reported. Not given to pregnant women or children < 10 years
old.
Wide spectrum including activity against streptococci and H. influenza.
Indicated PO for uncomplicated UTI, COPD/bronchitis, otitis media and PCP prophylaxis.
Indicated IV for active PCP with pO2 < 70 mmHg or if unable to tolerate PO. TMP/SMX (TMP 20mg/kg/day divided into 4 doses).
In HIV (+) pt allergic effects are as high as 50%. Avoid in G6PD deficiency.
Excellent against anaerobes, including such below the diaphragm pathogens as B. fragilis.
Covers streptococci and S. aureus (not MRSA).
Well absorbed orally Most frequent cause of C. difficile
pseudomembranous colitis.

Glycopeptide antibiotics Covers all G(+) including MRSA, C. difficile, Diphtheria,
Enterococcus.
Indications: alternative to PCN / Cephalosporin in the allergic patient, C. difficile (oral preparation) and MRSA.
Red-man syndrome is seen following rapid administration and is believed to be histamine mediated.
Vancomycin has good CSF penetration and is used as a secondary drug in meningitis to cover resistant Streptococcus.
Because of emerging patterns in drug resistance, Vancomycin should be reserved for specific situations and not be used as a first line agent.


30 yr old Malay man Gardener Left lower limb swelling and
redness X 5/7 Fever+ Diagnosis? What is the offending
organism? What antibiotics do you want to
initiate?

Uncomplicated /Immunocompetent
Staphylococcus aureus
Streptococcus pyogenes (Group A)
Streptococcus agalactiae (Group B)
Complicated (burns, diabetes, infected
pressure ulcers, traumatic/ surgical wounds)
Gram negative bacilli (Escherichia coli, Pseudomonas aeruginosa)
Group A streptococci or Clostridium species, with or without other anaerobes, can cause fulminant soft tissue infection and necrosis, especially in diabetic patients.
Anti-staphylococcal penicillin Cloxacillin/ flucoxacillin
Amoxicillin plus clavulanic acid (Augmentin) 1st gen. Cephalosporin (Cephalexin)
If allergic to penicillin
Fluroquinolones with good activity against gram positive organism (levofloxacin, moxifloxacin, gatifloxacin)
Clindamycin
Reasonable empiric monotherapy
Piperacillin/tazobactam (Tazocin)
Carbapenem (imipenem/ meropenem)
Methicillin-resistant Staphylococcus aureus (MRSA)
Vancomycin
Alternatives: Linezolid

21 yr old female Monoarthritis of the left knee Sexually active

Possible diagnosis?
Septic arthritis
Reactive arthritis
What investigation would you do to confirm
your suspicion?
Joint aspiration and send synovial fluid for FEME/ C&S

Gonococcal septic arthritis Neisseria gonorrhoeae
Non-gonoccal septic arthritis S. aureus (60-70%)
Strep species (15-20%)
Gram negative bacilli (haemophilus) 5-25%
Anaerobes (bacteroides/ Prophionibacterium acnes) 1-5%
Brucella/ mycoplasma (rare)

Gonococcal Non-gonococcal
Host Young, healthy adults Small children, elderly,
immunocompromised
Pattern Migratory,
polyarthralgias/ arthritis
Monoarthritis
Tenosynovitis Common Rare
Dermatitis Common Rare
Positive joint cultures < 25% > 95%
Positive blood cultures
Rare 40-50%
Outcome Good in > 95% Poor in 30-50%

Ceftriaxone
Covers for S. aureus, Strep and N.gonorrhoeae.

50 yr old Malay man Diabetes Type 2 Swelling of right big toe X
3/52 Associated with redness,
yellowish pus discharge+ x 1/52
Fever X 1/52
What investigations would you do?
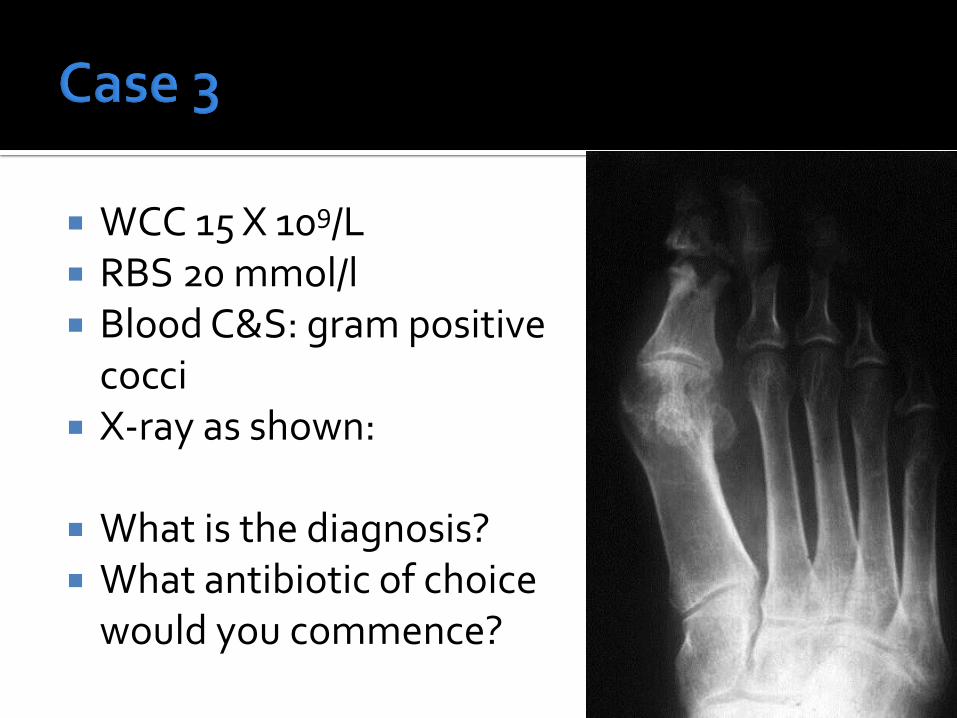
WCC 15 X 109/L RBS 20 mmol/l Blood C&S: gram positive
cocci X-ray as shown:
What is the diagnosis? What antibiotic of choice
would you commence?

Hallmark characteristics:- Bone destruction Periosteal new bone formation
Location: Lower extremities (most common)
▪ Over pressure areas in diabetics
Spine ▪ Lumbar > thoracic > cervical
Radial styloid Sacroiliac joint

S.aureus (most common) Streptococcus pyogenes Pseudomonas, Klebsiella (drug addicts) Salmonella spp (in sickle cell disease patients) Gram negative bacilli (E.coli, Pseudomonas) –
post-orthopaedic procedures
REMEMBER! Infections of the feet in diabetic patients often
involve both bone and soft tissue and are usually POLYMICROBIAL – both aerobic and anaerobic bacteria.

Gram positive cocci
Group A Strep (may cause acute sepsis)
Enterococcus (may be most common)
S. aureus
Enterobactericaeae

Streptococcus spp IV Penicillin
IV Ceftriaxone
Gram negative IV Ceftriaxone
IV Ceftazidime
IV Ciprofloxacin
IV Vancomycin/ Linezolid if MRSA
22 yr old male student Fever and headache of 2/7 Vomiting 10X today
What other information do you require?
Nature of headache Headache worse with coughing, sneezing,
bending over, defaecation – raised ICP Photophobia ENT symptoms – ENT region entry point to
meninges Reason for immunocompromised state
TB, cryptococcal Travel history Contact history
Orientated to time/ place/ person Photophobic++ Kernig’s positive Tone generally increased bilaterally Power 5/5 both UL and LL Plantars downgoing Unable to perform fundoscopy – severe
photophobia. No rash

What is the most likely diagnosis?
List the investigations that you would do in this case with justification.
FBC Hb 14, WCC 23, Plt 290 BU 9.0, Na 135, K 3.4, Cl 91, Creat 120 INR 1.05 , PTT 33s (n < 33) RBS 6.8 Blood C&S – prior to empirical antiBx Rx
CT brain - normal
What do you want to send for: CSF biochemistry – protein, glucose
CSF FEME/ Gram stain
CSF Indian ink
CSF culture and sensitivity
CSF AFB smear
CSF AFB stain
CSF virology
CSF cryptococcal antigen
LP results are as follows:- Opening pressure 20 cmH2O
Appearance cloudy
CSF protein 1.0 g/L
CSF glucose 1.5 mmol/l
CSF FEME: numerous polymorphonuclear neutrophils, RBC 0.2 X 106/L
COMMENT!

Value Normal Range
Appearance Clear & colourless
White Cells 0 - 5 x 106 /L (all lymphocytes with no neutrophils)
Red Cells 0 - 10 x 106 /L
Protein 0.2 - 0.4 g/L (or less than 1% of the serum protein concentration)
Glucose 3.3 - 4.4 mmol/L (or ≥ 60% of a simultaneously derived plasma glucose concentration)
pH 7.31
Pressure 7 – 18 cmH2O

Condition Appearance White Cells Red Cells Protein Glucose
Bacterial Meningitis
Cloudy & Turbid
Raised neutrophils
N H or VH VL
Viral Meningitis N Raised lymphocytes
N N or H N or L
Tuberculous Meningitis
N or slightly cloudy
Raised lymphocytes
N H or VH VL
Subarachnoid Haemorrhage
Usually blood stained
N VH N or H N or L
Guillan-Barré Syndrome
N N N H (only after 1 week)
N or L
Multiple Sclerosis
N Raised lymphocytes
N H N
N= normal, L= low, H = high, VH = very high, VL = very low
Streptococcus pneumoniae (pneumococcus) Neisseria meningitidis H. influenza type b
usually children, but now decreased incidence due to immunization
Enteric gram negative bacteria
neonates, elderly, recent neurosurgery, immunosuppressed
Group B strep
neonates
Listeria monocytogenes
pregnant women, newborns, elderly, immunosuppressed

Pending culture results High-dose IV Ceftriaxone or Cefotaxime
If suspect Cephalosporin-resistant pneumococci, add
vancomycin (usually very high doses needed to reach CSF [may need up to 4g/day) – needs very careful monitoring!)
STOP if organism known susceptible to cephalosporin/ penicillin

Nosocomial meningitis Make sure cover for Pseudomonas
IV Vancomycin and a cephalosporin with good activity against Pseudomonas e.g. IV Ceftazidime
If confirmed Pseudomonas, add an aminoglycoside e.g. gentamicin or amikacin.
Listeria meningitis
IV Ampicillin +/- gentamicin
IV Bactrim if allergic to penicillin
45 year old lady c/o fever and dysuria X 3/7 Chills and rigors Nausea+, poor appetite Vomiting 2-3X per day Lethargic+ BP 110/70 PR 96/min PA: soft, tender Rt loin with positive renal
punch, no ballotable kidneys.
What is the diagnosis?

UTI Pathogens Antibiotics
Uncomplicated: Cystitis/ urethritis
Enterobacteriacae (E.coli, Serratia, Klebsiella, Enterobacter, Citrobacter) Staph saprophyticus Enterococci
Augmentin Fluroquinolones (ciprofloxacin, levofloxacin) Bactrim
Recurrent cystitis (> 3 episodes per year)
As above As above with prophylaxis Bactrim
Complicated UTI: Indwelling cathter, obstruction, pyelonephritis
As above Possible pseudomonas
Beta-lactam plus aminoglycoside Fluroquinolones Piperacillin-tazobactam Imipenem

65 year old lady, non-smoker Diabetic Type 2 for 2 years Fever and cough X 4/7 Productive cough of yellowish sputum No haemoptysis Right-sided pleuritic chest pain Poor appetite No history of recent travel No contact with persons with respiratory
illness.

Pink on air, spO2 93%, alert Dyspnoeic RR 32/min Febrile T 38C BP 100/70 mmHg PR 115/ min reg Lungs: dull percussion note with coarse
crepitations at right lower zone, bronchial breath sounds.
Diagnosis? Investigation?

FBC Hb 14 Hct 50% Plt 239 TWC 20 BU 16 Na 134 K 4.2 Creat 140 RBS 15 UFEME gluc 1+, ketones nil, prot 1+ ABG pH 7.49 pO2 76 pCO2 29 HCO3 19
What other Investigations would you like to
do?


(urea > 7 mmol/l)

Streptococcus pneumoniae Adults with risk factors for “drug-resistant Strep pneumoniae” (DRSP):
older than 65, having exposure to children in day care, having alcoholism or other severe underlying disease, or recent treatment with antibiotics
Hemophilus influenzae commonly causes CAP in people who have suffered recent lung
damage from viral pneumonia. Enteric Gram negative bacteria
Escherichia coli and Klebsiella pneumoniae (bacteria in human intestines)
Risk factors for infection including residence in a nursing home, serious cardiac and pulmonary disease, and recent antibiotic use.
Pseudomonas aeruginosa An uncommon cause of CAP Risk factors: malnourished, bronchiectasis, on corticosteroids , or have
recently had strong antibiotics for a week or more.

Mycoplasma pneumoniae
Chlamydophila pneumoniae
Legionella pneumophilia (less common)
Atypical organisms are more difficult to grow.
Healthy outpatients without risk factors
No risk factors for DRSP, enteric Gram negative bacteria, Pseudomonas
Usually caused by viruses, atypical bacteria, penicillin sensitive Streptococcus pneumoniae, and Hemophilus influenzae.
Recommended management is with a macrolide antibiotic such as azithromycin/ clarithromycin/ erythromycin for 7 – 10 days.
IDSA 2007

Outpatients with underlying illness and/or risk factors but do not require hospitalization underlying cardiac (e.g. CCF) or pulmonary
disease (COPD) or is at risk for DRSP and/or enteric Gram negative bacteria.
Treatment: ▪ Fluroquinolone active against Streptococcus
pneumoniae such as levofloxacin or moxifloxacin, or
▪ A beta-lactam antibiotics (e.g. cefuroxime, augmentin) plus a macrolide (azithromycin, clarithromycin) for 7 – 10 days.

Hospitalized individuals NOT at risk for Pseudomonas Beta lactam antibiotics (cefotaxime, ceftriaxone,
ampicillin/sulbactam, ertapenem for selected patients), plus IV macrolide antibiotic (azithromycin) for 7 - 10 days (alternative to azithromycin is doxycycline)
Or
IV fluroquinolones active against Streptococcus pneumoniae such as levofloxacin or moxifloxacin
(if penicillin-allergy)

Hospitalized, ICU treatment NOT at risk for Pseudomonas
Beta lactam antibiotics (cefotaxime, ceftriaxone, ampicillin/sulbactam, ertapenem for selected patients), plus
IV macrolide antibiotic (azithromycin) or fluroquinolones (levofloxacin)

Individuals requiring intensive care at risk for Pseudomonas
2 regimes: IV anti-pseudomonal beta-lactam (cefipime, imipenem,
meropenem, piperacillin/ tazobactam) plus IV anti-pseudomonal fluoroquinolone (levofloxacin)
Or IV anti-pseudomonal beta-lactam (cefepime, imipenem,
meropenem, or piperacillin/ tazobactam) plus IV aminoglycoside (gentamicin) and IV macrolide (azithromycin) or IV anti-pneumococcal
fluroquinolone.

72 year old man Recent admission to a private hospital for
upper GIT bleed due to duodenal ulcer. Discharged 5/7 ago. c/o cough and dyspnoea for 2/7 OE: temp 37.5C, BP 110/78 PR 100/min Lungs: creps left lower zone with reduced air
entry What is the diagnosis?

Early onset Occurring < 5 days after hospital admission
Commonly associated with antibiotic-sensitive bacteria : H.influenzae, oxacillin-sensitive S. aureus, and S. pneumoniae
No risk factors for infection due to potentially antibiotic-resistant bacteria : antibiotic treatment or prior health care facility exposure
Late onset
Occurring ≥ 5 days after hospital admission
Usually antibiotic-resistant bacteria: MRSA, P. aeruginosa, Acinetobacter spp., and Enterobacter spp.
ATS. Am J Respir Crit Care Med. 171;388, 2005 Ibrahim EH, et al. Chest. 117:1434, 2000 ;
Trouillet JL, et al. Am J Respir Crit Care Med. 157;531, 1998

Antimicrobial therapy in preceding 90 days Current hospitalization of ≥ 5 days High frequency of antibiotic resistance in the
community or in the specific hospital unit Presence of risk factors for HCAP :
hospitalization for ≥ 2 days in the preceding 90 days residence in a nursing home home infusion therapy chronic dialysis within 30 days home wound care family member with MDR pathogens
Immunosuppressive disease and/or therapy






57 year old man Fever X 1/12 Lethargy+ O/E: febrile 38C Lungs: clear PA soft, hepatosplenomegaly Petechiae rashes on lower limbs
Hb 5.6 Plt 27 TWC 2.0 ANC 0.4
Fever in the presence of neutropenia Neutropenia:
ANC of <500 cells/mm3 or ANC that is expected to decrease to < 500 cells/mm3
during the next 48 h.
“Profound’’ is sometimes used to describe neutropenia in which the ANC is < 100 cells/mm3 a manual reading of the blood smear is required to
confirm this degree of neutropenia.

Infections (more commonly viral infections, but also bacterial or parasitic infections). E.g HIV, TB, malaria, EBV
Medications that may damage the bone marrow or neutrophils, including cancer and
chemotherapy
Vitamin deficiencies (megaloblastic anaemia – B12 and folate) Diseases of the bone marrow such as leukaemias, myelodysplastic syndrome, aplastic anaemia, myelofibrosis,
Radiation therapy
Congenital (inborn) disorders of bone marrow function or of neutrophil production
Autoimmune destruction of neutrophils (either as a primary condition or associated with another disease such as Felty’s syndrome) or from drugs stimulating the immune system to attack the cells
Hypersplenism, which refers to the increased sequestration and/or destruction of blood cells by the spleen

RP LFT FBP 2 sets of blood culture Culture from any suspected sites of infection CXR


Monotherapy with:
an anti-pseudomonal beta-lactam agent, such as cefepime, or
carbapenem (meropenem or imipenem-cilastatin), or
piperacillin-tazobactam
IDSA 2011

Other antimicrobials (aminoglycosides, fluoroquinolones, and/or vancomycin) may be added to the initial regimen for management of complications (eg, hypotension and pneumonia) or if antimicrobial resistance is suspected or proven.
Vancomycin (or other agents active against aerobic gram-positive cocci) is not recommended as a standard part of the initial antibiotic regimen for fever and neutropenia To be considered for specific clinical indications including
suspected catheter-related infection, skin or soft-tissue infection, pneumonia, or hemodynamic instability.
If MRSA: Consider early addition of vancomycin, linezolid, VRE: Consider early addition of linezolid
Empirical antifungal therapy and investigation for invasive fungal infections should be considered for patients with persistent or recurrent fever after 4–7 days of antibiotics and whose overall duration of neutropenia is expected to be > 7 days
Hand hygiene is the most effective means of preventing transmission of infection in the hospital.
Standard barrier precautions should be followed for all patients, and infection-specific isolation should be used for patients with certain signs or symptoms.
Plants and dried or fresh flowers should not be allowed in the rooms of hospitalized neutropenic patients.
Avoid attending to patient if health care workers are ill.
