antimicrobial self-stewardship: putting the cdcs antibiotic “timeouts” to work todd c. lee md...
TRANSCRIPT

Antimicrobial Self-Stewardship: Putting the CDCs antibiotic “timeouts” to work
Todd C. Lee MD MPH FRCPCInternal Medicine and Infectious Diseases
McGill University Health Centre (Royal Victoria Hospital / Montreal General Hospital)
Assistant Professor of Medicine, McGill University

What is Stewardship?
• Optimizing:
– Selection of spectrum– Dose– Route– Duration
• To MAXIMIZE clinical cure or prevention of infection
• While reducing:
1. Adverse drug events (including C. difficile)
2. Antimicrobial resistance within the hospital
3. Cost

• While reducing:
1. Adverse drug events (including C. difficile)
2. Antimicrobial resistance within the hospital
3. Cost



• While reducing:
1. Adverse drug events (including C. difficile)
2. Antimicrobial resistance within the hospital
3. Cost


• While reducing:
1. Adverse drug events (including C. difficile)
2. Antimicrobial resistance within the hospital
3. Cost

Methods of Stewardship
• Guidelines/Education
• Formulary restriction– Often using special forms
• Antibiotic rotation– i.e. change the common antibiotics used for
certain infections periodically
• Prospective audit and feedback

Guidelines
• Attempt to synthesize evidence-based recommendations based on local epidemiology
• Goal is to eliminate variability in practice for the most common infections
• Recommendations based on epidemiology and principles of stewardship

Local guidelines
• Consensus amongst ID faculty
• Based on professional society guidelines
• Adapted to base on local epidemiology/resistance patterns
• Adjusted for new publications within the field
• Revised annually since 2011
Community Acquired Pneumonia
• What are the common pathogens?
• Which antibiotics predictably cover them in your community?
• Which antibiotics do we favor locally?
• Does the patient have an epidemiologic risk for an infection not usually covered?

Community Acquired Pneumonia
• Notes:
• PO quinolones or azithromycin as soon as tolerates oral
• In the absence of bacteremic Staphylococcus aureus, empyema, abscess, necrotizing lung infection or Legionella: CAP may safely be treated with FIVE days total therapy – particularly with fluoroquinolones for which RCT data is available and robust– Clin Infect Dis. (2011) 52 (10): 1232-1240

COPD
• Who should receive antibiotics (if you accept that they are associated with benefit)?
• What are the major pathogens?
• What is our local resistance?
• What is known about the patient’s own microbiology?

COPD Exacerbations = 2 of 3 of sputum, purulence, dyspnea; not pneumonia
• No risk factors for resistance:
• One of: FEV1<50; 4 exacerbations/yr., home O2, steroids recently, abx in past 3 months

Cellulitis
• Uncomplicated:
– no venous catheter around site – no water borne injury or bite wound– non-neutropenic – not associated with purulence, gangrene, fasciitis or an infected
diabetic foot ulcer
**Up to 75% likely group A streptococcus and up to 95% will respond to narrow spectrum beta-lactams**
Jeng et al., Medicine July 2010 - Volume 89 - Issue 4 - pp 217-226

Empiric MRSA Coverage
• Unless shock or purulence, empiric VANCOMYCIN not required unless clearly not responding to beta-lactam

Frequent use of potentially unnecessary diagnostic studies, broad-spectrum antibiotic therapy, and prolonged treatment courses in these patients suggest targets for antimicrobial stewardship programs.

The diabetic foot• Mild:
• Moderate:

The diabetic foot
• LIMB THREATENING – i.e. vascular surgery probably should be the one admitting

C. Difficile – 1st episode or 1st relapse
• NB: 125mg VANCOMYCIN dose for moderate. Never been shown more is better – certainly costs more (especially when they go home!)
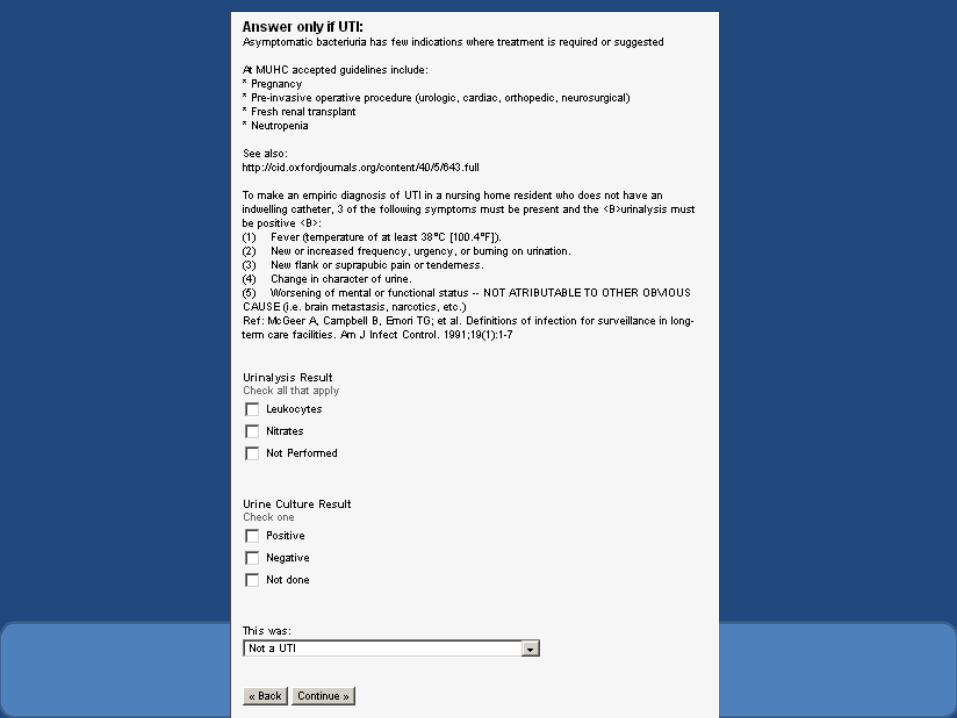
UTI
The elephant is in the room!

UTI
• In general requires:
– Positive urinalysis (unless neutropenic)
+– Symptoms attributable to lower or upper urinary
tract

Asymptomatic bacteriuria
• Very common
– especially in female patients from nursing homes, incontinent patients
• Free guidelines available online from the IDSA
– http://www.idsociety.org/uploadedFiles/IDSA/Guidelines-Patient_Care/PDF_Library/Asymptomatic%20Bacteriuria.pdf

Asymptomatic bacteriuria
• Treatment in adults should be limited to:
– Pregnant women
– Upcoming invasive urologic procedure • TURP• Procedure where there will be mucosal bleeding• Doing a renal transplant

Asymptomatic bacteriuria
• Randomized trials have shown no harm in not treating
– See also: Gross PA, Patel B Reducing antibiotic overuse: a call for a national performance measure for not treating asymptomatic bacteriuria. Clin Infect Dis 2007;45:1335-1337.

Asymptomatic bacteriuria
• Other randomized trials have shown treating causes more resistance and paradoxically more UTIs
– Clin Infect Dis. (2012) 55 (6): 771-777.

Asymptomatic bacteriuria
• Many will use in kidney transplant 1st month
• Beyond 1 month some evidence of increased rate of symptomatic UTIs requiring hospitalization


NOTE:
Excluded 1st MONTH
Cohort study – but similar effects seen in three other cohorts

Scope of the problem
• We performed 38048 urine cultures in 2012!
• Each urine culture costs $7.40
• Total Cost (lab only) = $281 555– Downstream costs exponentially more– Antibiotics (potentially IV)• C. difficile, resistance, $$$
– Length of Stay


CULTURES WITHOUT INDICATION VERY COMMON
INPATIENT CLINICAL YIELD EXTREMELY LOW (<2%)
UNNECESSARY ANTIBIOTICS IN UP TO 50%
RAISES THE QUESTION: DO THESE CULTURES DO MORE HARM THAN GOOD?



Take home message
• Avoid treating asymptomatic bacteriuria
• Avoid culturing urine looking for ASB without good reason

UTI – Hospitalized patients
• \
• Gentamicin with caution in:– Renal insufficiency or concomitant administration of other nephrotoxins– Cirrhosis (hepatorenal syndrome)– Existing sensorineural hearing loss or vestibular dysfunction
• Level independent side effects
– Existing sensory neuropathy for which loss of vestibular function would be severely disabling• Make sure levels are done after 48 hours of use and that you consult with your pharmacist to ensure
proper monitoring and targets• Culture data is going to be important to find alternative agent for longer use

Your mission…
• For each of your patients, at regular intervals
– Take a “time out” to reassess their antibiotics

Antibiotic Self-Stewardship
• Concept:
– Periodic twice weekly scheduled review of all antibiotics by the practicing team
– On demand involvement of ID

Advantages of self-stewardship!
• Maintain full control over antibiotic prescription without external influence
• Develop skills in antibiotic stewardship which are expected to have long term educational effects over a career

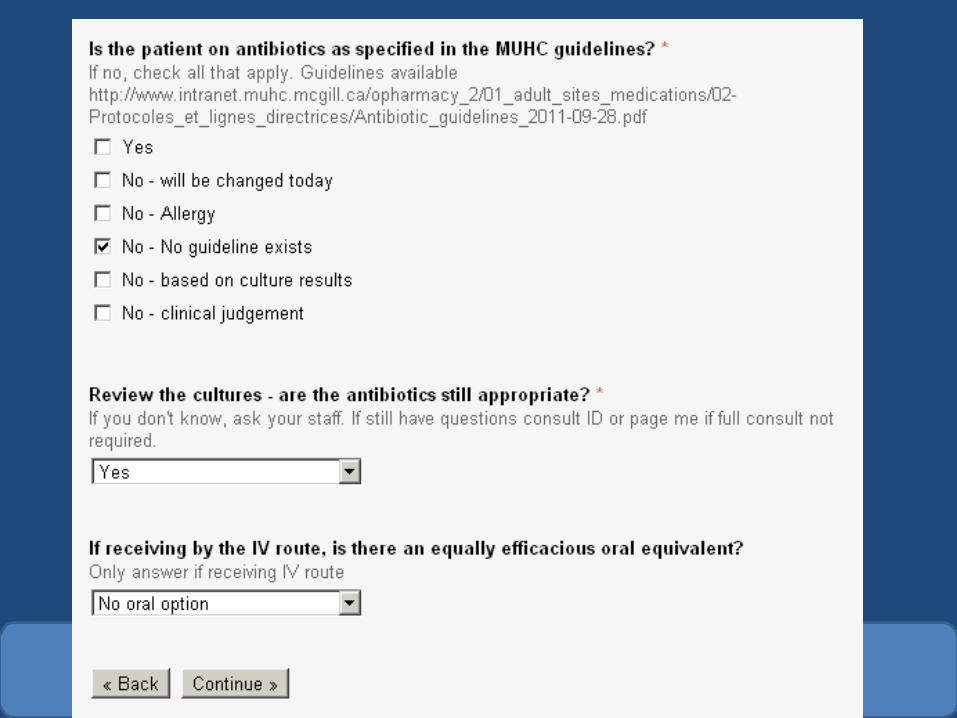
How do I perform self-stewardship?
• Then next several minutes dedicated to teaching our housestaff how to use the electronic audit tool properly.
• This tool is available for you to view in appendix 2


If the patient does not have a suspected or proven infection (i.e. you now know their hypotension was caused by a GI bleed and not sepsis) then it follows their empiric antibiotics should be stopped



Guidelines
• Compare the antibiotics the patient is receiving to those in the MUHC guidelines and the guidelines I presented
• If they aren’t on guideline approved antibiotics, why is that?– No guideline exists?– Culture data?– Allergy?– “Clinical judgment” to use alternative?
• In general it is best practice to follow your local guidelines

Microbiology
• Microbiology is essential to choosing the right antibiotics for the infection in question
• Timely review of all recent results leads to the most appropriate management

IV -> PO
• Many antibiotics are highly available PO (FQ, metronidazole, TMP/SMX)
• Many infections do not require parenteral antibiotics to achieve cure
• Change to PO, when appropriate, can reduce:– Need for IV access and associated complications– Length of stay– Cost
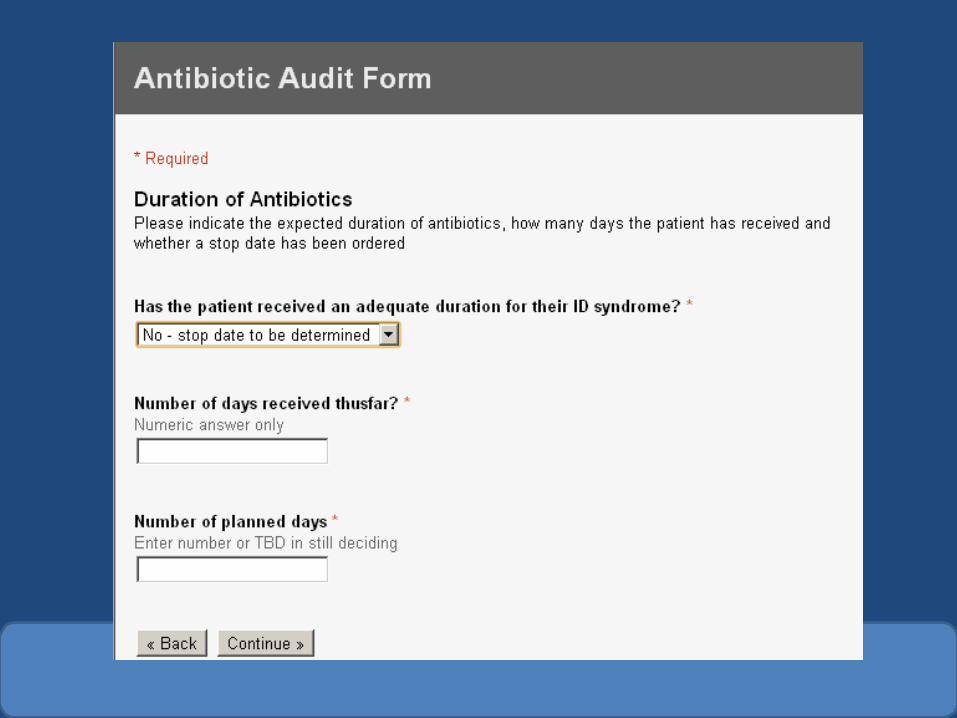

Duration
• Review the duration received and compare to what the guidelines, literature, clinical experience or consultants suggest
• Record the number of days received and compare against the number of planned days
• Stop today if it is time or set a stop date in the future to avoid inadvertent renewal or discontinuation


Targeted Drugs
• Review and optimize the use of targeted drugs• In particular:– Minimizing FQ use may help reduce C. difficile– “PIP-TAZO” is the one of the most used antibiotics at
our centre– Carbepenem use should be minimized as they are
expensive and our last-resort drugs (keep KPC out!)– Vancomycin is also probably overused and potentially
nephrotoxic requiring laboratory monitoring in patients without risk for MRSA or other organism




Audit Completed
• Thank you!• Expected workload not greatly in excess of
existing procedures– As little as 30 seconds per audit

Still don’t know what to do with the antibiotics?
• Ask your staff first
• Then if still in doubt:– Consult the Infectious Diseases Service– Page your self-stewardship advisor for advice (via
locating) if you aren’t sure if you need a full consult or have any questions about the antibiotic timeout process.