antimicrobial stewardship in post acute care - houston antimicrobial... · pharmerica hospital...
TRANSCRIPT

Antimicrobial Stewardship in Post Acute Care
Houston Antimicrobial Stewardship Symposium, March 5, 2015 Beth Weisz PharmD, MHA PharMerica HD/Kindred Healthcare

Topics
• Kindred/PharMerica Antimicrobial Stewardship Program
• Evolution of the Antimicrobial Stewardship Program • Successes in Antimicrobial Stewardship • Continued opportunities/ barriers to Antimicrobial
Stewardship • Transitions of Care and Antimicrobial Stewardship

Kindred Healthcare/PharMerica
• Kindred Healthcare is a multi-facility health-care corporation providing post-acute services.
• Service across the care continuum – Transitional Care Hospitals (LTACH) – Sub Acute Units – Nursing and Rehab – Home Care and Hospice
• PharMerica Hospital Division provides pharmacy management services to Kindred Hospital Division
• Partnership to provide Clinical, Operational and Regulatory support for Kindred both locally and nationally

Kindred Antimicrobial Stewardship
• In late 2009 a Hospital Division wide Antimicrobial Stewardship Program was initiated within Kindred Healthcare
• The initiative was developed within corporate Pharmacy Advisory Committee (PAC)
• Measures and Modalities used in the program have evolved since 2009.
• Multiple resources and tools have been created to assist hospitals with the initiative
• Early focus on education, with concurrent audit and feedback via an AS Team

Antimicrobial Stewardship
“Awareness for all Clinical Staff”
2009
Pharmacy Standards Committee Kindred/PharMerica
Kindred Antimicrobial Stewardship
• August 2009 education for Directors of Pharmacy – What is AS? – How to start an ASP
• 2010 began tracking AS metrics – Patients receiving antibiotics >10 days – Patients receiving >3 antibiotics – Cost of antimicrobials per patient day

Kindred Antimicrobial Stewardship • 2012 review of Antimicrobial Stewardship
Program outcomes • Survey to Directors of Pharmacy to assess
status of AS in the hospitals – Barriers Identified
• Time to gather data (manual processes) • Lack of lab data • Physician leadership • Lack of staff knowledge
– Successes Identified • Improved durations and documentation • Increased collaboration • Reduced costs • Improved susceptibilities • Improved lab results

Kindred Hospital Outcomes • Early Data
– Operational Outcome- Antibiotic Spend ppd – Quality Outcome- >3 Antibiotics, >10 days therapy – Data collection challenges- manual process/inconsistent
reporting
CALENDAR YEAR >3 antibiotics >10 days therapy
Total Antibiotic Spend ppd
Baseline data 3rd qtr 2009 3.2 5.7 $34.90
2010 3.38 4.97 $32.78
2011 4.04 6.20 $33.57
Kindred Antimicrobial Stewardship
• Pharmacy Advisory Review of AS data – Are we using the right metrics?
• >3 drugs • > 10days • Cost
– Are we using the right methods? • Education
– Who should we target for education? • All providers
– Have we been successful? • We can do more

Kindred Antimicrobial Stewardship
• Metrics – Quality – current metric doesn’t work, what should we be
reporting? • Appropriate therapy is sometimes subjective • Protocol adherence- Did not have established protocols • Resistance patterns- varied lab reporting, lack of antibiogram
data • Reduced HAI- data was not available at the time
– Operational outcomes cost- Improvement seen, but data collection was manual and inconsistent

Kindred Antimicrobial Stewardship Subcommittee
11
Antimicrobial Stewardship Subcommittee
• Subcommittee of our corporate Pharmacy Advisory Committee
• Formally established in late 2012 • Working group to develop training tools and
resources for Antimicrobial Stewardship as well as review utilization and trends
• Membership includes- Kindred DOPs, Kindred Infectious Disease Physicians, Kindred Laboratory and Infection Control Leadership, Kindred Pharmacy Leadership, other Clinical Content experts- CDC, clinical pharmacy, IT, MedAssets

13
Education- March 2014 Introducing the Revised Antimicrobial Stewardship Manual

Kindred Healthcare AS Manual
• Section 1- Overview of Antimicrobial Stewardship concepts • Focus on the 6 D’s • Marketing Antimicrobial Stewardship at your hospital • Enforcing sound infection control practices
14
Kindred Healthcare AS Manual • Section 2 Treatment Guides
– Designed to provide specific guidance and recommendations regarding common infections seen in the transitional care environment
• Section 3 Antimicrobials with Indications and Restrictions Defined – Carbapenems, Tigecycline, etc…
• Section 4 Important Pharmacokinetic Principles – Education around basics of Pharmacokinetics and renal dosing – Extended infusion guidance
• Section 5 Infection Control Principles – Review of infection principles related to antimicrobial stewardship – Evidence based bundles for management of Central lines, urinary
catheters, and mechanical ventilation
15

Kindred Healthcare AS Manual
• Section 6 Laboratory Recommendations – CDC based guidance on ordering of cultures
• Section 7 Antibiograms – How to read and use
• Section 8 Antimicrobial Stewardship Resources • Section 9 Case Studies and Post Test
– Physicians, pharmacists, nurses
16

17
Improving Antimicrobial Therapy, Providing Tools & Resources: The Antimicrobial Stewardship Manual Ask the I.D. Experts webcast Dialogues on Contemporary ID Issues in Transitional Care
Presenters: David Hines, M.D. FACP Diane Rhee. Pharm D.

18
Antimicrobial Stewardship Successes

Kindred Hospital Outcomes
CALENDAR YEAR TOP 3 Antibiotics spend ppd
Total Antibiotic Spend ppd
2012 18.42 30.53 2013 17.71 30.52
2014 16.64 26.53
Estimated Savings with AS in 2014 $4,972,401
•Operational Measure- Antibiotic Costs Per Patient Day(PPD) CALENDAR
YEAR >3 antibiotics >10 days
therapy Total Antibiotic Spend ppd
2010 3.38 4.97 $32.78
2011 4.04 6.20 $33.57

Kindred Hospital Outcomes 2010 – 2014 CLABSI Rate

Kindred Hospital Outcomes 2010 – 2014 Central Line Utilization
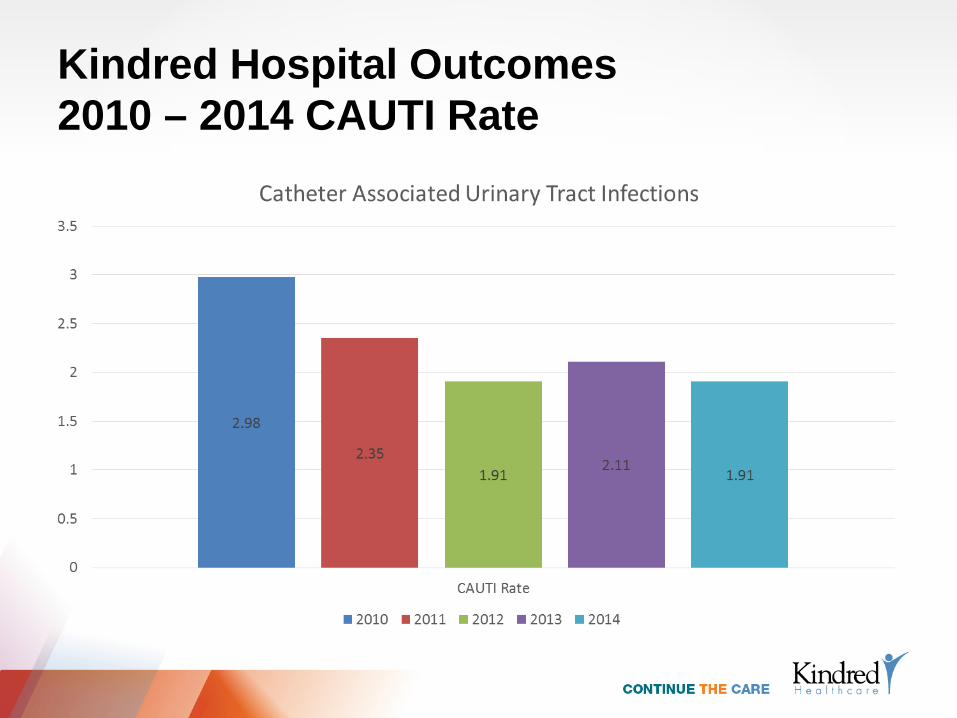
Kindred Hospital Outcomes 2010 – 2014 CAUTI Rate

Kindred Hospital Outcomes 2010 – 2014 Urinary Catheter Utilization

Kindred Success Hospital Case Study
•Hospital System in Southern California •History of high anti-infective costs •Clinical pharmacy coordinator hired in early summer •Boots on the ground •Primary focus on anti-infectives • Antimicrobial Stewardship program re-launch Mid August •Concurrent audit and feedback

Case Study: Anti-infective Cost PPD 2014 Impact of Clinical Pharmacist and Active AS Program

Anti-infective Cost PPD 2014 Impact of Clinical Pharmacist and Active AS Program
$52.70
$35.00
$47.33
$42.55
$38.76
$20.00
$30.00
$40.00
$50.00
$60.00
August September October November December
A reduction in AB cost from $52.70 to $38.76 represents an annualized reduction in cost of over $265,000
TARxGET Rx data, (ABC): Graphs do not reflect contract increases in 2014; savings is understated
27
Antimicrobial Stewardship Opportunities

Continued Opportunities • AS Implementation varies across our hospitals.
– Varied implementation of formal AS teams – We see success in hospitals with physician,
pharmacist, ICP rounds/meetings at least weekly – Need to continue to share Best Practice/Processes

Continued Opportunities • Pharmacist and Provider Education is needed
– Decision trees in development – AS manual updates on-going – Kinetics protocols established – Boots on the ground model expansion
• Physician Champion identification is key • Guideline and protocol adherence as a Quality
metric – P&T Dashboard 2015- micafungin – Scorecards- guideline adherence-daptomycin
• Restriction is used in some hospitals with success

Continued Opportunities
• Lab – Microbiology Interventions varies based on lab provider – Antibiogram availability underway – Appropriate ordering of cultures – Reflex orders for cultures and sensitivities
• Infection Control – Chlorhexidine bathing – Cohorting patients and staff assignments based on local
prevalence – Screening on admission (CRE) based on local rates.
• Clinical Decision Support • Auto-stop/ review process for all antimicrobials

Continued Opportunities/Transition of Care and Antimicrobial Stewardship • Applies to the entire Post Acute space- LTACH, SAU,
etc.. • Communication and Collaboration are Critical to
appropriate continuation of therapy. • We need to know
– Diagnosis – Plan for continuation of therapy – Anticipated duration – Cultures – Antibiotic therapy history

Continued Opportunities/Transition of Care and Antimicrobial Stewardship • Vancomycin treatment failure?
– LTACH are able to continue vancomycin therapy if that is the appropriate therapy
– Labs are evaluated routinely – Kinetics protocols are in place
• Osteomyelitis – What is the intended duration of therapy? – Acute versus chronic infection – Is surgical intervention a consideration?

Conclusion
• Kindred has identified local and national AS successes in both operational and quality metrics.
• There are some unique challenges to AS in the post acute space but many of the barriers to AS are the same across the healthcare continuum.
• Collaboration and effective communication are critical components to provision of quality care.
Questions?
Antimicrobial Stewardship in Post Acute Care
Houston Antimicrobial Stewardship Symposium, March 5, 2015 Beth Weisz PharmD, MHA PharMerica HD/Kindred Healthcare