antipsychotic drugs william h. anderson, ph.d. washoe county sheriff’s office reno, nv
TRANSCRIPT

Antipsychotic DrugsAntipsychotic Drugs
William H. Anderson, Ph.D.William H. Anderson, Ph.D.
Washoe County Sheriff’s Washoe County Sheriff’s OfficeOffice
Reno, NVReno, NV

Various Names for These Various Names for These DrugsDrugs
ANTIPSYCHOTICS MAJOR TRANQUILIZERS NEUROLEPTICS PSYCHOTROPIC AGENTS

SchizophreniaSchizophreniaDisturbance lasting at least 6 months & Disturbance lasting at least 6 months &
including at least 1 month of 2 or more of the including at least 1 month of 2 or more of the following positive symptoms:following positive symptoms:
PositivePositive symptoms include symptoms include Delusions-Delusions- beliefs that are contrary to beliefs that are contrary to
reality & can involve control, grandeur, or reality & can involve control, grandeur, or persecutionpersecution
Hallucinations-Hallucinations- perceptions that occur in perceptions that occur in the absence of stimuli the absence of stimuli
often auditory and/or olfactoryoften auditory and/or olfactory Disorganized speechDisorganized speech Grossly disorganized or catatonic behaviorGrossly disorganized or catatonic behavior Negative symptomsNegative symptoms
DMS-IV

SchizophreniaSchizophrenia NegativeNegative symptoms: symptoms:
Alogia-Poverty of speech and low Alogia-Poverty of speech and low initiativeinitiative
Avolition-lack of willAvolition-lack of will Anhedonia-absence of pleasureAnhedonia-absence of pleasure Affective flattening-lack of emotional Affective flattening-lack of emotional
expressionexpressionMoodMood symptoms: symptoms: Depression, Anxiety, Hopelessness, etc.Depression, Anxiety, Hopelessness, etc. Social or occupational dysfunctionSocial or occupational dysfunction
DMS-IV

SchizophreniaSchizophrenia
Common onset 15-25 years of ageCommon onset 15-25 years of age 1% general population develops at some 1% general population develops at some
point in their livespoint in their lives Common major mental illness in 65+ Common major mental illness in 65+
yearsyears Smoking: 3 times more likely in Smoking: 3 times more likely in
schizophrenia than general populationschizophrenia than general population Excessive mortalityExcessive mortality
20% shorter life expectancy20% shorter life expectancy 10% suicide rate10% suicide rate
Antipsychotic MedicationsAntipsychotic Medications
Antipsychotic medications diminish the Antipsychotic medications diminish the thought disorder evident in schizophreniathought disorder evident in schizophrenia AP medications have similar efficacy AP medications have similar efficacy
(mostly act on positive symptoms)(mostly act on positive symptoms)
AP medications require weeks to take AP medications require weeks to take effecteffect
Antipsychotic MedicationsAntipsychotic Medications
We don’t know how they work but they act upon We don’t know how they work but they act upon many receptorsmany receptors DD11, D, D22, D, D44, D, D55, 5HT, 5HT22, 5HT, 5HT66, 5HT, 5HT77, alpha, alpha11--
adrenergic, Hadrenergic, H11, cholinergic - muscarinic, , cholinergic - muscarinic, nicotinicnicotinic
They have many side effects and serious toxicitiesThey have many side effects and serious toxicities We are not sure of their therapeutic rangeWe are not sure of their therapeutic range There is overlap between therapeutic and toxic There is overlap between therapeutic and toxic
blood concentrations for some - many are difficult blood concentrations for some - many are difficult to analyze - they are ubiquitousto analyze - they are ubiquitous

Antipsychotic MedicationsAntipsychotic MedicationsReceptor Oriented Side EffectsReceptor Oriented Side Effects
Sedation – AntihistaminicSedation – Antihistaminic Weight gain – AntiserotonergicWeight gain – Antiserotonergic EPS, prolactin release – AntidopaminergicEPS, prolactin release – Antidopaminergic Urinary retention, dry mouth, blurred Urinary retention, dry mouth, blurred
vision, constipation, sinus tachcardia, vision, constipation, sinus tachcardia, cognitionand memory effects – cognitionand memory effects – AnticholinergicAnticholinergic
Orthostatic hypotension, reflex Orthostatic hypotension, reflex tachycardia – Anti-alphatachycardia – Anti-alpha11-adrenergic-adrenergic

Introduction of Introduction of Antipsychotics Antipsychotics
in the USin the US
1950 1960 1970 1980 1990 2000
Chlo
rpro
mazi
n
e ‘54
Clo
zapin
e ‘90
Ris
peri
done
‘94Ola
nza
pin
e ‘96
Queti
apin
e ‘97
Zip
rasi
done
‘01
Flu
phenazi
ne
‘59Thio
ridazi
ne
‘59 Halo
peri
dol
‘67
Era of “Typical Antipsychotics”

Terms used to categorize Terms used to categorize antipsychoticsantipsychotics
Typical Typical vs. vs. AtypicalAtypical ConventionalConventional vs. vs. NovelNovel Classic Classic vs. vs. NewNew StandardStandard vs.vs. ModernModern 11stst Generation Generation vs. vs. 22ndnd Generation Generation

Classes of Antipsychotic Classes of Antipsychotic MedicationsMedications
TypicalTypical (e.g. CPZ) (e.g. CPZ) Block D2 receptorsBlock D2 receptors Produce neurological effects (Produce neurological effects (neurolepticsneuroleptics…)…)
AtypicalAtypical Greater separation between AP action and Greater separation between AP action and
extrapyramidal activityextrapyramidal activity Block D4 receptors: Clozapine acts on D4 Block D4 receptors: Clozapine acts on D4
receptors in the accumbens (but not in the receptors in the accumbens (but not in the striatum)striatum)
Less risk of extrapyramidal (EP) effectsLess risk of extrapyramidal (EP) effects Negative symptoms may respond to atypical Negative symptoms may respond to atypical
AP medications (e.g. risperdal)AP medications (e.g. risperdal)

Typical vs. AtypicalTypical vs. Atypical TypicalTypical
High DHigh D22
Low 5-HTLow 5-HT2A2A
DD11=D=D22
Increases NT in caudate and nucleus accumbensIncreases NT in caudate and nucleus accumbens AtypicalAtypical
High 5-HTHigh 5-HT2A2A
Lower DLower D22
Low DLow D11
Increases NT in nucleus accumbens onlyIncreases NT in nucleus accumbens only

Antipsychotics: ADMEAntipsychotics: ADME
Large interindividual variation in Large interindividual variation in bioavailabilitybioavailability
GI absorption tends to be incompleteGI absorption tends to be incomplete High degree of first pass metabolismHigh degree of first pass metabolism
Large to very large VLarge to very large Vdd
Weak basesWeak bases Highly protein bound Highly protein bound

Antipsychotics: ADMEAntipsychotics: ADME
Extensive hepatic metabolismExtensive hepatic metabolism CYP 450CYP 450 Possible CYP 450 polymorphismPossible CYP 450 polymorphism Significant active metabolite profileSignificant active metabolite profile

Phenothiazine AntipsychoticsPhenothiazine Antipsychotics
MellarilMellaril®® (thioridazine)(thioridazine)ProlixinProlixin®® (fluphenazine)(fluphenazine)
SerentilSerentil®® (mesoridazine)(mesoridazine)StelazineStelazine® ® (trifluoperazine)(trifluoperazine)ThorazineThorazine® ® (chlorpromazine)(chlorpromazine)TrilafonTrilafon® ® (perphenazine)(perphenazine)VesprinVesprin® ® (triflupromazine)(triflupromazine)
N
S
N
Cl
CH3
CH3
N
S
N
S
CH3
CH3
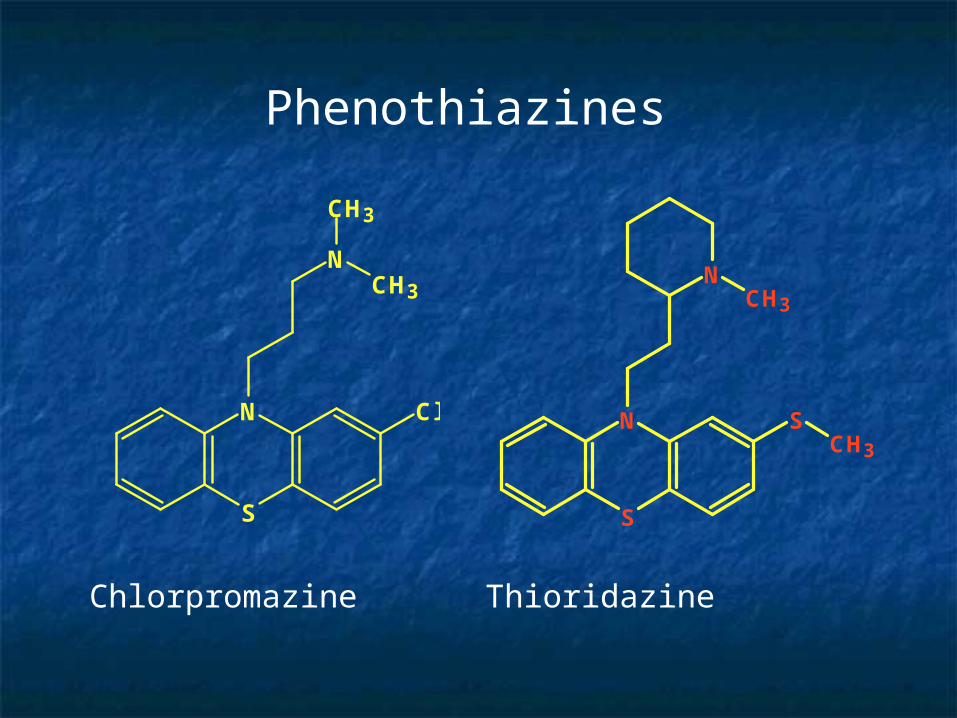
Phenothiazines
Chlorpromazine Thioridazine

ADDITIONAL CLASSICAL ADDITIONAL CLASSICAL ANITPSYCHOTICSANITPSYCHOTICS
HaldolHaldol® ® (haloperidol), (haloperidol), Haldol Haldol DecanoateDecanoate
LoxitaneLoxitane®® (loxapine)(loxapine)MobanMoban®® (molindone)(molindone)NavaneNavane® ® (thiothixene)(thiothixene)

Extrapyramidal SymptomsExtrapyramidal Symptoms Clinical SymptomsClinical Symptoms
Tremor Dystonic reactionsTremor Dystonic reactions Pseudo parkinsonism Pseudo parkinsonism Akathisia Akathisia
Therapy to Prevent EPSTherapy to Prevent EPS Treat EPS with benztropine (CogentinTreat EPS with benztropine (Cogentin), ),
trihexyphenidyl (Artane trihexyphenidyl (Artane ), biperiden ), biperiden (Akineton (Akineton ) or diphenhydramine) or diphenhydramine
Tardive dyskinesiasTardive dyskinesias Potentially irreversiblePotentially irreversible

Acute DystoniaAcute Dystonia (First week to month)(First week to month)
Severe spasm of the muscles of the Severe spasm of the muscles of the tongue, neck or backtongue, neck or back• These result in torticallis, facial grimacingThese result in torticallis, facial grimacing
Oculogyric Crisis: involuntary upward Oculogyric Crisis: involuntary upward deviation of the eyesdeviation of the eyes
Opisthotonus: tetanic spasm of the Opisthotonus: tetanic spasm of the back muscles causing the trunk to arch back muscles causing the trunk to arch forward while head and lower limbs are forward while head and lower limbs are thrust backward. thrust backward. • These may result in joint dislocationThese may result in joint dislocation
Laryngeal dystonia: can impair Laryngeal dystonia: can impair respirationrespiration

Pseudo-ParkinsonismPseudo-Parkinsonism bradykinesiabradykinesia
slowing of movementslowing of movement pill rollingpill rolling mask-like facesmask-like faces hyper salivation (drooling)hyper salivation (drooling) resting tremorresting tremor rigidityrigidity shuffling gaitshuffling gait cog wheelingcog wheeling stooped posturestooped posture

AkathisiaAkathisia
Inability to sit or remain quietInability to sit or remain quiet characterized bycharacterized by
pacing pacing squirming squirming the need to be in motion the need to be in motion profound sense of restlessnessprofound sense of restlessness

Tardive DyskinesiaTardive Dyskinesia Involuntary choreoathetiod movements of Involuntary choreoathetiod movements of
tongue and facetongue and face choreoathetiod: twisting, writhing worm-like choreoathetiod: twisting, writhing worm-like
movementsmovements lip smackinglip smacking tongue flicking motionstongue flicking motions may also produce movements of limbs, toes, fingersmay also produce movements of limbs, toes, fingers
Risk increases with length of time on medication and Risk increases with length of time on medication and dosage of medication. dosage of medication.
These symptoms are non-reversible for most These symptoms are non-reversible for most patients.patients.
There is no effective treatment for TDThere is no effective treatment for TD

Sudden Death SyndromeSudden Death Syndrome PhenothiazinesPhenothiazines Large daily doses (>1000 mg)Large daily doses (>1000 mg) Mechanism:Mechanism:
AsphyxiationAsphyxiation seizureseizure ventricular fibrillationventricular fibrillation
CV collapse during hypotensive crisisCV collapse during hypotensive crisis Some atypical drugs also cause Some atypical drugs also cause
sudden deathsudden death

Neuroleptic Malignant SyndromeNeuroleptic Malignant Syndrome
Loss of thermal regulationLoss of thermal regulation Contributing Factors:Contributing Factors:
ambient heat & dehydrationambient heat & dehydration underlying brain damage & dementiaunderlying brain damage & dementia high neuroleptic dose (genetic high neuroleptic dose (genetic
vulnerability?)vulnerability?) TreatmentTreatment
neuroleptic withdrawalneuroleptic withdrawal intensive supportive care (hydration, intensive supportive care (hydration,
temp. reg.)temp. reg.) medications (dantrolene or pergolide)medications (dantrolene or pergolide)

Phenothiazine LethalityPhenothiazine Lethality
Phenothiazines are generally safe Phenothiazines are generally safe drugs even when taken in overdose.drugs even when taken in overdose.
Their therapeutic indices ~200.Their therapeutic indices ~200. Deaths due to overdose have been Deaths due to overdose have been
reported, but these are rare. reported, but these are rare.

Emergency Department Episodes 1994-2001Estimated From SAMSHA DAWN Data
0500
100015002000250030003500
chlorpromazine
fluphenazine
perphenazine
thioridazine
trifluoperazine

Thioridazine (MellarilThioridazine (Mellaril))
1959 Formulations:1959 Formulations: Tablets (10-100 mg)Tablets (10-100 mg) Liquid (30-100 mg/mL)Liquid (30-100 mg/mL)
Initial doseInitial dose 25 mg po t.i.d.25 mg po t.i.d.
Maximum: 800 mg/dayMaximum: 800 mg/day Titrate down to maintenance doseTitrate down to maintenance dose
N
S
N
S
CH3
CH3

Thioridazine: Thioridazine: PharmacologyPharmacology
VVdd: 18 L/kg: 18 L/kg Half-life:Half-life:
26-36 hr26-36 hr MetabolismMetabolism
in the gastric mucosa and during first pass in the gastric mucosa and during first pass 12 metabolites12 metabolites Pathways:Pathways:
Oxidation (e.g. mesoridazine*, sulforidazine*)Oxidation (e.g. mesoridazine*, sulforidazine*) Ring oxidation (e.g. ring sulfoxide)Ring oxidation (e.g. ring sulfoxide) N-DemethylationN-Demethylation HydroxylationHydroxylation Glucuronidation Glucuronidation
N
S
N
S
CH3
CH3

Thioridazine: DosingThioridazine: Dosing
Single Acute OralSingle Acute Oral Average serumAverage serum
4 hr4 hr25 mg: 0.05 mg/L parent25 mg: 0.05 mg/L parent
0.17 mg/L mesoridazine0.17 mg/L mesoridazine
0.05 mg/L sulforidazine0.05 mg/L sulforidazine Peak plasmaPeak plasma
100 mg: 0.24 mg/L thioridazine (1.7 hr) 100 mg: 0.24 mg/L thioridazine (1.7 hr)
0.32 mg/L 0.32 mg/L mesoridazine (4 hr)mesoridazine (4 hr)
0.08 mg/L 0.08 mg/L sulforidazine (6.9 hr)sulforidazine (6.9 hr)
N
S
N
S
CH3
CH3

Liver Establishes OverdoseLiver Establishes Overdose
A. Poklis, Chap 31, Casarett & Doull’s Toxicology:the Basic Science of Poisoning. C.D. Klaassen, ed. 2001

Suicide via Suicide via ChlorpromazineChlorpromazine
SubjectSubject 62 year old white female62 year old white female
assisted living complex assisted living complex private apartmentprivate apartment
historyhistory schizophreniaschizophrenia paranoiaparanoia reclusive reclusive tobacco usetobacco use

Suicide via Suicide via ChlorpromazineChlorpromazine
InvestigationInvestigation found by apartment managerfound by apartment manager
living room couchliving room couch
last contact 10 days prior last contact 10 days prior no evidence of disturbance or struggleno evidence of disturbance or struggle ME caseME case
unknown/ possible natural causeunknown/ possible natural cause
autopsy ordered autopsy ordered two letters with wording indicating suicidal intenttwo letters with wording indicating suicidal intent

Suicide via Suicide via ChlorpromazineChlorpromazine
AutopsyAutopsy Pulmonary emphysema, moderate diffusePulmonary emphysema, moderate diffuse Probable colloid goiter, thyroid glandProbable colloid goiter, thyroid gland Postmortem decomposition, severePostmortem decomposition, severe ToxicologyToxicology
Central “blood”Central “blood” chlorpromazine: positive (qns for quantification)chlorpromazine: positive (qns for quantification) alprazolam: 0.17 mg/Lalprazolam: 0.17 mg/L ethanol: 40 mg/dLethanol: 40 mg/dL
LiverLiver chlorpromazine: 550 mg/kgchlorpromazine: 550 mg/kg

Suicide via Suicide via ChlorpromazineChlorpromazine
DispositionDisposition further investigation revealed: further investigation revealed:
a recent chlorpromazine prescription a recent chlorpromazine prescription 40-50 tablets (100 mg) missing40-50 tablets (100 mg) missing
the decedent’s estranged husband had committed the decedent’s estranged husband had committed suicide four weeks priorsuicide four weeks prior
cause of death cause of death chlorpromazine toxicitychlorpromazine toxicity
manner of death manner of death suicidesuicide
RE Winecker Amer Acad Forensic Sci, 2003

Haloperidol: DosingHaloperidol: Dosing
Single AcuteSingle Acute 0.5 to 5 mg0.5 to 5 mg > 100 mg daily> 100 mg daily up 1000 mg dailyup 1000 mg daily
Peak PlasmaPeak Plasma OralOral
≤ ≤ 5 hr5 hr10 mg: 3 10 mg: 3 μμg/L g/L
IntramuscularIntramuscular20 min20 min2 mg: 5 2 mg: 5 μμg/Lg/L
Cl
N OHCCH2CH2CH2
O
F
OH
N
Cl
F
OH

Phenothiazines:Phenothiazines: BioAnalytical ConsiderationsBioAnalytical Considerations
Absorption to glasswareAbsorption to glassware
Interference (artifacts and mtb’S)Interference (artifacts and mtb’S)
Loss of drug in plasma: PROTEIN BINDINGLoss of drug in plasma: PROTEIN BINDING
Liver important for PM interpretation (10 mg/kg)Liver important for PM interpretation (10 mg/kg)
Postmortem re-distribution (8x)Postmortem re-distribution (8x)
Drug/metabolite stability Drug/metabolite stability

Phenothiazines:Phenothiazines:
BioAnalytical ConsiderationsBioAnalytical Considerations Spot testsSpot tests Detection in Routine ScreensDetection in Routine Screens
Liquid/Liquid or Solid Phase Extraction of basesLiquid/Liquid or Solid Phase Extraction of bases TLCTLC GC-NPD, GC-ECDGC-NPD, GC-ECD HPLCHPLC
Quantitative AnalysisQuantitative Analysis GC/MS GC/MS LOD- 1 to 5 ng/mLLOD- 1 to 5 ng/mL

Atypical AntipsychoticsAtypical Antipsychotics
Serotonin & Dopamine AntagonistsSerotonin & Dopamine Antagonists Treats both positive & negative Treats both positive & negative
symptoms with fewer side effects.symptoms with fewer side effects. Much Less Extrapyramidal SymptomsMuch Less Extrapyramidal Symptoms Controls Controls
Mood & BehaviorMood & Behavior -Physical Coordination -Physical Coordination AppetiteAppetite -Body Temperature-Body Temperature SleepSleep

0
1000
2000
3000
4000
5000
6000
1994 1995 1996 1997 1998 1999 2000 2001
olanzapine
quetiapine
risperidone
Emergency Department Episodes 1994-2001Estimated From SAMSHA DAWN Data

Olanzapine Olanzapine ChemistryChemistry(Zyprexa(Zyprexa®®))
StructureStructure CC1717HH2020NN44S S MW = 312.44MW = 312.44 pKa = 5.0, 7.4pKa = 5.0, 7.4 Thienobenzodiazepine DerivativeThienobenzodiazepine Derivative
Organic base Organic base

OlanzapineOlanzapineGeneral InformationGeneral Information
FDA Approval in late 1996FDA Approval in late 1996 Tablets as free base Tablets as free base
2.5, 5, 7.5, and 10-mg doses2.5, 5, 7.5, and 10-mg doses Daily doses range from 10-20 mg a Daily doses range from 10-20 mg a
dayday

Olanzapine Olanzapine Adverse Adverse EffectsEffects
DrowsinessDrowsiness Dry mouthDry mouth HypotensionHypotension ParasthesiasParasthesias CNS DepressionCNS Depression Tachycardia Tachycardia Increased mortality Increased mortality
in elderly with in elderly with dementia-related dementia-related psychosispsychosis
Life-threatening Life-threatening hyperglycemiahyperglycemia
Alteration of blood lipids Alteration of blood lipids Elongated Q-T intervalsElongated Q-T intervals Possible weight Possible weight
problemsproblems Gain and lossGain and loss
ConstipationConstipation

Olanzapine Olanzapine PharmacokineticsPharmacokinetics
AbsorptionAbsorption Well absorbedWell absorbed Extensive 1Extensive 1stst pass metabolism - 40 % pass metabolism - 40 %
DistributionDistribution VdVd 10 -20 L/kg10 -20 L/kg T T 1/21/2 21 - 54 hours21 - 54 hours Protein BindingProtein Binding93 %93 %

OlanzapineOlanzapine PharmacokineticsPharmacokinetics
MetabolismMetabolism P450 CYP 1A2 & 2D6P450 CYP 1A2 & 2D6 N-desmethyl & 2 N-desmethyl & 2
HydroxymethylolanzapineHydroxymethylolanzapine GlucuronidationGlucuronidation
EliminationElimination 57 % dose recovered in urine 57 % dose recovered in urine 7 % as unchanged drug7 % as unchanged drug

OlanzapineOlanzapine Analytical ConsiderationsAnalytical Considerations
Thio group very unstable Thio group very unstable In-vitro In-vitro
16 % in extraction16 % in extraction 40 % during 1 week at 440 % during 1 week at 4OOCC
Possibly stabilize with 0.25 % ascorbic Possibly stabilize with 0.25 % ascorbic acidacid

OlanzapineOlanzapine Analytical MethodsAnalytical Methods
TLCTLC HPLCHPLC GLCGLC GC/MSGC/MS Internal standards:Internal standards:
promazine, ethylmorphinepromazine, ethylmorphineethyl-olanzapine (Lilly Co)ethyl-olanzapine (Lilly Co)

Olanzapine Olanzapine Therapeutic Therapeutic Steady-State Trough Steady-State Trough
ConcentrationsConcentrationsDaily Dose Olanzapine, ng/mL
5 710 9-1415 19-2120 ~26
Aravagiri et al. Therap Drug Monitor, 1997

Olanzapine Olanzapine Blood Blood ConcentrationsConcentrations
1653 Clinical 1653 Clinical SpecimensSpecimens
Olanzapine Olanzapine (ng/mL)(ng/mL)
RangeRange 3 - 390 3 - 390 MeanMean 36 +/- 4036 +/- 40 MedianMedian 2626 86 % of the cases 86 % of the cases
Range: 5-75Range: 5-75
58 Postmortem 58 Postmortem SpecimensSpecimens
Olanzapine (ng/mL)Olanzapine (ng/mL) RangeRange 10 – 5,000 10 – 5,000 MeanMean 358 +/- 758358 +/- 758 MedianMedian 130130 75 % less than 30O 75 % less than 30O 86 % less than 50086 % less than 500
Robertson et al. J Forensic Sci, 1999

Olanzapine Olanzapine Blood Blood ConcentrationsConcentrations
Suggested that toxicity should be considered at Suggested that toxicity should be considered at conc above 100 ng/mLconc above 100 ng/mL
One death due primarily to olanzapine at 160 One death due primarily to olanzapine at 160 ng/mLng/mL
Other studies showed postmortem toxicity Other studies showed postmortem toxicity often above 1000 ng/mLoften above 1000 ng/mL
Literature reports of death at 237, 675, 400 Literature reports of death at 237, 675, 400 heart (270 carotid) ng/mLheart (270 carotid) ng/mL
Robertson et al. J Forensic Sci, 1999

Olanzapine Olanzapine Postmortem Femoral Blood Postmortem Femoral Blood
ConcentrationsConcentrations Mode of Death Olanzapine, ng/mL
mean rangeSuicides (5) 400 25 – 1,600Accident (11) 90 25 – 190Natural (5) 50 25 - 180Homicide (1) 50Undetermined (2) 10; 1,200 D. Anderson, AAFS 2003

Olanzapine Postmortem Olanzapine Postmortem RedistributionRedistribution
16 deaths – 16 deaths –
Heart/femoral ratio averaged 4.9 Heart/femoral ratio averaged 4.9 (0.7-23)(0.7-23)
D. Anderson, SOFT 1998
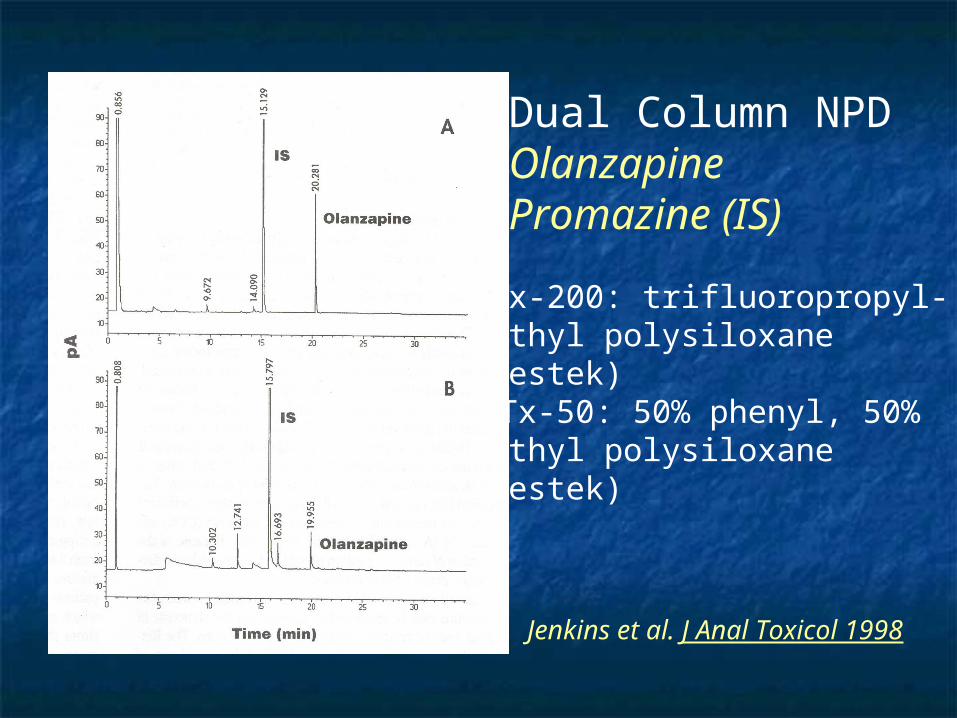
A. RTx-200: trifluoropropyl-methyl polysiloxane(Restek)
B. RTx-50: 50% phenyl, 50%methyl polysiloxane(Restek)
Dual Column NPD OlanzapinePromazine (IS)
Jenkins et al. J Anal Toxicol 1998

QuetiapineQuetiapine G General eneral InformationInformation
Developed in 1993Developed in 1993 FDA approval in Sept. 1997FDA approval in Sept. 1997 Manufactured by Zeneca Pharmaceuticals Manufactured by Zeneca Pharmaceuticals Tablets as a fumarate saltTablets as a fumarate salt (Seroquel(Seroquel®®))
25, 100 & 200 mg dose25, 100 & 200 mg dose Daily doses range from 150-750 mgDaily doses range from 150-750 mg

Quetiapine Quetiapine ChemistryChemistry
StructureStructure CC2121HH2525NN33OO22SS MW =383.6MW =383.6 pKa=3.3, 6.8pKa=3.3, 6.8 Dibenzothiazepine, organic base Dibenzothiazepine, organic base Structurally related to ClozapineStructurally related to Clozapine

Quetiapine Quetiapine Adverse EffectsAdverse Effects
DizzinessDizziness Somnolence, Somnolence,
sedationsedation ConstipationConstipation Dry mouthDry mouth DyspepsiaDyspepsia TachycardiaTachycardia HypotensionHypotension
HyperglycemiaHyperglycemia DiabetesDiabetes HeadacheHeadache

QuetiapineQuetiapine Pharmacokinetics Pharmacokinetics
AbsorptionAbsorption Rapidly and completely absorbed after Rapidly and completely absorbed after
oral administration.oral administration. DistributionDistribution
VdVd 10 L/kg10 L/kg T T 1/21/2 2.7-9.3 hours2.7-9.3 hours Protein BindingProtein Binding83 %83 %

QuetiapineQuetiapine PharmacokineticsPharmacokinetics
MetabolismMetabolism CYP3A4CYP3A4
Sulfoxidation - InactiveSulfoxidation - Inactive Oxidation - InactiveOxidation - Inactive
Active Metabolite : 7-HydroxyquetiapineActive Metabolite : 7-Hydroxyquetiapine EliminationElimination
73 % dose recovered in urine73 % dose recovered in urine Less 1% as unchanged drugLess 1% as unchanged drug

Quetiapine Quetiapine Dosage Dosage RegimenRegimen
Peak Plasma conc within 1.5 hoursPeak Plasma conc within 1.5 hours Steady state within 2 days of dosingSteady state within 2 days of dosing DosingDosing
Day 1: Day 1: 25 mg bid25 mg bid Day 2-3:Day 2-3: 25-50 mg bid or tid25-50 mg bid or tid Target:Target: 300-400 mg a day300-400 mg a day

QuetiapineQuetiapineTherapeutic Therapeutic
ConcentrationsConcentrations 75 mg oral dose75 mg oral dose
mean, 279 ng/mLmean, 279 ng/mLrange, 140 – 365 ng/mLrange, 140 – 365 ng/mL
450 mg daily dose450 mg daily dosemean, 402 ng/mL mean, 402 ng/mL range, 195 – 632 ng/mLrange, 195 – 632 ng/mL

QuetiapineQuetiapine
Mode Heart Blood Femoral Blood LiverSuicide (22 cases) 6.6 (14 ) 5.3 (12) 76 (7)Accident (24) 2.3 (12) 2.3 (7) 37 (4)Natural (33) 0.65 (7) 0.62 (4) 5.4 (3)
Total 79 cases**Not all cases contained parent drug - metabolites only in some
Average Quetiapine (ug/ml or ug/g)
D. Anderson, AAFS 2003

Toxic Quetiapine Toxic Quetiapine ConcentrationsConcentrations
Parker and McIntyre, JAT, 2005 (21 cases)Parker and McIntyre, JAT, 2005 (21 cases) > than 1 mg/L in peripheral and central blood> than 1 mg/L in peripheral and central blood > than 0.5 mg/L in vitreous> than 0.5 mg/L in vitreous > than 5 mg/kg in liver – especially helpful > than 5 mg/kg in liver – especially helpful
Wise and Jenkins, JFS, 2005 (3 cases)Wise and Jenkins, JFS, 2005 (3 cases) Heart blood 0.72-18.37 mg/LHeart blood 0.72-18.37 mg/L
Langman, Kaliciak, Carlyle, JAT, 2004 (3 Langman, Kaliciak, Carlyle, JAT, 2004 (3 cases)cases) Blood: 7.2, 16, 5.9 mg/LBlood: 7.2, 16, 5.9 mg/L Liver: 120 mg/kg (only data reported)Liver: 120 mg/kg (only data reported)
Similar reports in literatureSimilar reports in literature

QuetiapineQuetiapine Analytical ConsiderationsAnalytical Considerations
Basic DrugBasic Drug L/L extractions-VariousL/L extractions-Various TLCTLC GC/NPD GC/NPD HPLCHPLC GC/MSGC/MS
Metabolite PatternMetabolite Pattern

Quetiapine Quetiapine Cross-reacts Cross-reacts with TCA Immunoassayswith TCA Immunoassays
Emit & CEDIA, not Triage Emit & CEDIA, not Triage cross-reacts at 100 ug/mL parent drug in urinecross-reacts at 100 ug/mL parent drug in urine
Normal therapeutic urine <1.0 ug/mL Normal therapeutic urine <1.0 ug/mL parent drugparent drug
Patient urine following therapy & Patient urine following therapy & overdose, positive yield TCA resultsoverdose, positive yield TCA results
Cross-reactivity related to metabolitesCross-reactivity related to metabolites
Hendrickson & Morocco, J Clin Toxicol 2003

Capillary HP-5 NPDCapillary HP-5 NPD
A. 7-Hydroxyquetiapine C. quetiapine metaboliteB. quetiapine metabolite D. quetiapine
Anderson & Fritz J Anal Toxicol 2000

QuetiapineQuetiapine GC/MSGC/MS
Quetiapine: Quetiapine: 210, 239, 144, 253, 321210, 239, 144, 253, 321 Major Metabolite:Major Metabolite: 227, 210, 209, & 251227, 210, 209, & 251 Minor Metabolites:Minor Metabolites: 210, 239, 209, 251210, 239, 209, 251
210, 209, 239, 251, 322210, 209, 239, 251, 322

Suicide via QuetiapineSuicide via Quetiapine
SubjectSubject 44 year old white female - homemaker44 year old white female - homemaker History - depressionHistory - depression
medicationsmedications bupropionbupropion fluoxetinefluoxetine dextroamphetaminedextroamphetamine quetiapinequetiapine

Suicide via QuetiapineSuicide via Quetiapine
InvestigationInvestigation found by neighbors 3 p.m.found by neighbors 3 p.m. last seen alive 9:30 a.m. last seen alive 9:30 a.m. no evidence of disturbance or struggleno evidence of disturbance or struggle
body in bedroombody in bedroom an autopsy orderedan autopsy ordered
a letter addressed to “my dear husband” - a letter addressed to “my dear husband” - wording indicating suicidewording indicating suicide
a bottle of quetiapine - 70 pills missinga bottle of quetiapine - 70 pills missing

Suicide via QuetiapineSuicide via Quetiapine AutopsyAutopsy
Mild pulmonary congestion and edemaMild pulmonary congestion and edema Healing contusions of abdomen and thighHealing contusions of abdomen and thigh Granular material in stomachGranular material in stomach ToxicologyToxicology
Central bloodCentral blood Trace: bupropion, detromethorphan, doxylamineTrace: bupropion, detromethorphan, doxylamine Fluoxetine: 0.7 mg/LFluoxetine: 0.7 mg/L Norfluoxetine: 1.1 mg/LNorfluoxetine: 1.1 mg/L Quetiapine: 230 mg/LQuetiapine: 230 mg/L
Peripheral bloodPeripheral blood Quetiapine: 43 mg/LQuetiapine: 43 mg/L
LiverLiver Quetiapine: 200 mg/kgQuetiapine: 200 mg/kg

Suicide via QuetiapineSuicide via Quetiapine
Disposition of deathDisposition of death cause - quetiapine toxicitycause - quetiapine toxicity manner - suicidemanner - suicide
RE Winecker Amer Acad Forensic Sci, 2003

Risperidone Risperidone General InformationGeneral Information
Available since 1993Available since 1993 Tablets 0.25, 0.5, 1, 2, 3, 4-mgTablets 0.25, 0.5, 1, 2, 3, 4-mg Solution 1 mg/mlSolution 1 mg/ml

RisperidoneRisperidone ChemistryChemistry
CC2323HH2727FNFN44OO22
MW = 410.49MW = 410.49 pKa = ??pKa = ?? Benzisoxazole DerivativeBenzisoxazole Derivative

RisperidoneRisperidone PharmacokineticsPharmacokinetics
DosingDosing Initial DoseInitial Dose 1 mg bid1 mg bid
Increase 1 mg bid on 2nd and 3rd dayIncrease 1 mg bid on 2nd and 3rd day Maximum 3 mg bidMaximum 3 mg bid
Dosage adjustments at 1-week intervalsDosage adjustments at 1-week intervals
BioavailabilityBioavailability 68-82 %68-82 %
DistributionDistribution VdVd 0.7-2.1 L/kg0.7-2.1 L/kg

RisperidoneRisperidone PharmacokineticsPharmacokinetics
MetabolismMetabolism Hydroxylation Hydroxylation
9-Hydroxyrisperidone 9-Hydroxyrisperidone (9-OH-R) (9-OH-R) ActiveActive - - equivalent to risperidoneequivalent to risperidone CYP2D6 polymorphismCYP2D6 polymorphism
~ 6-10% caucasians~ 6-10% caucasians ~ 1% Asian~ 1% Asian
Oxidative N-dealkylationOxidative N-dealkylation inactiveinactive

RisperidoneRisperidone PharmacokineticsPharmacokinetics
Plasma half-lifePlasma half-life risperidonerisperidone ~ 3 hr (fast) ~ 3 hr (fast) risperidone ~ 20 hr (slow)risperidone ~ 20 hr (slow) 9-OH-risperidone9-OH-risperidone ~ 21 hr (fast) ~ 21 hr (fast) 9-OH-risperidone 9-OH-risperidone ~ 30 hr ~ 30 hr
(slow)(slow) EliminationElimination
70% dose recovered in urine70% dose recovered in urine 15% dose recovered in feces15% dose recovered in feces

RisperidoneRisperidone PharmacokineticsPharmacokinetics
Blood/plasma ratio 0.67Blood/plasma ratio 0.67 Time to peak plasma concentrationTime to peak plasma concentration
risperidonerisperidone ~ 1 hr~ 1 hr 9-OH-risperidone9-OH-risperidone ~ 3 hr (fast)~ 3 hr (fast)
~~ 17 hr 17 hr (slow)(slow)
Time to steady stateTime to steady state risperidonerisperidone ~ 1 day (fast -EM) ~ 1 day (fast -EM)
~ 5 day (slow-PM)~ 5 day (slow-PM) 9-OH-risperidone9-OH-risperidone ~ 5 days (fast)~ 5 days (fast)

Risperidone Risperidone Therapeutic Therapeutic Steady-State Plasma Steady-State Plasma
Concentrations, ng/mLConcentrations, ng/mLDose, mg Risperidone 9-hydroxyrisperidone
2 3.2 11 6 9.2 3410 13 6016 15 98
Recent Case WCSO – None DetectedLong Term Care Facility – Dose to patient 0.5 mg/day
Were they providing adequate care and giving prescribed dose?
National Medical Services, Toxi-News,2001

RisperidoneRisperidoneAdverse EffectsAdverse Effects
DizzinessDizziness SomnolenceSomnolence NauseaNausea HypotensionHypotension AnxietyAnxiety HeadacheHeadache
TachycardiaTachycardia EKG changesEKG changes ConfusionConfusion LethargyLethargy DroolingDrooling Sudden death in Sudden death in
elderly with elderly with dementiadementia

RisperidoneRisperidoneOverdose CasesOverdose Cases
8 cases: 20 - 300 mg ingested8 cases: 20 - 300 mg ingested No fatalitiesNo fatalities Drowsiness & sedationDrowsiness & sedation Tachycardia & hypotensionTachycardia & hypotension Extrapyramidal symptomsExtrapyramidal symptoms
MM McMullin, AAFS 1995

RisperidoneRisperidoneAnalytical ConsiderationsAnalytical Considerations
Large MW & Polar moleculeLarge MW & Polar molecule Low Therapeutic ConcentrationsLow Therapeutic Concentrations RIA (Janssen)RIA (Janssen) ToxiLab RToxiLab Rff 0.25 Ris/9-OH, brown stage 0.25 Ris/9-OH, brown stage
IV IV Liquid-liquid extractionLiquid-liquid extraction GC: Thermal degradationGC: Thermal degradation HPLC: diode-array or MSHPLC: diode-array or MS

RisperidoneRisperidoneToxic &Toxic & Lethal Lethal ConcentrationsConcentrations
100 mg ingestion100 mg ingestion 1,070/100 ng/ml (Ris/9-OH-R)-1,070/100 ng/ml (Ris/9-OH-R)-
Admission BloodAdmission Blood 74/50 ng/ml - 48 hours post ingestion74/50 ng/ml - 48 hours post ingestion
Suicidal IngestionSuicidal Ingestion1,800 ng/ml1,800 ng/ml BloodBlood14,400 ng/ml14,400 ng/mlUrineUrine
Lee et al., J. Clin., Psychopharm., 1997Springfield & Bodiford, J Anal Toxicol, 1996

ClozapineClozapineGeneral InformationGeneral Information
Available since 1989Available since 1989
Tablets 25, 100 mgTablets 25, 100 mg
CC18HH19ClNClN4
MW = 326.83MW = 326.83
pKa = 3.7, 7.6pKa = 3.7, 7.6
Tricyclic Tricyclic dibenzodiazepine dibenzodiazepine derivativederivative

ClozapineClozapinePharmacokineticsPharmacokinetics
DosingDosing Initial 12.5 mg once or twice per dayInitial 12.5 mg once or twice per day Increase to 300-450 mg/day after two weeksIncrease to 300-450 mg/day after two weeks
Bioavailability Bioavailability 50-60%50-60% Vd Vd 2-7 L/kg2-7 L/kg Half-LifeHalf-Life 6-17 hrs.6-17 hrs. MetabolismMetabolism
N-demethylationN-demethylation, N-oxidation, oxidation of chlorine-, N-oxidation, oxidation of chlorine-containing ring, and thiomethyl conjugation.containing ring, and thiomethyl conjugation.
N-desmethylclozapine has very little activity; others N-desmethylclozapine has very little activity; others inactiveinactive
Metabolized by P450 CYP1A2Metabolized by P450 CYP1A2

ClozapineClozapinePharmacokineticsPharmacokinetics
EliminationElimination 50% dose excreted in urine50% dose excreted in urine 30% dose excreted in feces30% dose excreted in feces Trace amounts of unchanged drug Trace amounts of unchanged drug
excreted in urine in therapeutic dosingexcreted in urine in therapeutic dosing Blood/plasma ratio 0.80Blood/plasma ratio 0.80 Time to peak plasma concentrationTime to peak plasma concentration
3 hrs 3 hrs Range: 1-6.3 hrs Range: 1-6.3 hrs

Clozapine Clozapine TTherapeutic Steady herapeutic Steady State Plasma ConcentrationsState Plasma Concentrations
500 mg daily for 12 weeks500 mg daily for 12 weeks Clozapine 0.472 mg/L Norclozapine 0.201 mg/LClozapine 0.472 mg/L Norclozapine 0.201 mg/L
in those who responded to treatmentin those who responded to treatment Clozapine 0.328 mg/L Norclozapine 0.156 mg/LClozapine 0.328 mg/L Norclozapine 0.156 mg/L
in those unresponsive to treatmentin those unresponsive to treatment Threshold for response 0.350–0.400 mg/L but adverse Threshold for response 0.350–0.400 mg/L but adverse
effects over twice as high at 0.350 or greater as effects over twice as high at 0.350 or greater as compared to below 0.350compared to below 0.350
200-700 mg/day200-700 mg/day 0.03-1.016 mg/L 0.03-1.016 mg/L
All studies show wide variations in concentrations All studies show wide variations in concentrations as a function of doseas a function of dose

ClozapineClozapineAdverse AffectsAdverse Affects
AgranulocytosisAgranulocytosis Risk so high that drug should be reserved for use Risk so high that drug should be reserved for use
in in Severely ill patients who show inadequate response to Severely ill patients who show inadequate response to
conventional antipsychoticsconventional antipsychotics Reducing the risk of recurrent suicidal behaviorReducing the risk of recurrent suicidal behavior
Patients must have a baseline WBC and ANC Patients must have a baseline WBC and ANC before initiation of therapy as well as regular before initiation of therapy as well as regular WBC and ANC during treatment and for a least 4 WBC and ANC during treatment and for a least 4 weeks after discontinuation of treatment.weeks after discontinuation of treatment.
SeizuresSeizures Greater chance at higher doseGreater chance at higher dose

ClozapineClozapineAdverse AffectsAdverse Affects
Myocarditis –Myocarditis – Potentially fatal especially in first month of Potentially fatal especially in first month of
therapytherapy Orthostatic hypotensionOrthostatic hypotension Increased mortality in elerdly patients with Increased mortality in elerdly patients with
dementia-related physhosisdementia-related physhosis HyperglycemiaHyperglycemia NMS – Neuroleptic Malignant SyndroneNMS – Neuroleptic Malignant Syndrone Anticholinergic toxicityAnticholinergic toxicity

Clozapine Clozapine Analytical ConsiderationsAnalytical Considerations
Not a difficult drug to assayNot a difficult drug to assay Gas ChromatographyGas Chromatography
FID, NPD, MSFID, NPD, MS Concern over N-oxide reduction to clozapineConcern over N-oxide reduction to clozapine
HPLCHPLC UV, electrochemical detection, MSUV, electrochemical detection, MS

Clozapine Clozapine Concentrations in Concentrations in Non-Lethal Overdose CasesNon-Lethal Overdose Cases
Pediatric patientsPediatric patients Confusion, ataxia, hyper-hypo tonic Confusion, ataxia, hyper-hypo tonic
disordersdisorders 0.51; 0.54 mg/L0.51; 0.54 mg/L
Adults (accidental overdose)Adults (accidental overdose) SeizuresSeizures
1.3; 2.2 ; 3.8 mg/L1.3; 2.2 ; 3.8 mg/L Adults (intentional overdose – 7 cases)Adults (intentional overdose – 7 cases)
2.9 – 9.5 mg/L2.9 – 9.5 mg/L

Clozapine Clozapine Concentrations in Concentrations in Fatal Overdose CasesFatal Overdose Cases
BloodBlood(mg/L)(mg/L)
LiverLiver(mg/kg)(mg/kg)
AverageAverage 5.25.2 4646
RangeRange 1.2 - 131.2 - 13 19 - 8519 - 85
Baselt, Disposition of Toxic Drugs and Chemical in Man, Seventh Baselt, Disposition of Toxic Drugs and Chemical in Man, Seventh Ed., 2004Ed., 2004

ZiprasidoneZiprasidone(Geodon(Geodon®®))
Available since 1992Available since 1992 Capsules 20,40,60,80 Capsules 20,40,60,80
mgmg Solution for injectionSolution for injection
20 mg/mL20 mg/mL
CC2121HH2121ClNClN44OSOS MW = 412 MW = 412
If you are a mass spectrometerIf you are a mass spectrometer

ZiprasidoneZiprasidonePharmacologyPharmacology
High affinity for:High affinity for: DD22, D, D33, 5HT, 5HT2A2A, 5HT, 5HT2C2C,5HT,5HT1A1A, 5HT, 5HT1D1D, , 11
Moderate affinity for HModerate affinity for H11
Antagonist for:Antagonist for: DD22, 5HT, 5HT2A2A, 5HT, 5HT1D 1D High 5HT/DHigh 5HT/D
Agonist for 5HTAgonist for 5HT1A1A
Inhibits serotonin and norepinephrine reuptakeInhibits serotonin and norepinephrine reuptake No affinity for muscarinic receptorNo affinity for muscarinic receptor

ZiprasidoneZiprasidonePharmacokineticsPharmacokinetics
DosingDosing SchizophreniaSchizophrenia
Initial 20 mg BID with foodInitial 20 mg BID with food If necessary, may increase slowly to 80 mg BIDIf necessary, may increase slowly to 80 mg BID
Bipolar maniaBipolar mania 40 mg BID with food40 mg BID with food Increase to 60 or 80 mg BID on second dayIncrease to 60 or 80 mg BID on second day Adjust dose efficacy and tolerance to 40-80 mg BIDAdjust dose efficacy and tolerance to 40-80 mg BID
Bioavailability Bioavailability 60%60% VdVd 1.5 L/kg1.5 L/kg Half-LifeHalf-Life 4 – 8 hrs4 – 8 hrs

ZiprasidoneZiprasidonePharmacokineticsPharmacokinetics
MetabolismMetabolism 12 known metabolites12 known metabolites
Therapeutic affect primarily due to parent drugTherapeutic affect primarily due to parent drug Major circulating metabolites are:Major circulating metabolites are:
Benzisothiazole (BITP) sulphoxideBenzisothiazole (BITP) sulphoxide BITP-sulphoneBITP-sulphone Ziprasidone sulphoxideZiprasidone sulphoxide S-methyl-dihydroziprasidoneS-methyl-dihydroziprasidone
Metabolism mediated by P450 CYP3A4Metabolism mediated by P450 CYP3A4 CYP1A2 to a much lesser extentCYP1A2 to a much lesser extent

ZiprasidoneZiprasidonePharmacokineticsPharmacokinetics
EliminationElimination 20% in urine20% in urine
Only trace amounts of unchanged drugOnly trace amounts of unchanged drug 66% in feces66% in feces
Time to peak plasma concentrationTime to peak plasma concentration 2 – 6 hrs2 – 6 hrs

ZiprasidoneZiprasidoneAdverse AffectsAdverse Affects
During TherapyDuring Therapy SedationSedation HeadacheHeadache Postural hypotensionPostural hypotension NMSNMS Tardive dyskensiaTardive dyskensia Prolongation of QT Prolongation of QT
intervalinterval Less weight gain than Less weight gain than
other atypicalsother atypicals DizzinessDizziness
OverdoseOverdose Several cases all non-Several cases all non-
fatalfatal QT changes (minimal)QT changes (minimal) DeleriumDelerium Hemodynamic instabilityHemodynamic instability DiarrheaDiarrhea Urinary retentionUrinary retention No EPSNo EPS
If you have a fatal If you have a fatal case, let me know!case, let me know!

ZiprasidoneZiprasidoneBlood ConcentrationsBlood Concentrations
4 healthy males administered 20 mg 4 healthy males administered 20 mg Ziprasidone for 11 daysZiprasidone for 11 days Mean plasma concentration 45.4 ng/mL with a Mean plasma concentration 45.4 ng/mL with a
range of 28.8-62 ng/mLrange of 28.8-62 ng/mL 39 males administered fixed doses of 10, 39 males administered fixed doses of 10,
40, and 40 escalated to 80, and 40 40, and 40 escalated to 80, and 40 escalated to 120 mgescalated to 120 mg On day 18, peak plasma concentrations wereOn day 18, peak plasma concentrations were 14.8, 44.6, 118.6, 139.4 ng/mL14.8, 44.6, 118.6, 139.4 ng/mL

ZiprasidoneZiprasidoneAnalytical ConsideratioinsAnalytical Consideratioins
ExtractionExtraction Liquid-liquidLiquid-liquid CC1818 cartridges cartridges
Detection/QuantificationDetection/Quantification HPLC – UV detectionHPLC – UV detection LC/MS/MSLC/MS/MS

AripiprazoleAripiprazole(Abilify(Abilify®®))
Available since Available since 20022002
TabletsTablets 10, 15, 20, 30 mg10, 15, 20, 30 mg
Oral Solution Oral Solution 1 mg/mL1 mg/mL
CC2323HH2727ClCl22NN33OO22
MW = 448.38MW = 448.38
AripiprazoleAripiprazolePharmacologyPharmacology
High Affinity for:High Affinity for: DD22, D3, 5HT1A, 5HT2A, D3, 5HT1A, 5HT2A
Moderate affinity for:Moderate affinity for: D4, 5HTD4, 5HT2C2C, 5H, 5HT7T7, , 11, H, H11, serotonin , serotonin
reuptake sitereuptake site No affinity for muscarinic receptorsNo affinity for muscarinic receptors * Partial agonist D* Partial agonist D22 and 5HT and 5HT1A 1A ** Antagonist at 5HTAntagonist at 5HT2A2A

AripiprazoleAripiprazolePharmacokineticsPharmacokinetics
DosingDosing 10 or 15 mg qd 10 or 15 mg qd
BioavailabilityBioavailability Tablets 87%Tablets 87% Solution near 100%Solution near 100%
VdVd = 4.9 L/kg= 4.9 L/kg Half-LifeHalf-Life
AripiprazoleAripiprazole 75 hrs EM 146 hrs 75 hrs EM 146 hrs PMPM
Dehydroariprazole 94 hrsDehydroariprazole 94 hrs

AripiprazoleAripiprazolePharmacokineticsPharmacokinetics
MetabolismMetabolism Dehydrogenation and hydroxylation Dehydrogenation and hydroxylation
CYP3A4 and CYP2D6CYP3A4 and CYP2D6 N-dealkylationN-dealkylation
CYP3A4CYP3A4 Active metabolite Active metabolite
DehydroaripiprazoleDehydroaripiprazole Approximately = parentApproximately = parent About 40% of parent in EMAbout 40% of parent in EM Measure total active moietyMeasure total active moiety

AripiprazoleAripiprazolePharmacokineticsPharmacokinetics
EliminationElimination 25% of dose excreted in urine25% of dose excreted in urine
Less than 1% excreted unchangedLess than 1% excreted unchanged 55% excreted in feces55% excreted in feces
Time to peak plasma concentrationTime to peak plasma concentration 3-5 hrs3-5 hrs
Steady state attained within 14 days Steady state attained within 14 days for both active moietiesfor both active moieties
AripiprazoleAripiprazoleAdverse AffectsAdverse Affects
Schizophrenia and Schizophrenia and Bipolar DisorderBipolar Disorder Headache, NauseaHeadache, Nausea Vomiting, Vomiting,
ConstipationConstipation Anxiety, agitationAnxiety, agitation Insomnia, sleepinessInsomnia, sleepiness DizzinessDizziness Akathisia, EPSAkathisia, EPS Drug InteractionsDrug Interactions
OverdoseOverdose Nausea, vomiting, Nausea, vomiting,
asthenia, diarrhea, asthenia, diarrhea, somnolencesomnolence
Tachycardia, EPSTachycardia, EPS CNS depressionCNS depression
Somnolence, Somnolence, transient loss of transient loss of consciousness, CNS consciousness, CNS effects for 2 weekseffects for 2 weeks
AripiprazoleAripiprazoleConcentration in BloodConcentration in Blood
27-year-old female27-year-old female Ingested 330 mg of aripiprazoleIngested 330 mg of aripiprazole Total active moiety of 716 ng/mLTotal active moiety of 716 ng/mL
According to manufacture = ~ 6X upper limit of According to manufacture = ~ 6X upper limit of therapeutic dosingtherapeutic dosing
One clinical study suggest range for aripiprazole of 146-One clinical study suggest range for aripiprazole of 146-254 ng/mL (metabolite not measured)254 ng/mL (metabolite not measured)
Not aware of a death case – doesn’t mean there isn’t oneNot aware of a death case – doesn’t mean there isn’t one AnalysisAnalysis
Clean up by direct injection of diluted sample and Clean up by direct injection of diluted sample and column-switchingcolumn-switching
LC/MS/MS or with UV detectionLC/MS/MS or with UV detection

AcknowledgementAcknowledgement
The presenter would like to thank Dr. The presenter would like to thank Dr. Alphonse Poklis for the organizational Alphonse Poklis for the organizational concept for this presentation.concept for this presentation.