antimicrobial stewardship - acipc 2016 - 2016...
TRANSCRIPT

Antimicrobial Stewardship
for Nurses
Dr Noleen Bennett
1. acNAPS Project Officer, National Centre for Antimicrobial Stewardship
2. Infection Control Consultant, Victorian Nosocomial Infection Surveillance System
Coordinating Centre

Acknowledgments
• Ms Fiona Gotterson – Senior Project Officer, Australian Commission on Safety and Quality in
Health Care
• Assoc/Prof Caroline Marshall – Head, Infection Prevention and Surveillance Service, Melbourne Health
– Infectious Diseases Physician, Victorian Infectious Diseases Service
– Principal Research Fellow, University of Melbourne


From: Director of Nursing Sent: Wednesday, 29 Oct 2014 3:32 PM To: Noleen Bennett Subject: Question
Hi Noleen,
I have just noticed the proposed UTI clinical pathway detailed in the regional newsletter.
At a quick glance, the pathway looks way over the top for our purposes. It might be ok to guide medical staff but nurses do not need to know about antimicrobial use.
Can you please advise where exactly this is going and what ‘issues’ it is based on?
DON
Response email
From: Sent: NOT sent (20th Nov 2016) To: DON Subject: Response
Hi DON,
Nurses DO have a role in implementing successful AMS programs……..
From the 2016 ACIPC AMS for Nurses Workshop participants

Aims
• To highlight why it is important clinical nurses are
actively involved in AMS programs.
• To describe the activities that clinical nurses can
undertake as part of an AMS program.
• To outline the support systems required to successfully
enable clinical nurses to be involved in AMS programs.
• To describe some specific nurses’ roles.
• To outline some potential research studies.

Methodology
• PubMed search – Nurse/ Nurse Practitioner/ ICP
– Antibiotic/antimicrobial
– Resistance/Stewardship
• Nursing – Australian College of Nursing (ACN)
– UK Royal College of Nursing (RCN)
• Australasian College for Infection Prevention & Control (ACIPC)
• Australian Commission Quality & Safety in Healthcare (ACQSHC)
• Centers for Disease Control and Prevention

To highlight why it is
important clinical nurses
are actively involved in
AMS programs

Reasons
• LARGE part of the health care workforce.
• Are the most constant presence for patients/residents.
• Are patient/resident advocates.
• Are involved in all aspects of patient/resident care. • Education
• Medication management
• Work & communicate with most other key healthcare
worker groups.
• Work within multiple levels at the local clinical setting.
• Work at a local, national & international level.

AMR Strategy
Goal:
Minimise the development
and spread of AMR and
ensure the continued
availability of effective
antimicrobials
ACN Comment on Draft AMR Strategy
• Nurses are integral to much of the health care
delivered in Australia & thus have a key role to play in
safeguarding antibiotic’s effectiveness for future
generations.
• Nurses are involved in most aspects of the prevention
& control of AMR, including through patient education,
infection prevention & control, monitoring of antibiotic
use, prescribing & the development of organisational
policies.
• Engagement with nurses is an important factor in
addressing the emerging threat of AMR.
UK RCN Position Statement
• Nurses have a significant role to play in limiting the
threat posed by AMR through their leadership skills
supporting infection prevention and control,
antimicrobial stewardship & public health.
• It is essential that nurses are recognised as influential
members of the multidisciplinary team in combating
AMR & assuring stewardship.

To describe some
activities that clinical
nurses can undertake as
part of an AMS programs
Activities
• Patient Management Plans
• Infection Control and Prevention
• Medication (antimicrobial) management
• Collaboration
• Education
• Surveillance

Patient management plans
• Assess patients risk of both acquiring & transmitting
an infection.
• Complete nursing care plans or notes that accurately
reflect infection.
• Facilitate efficient discharge planning.
• Assess patients’ suitability for Hospital in the Home
programs.
Infection prevention & control
• Implement standard & traditional precautions.
• Correctly collect microbiological specimens if clinical
need is clearly indicated.
• Ensure timely transfer of microbiological specimens to
laboratories to maintain specimen quality.
• Review & recognise when treatment is not in line with
microbiological result.

Medication management
• Question suboptimal antimicrobial management & documentation.
• Recognise when patients are able to tolerate oral intake & could change from IV to oral
antimicrobials.
• Ensure timely administration of antimicrobials & follow up on missed doses.
• As applicable, administer antimicrobials at the right rate.
• Undertake timely therapeutic drug monitoring to ensure antimicrobials that perform
optimally within a specific therapeutic level are in line with recommended guidance.
• Monitor the patient to ensure antimicrobial has the intended effect.
• Recognise antimicrobial allergies & side effects.
• Support the use of standardised medication charts that document for each prescribed
antimicrobial its generic name, dose, time, route, reason for administration, review &
stop date.
• Accurately & clearly document the administration of any antimicrobials.
• Correctly dispose of unused antimicrobials

Medication management
FIVE rights
1. Right patient
2. Right drug
3. Right route
4. Right time
5. Right dose
NINE rights
Five rights plus
7. Right documentation
8. Right action
8. Right form
9. Right response
Ref: Elliott M & Liu Y. 2010
Collaboration
• Participate in (AMS) ward rounds.
• Participate in the development of guidelines & policies
that detail the use of medications.
• Suggest antimicrobial choices to medical staff in line
with guideline recommendations.
• Liaise between (offsite) doctors, microbiologists,
pharmacists, patients/residents and families.
Education
• Provide patient (consumer) education about
antimicrobials, especially prior to discharge.
• Educate (new) colleagues about the appropriate use of
antimicrobials, especially in relation to a specialist area.
• Encourage patients & other colleagues to question
suboptimal antimicrobial management & documentation.

Consumer education
• About actions consumers can take to help tackle AMR
& how to correctly use antimicrobials.
• Includes explaining: – Differences between bacteria and viruses & why viruses do not respond
to antibiotics
– What AMR is
– What antimicrobial allergies mean
– Why the antimicrobial is needed
– How & when antimicrobials should be taken
– How long antimicrobials should be taken for
– Not to share antimicrobials with others
– Not take antibiotics left over from a previous illness.

Surveillance
• Audit medical records and collect data.
• Analyse data and present in easy to understand
formats.
• Feedback analysed data to the team
• Instigate as necessary (and review) new interventions.
Surveillance
To register: naps.org.au

Surveillance: Example
• UK point incidence study
• Aim: To investigate delayed & omitted antimicrobials
Measurement No (%)
Participating organisations 45
Patient records audited 17,470
Patients prescribed antimicrobials (% total patient records)
5899 (33.7%)
Doses prescribed 21,390
Doses omitted (% doses prescribed) 1120 (5.2%)
Patients missing one or more doses (% prescribed antimicrobials)
781 (13.2%)
Ref: Wright J. 2013
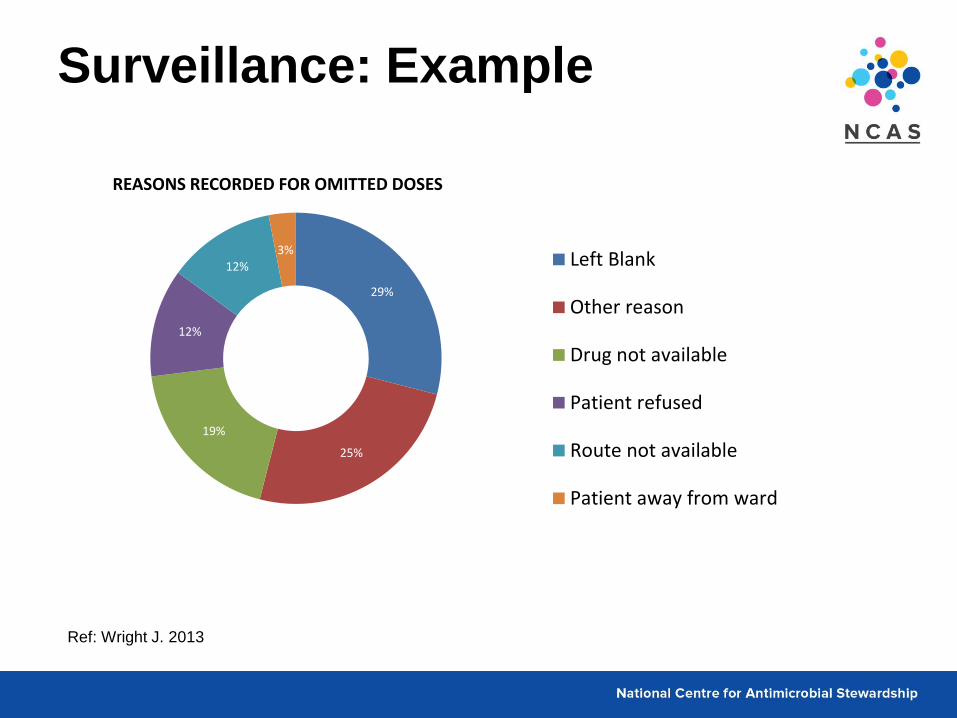
Surveillance: Example
Ref: Wright J. 2013
29%
25%
19%
12%
12% 3%
REASONS RECORDED FOR OMITTED DOSES
Left Blank
Other reason
Drug not available
Patient refused
Route not available
Patient away from ward

To outline the support
systems required to
enable nurses to be
successfully involved in
AMS programs

Leadership commitment
• Formal statements that the facility supports efforts to
improve antimicrobial use are developed.
• Participation in AMS programs is expected from key groups.
• Stewardship-related duties are detailed in job descriptions &
annual performance reviews
• Staff are given sufficient time to participate in AMS activities.
Ref: CDC 2014

Nurses knowledge
Refs: Cotta M.O, Robertson M.S, Tacey M, Marshall C, Thursky K.A, Liew D and Buising K.L. 2014.
McGregor W, Brailey A, Bayne G, Sneddon J and McEwen J. 2015
Australian private
hospital
Percentage
Heard of AMS Willingness to
participate in AMS
Anaesthetists 36 51
Pharmacists 80 100
Physicians 64 55
Surgeons 37 48
Nurses (n=105) 22 43
The Scottish Antimicrobial Prescribing Group identified 21.5% of nurses had heard of AMS.

Education
• Under & post graduate
• Content – Antimicrobial resistance
– Antimicrobial stewardship
– Infectious diseases
– Microbiology
• Specimen collection
– Pharmacology
– Principles of surveillance
National medication charts
• National Inpatient Medication Charts – Acute (public and private)
– Long stay (public and private
– GP e-version
• National Residential Medication chart

NRMC
To describe the ICP
(nurse) role

ACIPC Position Statement
• AMR is a serious & significant problem.
• Reducing AMR by prudent & rational antibiotic use is
the responsibility of all healthcare workers.
• ICPs & nursing staff should play a role in AMS
programs as part of their role in preventing &
containing HAIs & antimicrobial resistant organisms.
Infection Control Practitioner
• Dependent on facility size, type & location.
• Undertake a feasibility study
– Identify current perceptions in relation to AMS & nurses’
role.
– Assess how the nurses’ role can be strengthened.
– Identify other key groups who can support AMS.
• Work with other key groups
– To enable appropriate ‘support systems’ are in place.
– Influence governance frameworks
Infection Control Practitioner
• Organise educational strategies.
• Co-ordinate surveillance programs.
• Advise on IT systems to support surveillance,
education & medication management.
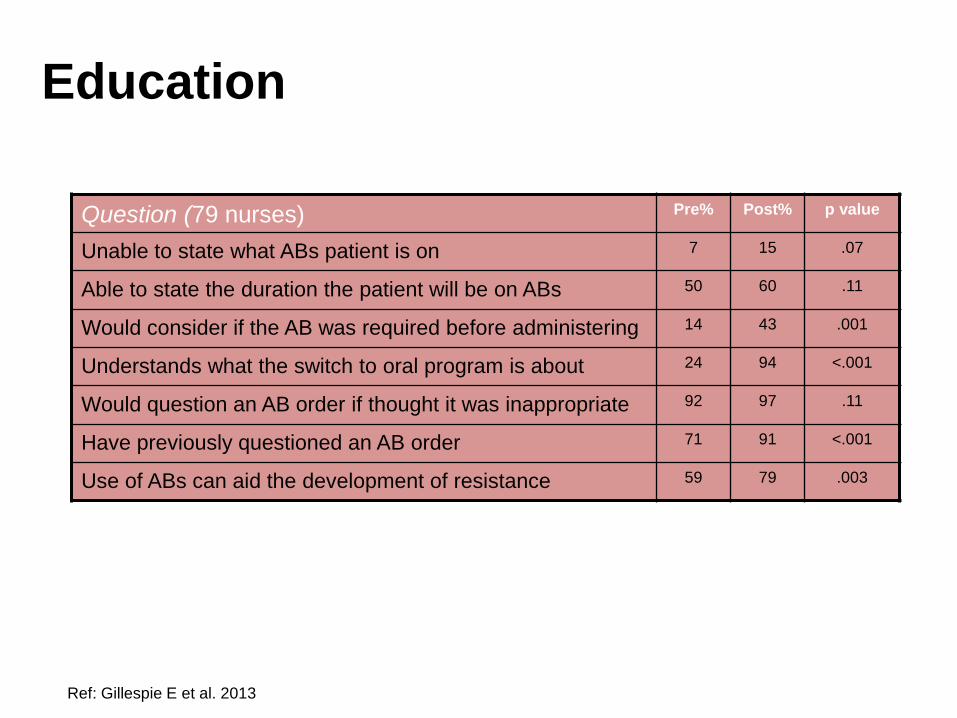
Education
Ref: Gillespie E et al. 2013
Question (79 nurses) Pre% Post% p value
Unable to state what ABs patient is on 7 15 .07
Able to state the duration the patient will be on ABs 50 60 .11
Would consider if the AB was required before administering 14 43 .001
Understands what the switch to oral program is about 24 94 <.001
Would question an AB order if thought it was inappropriate 92 97 .11
Have previously questioned an AB order 71 91 <.001
Use of ABs can aid the development of resistance 59 79 .003

ICP: Leadership
• Pilot study to assess ICP AMS leadership role
• Three stages (pre, intra & post intervention)
• ICP responsibilities included – Intermediary b/w GP & an off-site ID physician
– Education of GPs & nurses
– Surveillance
– Monitoring of pathology reports
• Result – Significant decrease in total days of antimicrobials prescribed
(p<0.0001)
Ref: Stuart RL. et al 2014
To outline some potential
research studies
Research
• Australian nurses knowledge of AMR & AMS.
• Experience of Australian clinical nurses/ ICPs/ nurse
practitioners in AMS.
• Successful nurse led models of AMS.
• Perceptions of other key groups regarding nurse’s role
in AMS.

Summary
Response email
From: Sent: NOT sent To: DON Subject: Response
Hi DON,
Nurses DO have a role in implementing successful AMS programs……..
• Why clinical nurses should be involved
• Activities that clinical nurses can undertake
• Support systems required
• ICP’s role
From the 2016 ACIPC AMS for Nurses Workshop participants

ACSQHC AMS Publication
The AMS team (page 9) Multidisciplinary teams are better suited to implement the kind of improvement and change required for effective AMS. There are a range of professions and individuals that have an interest in and responsibility for AMS, each with different perspectives and skills. Involving prescribers, pharmacists, administrators, infection control experts, information systems experts, microbiologists and ID physicians into a well-managed team effectively incorporates their views and expertise.
ACSQHC AMS Publication
Chapter on the Role of Nurses
2017

References
Atik A, Adherence to the Australian National Inpatient Medication Chart: The efficacy of a uniform
national drug chart on improving prescription error. Journal of Evaluation in Clinical Practice
2012
CDC. Core Elements of Hospital Antibiotic Stewardship Programs. Atlanta, GA: US Department
of Health and Human Services, CDC; 2014. Available at http://www.cdc.gov/getsmart/healthcare/
implementation/core-elements.html
Cotta M.O, Robertson M.S, Tacey M, Marshall C, Thursky K.A, Liew D and Buising K.L. 2014.
Attitudes towards antimicrobial stewardship; results from a large private hospital in Australia.
Healthcare Infection 19(3)
Edwards SR, Drumright LN, Kiernan M and Holmes A. 2011 Covering to fight resistance;
Consideration nurses role in antimicrobial stewardship. J Infect Prev Jan 12 (1) 6-10.
Elliott M and Liu Y. The nine rights of medication administration; an overview. 2010 British
Journal of Nursing Vol 19 No. 5
Gillespie E, Rodrigues A, Wright L, Williams N & Stuart R.L. 2013 Improving antibiotic
stewardship by involving nurses. AJIC. 41:365-7.
Royal College of Nursing Antimicrobial resistance. RCN position on the nursing contribution.
Stuart R.L, Orr E et al. 2014 A nurse led antimicrobial stewardship intervention in two residential
aged care facilities. Healthcare Infection
Ladenheim D, Rosembert D, Hallam C & Micallef C. 2013. Antimicrobial stewardship; the role of
the nurse. Nursing Standard 28 (6):46-49
Wright J. Audit of missed or delayed antimicrobial drugs. Nursing times Vol 109 no 42.
References: NP
Roumie CL, Halasa NB, Edwards Km, Zhu Y, Dittus RS, Griffin MR. Differences in antibiotic
prescribing among physicians, residents and non-physician clinicians Am j Med. 2005 118(6):
641-8
Undeland DK, Kowalski TJ, Berth WL,. Gundrum JD. Appropriately Prescribed Antibiotics for
Patients with Pharyngitis: A Physician-Based Approach vs a Nurse-Only Triage and Treatment
Algorithm, Mayo Clinical Proceedings, 2010; 85(11):1011-5
Nuttall SE. Evaluation of the antibiotic prescribing of nurse practitioners trained to prescribe in
primary care Primary Health Care Research and Development 2008; 9:199-204
Cashin A, Buckley T, Newm A, C Dunn S. Nurse practitioner provision of patient education
related to medicine Australian Journal of Advanced Nursing 27(2):12-8
Rowbotham S, Chisholm A, Moschogianis S, Cew-Graham C, Cordingly L, Wearden A, et al.
Challenges to nurse prescribers of a no-antibiotic prescribing strategy for managing self-limiting
respiratory tract infections. Journal of Advanced Nursing 2012;68(12):2622-32
Offredy M. The use of cognitive continuum theory and patient scenarios to explore nurse
prescribers’ pharmacological knowledge and decision-making. International journal of nursing
studies. 2008; 45(6):855-68