antimicrobial overview- background informationenp-network.s3.amazonaws.com/rrap/2014_handouts/talk...
TRANSCRIPT
1
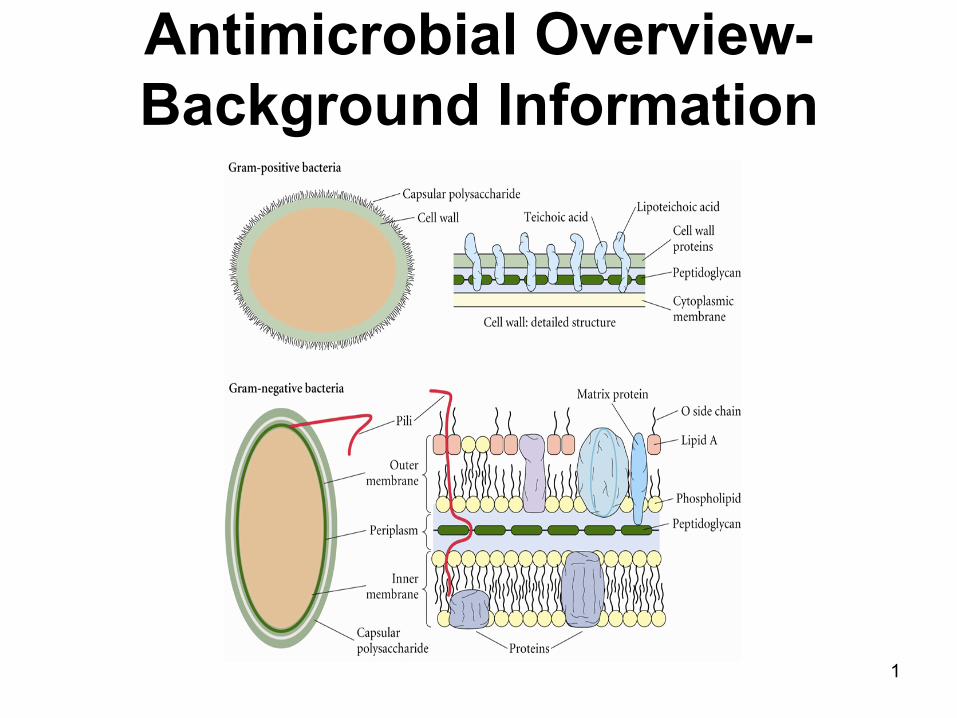
Antimicrobial Overview-Background Information

2
Objectives
• Learn the bugs (a very brief review) • To learn the characteristics of
antimicrobials – Mechanism of action – Pharmacokinetics – Spectrum of activity – Adverse drug effects – Any other fascinating tidbits
• Learn how to get the drugs to kill the bugs
3
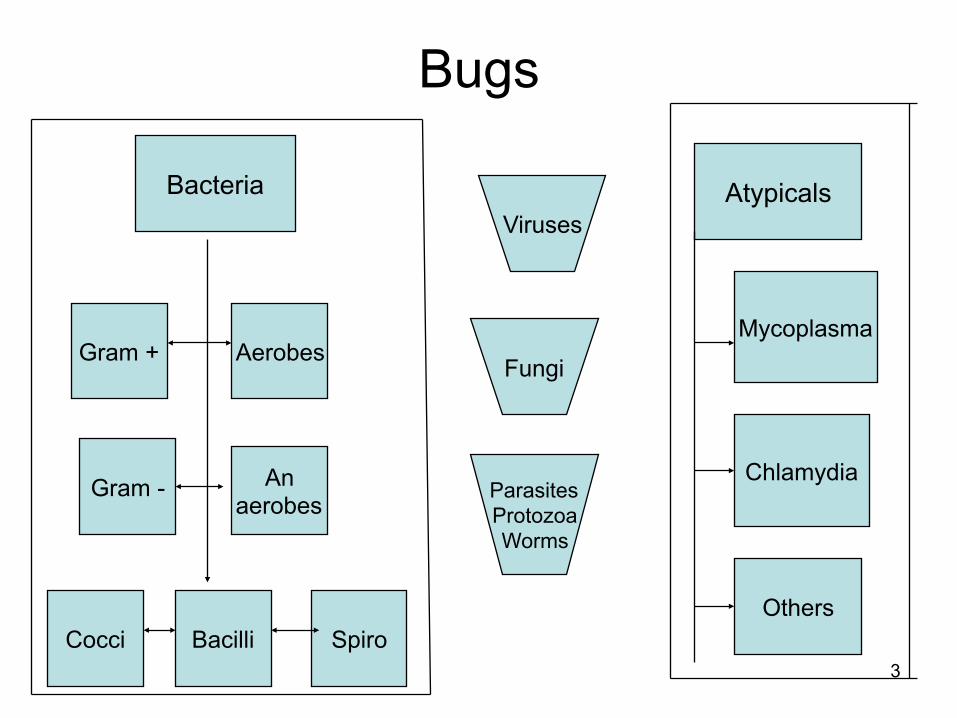
Bugs
Bacteria
Gram + Aerobes
Gram - An aerobes
Cocci Bacilli Spiro
Viruses
Fungi
Parasites Protozoa Worms
Atypicals
Mycoplasma
Chlamydia
Others

4
The difference between Gram (+) and Gram (-) organisms
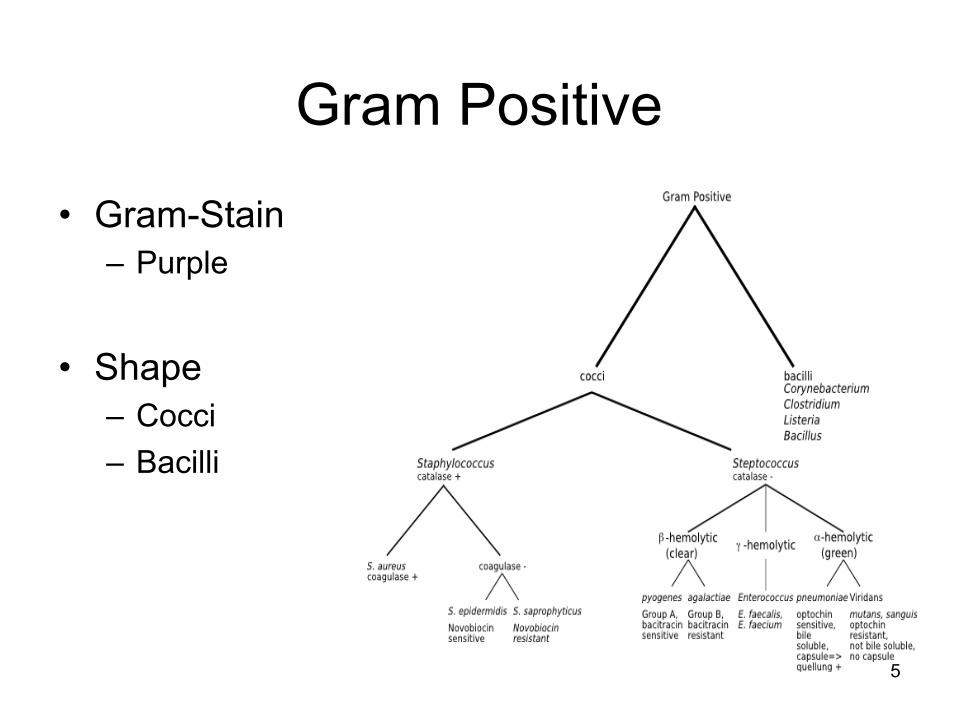
Gram Positive
• Gram-Stain – Purple
• Shape – Cocci – Bacilli
5

6
Gram Positive Cocci
• Staphylococcus – aureus
• Methicillin-sensitive (MSSA) • Methicillin-resistant (MRSA) • Vancomycin-intermediate (VISA) {fairly rare} • Vancomycin-resistant (VRSA) {very rare}
– epidermidis • Methicillin-resistant (MRSE)

7
Gram Positive Cocci
• Streptococcus – pneumoniae
• Penicillin resistant streptococcus pneumoniae (PRSP) – pyogenes (Group A, GABHS) – agalactiae (Group B, GBS) – Viridans Streptococci
• Enterococcus
– Faecalis, faecium • Vancomycin-resistant enterococcus (VRE)
– Usually facecium

8
Gram Positive Bacilli
• Corynebacterium diphtheriae
• Propionibacterium acnes
• Listeria monocytogenes

Gram Negative
• Gram-Stain – Red
• Shape – Coccobacilli – Cocci – Bacilli
9

10
Gram negative cocci
• Neisseria – meningitidis – gonorrhoeae
• Moraxella catarrhalis (cocco-bacillus)

11
Gram negative bacilli (bacilli=rods)
• Proteus – vulgaris (indole-positive) – mirabilis, M morganii (indole-negative)
• E. coli • Enterobacter species • Acinetobacter species • Klebsiella pneumoniae • Serratia marcescens

12
Gram negative bacilli Enteric bacteria
• Salmonella typhi
• Shigella sp.
• Campylobacter jejuni
• E. coli (0157:H7)
13
Gram negative bacilli Pseudomonads
• Pseudomonas aeruginosa
• Stenotrophomonas maltophilia
• Aeromonas hydrophilia

14
Gram negative bacilli
• Haemophilus influenzae
• Legionella pneumophilia
• Gardnerella vaginalis
• Helicobacter pylori
15
Anaerobes
• Bacteroides fragilis
• Clostridium difficile

16
Encapsulated organisms
• Streptococcus pneumoniae
• Haemophilus influenzae
• Neisseria sp.
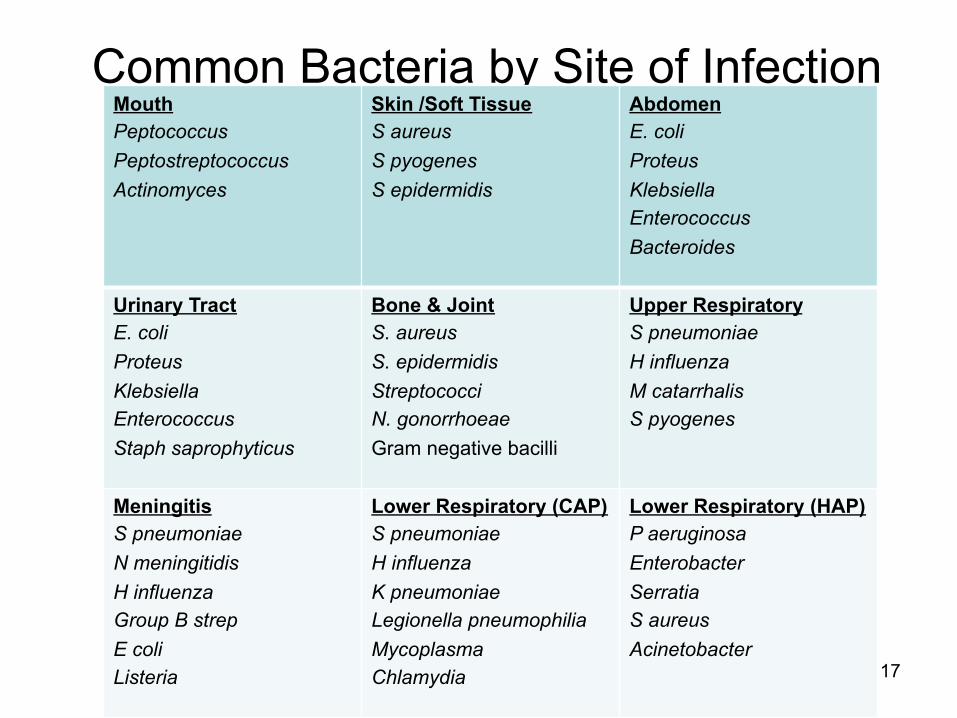
Common Bacteria by Site of Infection Mouth Peptococcus Peptostreptococcus Actinomyces
Skin /Soft Tissue S aureus S pyogenes S epidermidis
Abdomen E. coli Proteus Klebsiella Enterococcus Bacteroides
Urinary Tract E. coli Proteus Klebsiella Enterococcus Staph saprophyticus
Bone & Joint S. aureus S. epidermidis Streptococci N. gonorrhoeae Gram negative bacilli
Upper Respiratory S pneumoniae H influenza M catarrhalis S pyogenes
Meningitis S pneumoniae N meningitidis H influenza Group B strep E coli Listeria
Lower Respiratory (CAP) S pneumoniae H influenza K pneumoniae Legionella pneumophilia Mycoplasma Chlamydia
Lower Respiratory (HAP) P aeruginosa Enterobacter Serratia S aureus Acinetobacter 17
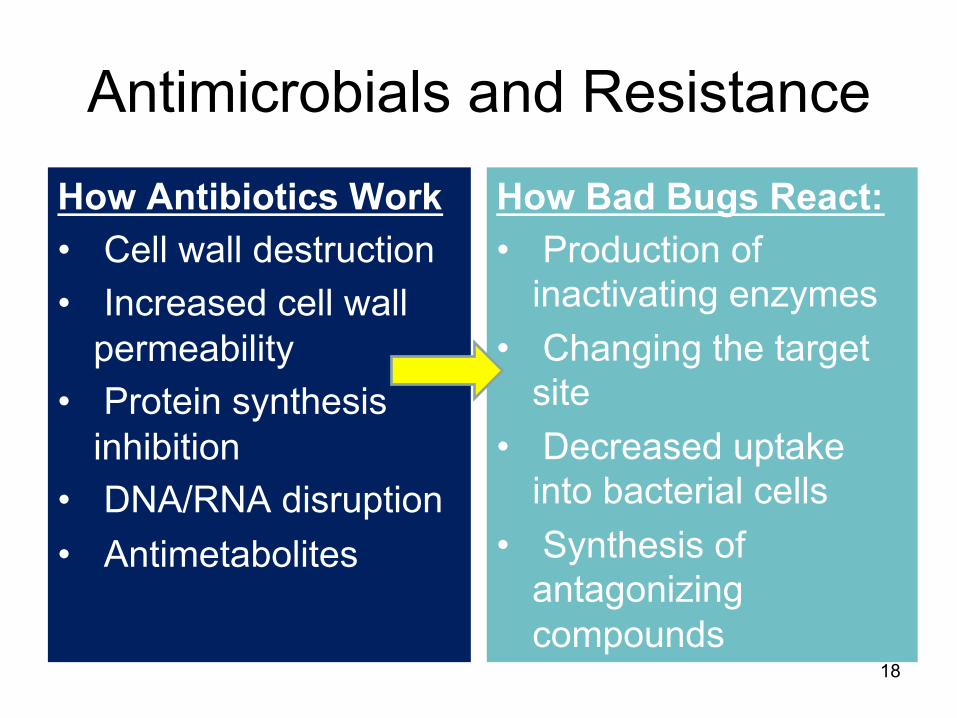
Antimicrobials and Resistance
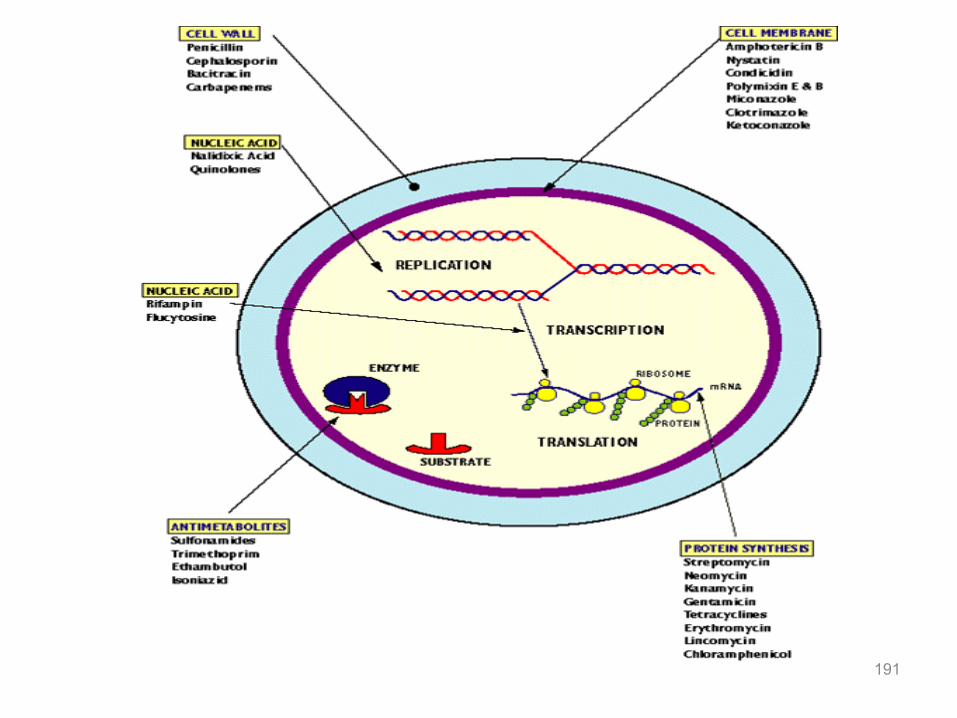
How Antibiotics Work • Cell wall destruction • Increased cell wall
permeability • Protein synthesis
inhibition • DNA/RNA disruption • Antimetabolites
How Bad Bugs React: • Production of
inactivating enzymes • Changing the target
site • Decreased uptake
into bacterial cells • Synthesis of
antagonizing compounds
18

Ribosomes
(Proteins)
2. Penetrate Cell
3. Reach Target and Kill
Organism
Bacterium
Requirements for Antimicrobial Activity
Antibiotics
1. Reach site of infection
Porin Proteins
PBPs DNA gry Topo IV
Feldstein TJ 00 19
Four Main Types of Resistance
• Decreased Permeability • Drug Efflux • Drug Inactivation • Altered Target
20

• Decreased Permeability • Drug Efflux • Drug Inactivation • Altered Target
Ribosomes
(Proteins)
Mechanisms of Resistance
Bacterium
Porin Channels (Gram-negatives)
Antibiotics
Antibiotics Porin channels closed or decreased number
Example: Pseudomonas aeruginosa
DNA gry Topo IV
Feldstein TJ 00 21

• Decreased Permeability • Drug Efflux • Drug Inactivation • Altered Target
Ribosomes
(Proteins)
Feldstein TJ 00
Mechanisms of Resistance
Bacterium
Antibiotics
Examples: 1. S. pneumoniae vs. Macrolides and Quinolones 2. E. coli vs. Quinolones
Efflux Pump
DNA gry Topo IV
22

• Decreased Permeability • Drug Efflux • Drug Inactivation • Altered Target
Ribosomes
(Proteins)
Mechanisms of Resistance
Bacterium
Antibiotics
Examples: - Beta-lactamase (H. flu, M. cat) - Aminoglycoside modifying enzymes (Pseudomonas)
Enzymes
DNA gry Topo IV
Feldstein TJ 00 23

Ribosomes
(Proteins)
2. Penetrate Cell
3. Reach Target and Kill
Organism
Porin Proteins
Pencillin-Binding Proteins (PBPs)
(β-lactams)
DNA gry Topo IV
Feldstein TJ 00
DNA Gyrase Topoisomerase IV
• Decreased Permeability • Drug Efflux • Drug Inactivation • Altered Target
Mechanisms of Resistance
Ribosomal Mutation (Macrolides)
24
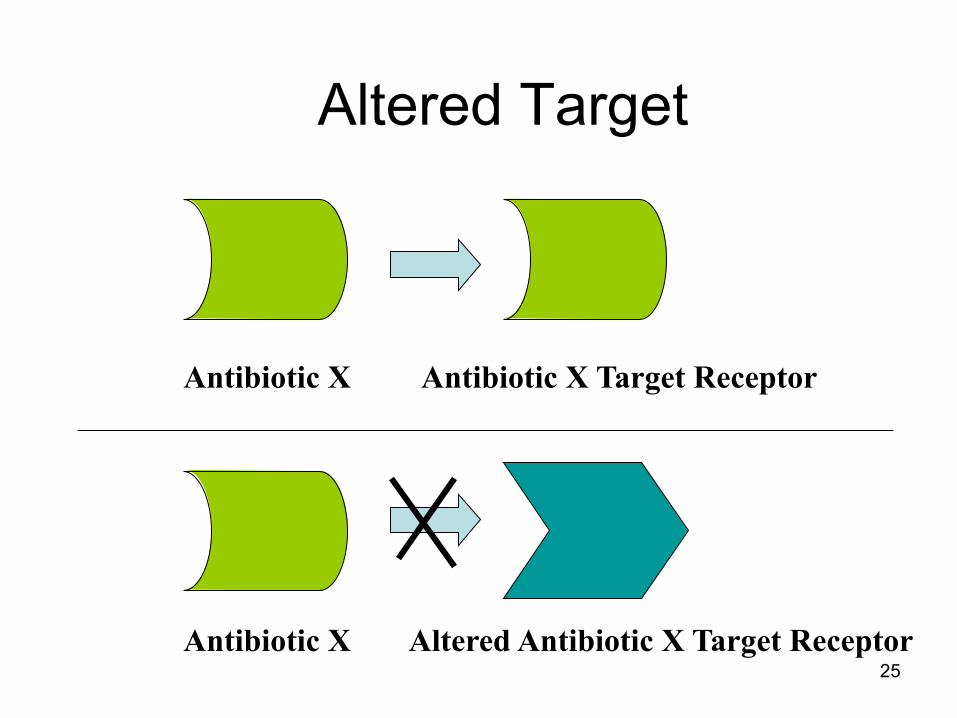
Altered Target
Antibiotic X Target Receptor Antibiotic X
Antibiotic X Altered Antibiotic X Target Receptor 25

Terms
• Bacteriostatic
• Bacteriocidal
• Colonization
• Synergy
• Antibiogram
• Prophylaxis
• Empiric
• Targeted
• Definitive 26
Antibiotic Activity and Effectiveness are determined by...
• MIC (minimal inhibitory concentration) – in vitro potency of the drug
• Pharmacokinetics – “What the body does to the drug” – Absorption, Distribution, Metabolism, Elimination
• Pharmacodynamics – “What the drug does to the body/organism” – Time-kill profile
27

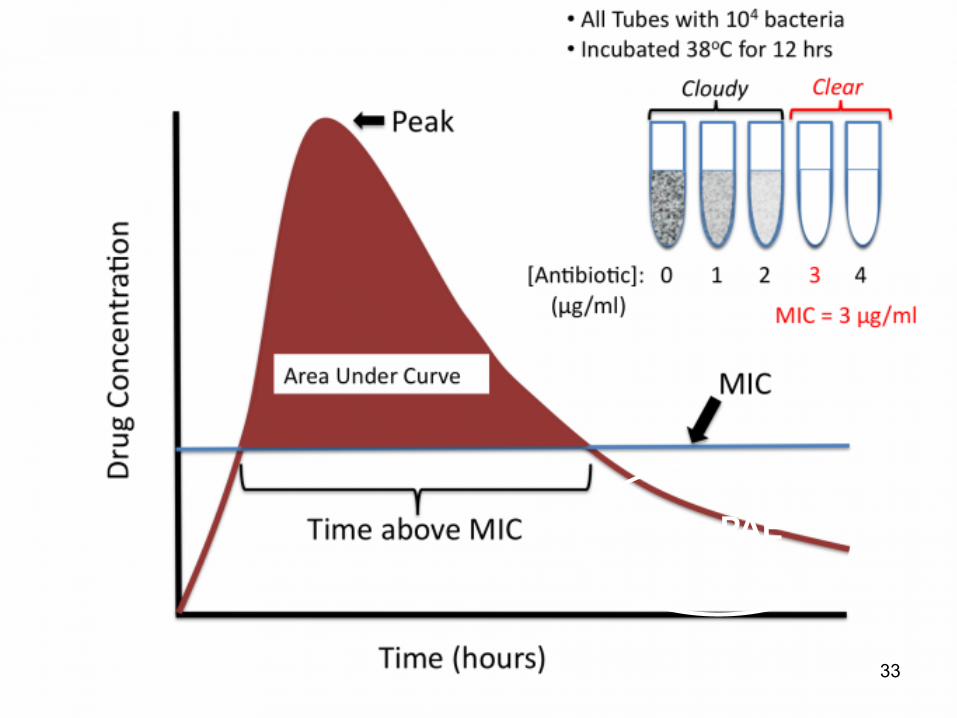
General Definitions • The minimum inhibitory concentration (MIC)
is the minimum concentration of the antibacterial agent in a given culture medium below which bacterial growth is not inhibited
• The therapeutic index is the plasma or tissue toxic concentration divided by the MIC.
• Post-antibiotic effect (PAE) means the continued inhibition of the organism for a period of time after the concentration of the antimicrobial agent has dropped below the MIC.
28

• Definition: The lowest antibiotic concentration required to visually inhibit bacterial growth following an overnight incubation.
Susceptibility Testing Minimal inhibitory concentration (MIC)
Broth: 104-105 CFU/ml (pathogen)
0.25 ug/ml 0.5 ug/ml 1 ug/ml 2 ug/ml 4 ug/ml 8 ug/ml 16 ug/ml Antibiotic Conc
29

Susceptibility Testing • Determining the MIC
– Methods: • Organism is placed in broth solution
– Turbidity = microbial growth – Adding antibiotic à no turbidity
• Agar solution • Epsilometer strip (E-test) • Automated systems
– Micro lab uses CLSI guidelines to determine whether a organism is “susceptible”, “intermediate”, or “resistant”
Zone of inhibition
correlates to MIC
CLSI= Clinical and Laboratory Standards Institute 30

MIC Breakpoints
• CLSI Guidelines – Different for each organism for each antibiotic! – Susceptible – Intermediate – Resistant
• Can concentration be met in the body? – At infection site?
31

MIC Drug Concentrations
0
1
2
3
4
5
6
7
8
9
Control
2x MIC
4x MIC
Time in Hours
Log
Col
ony-
Form
ing
Uni
ts /
mL
General Understanding that Drug Concentration greater than 4-5 fold
higher than the MIC, lack of increased organism killing for TIME DEPENDENT
Antibiotics 32
PAE
33

MICs and Pharmacodynamics…in English
• Pharmacodynamics – Can we achieve MIC-achieving abx
concentration in body safely? • Too much drug à toxicities
– Typical killing characteristics of a drug: • Time above MIC (ex. Beta-lactams) • AUC/MIC • Peak/MIC
34 AUC= area under the curve

Another view-Pharmacokinetic/pharmacodynamic parameters
affecting abx potency
http://www.antimicrobe.org/h04c.files/history/PK-PD%20Quint.pdf 35

Antibiograms: The Susceptibility “Report Card”
• Represents how often a drug has activity against the organism (as a percentage)
• Useful for empiric therapy • Consider:
– Which agents have highest likelihood of being active – Which agent will penetrate site of infection – Are there patient factors that exclude the drug of choice
(allergies, renal toxicity risk, etc.)
Gentamicin Piperacillin/ Tazobactam
Cefepime Ciprofloxacin
Pseudomonas aeruginosa 80 89 91 82 Klebsiella pneumoniae 92 95 96 90
36

Antibiotic Activity
• Killing Properties – Time-dependent killing – Concentration-dependent killing
• Mechanism of Action – Generalizations but different between most
classes
37

Time Dependent or Concentration-Dependent Killing
• Concentration-dependent Killing
• Increasing the dose, increases the bactericidal effect
– Quinolones – Aminoglycosides – Azalides (eg. azithro) – Streptogramins – Glycylcylines – Oxazolidinones
• Time Dependent (aka Concentration-independent Killing)
• There is an upper limit of 4-5
times the MIC in which concentration-dependent effect is seen; further increases produce little additional killing – β -lactams – Macrolides – TMP/SMX
38
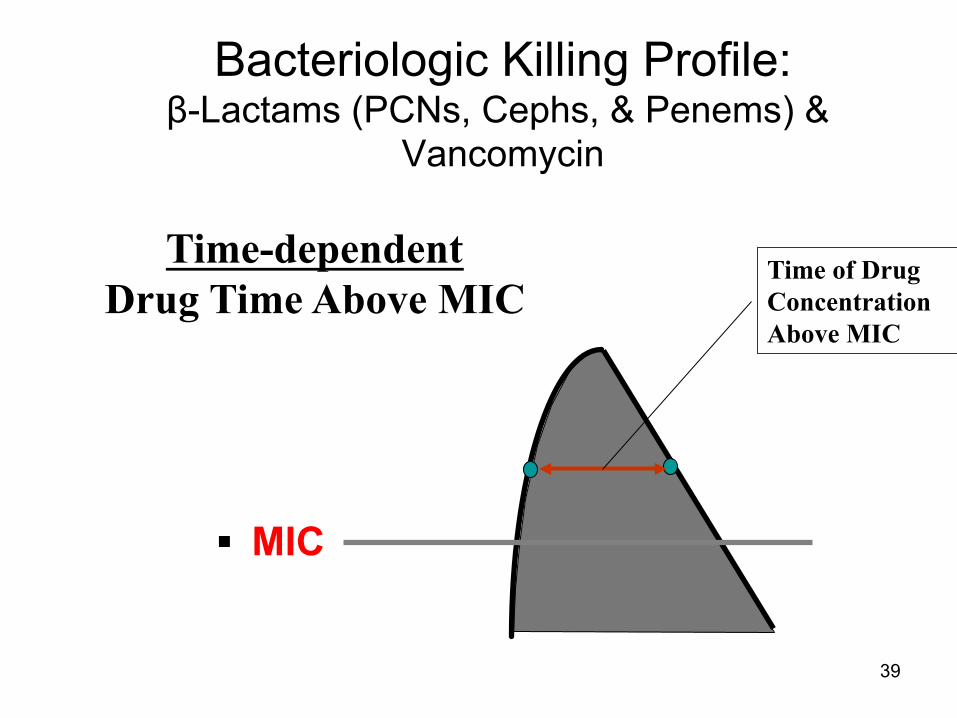
Bacteriologic Killing Profile: β-Lactams (PCNs, Cephs, & Penems) &
Vancomycin
Time-dependent Drug Time Above MIC
Time of Drug Concentration Above MIC
§ MIC
39

Bacteriologic Killing Profile: Aminoglycosides, Fluoroquinolones
Concentration-dependent Concentration of Drug at Target Site
Peak Concentration of Drug
§ MIC
40
Antimicrobial Stewardship
• Involves the optimal selection, dose, and duration of an antibiotic
• Minimal unintended consequences – Emerging resistance – Adverse drug events (ex. C. diff) – Cost
• Goal: improve patient care and healthcare outcomes
41

Antimicrobials Principles • De-escalation/streamlining
– After cultures and susceptibilities return, guide clinician in transitioning from broad spectrum to narrow spectrum
• Dose optimization via PK/PD – Ex. Levofloxacin 750mg daily for Community
Acquired Pneumonia (adjust for renal fxn) • IV to PO switch
– Reduces line-related infection – Can decrease length of stay – Cost savings 42

Other Tips • Clarify infection vs colonization vs
contaminants – Ex. UTIà was urine culture from catheter?
Was culture only yeast with a catheter in place? Does patient have UTI symptoms?
– Ex. Tracheal aspirates à ICU pts are frequently colonized; other signs/symptoms are helpful
• WBC? Fever? New infiltrate on chest x-ray?
• If “broadening therapy,” draw new cultures before antibiotics administered 43

44

45 Slide from Nancy Baily, Pharm.D. Sep 2005
Carbapenems, Monobactams, Vancomycin
Clindamycin, Linezolid, Synercid, Tigecycline
Colistin Metronidazole

46
Drugs
Beta-Lactam Antibiotics Pencillins Cephalosporins Monobactams Cephamycins Carbapenems
Tetracyclines Fluoro-
quinolones
Aminoglycosides Macrolides
Sulfonamides
Miscellaneous
Vancomycin
Metronidazole
Bacitracin Polymyxin
Chloramphenicol
Linezolid

β-Lactams
• Penicillins
• Cephalosporins
• Carbapenems
• Monobactams
47

Meet the Beta-Lactam All-Stars Penicillins Cephalosporins Carbapenems “Natural Penicillins” 1st- generation Imipenem
Meropenem Doripenem
Penicillin G & Penicillin V Cefazolin & Cephalexin Anti-staph penicillins 2nd-generation Nafcillin & Dicloxacillin Cefuroxime Ertapenem Aminopenicillins Cefotetan & Cefoxitin Ampicillin & amoxicillin 3rd-generation Monobactams Ampicillin/sulbactam & Amoxicillin/clavulanate
Ceftriaxone & Cefotaxime Aztreonam Ceftazidime
Antipseudomonal penicillins 4th-generation Piperacillin/tazobactam Cefepime
“5th-generation” Ceftaroline
48
β-lactams • Mechanism of action
– Interferes with cell wall synthesis – Binds penicillin-binding proteins (PBPs)
• Leads to inhibition of peptidoglycan synthesis
• Class adverse effects – hypersensitivity – rare seizures (at high doses) – interstitial nephritis – bone marrow suppression (rare)
• Time-dependent bacteriocidal activity
Penicillins Cephalosporins Carbapenems Monobactams
49

50
The Penicillins

51
The Beta-lactam Ring

Natural Penicillins
Penicillin G Pen VK (PO)
Gram-positive Pen-susc S. aureus Pen-susc S. pneumoniae Streptococci Enterococcus
Gram-Negative Neisseria
Anaerobes (Above the diaphragm) Clostridium
Other Treponema pallidum Syphilis
52

Penicillinase-Resistant Penicillins
Nafcillin Oxacillin
Methicillin* Dicloxicillin (PO)
Gram-positive Methicillin-susceptible Staph. aureus Viridans streptococci (less than natural penicillins) NO enterococci
• Developed to overcome the penicillinase enzyme of S. aureus which inactivated natural penicillins
• Preferred for beta-lactamase + MSSA
*Methicillin-no longer available 53

Aminopenicillins Ampicillin Amoxicillin (PO)
Gram-positive Pen-susc S. aureus Group streptococci Viridans streptococci Enterococcus sp Listeria monocytogenes
Gram-Negative Proteus mirabilis Salmonella Shigella E. coli H. influenza
• Developed to increase activity against gram-negatives • Major uses:
– Endocarditis (usually given in combo with gent) – Empiric:
• Meningitis (Listeria)- Ampicillin IV for age <3 or >50 years
54

Aminopenicillin + β-lactamase inhibitor
Ampicillin/sulbactam (IV) Amoxicillin/clavulanate (PO)
Gram-positive S. aureus (not MRSA) Anaerobes Bacteroides sp. (excellent)
Gram-Negative (β-lactamase producers) H. influenza E. coli Proteus sp. Klebsiella sp.
• Developed to overcome resistance from β-lactamase producing gram-negatives
• Sulbactam – beta lactamase inhibitor • Clavulanate – beta lactamase inhibitor
55

Extended-spectrum Penicillins + β-lactamase inhibitor Piperacillin/tazobactam
Ticarcillin/clavulanate Gram-positive S. aureus (Not MRSA) Anaerobes Excellent activity Bacteroides sp.
Gram-Negative (β-lactamase producers) H. influenza E. coli Proteus mirabilis Salmonella Shigella P. Aeruginosa Enterobacter Stenotrophomonas (Ticarcillin/clavulanate) • Added Pseudomonas coverage
• Major uses: – Intra-abdominal infections – Pneumonia (Piperacillin/Tazobactam)
56

57
Beta-lactamase Inhibitors • Sulbactam, Clavulanate (clavulanic acid), and
Tazobactam • Binds to and inhibits beta-lactamases which
destroy penicillins • Piperacillin/tazobactam- Zosyn (IV only) • Ampicillin/sulbactam-Unasyn (IV only) • Ticarcillin/clavulanate (IV only) • Amoxicillin/Clavulanate acid-Augmentin (oral
only)
Beta-Lactamase Inhibitors • Tazobactam
– Piperacillin/tazobactam (IV) • Wide range of G(+)
– MSSA, Strep spp, enterococcus • Wide range of G(-)
– Pseudomonas, Serratia, Enterobacter • Anaerobes: great for Bacteroides fragilis • Can prolong infusion (3-4hrs) to increase T>MIC; q8h • Renal adjustment needed • Uses: Pseudomonas infections, intra-abdominal, febrile
neuptropenia, healthcare associated pneumonia (HCAP)
58

59
Mechanism of Action • Inhibit bacterial cell wall synthesis
– binding to 1 or more of the penicillin-binding proteins (PBP)
• PBP are a normal part of many bacteria
– inhibits final transpeptidation step in peptidoglycan synthesis
• Peptidoglycans is major component of bacterial cell wall – bacteria lyse due to ongoing activities of cell wall
autolytic enzymes – cell wall assembly arrested
• Bacteriocidal

60
Mechanisms of Resistance
• Failure to penetrate the outer membrane – Alterations in PBPs
• Production of beta-lactamases

Resistance: Beta-Lactamase
61
62
Spectrum of Activity - summary • Natural
– mostly Gram (+) – some anaerobes
• PCNase-resistant – Staphylococci – Streptococci
• Aminopenicillins – mostly Gram (+) – some Gram (-) – some anaerobes
• Extended Spectrum – Gram (+), but not as
good as other groups – Excellent Gram (-)
coverage – Anaerobes

63
Pharmacokinetics • Oral Bioavailability of
20-60% • Half-lives of all
penicillins are short, typically 30-60 min – require q4-6h dosing
• Excellent tissue distribution
• < 80% protein binding, except for PRPs (>90%)
• Eliminated primarily by renal (Glomerular Filtration and Tubular Secretion) except for oxacillin and nafcillin, which are extensively metabolized via the liver – Note: there is no need
to dose adjust oxacillin or nafcillin in patients with renal impairment

64
Indications • Pneumonia • Group B streptococcal disease prevention • URI • Bronchitis (acute/chronic) • Otitis media • Sinusitis • Pharyngitis • UTI • Skin/tissue infections • Meningitis • Endocarditis • H.Pylori infections • Dog and cat bites (mostly amoxillin/clav acid)
65
Adverse Effects
• IgE-mediated Hypersensitivity – Anaphylaxis – Accelerated (early)
skin rashes • “Late” skin rashes • Serum Sickness Rxn • Drug-induced fever
• Hematologic effects • Diarrhea and CDAD* • Neuromuscular
effects • Nephropathy • ADEs specific to
certain penicillins • Cross sensitivity to
cephs, carbapenems – Important to know rxn
*CDAD=clostridium difficile associated disease

66
The Cephalosporins

67
Beta Lactam ring

Cephalosporins
• Disrupt bacteria cell wall
• Divided into 4 or 5 generations
• Antibacterial activity varies between generations and agents
• Resistance (drug inactivation vs. altered target)
68

69
1st Generation Cephalosporins
Injectables • Cefazolin
(Ancef®, Kefzol®) • Cephalothin
(Keflin®) • Cephapirin
(Cefadyl®) • Cephradine
(Velosef®)
Orals • Cephalexin
(Keflex®) • Cefadroxil
(Duricef®)
70
1st Generation Cephalosporin coverage includes...
• Activity similar to PRP vs staph and strep – Most activity against gram positives
• Limited gram-negative coverage, including E. coli, Proteus mirabilis, and Klebsiella (many strains are now resistant)
• No significant differences in spectrum of activity among the first-generation cephalosporins
• Susceptible to β-Lactamases
71
2nd Generation Cephalosporins
Injectables • Cefuroxime (Zinacef®,) • Cefamandole
(Mandol®) • Cefonicid (Monocid®) • Cefmetazole
(Zefazone®) • Cefoxitin (Mefoxin®) • Cefotetan (Cefotan®)
Orals • Cefaclor (Ceclor®) • Cefuroxime axetil (Ceftin ®) • Cefprozil (Cefzil®) • Loracarbef (Lorabid®)
2nd Generation Cephalosporins
• Cefotetan, Cefoxitin, Cefuroxime, Loracarbef, Cefaclor, Cefprozil – Loracarbef & Cefprozil Susceptible to β-
Lactamases
• Gram-positive organisms – Variable activity against Staphylococci – No Enterococcus coverage
• Broader Gram-negative coverage – No Pseudomonas coverage
72

73
Cephalosporin Generations
• Gram(+) Coverage – 1st: +++ – 2nd: ++ – 3rd: +
• Gram (-) Coverage – 1st: + – 2nd: ++ – 3rd: +++
• Anaerobic Coverage – 1st: 0 – 2nd: +++ – 3rd: +/-
Notice the pattern!
74
2nd Generation Cephs cover...
• Slightly lower activity against S. aureus when compared to 1st gen
• Increased activity against Gram (-) such as E. coli, Proteus, and Klebsiella, as well as, Haemophilus influenzae
• Cephamycins (cefmetazole, cefoxitin, and cefotetan) also add additional coverage against anaerobes such as Bacteroides fragilis
2nd Generation Cephalosporins
• Cephamycins – Cefoxitin – Cefotetan
• Gram-negative organisms • Gram-positive organisms
– No Enterococcus coverage • Additional anaerobic coverage
75
76
3rd Generation Cephalosporins Injectables • Cefotaxime (Claforan®) • Ceftriaxone (Rocephin®) • Ceftizoxime (Cefizox®) • Cefoperazone (Cefobid®) • Ceftazidime (Fortaz®) • Cefepime (Maxipime®)
– considered by some to be a “fourth” generation cephalosporin
Orals • Cefixime (Suprax®) • Ceftibuten (Cedax®) • Cefdinir (Omnicef®) • Cefpodoxime
(Vantin®)

77
Bacterial Coverage of the 3rds...
• Excellent Gram (-) coverage • Two categories: those which kill
Pseudomonas aeruginosa (cefoperazone, ceftazidime, cefepime) and those that do not
• Ceftazidime has poorest activity against Gram (+)
• Cefotaxime has best activity vs Gram (+) • Ceftizoxime has best activity vs anaerobes
3rd Generation Cephalosporins • Ceftazidime, Ceftriaxone, Ceftizoxime,
Cefotaxime, Cefixime
• Cefixime – susceptible to β-Lactamases
• Ceftriaxone and Cefotaxime – Fine for community-acquired infections – ?Nosocomial
• Ceftazidime – Pseudomonas-be aware of resistance; 2gm IV Q8hr – Weak Gram + coverage – Susceptible to Amp C and ESBLs
78

4th Generation Cephalosporins
• Cefepime – Others investigational only – Like ceftriaxone and ceftazidime together
• Does have Pseudomonas coverage – Decent Gram + coverage, less affected by
type 1 mutations – ?Susceptibility to β-Lactamases – Dosing
• 1gm IV Q12hr - 2gm IV Q8hr
79
80
1st-4th generation Cephalosporins Do Not cover….
• Methicillin-resistant Staphylococcus aureus or epidermidis
• Enterococci • Listeria monocytogenes • Legionella pneumophilia • Stenotrophomonas maltophilia

“5th” generation Cephalosporin
• Injectable • Ceftaroline (Teflaro®) • Not allowed to call themselves “5th” per
FDA
81

5th generation-approved 11/10 • Ceftaroline (Teflaro®) • Community-acquired bacterial pneumonia
(CABP) caused by: – Streptococcus pneumoniae, Staphylococcus aureus
(MSSA only) ,Haemophilus influenzae, Klebsiella pneumoniae, Klebsiella oxytoca, Escherichia coli
• Acute bacterial skin and skin structure infections (ABSSSI) caused by: – Staphylococcus aureus (including MRSA),
Streptococcus pyogenes,Streptococcus agalactiae, Escherichia coli,Klebsiella pneumoniae, Klebsiella oxytoca
82

Ceftaroline • Quite active against most Gram-positive cocci including
MRSA, Coag-neg Staph (methicillin resistant), and PNSP. • MRSA activity is due to high binding affinity for PBP2a. • Gram-negative activity resembles ceftriaxone • The drug is poorly active vs. P. aeruginosa and Acinetobacter • Ceftaroline-demonstrates good-to-excellent activity against
Gram-positive anaerobic pathogens (Clostridium & Peptostreptococcus) but poor activity against Gram-negative anaerobic pathogens, particularly members of the B. fragilis group.
• Has been described as a short half-life version of ceftriaxone with souped-up Gram-positive activity including MRSA. Dosage: 600mg IV q12hrs for adults > 18
– Adjust dosage in renal patients
83

84
Mechanism of Action of Cephalosporins
• Inhibit bacterial cell wall synthesis – binding to 1 or more of the penicillin-binding proteins
(PBP) – Inhibits the final transpeptidation step in
peptidoglycan synthesis – bacteria eventually lyse due to ongoing activities of
cell wall from autolytic enzymes – cell wall assembly is arrested

85
Mechanisms of Resistance
• Decreased penetration of cell wall
• Altered target site • Inactivation by beta-lactamases

86
Pharmacokinetics-Cephs
• Widely distributed – 3rd generation agents cross the Blood Brain
Barrier to treat meningitis • All 1st & 2nd, and most 3rd (except
cefoperazone, and ceftriaxone) are eliminated renally
• None of the cephalosporins are bound to plasma proteins to an extent that they will displace highly protein-bound drugs

87
Indications
• Otitis media • Sinusitis • STDs • UTIs • Skin/Tissue • Pneumonia • Meningitis

88
Adverse Effects • Hypersensitivity
similar to PCNs – cross-sensitivity:
0-10% – most with PCN allergy
can take cephalosporin
• Thrombocytopenia • Liver function tests • CDAD
– 3rds are most common cause
• Ceclor Reaction • Pseudocholelithiasis
– Ceftriaxone
• Disulfiram-like Rxn – NMTT side chain – Cefamandole,
cefotetan, cefmetazole • Hypoprothrombinemia
– NMTT side chain

Cephalosporin Clinical Pearls
• Many oral and IV formulations • No Coverage for Enterococcus • 3rd Generation Cephalosporins are
susceptible to ESBL producing organisms • Some 2nd Generation Cephalosporins are
effective for Gram (–) organisms AND Anaerobic organisms
89

Cephalosporin Summary 1st Gen. 2nd Gen. 3rd Gen. 4th Gen.
Cephalexin Cefoxitin Ceftazidime Cefepime
Cefazolin Cefotetan Ceftriaxone
Cefaclor Cefuroxime Ceftizoxime
Cephalothin Loracarbef Cefotaxime
Cefprozil Cefixime
Increasing Gram-positive Coverage – No Cephalosporin covers Enterococcus
Increasing Gram-negative Coverage
90

The Carbapenems
91

Representative antibiotics
• Imipenem/cilastatin (Primaxin®) • Meropenem (Merem®) • Ertapenem (Invanz®) • Doripenem (Doribax®)
92

Mechanism of Action-Carbapenems
• Inhibits bacterial cell wall synthesis by binding to PBPs
• Preferentially binds to PBP 1 and PBP 3 • Highly resistant to degradation via
beta-lactamases
93

Mechanisms of Resistance-Carbapenems
• Reduced binding to PBPs • Decreased penetration of
periplasmic space • Inactivation via
carbapenemases
94

Spectrum of Activity-Imipenem, Doripenem, Meropenem
• “Gorilla” cillin – the broadest spectrum
of activity of all available antibiotics
• Excellent coverage of staphylococci and streptococci
• Don’t use vs MRSA, MRSE, enterococci, or Listeria
• Stenotrophomonas maltophilia is innately resistant - produces carbapenemase!
• Highly active against all obligate anaerobes
• Pseudomonas aeruginosa often becomes resistant during therapy
95
Resistance to carbapenems • Organisms from the Enterobacteraciae family
are increasingly producing carbapenemases that are rendering carbapenems ineffective.
• Original name was KPCs because it was most often isolated from Klebsiella pneumonia.
• Name has changed to CRE to represent carbapanem resistant enterobacteraciae (not just from Klebsiella any more)
• Note other MDROs can be resistant to carbapenems as well
96

When should carbapenems be used??? – Imipenem, doripenem, meropenem
• Do not use indiscriminately!!!!
• Monotherapy for infections in which other antibiotics have failed
• Empiric therapy in critically ill, immunocompromised patients if resistant bugs anticipated
• Must renal dose all • Will see many institutions
use only one
• Directed therapy against organisms known to be resistant to other agents
• In general, imipenem should not be used in combination with other antibiotics – no synergy with AGs – strong inducer of beta-
lactamases
97

Ertapenem (Invanz®) • Indicated for the following moderate to
severe infections: – Diabetic foot infections without osteomyelitis – Complicated intra-abdominal infections – Complicated skin/skin structure infections – Community-acquired pneumonia – Acute pelvic infections – Complicated urinary tract infections – Prophylaxis of Surg. Site infxn following
elective colorectal surgery – No activity against Pseudomonas
98

Pharmacokinetics – Imipenem/cilastatin • Eliminated almost exclusively via
glomerular filtration and tubular secretion • It is very important to dose adjust in
patients with renal dysfunction because of a particularly nasty ADR (which we’ll discuss in more detail shortly)
• Cilastatin prevents the degradation by renal peptidase dehydropeptidase-1 in the proximal tubules of the kidneys –this enzyme will hydrolyze imipenem
99

Adverse Effects - Imipenem • Gastrointestinal
– most common (n/v/d) – rapid infusion may
increase • Neurologic
– SEIZURE! • CNS Disease • High dose in elderly and
renal dysfunction • concurrent theophylline • If carbapenem treatment
required-meropenem may be an option (renal dose)
• Other – hypersensitivity
• rash • pruritus • urticaria • drug fever • cross-reactivity with
other beta-lactams – Leukopenia – Thrombocytopenia
100

Indications-Imipenem • Lower RTI
– S. aureus, acinetobacter sp, enterobacter sp, E.coli, H. flu, Kleb sp, and Serratia marcescens
• Intra-abdominal infections
• Skin and skin structure
• Gynecologic
• Septicemia – E. faecalis, S. aureus,
enterobacter sp, E.coli, H. flu, Kleb sp, P. aeruginosa, serratia sp. And bacteriodes sp. Including B frag.
• Bone and bone joint • Polymicrobic
101

Doripenem (Doribax®)
• Indications – Comp. Intra-abdominal – Comp. UTI (inc. pyelo)
• Dosing – Adj. in renal patients
• Adverse Reactions – Hypersensitivity
• Similar to other carbapenems
– CDAD (Clostridium difficile associated disease)
• Drug Interactions – Valproic Acid (VA)
• Reduces conc. Of VA which could precipitate seizure activity
– Probenecid • Reduces renal
clearance of doripenem resulting in increased doripenem concentration
102

Meropenem (Merem®)
• Indications – Comp. intra-abdominal – Comp. skin and skin
structure infections
• Dosing – Adjust in renal patients
• Adverse Reactions – Headache, rash,
diarrhea, anemia – CDAD
• Drug Interactions – Probenecid: avoid use – Decrease level of:
• Valproic acid • Typhoid vaccine
103

Aztreonam (Azactam®) • The only marketed
monobactam • Binds preferentially to PBP
3 of Gram (-), so only activity
• Gram(-) coverage comparable to Aminoglycosides (AGs & 3rds gen. cephalosporins)
• Probably most suited as an alternative to AGs in patients with AG-R bugs or high-risk for AG Tx
• Most common ADEs are GI symptoms, mild skin rashes, and reversible elevations of LFTs
• Eliminated primarily via the kidneys
• May be inactivated by extended-spectrum beta-lactamases
• No cross-sensitivity with penicillins
• IV, no oral form
104

Clindamycin Cleocin®
105

Mechanism of Action
• Reversibly binds to the RNA of the 50S ribosomal subunit – prevents peptide bond formation – inhibiting protein synthesis
106
Mechanisms of Resistance
• Altered or mutation of target site
• Inactivation by bacterial esterases
107
Spectrum of Activity
• Aerobic gram positive cocci – staph aureus, staph epidermidis, streptococci,
pneumococci • Anerobic gram negative bacilli
– bacteroides • Anaerobic gram positive bacilli
– propionibacterium 108
Pharmacokinetics
• Bioavailability ~90% • Both IV and PO forms • Metabolized by liver • Not renally dosed (not renally excreted) • Does not cross blood brain barrier • Is a derivative of lincomycin so classifed
as Lincosamides • Wide distribution-CNS penetratation
109
Adverse Effects
• GI effects – Warning for pseudomembranous colitis
• Hypersensitivity rxns • Jaundice • Transient neutropenia, eosinophilia
110
Vancomycin (Glycopeptide)
111

Mechanism of Action
• Interferes with cell wall synthesis – disrupts cross-linkage of peptidoglycan
strands in the developing cell wall – also interferes with cytoplasmic RNA
synthesis – alters the permeability of the cytoplasmic
membrane
112
Mechanisms of Resistance
• Gram-negative bacteria • VRE
– VanA – VanB – VanC
• VISA/VRSA
113

Spectrum of Activity
• Staphylococci • Streptococci • Enterococci
• Bacillus • Corynebacterium • Clostridium • Listeria
114

Vancomycin
• Used clinically for over 45 years • Active against gram positive pathogens
– MRSA, MRSE – drug of first choice • Increasing resistant organisms observed
during 1990’s – e.g. VRE • Very few cases of VISA and VRSA • Other Glycopeptides-but they are not
commonly used at this time (e.g. televancin)
115

Vancomycin • Most common clinical uses
– Exclusively for gram positive infections – Drug of first choice for MRSA, MRSE regardless of infection site
BUT not drug of choice for MSSA. Nafcilin or oxacillin is a better choice for MSSA (hint: check allergies: can’t give nafcillin or oxacillin in a patient with a true penicillin allergy)
– Often added empirically in cases of suspected bacterial meningitis along with 3rd generation cephalosporins
– Bone and joint infections • Infected prosthesis infections for methicillin-resistant
pathogens – Surgery prophylaxis if PCN allergic patient – PO: Clostridium difficile-after metronidazole tried first (i.e. 2nd line)
116

Appropriate Use of Vancomycin
• Beta-lactam resistant bacteria
• Serious allergy to beta-lactams
• CDAD which fails metronidazole or is severe and life-threatening
• Prophylaxis for endocarditis following certain procedures
• Prophylaxis for major surgical procedures involving implantation of prosthetic material or devices with a high rate of MRSA or MRSE infections
117
Vancomycin • Displays time-dependent pharmacodynamic/
bactericidal activity • Few published, prospective trials associating
vancomycin serum levels and clinical response
• Dosing should be individualized (often dosed by pharmacy)
• Established peak and trough ranges based primarily on clinical observations
• Trough levels most commonly used to monitor therapy for safety and efficacy at this time.
118

Inappropriate Uses • Routine surgical
prophylaxis • Single positive BC for
coag(-) staph – likely a contaminant
• Continued empiric therapy with negative cultures for MRSA/MRSE
• First-line tx of CDAD • Prophylaxis for infection or
colonization of catheters • Eradication of MRSA
colonization • Selective decontamination
of the GI tract • Routine prophylaxis of very
LBW infants • Routine prophylaxis in HD
or CAPD
119
Pharmacokinetics • Insignificant
absorption following oral administration (used only for C.Diff)
• Penetrates well into most body tissues
• Crosses BBB ONLY when meninges inflamed
• Half-life = 6-10 hrs
• Levels – peak: 20-40 mg/L – trough: 10-15 mg/L
• Relatively large Vd – 0.6-0.9 L/kg
• Eliminated via glomerular filtration
120
Adverse Effects
• Red Neck (Man) Syndrome • Thrombophlebitis • Ototoxicity • Nephrotoxicity • Other
– hyperbilirubinemia – neutropenia, anemia, thrombocytopenia
121
Aminoglycosides
122

Aminoglycoside Antimicrobials
• Streptomyces group – Streptomycin – Neomycin (Mycifrandin ®) – Kanamycin (Kantrex®) – Tobramycin (Nebcin®) – Amikacin (Amikin®)
• Micromonospora group – Gentamicin (Garamycin®) – Netilmicin (Netromycin®)
123
Mechanism of Action
• Involves inhibition of bacterial protein synthesis – bind irreversibly to 30S ribosomal subunit
• Disruption of protein synthesis – rapid cell death-loss of essential cellular
contents • Irreversible binding of AG
– prolonged postantibiotic effect
124

Mechanisms of Resistance
• Adaptive resistance – If 1st exposure is sub-lethal,
• organism may decrease its AG uptake – Exposure of the organism to a high
initial AG concentration is important • Concentration-Dependent Killing
125

Mechanisms of Resistance
• Acquired resistance – Decreased permeability – Reduced binding affinity for ribosomal
target site – Enzymatic inactivation
• Amikacin -least susceptible – contains 3 sites that must be enzymatically
modified vs. 2 sites on other AG
126

Synergy
• AG require active transport to penetrate into the cell wall of the bacteria
• Enterococci and streptococci are innately resistant to low levels of AG
• Cell wall synthesis inhibitors – beta-lactams and vancomycin increase AG
penetration into the bacteria – SYNERGY
127

Spectrum of Activity
• Gram (-) bacilli (major clinical role) • Activity against Gram (+) cocci is highly
variable • Gram (-) cocci (Neisseria and Moraxella)
usually susceptible • No anaerobic coverage • Synergy: Enterococcus, Streptococci
128

Clinical Uses • Pseudomonas aeruginosa infections
– Used with extended-spectrum penicillins (piperacillin) for treatment of severe infections
• With ampicillin – treatment of severe enterococcal infections
• With clindamycin or metronidazole – treatment of severe intra-abdominal infections
129
Clinical Uses
• Most common clinical uses – Additive therapy in combination with carbapenems or β-lactams for enhanced gram-negative activity
– UTIs, pyelonephritis, prostatitis – Endocarditis – synergy – Nosocomial pneumonia – CF – Any Pseudomonas aeruginosa infection in
combination with other antipseudomonals – In combination against selected resistant pathogens – Be leary of combining with vancomycin: very
nephrotoxic 130

Pharmacokinetics • Oral bioavailability is
negligible • Administered parenterally • PO neomycin rarely used any
more • Half-life 2 hrs in normal
individuals • Low protein binding • Vd ~ = to extracellular space • Penetrate BBB poorly and do
not attain high levels in the lungs
• 95% eliminated renally
• Obtain peaks and troughs after reaching SS (usually after 5th dose)
• Extended Interval dosing – Concentration –dependent
killing – Post antibiotic effect – Potentiates tissue penetration – Reduces ADRs – Give higher dose and less
frequent intervals (q24,36, 48hr)
• Use a graph to calculate frequency
• Can’t be used in everyone
131

Adverse Effects • Nephrotoxicity
– AG bind to brush border cells of renal tubules (saturable process).
• accumulation -release of toxic hydrolases, killing the cells, which slough off into the lumen resulting in decreased GFR.
– Always reversible – 5-10% frequency – Use caution when giving with other nephrotoxins (e.g.
amphotericin B, cyclosporine, vancomycin)
132

Adverse Effects
• Ototoxicity – Accumulation of AG in inner ear tissues
• destruction of sensory hair cells in the cochlea and vestibular labyrinth
– Manifested as auditory toxicity, vestibular toxicity, or both
– May be preceded by tinnitus or sensation of fullness
– Reversible if caught early but rare – Vestibular toxicity is usually irreversible
133

The Macrolides
134

Macrolide/Azolid Agents
• Erythromycin (E-Mycin®, Ery-Tab®,Erythrocin®) – Base – Estolate – Ethylsuccinate – Stearate – Lactobionate
• Clarithromycin (Biaxin®, Biaxin -XL ®,)
• Azithromycin (Zithromax®)
• Dirithromycin (Dynabac®)
135
Mechanism of Action
• Reversibly binds to the 50s subunit of bacterial ribosomes – Results in inhibition of bacterial protein synthesis.
• Macrolides are generally considered bacteriostatic – may be bacteriocidal when present in high
concentrations – when used against highly susceptible organisms
136
Mechanisms of Resistance • Decreased penetration
– Gram (-) bacteria • Altered target site (most common) • Inactivation by bacterial esterases • Active efflux from the bacterial cell
137
Macrolides do not cover:
• MRSE or MRSA • Enterococci • Enterobacteriaceae • Pseudomonaceae • Neisseria meningitidis (does not penetrate
BBB) • Bacteroides fragilis
138

Macrolide coverage includes...
ERY Clar AZR MSSA/MSSE ± + + Streptococcus + + + N. Gonorrhoeae + + + M.catarrhalis + ++ ++ H. Influenzae ± + + H. Ducreyi + + + Legionella + + +
139
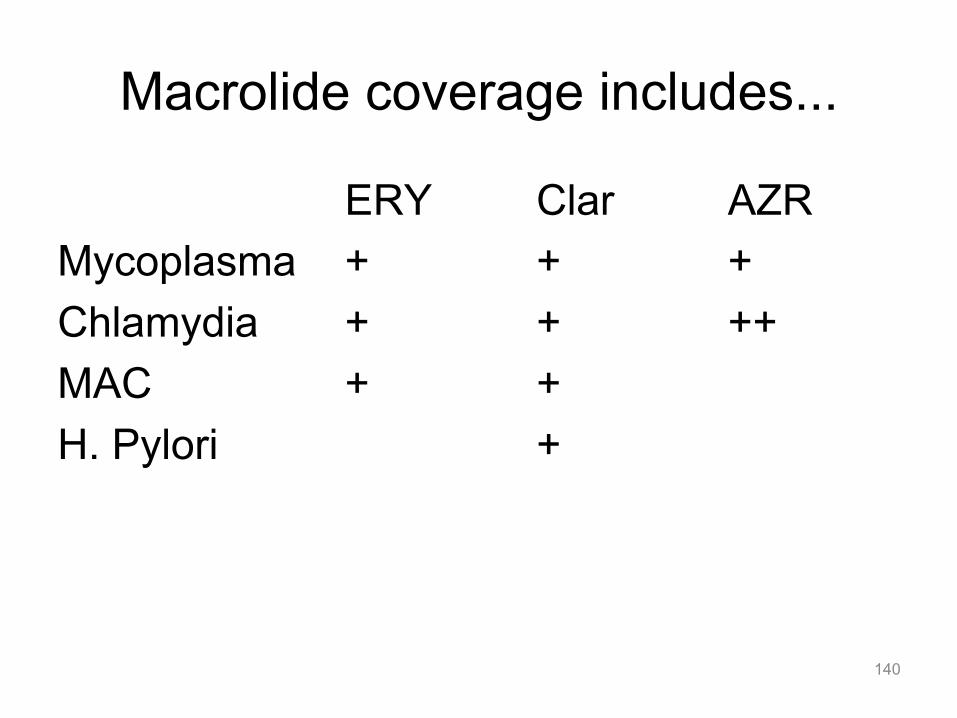
Macrolide coverage includes...
ERY Clar AZR Mycoplasma + + + Chlamydia + + ++ MAC + + H. Pylori +
140

Pharmacokinetics • Bioavailability
– Oral erythromycin varies with formulation • Bioavailability of base reduced by food • Stearate preparations -acid unstable, estolate are
more acid stable • Ethylsuccinate preparations -absorbed unchanged • Enteric-coated may have greatest oral bioavailability • Lactobionate are parenteral preparations
– Clarithromycin ~ 55%. • Administer with food- increases extent of absorption
– Azithromycin ~37%. • Administered 1 hr b/f or 2 hr after meals
141
Pharmacokinetics cont…. • Distribution- extensive except BBB • Erythromycin metabolized-
– several inactive metabolites in liver – ~2-5% eliminated unchanged in urine – Clarithromycin ~30-40% excreted unchanged in urine ~10-50% as a
metabolite, rest eliminated via the biliary route
– Azithromycin is not hepatically metabolized • Half-life of Ery ~1.5-2h, Clarithromycin 4-5hr,
Azithromycin ~ 50-70h • Due to low bioavailability recommended to
load azithromycin – i.e. Zpak dosing: 500mg day 1: 250mg days 2-5 142

Macrolides: Toxicity
Common Gastrointestinal (erythromycin): Nausea/vomiting/diarrhea (30%) -Erythromycin motilin receptor agonist in GI tract
Uncommon Gastrointestinal (azithro, clarithro): Nausea/vomiting/diarrhea (1-5%) Hepatic: transaminase elevation (1-5%) -usually transient, resolves upon d/c
Rare Sensory: ototoxicity (<1%) -Hearing loss, usually reversible Hepatic: severe hepatotoxicity, cholestatic jaundice (<1%) Cardiac: QT prolongation, arrhythmias (<1%) -Indirect: drug interaction effects on proarrythmics -Direct: HERG channel blockade, torsades des pointes
143

Macrolides: Drug Interactions
Second Drug Action Rifampin, rifabutin ↓ Macrolide levels à failure
↑ Rifabutin levels à uveitis Phenytoin ↑ 2nd Drug levels à sedation
Amiodarone, quinidine, sotalol ↑ 2nd Drug levels à arrhythmia
Tacrolimus Cyclosporine
↑ 2nd Drug levels à nephrotoxicity
Benzodiazepines Statins Ca-channel blockers Warfarin
↑ 2nd Drug levels à various dose-related adverse effects
Interaction Profile 1A2 2C9 2C19 3A4 Erythro > clarithro >>> azithromycin
Inhibitor + Inhibitor + Inhibitor + Inhibitor ++ Substrate +
144

Telithromycin (Ketek®)
145

• A ketolide, oral only • Related to macrolides • MOA-blocks protein
synthesis by binding at 23RNA of 50S ribosomal unit
• Resistance-production K-peptide and riboprotein (target site)mutations
• For gram + infections • Has activity against
macrolide resistant pneumococci
• Oral only • SE-GI, headache,
hypersensitivity • QT interval
prolongation • Contraindicated in
patients with myasthenia gravis
146

Metronidazole (Flagyl®)
147

Mechanism of Action • Nitroimidazole containing a nitro group which is
reduced within the cells of susceptible organisms – yielding highly toxic intermediates which damage
microbial DNA of organism • Most effective in active obligate anaerobes • Bactericidal
148

Mechanisms of Resistance
• Aerobes- innately resistant due to its MOA • reduction reaction needed to produce
toxic metabolites that damage microbial DNA competes with oxygen for available electrons
• Rare acquired resistance
149
Spectrum of Activity
• All obligate anaerobes – Bacteroides fragilis – Clostridium difficile (AOC for CDAD)
• Gardnerella vaginalis • Trichomonas vaginalis • Invasive amebiasis • Giardia intestinalis
150

Pharmacokinetics • Oral absorption 100% (bioavailability) • Similar peak concentrations are attained after
oral and IV doses • Crosses CNS • Half life is 8 hrs. Now recommended to use q12h
dosing instead of q 8 or q 6 h. • Hepatically metabolized. 60-80% is eliminated in
urine as parent and metabolites • May need to decrease dose by 50% in severe
hepatic impairment
151

Adverse Effects • Gastrointestinal
– most common (n/v/d) • Disulfiram like reaction
(flushing, HA, sweating, abdominal pain, N/V)
• Do not take with alcohol – Altered taste sensation
(metallic taste) • Neurologic
– HA, dizziness, or confusion. High doses cause seizures, ataxia, paresthesias
– Peripheral neuropathy (<1%)
• Other – Discoloration of urine to a
dark reddish brown. – Do not use in 1st trimester or
during breast feeding • Drug Interactions -Warfarin: increased INR,
risk of bleeding -Alcohol: potential for
disulfiram-like reaction
152

The Fluoroquinolones
153

Fluoroquinolones
• First-Generation – Nalidixic Acid - obsolete
• Second-Generation – Add pseudomonas coverage – Urine - Norfloxacin – Systemic- Ciprofloxacin, Ofloxacin
154

Fluoroquinolones
• Third-Generation – Add Strep. pneumoniae – Levofloxacin – Sparfloxacin
• Fourth Generation – Add anaerobes – Moxifloxacin (Avelox)
155

Mechanism of Action
• Inhibit DNA gyrase, – enzyme that catalyzes the formation of
supercoiled bacterial DNA – stabilize enzyme in tertiary complex after the
insertion of a single strand break – cell is unable to repair break - death results
• Bactericidal • Active against-dividing and stationary
bacterial cells
156

Mechanisms of Resistance
• Reduced binding affinity for DNA gyrase
• Decreased cell wall permeability due to changes in porion channels
157
Spectrum of activity
• Spectrum: – G(-): Enterobacteriaceae, enteric pathogens – G(+): MSSA, some Strep – Atypicals: Legionella, Mycoplasma, Chlamydia
• First-Generation – UTIs (seldom used)
• Anti-pseudomonal: ciprofloxacin, levofloxacin • Respiratory organisms: moxifloxacin, levofloxacin
– H. influenzae, Moraxella, Neisseria and atypicals like Chlamydia trachomatis, mycobacterium tuberculosis
• Anaerobes: moxifloxacin • B. fragilis
158

Pharmacokinetics • Oral Bioavailability of
80-100% • Easily convert from IV
to PO dosage form • Wide extravascular
distribution and tissue penetration – Negligible protein
binding – Small molecular size – modest CSF penetration
• Eliminated renally • Dosage adjustment in
patients with mild-to-moderate renal impairment (CrCl < 50 ml/min) (levofloxacin, ciprofloxacin) not necessary with moxifloxacin
159
Adverse Effects • QT prolongation • Gastrointestinal • Neurologic
– dizziness, headache, restlessness, tremors
– dose related and more common in elderly
– GABA inhibition • C.diff • Hypersensitivity
– mild-to-moderate rash
• Hyper/hypoglycemia • Musculoskeletal
– cartilage erosion and arthropathy in weight bearing joints of animals
– contraindicated in pregnancy and nursing mothers
– use in children < 18 should be limited
• Drug Interactions • -Oral divalent/trivalent
cations (Ca, Mg, Fe, Al): reduced concentration of orally administered fluoroquinolones via chelation
160

The Tetracyclines
161

Tetracycline Classes
• Short-acting – Tetracycline (Achromycin®, Sumycin®) – Oxytetracycline (Terramycin®)
• Intermediate-acting – Demeclocycline (Declomycin®)
• Long-acting – Doxycycline (Vibramycin®) – Minocycline (Minocin®)
162

Mechanism of Action
• Bind to the 30S subunit of the 70S bacterial ribosome – prevents production of essential bacterial proteins
• Bacteriostatic-reversible binding • Concurrent administration with B-lactams - mask
bactericidal actions of B-lactams
163
Mechanisms of Resistance
• Prevention of accumulation within the cell – decreased influx – increased ability of cell to actively
remove antibiotic (increased efflux)
164

Spectrum of Activity • Vibrio species • UTIs associated with
E. coli or P. mirabilis • Acute exacerbations
of chronic bronchitis • H. pylori • Outpatient therapy for
CAP
• Propionibacterium acnes
• Borrelia burgdorferi (Lyme disease)
• Chlamydia • Mycoplasma
pneumoniae • Rickettsia (Rocky
Mountain Spotted Fever)
165

Pharmacokinetics • Irregular absorption
– Take on empty stomach except for doxycycline and minocycline
• Chelate polyvalent metal ions – Ca, Mg, Iron, Al – Separate dosing from
MVI, Ca, Iron • Widely distributed
– placenta, breast milk
• Hepatic metabolism; eliminated in urine/feces
• Should not admin to renally impaired pts due to antianabolic effect – inhibits protein synthesis
which results in metabolism of AA and azotemia
– occurs with all tetracyclines except doxycycline
166

Adverse Effects • Gastrointestinal
– anorexia, nausea, vomiting
– dose-related • Musculoskeletal
– discoloration of teeth, retardation of skeletal growth
– contraindicated in pregnant women and kids up to age 8
• Phototoxicity • Hepatotoxicity
– dose-related with IV (>2 g/day)
– fat deposition in liver • Neurologic (Minocin)
– dizziness, loss of balance, tinnitus
• Oral/vaginal Candida superinfections
167

Trimethoprim-Sulfamethoxazole (TMP/
SMX,Bactrim®)
168

Mechanism of Action
• SMX- inhibits conversion of Para-aminobenzoic acid (PABA) to dihydropteroic acid
• TMP- inhibits bacterial dihydrofolate reductase • Overall effect: inhibition of biosynthesis of
tetrahydrofolic acid, a precursor in the synthesis of certain nucleosides and amino acids
• Classified as an antifolate
169

Mechanisms of Resistance
• Decreased cell permeability • Overproduction of dihydrofolate
reductase or PABA • Reduced binding affinity of
enzymes
170

Spectrum of Activity
• Staph and Strep • Neisseria • H. influenzae • Moraxella catarrhalis • Enterobacteriaceae • Pseudomonas
cepacia • Stenotrophomonas
maltophilia
• Brucella • Chlamydia • Pneumocystis carinii • Enterococcus,
Salmonella, Shigella, Pseudomonas aeruginosa, and obligate anaerobes are RESISTANT
171

Antifolates: ADME
Absorption • PO well-absorbed (~90%); also available as IV
Distribution • Wide distribution, good CNS penetration
Metabolism • Some metabolism Adjust in hepatic dz? • No Excretion • Mostly eliminated in urine Adjust in renal dz? • Yes
Drug Interactions -Warfarin: increased INR, risk for bleeding

Adverse Effects
• Cutaneous – mild skin rashes – SJS and TEN are rare
• Hematologic – thrombocytopenia – neutropenia (AIDS pts) – hemolytic anemia – megaloblastic anemia
• Neurologic – headache, depression,
hallucinations, tremor • Hepatotoxicity • Reversible
hyperkalemia • Benign, reversible
elevation of SCr
173
Miscellaneous
• Linezolid (Zyvox) • Daptomycin (Cubicin) • Quinupristin/dalfopristin (Synercid®) • Alternatives to vancomycin for resistant
gram positive infections • Very expensive and need to be reserved
for resistant infections
174

Linezolid (Zyvox) Mechanism of Action
• Oxazolidinone • Inhibits bacterial protein synthesis by
binding to site on 23S ribosomal RNA of the 50 S subunit and prevents formation of functional 70S initiation complex (essential component for translation process)
• Bacteriostatic against enterococci and staphylococci
• Bacteriocidal for streptococci
175

Mechanism of Resistance
• Mutations in 23S RNA
176

Spectrum of Activity
• Enterococcus faecium (vancomycin resistant strains)
• Staphylococcus aureus (including methicillin-resistant strains)
• Strep agalactiae, pneumoniae (including multi-drug resistant isolates), pyogenes
177

Oxazolidinones: ADME
Absorption • PO form has 100% absorption (bioavailability)
Distribution • Wide distribution, including CNS but not to be used in bacteremia (concentrations are maintained high enough)
Metabolism • Nonenzymatic oxidation; mild-moderate inhibitor of monoamine oxidase
Adjust in hepatic dz? • No Excretion • Metabolites excreted in urine Adjust in renal dz? • No
Drug Interactions -Serotenergic drugs (SSRIs, TCAs, triptans): risk of serotonin syndrome with co-administration (often prevents use)

Adverse Effects
• Myelosuppression- monitor CBC weekly • Diarrhea, Headache, Nausea
179

Oxazolidinones: Toxicity
Uncommon Hematologic: Thrombocytopenia, neutropenia, anemia (1-5%) -Mild-moderate myelosuppression -Seen w/tx courses >7-10 days -Reversible on d/c Gastrointestinal: Nausea/vomiting/diarrhea (1-5%)
Rare Metabolic: Mitochondrial toxicities (<1%) -Peripheral neuropathy, optic neuritis -Lactic acidosis -Associated with prolonged (>4 weeks) duration of treatment -May be irreversible
180

A point to consider
• Linezolid is VERY expensive as an OP Rx (~$55/tablet)
• Given BID for 7-10 days • Clinical judgment MUST be used before
prescribing this in an OP setting • There are assistance programs now
available: work closely with case management to utilize these programs
181

Daptomycin (Cubicin®) • Classified as a lipopeptide • Indications • Complicated skin and skin structure
infections – caused by susceptible isolates of the following Gram-
positive microorganisms: Staphylococcus aureus (including methicillin-resistant isolates), Streptococcus pyogenes, Streptococcus agalactiae, Streptococcus dysgalactiae subsp. equisimilis, and Enterococcus faecalis (vancomycin-susceptible isolates only).
– Staphylococcus aureus bloodstream infections (bacteremia), including those with right-sided infective endocarditis, caused by methicillin-susceptible and methicillin-resistant isolates.
182

Daptomycin (Cubicin®) • Not indicated for the treatment of pneumonia • Patients need to monitor for development of muscle
pain/ weakness particularly of the distal extremities. • Monitor CPK levels weekly- any unexplained elevations
should be monitored more frequently. • Discontinue in patients with unexplained signs and
symptoms of myopathy in conjunction with CPK elevation >1000 U/L, or in patients without reported symptoms who have marked elevations in CPK (≥10X ULN).
• Most adverse events -mild to moderate in intensity. The most common were anemia, constipation, diarrhea, nausea, vomiting, injection site reactions, and headache.
183

Lipopeptides: ADME Absorption • IV only
Distribution • High protein binding; unknown/questionable CNS penetration; inactivated by pulmonary surfactant (not useful for pneumonia)
Metabolism • Minimal hepatic metabolism Adjust in hepatic dz? • No Excretion • >60% eliminated in urine Adjust in renal dz? • Yes
Lipopeptides: Resistance: Uncommon, mechanisms poorly defined

Lipopeptides: Toxicity
Uncommon Musculoskeletal: Myopathy (1-5%) -Muscle pain/weakness in skeletal muscle -With/without elevation in creatine phosphokinase (CPK) -Reversible on drug discontinuation -Monitor symptoms of myalgias; consider monitoring CPK
Rare Musculoskeletal: Rhabdomyolysis (<1%) -Muscle breakdown with renal damage -Associated with elevations in CPK -D/c dapto if CPK>10x ULN w/ or w/o sxs
185
Quinupristin/dalfopristin (Synercid®)
• Streptogramin • Serious or life-threatening infections associated
with vancomycin-resistant Enterococcus faecium (VREF) bacteremia.
• Also approved for complicated skin and skin structure infections caused by Staphylococcus aureus (methicillin susceptible) or Streptococcus pyogenes
• Standardized dosing regardless of renal impairment: 7.5 mg/kg IV q8h for vancomycin-resistant E faecium and 7.5 mg/kg IV q12h for complicated skin and skin structure infections
186
Quinupristin/dalfopristin (Synercid®) • Pharmacokinetic data in patients with hepatic
cirrhosis (Child-Pugh A or B) - dosage reduction may be necessary, but exact recommendations cannot be made at this time
• common adverse drug reactions - inflammation at the infusion site and pain at the infusion site; arthralgia and myalgia and nausea
• P450 3A4 substrates (e.g., cyclosporin A, midazolam, nifedipine, and terfenadine) should be used with caution and monitored when coadministered Those drugs used concomitantly that may prolong the QTc interval should be avoided.
187

Tigecycline (Tygacil®) • Newer Class – Glycylcycline (structurally similar
to tetracylines); IV only • Inhibits protein translation in bacteria by binding
to the 30S ribosomal subunit • Very broad spectrum, aerobes, anaerobes, gram
negative, and gram positive including MRSA, MRSE, and VRE – For skin/skin structure infections and intra-abdominal
infections • May cause permanent tooth discoloration in
pediatrics-avoid in pregnancy and those under 8 years
188

Tigecycline (Tygacil®) • Dosage reductions in patients with Childs Pugh C • Monitor PT/INR if used with warfarin • May decrease effectiveness of oral contraceptives • March 2011 FDA caution on increased mortality in
pneumonia patients • Adverse effects similar to tetracylines:
– photosensitivity, pseudotumor cerebri, pancreatitis, and anti-anabolic action (which has led to increased BUN, azotemia, acidosis, and hypophosphatemia
189

Clostridium difficile Risk by Antimicrobial Therapy
Characteristic Adjusted hazard ratio (95% Confidence Interval)
Penicillins 1.9 (0.9 – 4.0) B-lactamase combos 2.3 (1.5 – 3.5) 1st – 2nd Gen Cephs 2.4 (1.4-4.1) 3rd- 4th Gen Cephs 3.1 (1.9 – 5.2) Glycopeptides 2.6 (1.7 – 4.0) Clindamycin 1.9 (0.8 – 4.4) Macrolides 1.5 (0.7 – 3.1) Aminoglycosides 0.9 (0.3 – 3.0) TMP/SMX 1.9 (1.1 – 3.4) Fluoroquinolones 4.0 (2.7 – 5.9) Metronidazole 0.3 (0.1 – 0.9)
Stevens V, et al Clin Infect Dis 2011;53:42-48 190
191

Some Information Sources
• Sanford Guide-updated yearly • Infectious Disease Society of America
– http://www.idsociety.org/
192