“the imminent danger of lp(a): time to face the challenge ... · faculty disclosure i i have...
TRANSCRIPT

Lp(a): Phase 2 Data and NHLBI Recommendations
“The imminent danger of Lp(a):
Time to Face the Challenge”
EAS satellite meeting
Maastricht, The Netherlands
Sotirios Tsimikas, MD
Director of Vascular Medicine
Professor of Medicine
University of California San Diego
May 24, 2019
1

Faculty Disclosure
I I have received a research grant(s)/ in kind support
A From current sponsor(s) NO.
B From any institution NO
II I have been a speaker or participant in accredited CME/CPD
A From current sponsor(s) NO
B From any institution NO
III I have been a consultant/strategic advisor etc
A For current sponsor(s) NO
B For any institution (Boston Heart Dx) YES
IV I am a holder of (a) patent/shares/stock ownerships
A Related to presentation NO
B Not related to presentation (UCSD) YES
Declaration of financial interests
For the last 3 years and the subsequent 12 months:

Disclosures
Co-inventor and receives royalties from patents owned by the
University of California San Diego on oxidation-specific antibodies
Dual appointment at UCSD and Ionis Pharmaceuticals
Co-Founder Oxitope, Inc and Kleanthi Diagnostics
3

Association of Lp(a) with CVD risk in Patients on Statins from 7 Landmark Trials
• 29 069 patients8064 [28%] women; 5751 events, 95,576 person-years at risk
• AFCAPS, CARDS, 4D, JUPITER, LIPID, MIRACL, and 4S trials.
• Comparison of groups with lipoprotein(a) levels of <15 mg/dL, 15 to <30 mg/dL, 30 to <50 mg/dL, and ≥50 mg/dL.
• Multivariable adjustment included age, sex, previous CVD, diabetes, smoking, systolic blood pressure, LDL cholesterol corrected for lipoprotein(a) cholesterol, and HDL cholesterol.
• Associations were independent of established risk factors.
• In an interaction analysis, the association of high lipoprotein(a) with CVD risk was stronger in patients allocated a statin than in patients allocated placebo
Willeit et al. Lancet 2018;392:1311-20 4

Predictive value of on-statin vs. on-placebo Lp(a) with CVD risk from 7 Landmark Trials
In an interaction analysis, the association of high lipoprotein(a) with CVD risk was stronger in patients allocated a statin than in patients allocated placebo
Willeit et al. Lancet 2018;392:1311-20 5

Predictive value of on-statin vs. on-placebo Lp(a) with CVD risk from 7 Landmark Trials
In an interaction analysis, the association of high lipoprotein(a) with CVD risk was stronger in patients allocated a statin than in patients allocated placebo
Willeit et al. Lancet 2018;392:1311-20 6
“When LDL-attributable
risk is reduced with statin treatment, lipoprotein(a)-
associated risk becomes an even stronger predictor of
residual risk. This observation is especially evident at
lipoprotein(a) concentrations exceeding 50 mg/dL.”

Antisense Oligonucleotides Targeting Lp(a)
Antisense
Oligonucleotide
Tsimikas JACC 2017;69:692-711 7

AntisenseSingle-Strand
Multiple Mechanisms
DNAPhosphorothioate (PS)
2’-MOE, 2’-OMe, cEt, LNA
siRNADouble-strandRISC Mechanism
RNAPhosphodiester
2’-OMe, 2’-F
Aliphatic substituents
AptamerStructured
DNA or RNA Mixed modifications
Pegylation(REG1 anticoagulation system)
Distinct Chemical Classes of RNA-Based
Technologies & Therapeutics
Aptamer
Target
Protein
Sense
Strand
Antisense
Strand
Antisense
Strand
8

Antisense
Oligonucleotide RNA Target
The Antisense Drug-Receptor Interaction
~15-20 base pairs required for specificity and bindingNatural DNA and RNA do not make good drugs due to insufficient stability and distribution in animalsThis can be addressed with appropriate chemical modification
9
9

Isis Pharmaceuticals Confidential
RNaseH1 and siRNA Antisense Mechanisms
◼ siRNA Mechanism ◼ RNase H1 Mechanism
Antisense Strand
mRNA-Antisense Duplex
RNase H1
DNA
mRNA
Nucleus
Cytoplasm
Cell Membrane
Cell Membrane
CytoplasmNucleus
Antisense Strand
RNase H like nuclease
DNA
mRNA
RISCSense Strand
siRNA Duplex
10
10

Examples of Chemical Modifications Used in RNA Therapeutic Agents
2ʹ-O-methoxyethyl (MOE)
OB
O
O
B
O
O
B
O
O
O
B
O
O
OP
O
O
OP
O
B
O
OP
O
OP
O
OP
OMe
OO
Me
OO
Me
OO
Me
OO
MeX = S, O
-X
-X
-X
-X
-X
11
11

Significant Advances in Medicinal Chemistry of Antisense Improve Potency and Tolerability
LICALICA
Gen 2.5LICA Gen 2/2+
cEt Gapmer Design GalNac DesignMOE Gapmer Design
LICA 1st Gen
P-S
1X ↑10X ↑10X ↑10X =1000X
Side effect profile
Potency
(600-1200/wk) 100-300/wk 10-40/wk 10-40/wk 1-3/wk
12

Genetic architecture of the LPA gene
Schmidt et al J Lipid Res 2016;57:1339-5913

IONIS-APO(a)Rx Targets a unique splice site of Kringle-IV2
exon 24/25 junction present in 1 copy of all apo(a) mRNA
14
Graham et al J Lipid Res 2016;57:340-51 14

IONIS-APO(a)Rx ASO to Lower Plasma Lp(a)Targets a unique splice site of exon 24/25 present in 1 copy of all apo(a) mRNA, corresponding to a Kringle-IV2 repeat
2‘ Methoxyethyl Phosphorothioate Oligonucleotide (2’ MOE Gapmer)
S
S
OO
C H3
OO
C H3
OB
O
O
B
O
O
B
O
O
B
O
O
OP
O
O
OP
S
O
OP
S
O
OP
5'
3'
H
H
Chimera / Gapmer
affinity
stability
tolerability
RNase H1
Substrate
It does not bind to or reduce hepatic
expression or plasma levels of
plasminogen
C T T G T T C T G C T C C G T T G G T C
MOE MOEDeoxyMOE
Deoxy
15
15

Screening Process for ASOs
In Vivo
IND Toxicology/PK
Monkey Study (Tolerability)
Transgenic MouseRodent PK/Tox
Microwalk DRCs (Multiple Rounds)
Select Lead Sites For Microwalk
DRC (Multiple Rounds)
38 ASOs
6 ASOs
1 ASO
In Vitro
2280 ASOs
16
16

Pre-Clinical Proof-of-Concept Studies with ASO Therapy for Lp(a)Reduction in Lp(a) levels with ASO to apoB and apo(a)
Merki E et al Circulation 2008;118:743–53 Merki et al. JACC 2011;57:1611–2
17

Relationship of Plasma ISIS-APO(a)Rx Trough Concentrations and Mean Percent Change in Lp(a), OxPL-apoB and OxPL-apo(a) - 300 mg
18
Terminal elimination half-
life of ASO = ~23 days
Tsimikas et al Lancet 2015;386:1472-1483 18

IONIS-APO(a)Rx Phase 2 trial- Effect on Lp(a) and OxPL Patients with Lp(a) >50 mg/dL
Placebo Cohort A (50-175 mg/dL) Cohort B (>175 mg/dL)
Viney et al Lancet 2016;388:2239-53
Lp(a) OxPL-apoB OxPL-apo(a)
19

Reduction in Lp(a), OxPL-apoB and OxPL-apo(a) is strongly associated with reduced transendothelial monocyte migrationFirst In vivo demonstration of anti-inflammatory effect of Lp(a)-OxPL lowering
Placebo
Cohort A (50-175 mg/dL)
Cohort B (>175 mg/dL)
Transendothelial
monocyte migration
Viney et al Lancet 2016;388:2239-53
With van Capelleveen and Stroes
20

Traditional Lipid Profile
TC = LDL-C + VLDL-C+ HDL-
C
HDL-C
51 mg/dL
“LDL-C”
112 mg/dL
VLDL-C
26 mg/dL
To
tal C
ho
leste
rol
18
8 m
g/d
L
LDL-Ccorr
56 mg/dL
Lp(a)-C
56 mg/dL
HDL-C
51 mg/dL
VLDL-C
26 mg/dLTo
tal C
ho
leste
rol
18
8 m
g/d
L
To
tal C
ho
leste
rol
16
2 m
g/d
LA
po
B-1
00
95
mg
/dL
Ap
oB
-10
0
95
mg
/dL
Ap
oB
-10
0
79
mg
/dL
HDL-C
48 mg/dL
Corrected Lipid Profile for Lp(a)-C
TC = LDL-C + Lp(a)-C + VLDL-C + HDL-C
Corrected Lipid Profile
Post IONIS-Apo(a)Rx
LDL-Ccorr
72 mg/dL
Lp(a)-C
17 mg/dL
VLDL-C
25 mg/dL
Additional Net Reduction of Atherogenic LDL-
ApoB-100 with ASO to Apo(a)
Viney et al J Clin Lipidol 2018;12:702-10 21

Hepatocyte Targeting Antisense via Asialoglycoprotein Receptor Enhances Drug Delivery to the Liver 10-15xLICA - ligand conjugated antisense
Prakash et al Nucleic Acids Res 2014;42:8796-807 22

Dose-Dependent Effect of Optimized ASO to Apo(a) in Reducing Plasma Lp(a)IONIS-APO(a)-LRx has ~30x Improved Potency vs. IONIS-APO(a)Rx in Humans
ED50 4 mg vs 122 mg, 30-fold more potent
Viney et al Lancet 2016;388:2239-53 23

IONIS-APO(a)-LRx Produced Dose-dependent, Significant Reductions in Lp(a) in Phase 1 Study in Subjects with Lp(a) >30 mg/dL
Up to 97% Reduction in Lp(a),
with Mean Reduction of 85%Up to 99% Reduction in Lp(a),
with Mean Reduction of 92%
Single Ascending Dose Multiple Ascending Dose
Lp
(a)
(nm
ol/
L)
Mean
% C
ha
ng
e f
rom
Baseli
ne
(+
/-S
EM
)
Study Day
20 mgPlacebo 80 mg10 mg 40 mg 120 mg
Lp
(a)
(nm
ol/
L)
Mean
% C
ha
ng
e F
rom
Baseli
ne
(+
/-S
EM
) Study Day
20 mgPlacebo 10 mg 40 mg
Mean Lp(a) reductions:
10 mg = ↓ 68%
20 mg = ↓ 80%
40 mg = ↓ 92%Viney et al, Lancet 2016;388:2239-53 24

Safety and efficacy of AKCEA-APO(a)-LRx to lower
lipoprotein(a) levels in patients with established cardiovascular disease:
A phase 2 dose-ranging trial
University of California San Diego (ST, JLW); Akcea Therapeutics (E K-P, JG, LO’D), University of Cologne
(IG-B); Montreal Heart Institute, (J-CT); Excel Medical Clinical Trials, (SJB); Charité-UniversitätsmedizinBerlin and University Medicine Greifswald (E S-T); Oregon Health & Science University (MDS); Academic
Medical Center (ESS); University of Kansas Medical Center, (P.M.M.); Herlev and Gentofte Hospital, Copenhagen University Hospital and University of Copenhagen (BGN); Ionis Pharmaceuticals, Inc. (NJV,
ST)
Sotirios Tsimikas, Ewa Karwatowska-Prokopczuk, Ioanna Gouni-Berthold,
Jean-Claude Tardif, Seth J. Baum, Elizabeth Steinhagen-Thiessen, Michael D.
Shapiro, Erik S. Stroes, Patrick M. Moriarty, Børge G. Nordestgaard, Jonathan
Guerriero, Nicholas J. Viney, Louis O'Dea, Joseph L. Witztum on behalf of the
AKCEA-APO(a)-LRx Study Investigators
25

Study Design and Endpoints - AKCEA-APO(a)-LRx Trial
QW = every week; Q2W = every 2 weeks; Q4W = every 4 weeks; R = randomization; SC = subcutaneous.
*Cohorts (SC administration):
20 mg or placebo Q4W40 mg or placebo Q4W60 mg or placebo Q4W20 mg or placebo Q2W20 mg or placebo QW
Treatment duration: 6-12 months
Five cohorts*,N per cohort=54, randomized 5:1
(45 active, 9 placebo)
≤4 weeksScreening
16 weeks follow up
R
The primary endpoint was the mean percent change in Lp(a) from baseline to week 25–27 depending on dose regimen
Secondary endpoints included:
• Mean percent change in OxPL-apoB, OxPL-apo(a), LDL-C, apoB and the percentage of patients reaching Lp(a) <50 mg/dL (<125 nmol/L)
Tsimikas et al AHA 2018 26

Principal Investigators and Sites
Principal Investigator Investigator Site NamePatients
enrolled, n
Ioanna Gouni-BertholdPolyclinic for Endocrinology, Diabetes and Preventive Medicine, University of
Cologne29
Jean-Claude Tardif Montreal Heart Institute, University of Montreal 29
Seth Baum Excel Medical Clinical Trials, LLC 19
Elizabeth Steinhagen-Thiessen Charite - University Hospital Berlin - Campus Virchow - Hospital 19
Michael Shapiro Oregon Health & Science University 17
Erik Stroes Academic Medical Center 16
Patrick Moriarty University of Kansas Medical Center 15
Bǿrge Nordestgaard Copenhagen University Hospital 15
Daniel Gaudet ECOGENE-21 13
Marina CuchelPerelman School of Medicine at The University Perelman School of Medicine at
The University of Pennsylvania Translational Medicine & Human Genetics12
David Maron/Abha Khandelwal Stanford University Medical Center 11
Ib Christian Klausen Regionshospitalet Viborg, Hospitalsenhed Midt 10
Robert Rosenson Cardiometabolics Unit, Icahn School of Medicine at Mount Sinai 10
Anthony DeMaria UC-San Diego 9
Samuel Butman Verde Falley Medical Center Cardiovascular Research 9
Tsimikas et al AHA 2018 27

Principal investigators and Sites
Principal investigator Investigator Site Name Patients enrolled, n
Howard Weintraub New York University School of Medicine 8
Ruth McPherson University of Ottawa Heart Institute 8
Michael Koren Jacksonville Center for Clinical Research 6
Jean Bergeron Clinique des maladies lipidiques de Québec 6
Christie BallantyneCenter for Cardiovascular Disease Prevention
Baylor College of Medicine and DeBakey Heart & Vascular Center5
Anthony DeFranco Aurora St. Luke's Medical Center 5
Karen Aspry Miriam Hospital 5
Haitham Ahmed Cleveland Clinic 2
Rolf Andersen LGHealth / Penn Medicine Research Institute 2
Linda Hemphill Massachusetts General Hospital 1
Prediman Krishan Shah Cedars Sinai Medical Center 1
Michael Miller University of Maryland Medical Center 1
Russell Strader UCH-MHS 1
Merle Myerson Bassett Medical Center – Bassett Research Institute 1
George Thanassoulis Research Institute of the McGill University Health Centre 1
Tsimikas et al AHA 2018 28

Objectives, Patient Population and Key Inclusion/Exclusion Criteria
• This was a multicenter, international, randomized, blinded, placebo-controlled, dose-ranging Phase 2bstudy
• The patient population included:• Subjects with pre-existing cardiovascular disease (CAD, MI, PAD, stroke/TIA)
and baseline Lp(a) ≥60 mg/dL (~≥150 nmol/L) (normal levels: <30 mg/dL or <75 nmol/L)
• Key exclusion criteria included:• Revascularization or lipoprotein apheresis within 3 months of screening
• Acute coronary syndrome, major cardiac surgery, or stroke/TIA within 6 months of screening
• NYHA class IV
• Uncontrolled hypertension (>160/100 mm/Hg)
• Use of oral anticoagulants
Tsimikas et al AHA 2018 29

Laboratory measurements
OxPL-apoB, oxidized phospholipids on apolipoprotein B-10
OxPL-apo(a), oxidized phospholipids on apolipoprotein(a)
• Lp(a) molar concentrations (nmol/L) were measured with an isoform-independent assay at the Northwest Lipid Metabolism and Diabetes Research Laboratories, University of Washington
• Lp(a) mass (mg/dL) was estimated by dividing molar concentration by 2.5 (nmol/L ÷ 2.5 = mg/dL)
• OxPL-apoB and OxPL-apo(a) levels were measured with established assays at the University of California San Diego
• All safety lab measurements were measured at Medpace Reference Laboratories
Tsimikas et al AHA 2018 30

Baseline patient demographic characteristics
PCSK9 = proprotein convertase subtilisin/kexin type 9; QW = once a week; Q2W = every 2 weeks; Q4W = every 4 weeks; SD = standard deviation.
20 mg/Q4W
N=48
40 mg/Q4W
N=48
20 mg/Q2W
N=48
60 mg/Q4W
N=47
20 mg/QW
N=48
Pooled
Rx
N=239
Pooled
placebo
N=47
Age, years, mean (SD) 60 (9.6) 61.3 (10.6) 57.9 (11.5) 62.2 (9.7) 58.9 (8.0) 60.1 (10.0) 59.9 (10.5)
Sex, male, n (%) 29 (60.4) 36 (75.0) 31 (64.6) 33 (70.2) 28 (58.3) 157 (65.7) 32 (68.1)
Anti-Platelet Rx, n (%) 47 (97.9) 47 (97.9) 47 (97.9) 47 (100) 48 (100.0) 236 (98.7) 43 (91.5)
Lipid-Lowering Rx, n (%)
Statin
Ezetimibe
PCSK9 inhibitor
42 (87.5)
25 (52.1)
8 (16.7)
44 (91.7)
25 (52.1)
11 (22.9)
43 (89.6)
23 (47.9)
9 (18.8)
44 (93.6)
19 (40.4)
10 (21.3)
44 (91.7)
23 (47.9)
13 (27.1)
217 (90.8)
115 (48.1)
51 (21.3)
39 (83.0)
23 (48.9)
10 (21.3)
Previous history, n (%)
Coronary artery disease
Carotid artery disease
Peripheral artery disease
44 (91.7)
13 (27.1)
9 (18.8)
45 (93.8)
12 (25.0)
10 (20.8)
45 (93.8)
10 (20.8)
4 (8.3)
46 (97.9)
11 (23.4)
1 (2.1)
44 (91.7)
14 (29.2)
5 (10.4)
224 (93.7)
60 (25.1)
29 (12.1)
45 (95.7)
9 (19.1)
4 (8.5)
MI, n (%) 25 (52.1) 25 (52.1) 31 (64.6) 20 (42.6) 27 (56.3) 128 (53.6) 27 (57.4)
Stroke/TIA, n (%) 6 (12.5) 6 (12.5) 7 (14.6) 4 (8.6) 5 (10.4) 28 (11.7) 8 (17.0)
Hypertension, n (%) 28 (58.3) 35 (72.9) 34 (70.8) 31 (66.0) 25 (52.1) 153 (64.0) 30 (63.8)
Type 2 Diabetes, n (%) 7 (14.6) 8 (16.7) 5 (10.4) 4 (8.5) 6 (12.5) 30 (12.6) 10 (21.3)
AKCEA-APO(a)-LRx dose/regimen
Tsimikas et al AHA 2018 31
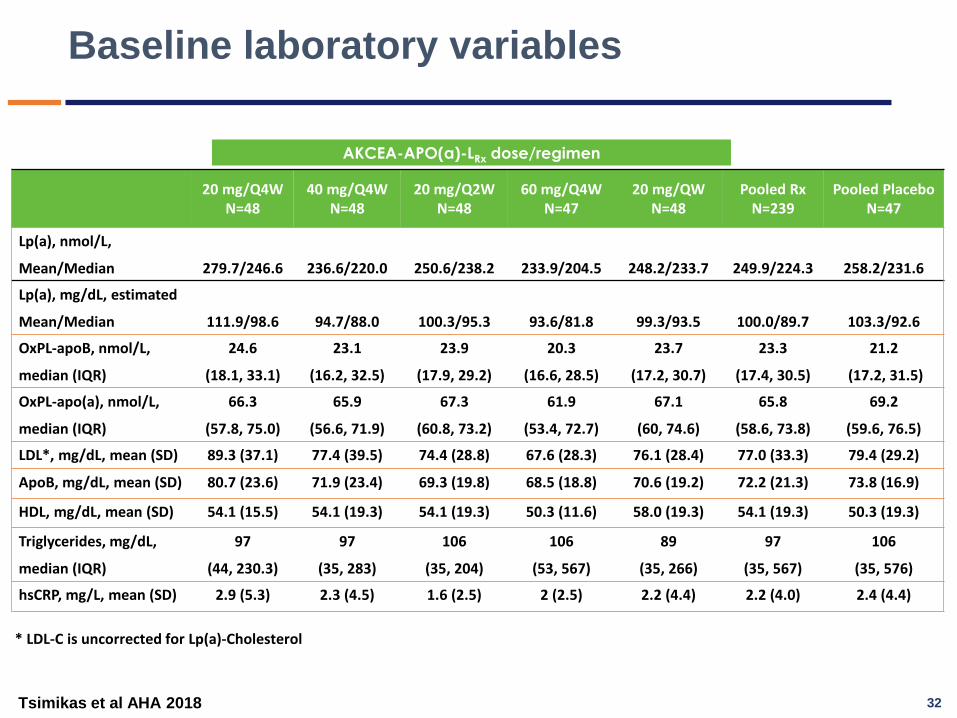
Baseline laboratory variables
20 mg/Q4WN=48
40 mg/Q4WN=48
20 mg/Q2WN=48
60 mg/Q4WN=47
20 mg/QWN=48
Pooled RxN=239
Pooled PlaceboN=47
Lp(a), nmol/L,
Mean/Median 279.7/246.6 236.6/220.0 250.6/238.2 233.9/204.5 248.2/233.7 249.9/224.3 258.2/231.6
Lp(a), mg/dL, estimated
Mean/Median 111.9/98.6 94.7/88.0 100.3/95.3 93.6/81.8 99.3/93.5 100.0/89.7 103.3/92.6
OxPL-apoB, nmol/L,
median (IQR)
24.6
(18.1, 33.1)
23.1
(16.2, 32.5)
23.9
(17.9, 29.2)
20.3
(16.6, 28.5)
23.7
(17.2, 30.7)
23.3
(17.4, 30.5)
21.2
(17.2, 31.5)
OxPL-apo(a), nmol/L,
median (IQR)
66.3
(57.8, 75.0)
65.9
(56.6, 71.9)
67.3
(60.8, 73.2)
61.9
(53.4, 72.7)
67.1
(60, 74.6)
65.8
(58.6, 73.8)
69.2
(59.6, 76.5)
LDL*, mg/dL, mean (SD) 89.3 (37.1) 77.4 (39.5) 74.4 (28.8) 67.6 (28.3) 76.1 (28.4) 77.0 (33.3) 79.4 (29.2)
ApoB, mg/dL, mean (SD) 80.7 (23.6) 71.9 (23.4) 69.3 (19.8) 68.5 (18.8) 70.6 (19.2) 72.2 (21.3) 73.8 (16.9)
HDL, mg/dL, mean (SD) 54.1 (15.5) 54.1 (19.3) 54.1 (19.3) 50.3 (11.6) 58.0 (19.3) 54.1 (19.3) 50.3 (19.3)
Triglycerides, mg/dL,
median (IQR)
97
(44, 230.3)
97
(35, 283)
106
(35, 204)
106
(53, 567)
89
(35, 266)
97
(35, 567)
106
(35, 576)
hsCRP, mg/L, mean (SD) 2.9 (5.3) 2.3 (4.5) 1.6 (2.5) 2 (2.5) 2.2 (4.4) 2.2 (4.0) 2.4 (4.4)
AKCEA-APO(a)-LRx dose/regimen
* LDL-C is uncorrected for Lp(a)-Cholesterol
Tsimikas et al AHA 2018 32

-6
-35
-56 -58
-72-80
-90
-70
-50
-30
-10
10
PooledPlacebo 20 mg/Q4W 40 mg/Q4W 20 mg/Q2W 60 mg/Q4W 20 mg/QW
LSM
ean
% c
han
ge in
Lp
(a)
P-values represent comparison to pooled placebo
Primary endpoint: Mean percent change (95% CI) in Lp(a) from baseline to week 25-27
P-values from an ANCOVA model with treatment as fixed factor and log-scale baseline as a covariate. Adjusted % change = (ratio of endpoint/baseline – 1) ×100. CI, confidence interval; Lp(a), lipoprotein(a); LS, least squares
P=0.0032
P<0.0001 P<0.0001
P<0.0001
P<0.0001
Primary efficacy endpoint was not affected by baseline Lp(a) levels, statin or PCSK9i use
Tsimikas et al AHA 2018 33

Primary endpoint: Mean percent change (SEM) in Lp(a) from baseline to week 25-27
PAT, primary analysis timepoint; QW, once a week; Q2W, every 2 weeks; Q4W, every 4 weeks; SEM, standard error of the mean.
-90
-80
-70
-60
-50
-40
-30
-20
-10
0
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28
Me
an
pe
rce
nt
ch
an
ge
(±
SEM
) fo
r Lp
(a)
ov
er
tim
e
Weeks
PAT(25-27)
60 mg/Q4W
20 mg/QW
40 mg/Q4W
20 mg/Q2W
Pooled placebo
20 mg/Q4W
Tsimikas et al AHA 2018 34

Absolute change in Lp(a) from baseline to week 25-27
20 mg/Q4W
N=48
40 mg/Q4W
N=48
20 mg/Q2W
N=48
60 mg/Q4W
N=47
20 mg/QWN=48
Pooled placebo
N=47
Absolute change
from baseline in
Lp(a), mg/dL
Mean (SD)
Absolute change
from baseline in
Lp(a), nmol/L
Mean (SD)
-38.4
(37.7)
-95.9
(94.4)
-46.8
(28.7)
-116.9
(71.7)
-52.1
(26.4)
-130.3
(66.1)
-59.8
(27.0)
-149.5
(67.4)
-75.1
(32.1)
-187.8
(80.3)
-6.1
(13.8)
-15.2
(34.6)
AKCEA-APO(a)-LRx dose/regimen
Tsimikas et al AHA 2018 35

Secondary endpoint: Percent of patients achieving Lp(a) ≤50 mg/dL (≤ 125 nmol/L) at PAT
6,4%
25.0%
62,5%64,6%
80,9%
97,7%
0
10
20
30
40
50
60
70
80
90
100
Pooled Placebo 20 mg/Q4W 40 mg/Q4W 20 mg/Q2W 60 mg/Q4W 20 mg/QW
Pe
rce
nt
of
pat
ien
ts a
chie
vin
g Lp
(a)
≤50
mg/
dL
(≤1
25
nm
ol/
L)P-values represent comparison
to pooled placebo
P=0.029
P<0.0001 P<0.0001
P<0.0001
P<0.0001
Tsimikas et al AHA 2018 36

Secondary endpoints: Percent change from baseline at week 25-27
P-value vs pooled placebo: * p<0.05; ** p<0.01; *** p<0.001
%change is at primary analysis timepoint. LDL-C, low-density lipoprotein cholesterol; QW, once a week; Q2W, every 2 weeks; Q4W, every 4 weeks.
Treatment
(dose/regimen)OxPL-apoB OxPL-apo(a) LDL-C ApoB
AKCEA-APO(a)-LRx
20 mg Q4W
40 mg Q4W
20 mg Q2W
60 mg Q4W
20 mg QW
-26.8**
-42.4***
-52.8***
-65.5***
-81.8***
-24.8
-37.5*
-38.6*
-53.5***
-61.2***
-5.2
-20.4***
-11.1*
-6.9*
-20.5**
-1.9
-12.8***
-7.6*
-4.0*
-14.5***
Pooled placebo 22.4 -17.6 1.2 2.0
Tsimikas et al AHA 2018 37

Summary of treatment emergent adverse events
Event, N (%)20 mg/Q4W
N=4840 mg/Q4W
N=4820 mg/Q2W
N=4860 mg/Q4W
N=4720 mg/QW
N=48Pooled Rx
N=239
Pooled placebo
N=47
At least one TEAE* 46 (95.8) 41 (85.4) 41 (85.4) 43 (91.5) 42 (87.5) 213 (89.1) 39 (83.0)
At least one serious TEAE 6 (12.5) 7 (14.6) 3 (6.3) 6 (12.8) 3 (6.3) 25 (10.5) 1 (2.1)
At least one related serious TEAE**
1 (2.1) 0 (0.0) 0 (0.0) 1 (2.1) 0 (0.0) 2 (0.8) 0 (0.0)
At least one TEAE leading to treatment discontinuation
2 (4.2) 0 (0.0) 1 (2.1) 3 (6.4) 5 (10.4) 11 (4.6) 2 (4.3)
TEAE leading to death*** 0 (0.0) 0 (0.0) 0 (0.0) 1 (2.1) 1 (2.1) 2 (0.8) 0 (0.0)
AKCEA-APO(a)-LRx dose/regimen
* The most frequent TEAE: Injection site erythema (25% in pooled Rx group)** Auto accident; Malaise*** Auto accident (same patient); Depression/suicide
Tsimikas et al AHA 2018 38
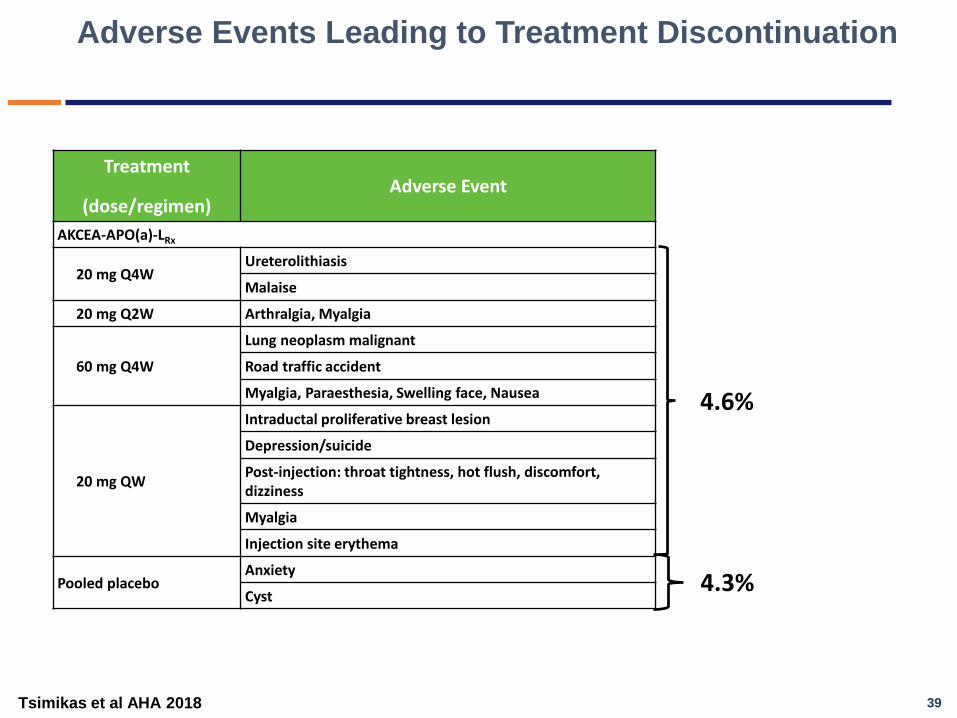
Adverse Events Leading to Treatment Discontinuation
Treatment
(dose/regimen)Adverse Event
AKCEA-APO(a)-LRx
20 mg Q4WUreterolithiasis
Malaise
20 mg Q2W Arthralgia, Myalgia
60 mg Q4W
Lung neoplasm malignant
Road traffic accident
Myalgia, Paraesthesia, Swelling face, Nausea
20 mg QW
Intraductal proliferative breast lesion
Depression/suicide
Post-injection: throat tightness, hot flush, discomfort, dizziness
Myalgia
Injection site erythema
Pooled placeboAnxiety
Cyst
4.6%
4.3%
Tsimikas et al AHA 2018 39

Changes in platelet-count, LFTs and renal function categories by treatment group
*2 occurrences across the study (regulatory standard)
**LFTs- No patient meet a Liver Safety Stopping Rule; However, 1 patient at the End of Treatment visit had AST 103 U/L (ULN =34 U/L, 3X ULN 102 U/L) and ALT 72 U/L (ULN = 41 U/L), with no change in total bilirubin, INR or Hy’s Law.
***Renal Function - 1 patient had unrelated pre-renal azotemia and 1 patient had unrelated incomplete 24 hour urine collection, creating an artifactual safety alert. Both continued in treatment.
n (%) 20 mg/Q4WN=48
40 mg/Q4WN=48
20 mg/Q2WN=48
60 mg/Q4WN=47
20 mg/QWN=48
Pooled RxN=239
Pooled Placebo
N=47
Platelet count, mm3
<140,000* 3 (6.3) 8 (16.7) 3 (6.4) 3 (6.3) 8 (16.7) 25 (10.5) 7 (14.9)
No confirmed platelet value <100,000 mm3
LFTs >3X ULN** 0 (0.0) 0 (0.0) 0 (0.0) 1 (2.1) 0 (0.0) 1 (0.4) 0 (0.0)
24 hr CrCl decrease
> 40% from baseline***
0 (0.0) 1 (2.1) 1 (2.1) 0 (0.0) 0 (0.0) 2 (0.8) 0 (0.0)
Tsimikas et al AHA 2018 40

Conclusions
• This trial achieved its primary endpoint and all of its secondary endpoints. AKCEA-APO(a)-LRx
significantly reduced Lp(a), OxPL-apoB, OxPL-apo(a), LDL-C and apoB levels
• 98% of patients achieved Lp(a) levels ≤50 mg/dL at the highest dose
• There were no safety concerns related to platelet counts, liver function or renal function
• A phase 3 outcomes trial to test the “Lp(a) hypothesis”, namely that lowering Lp(a) levels will reduce cardiovascular events, will start late 2019/early 2020
Tsimikas et al AHA 2018 41

Lp(a) cutoffs signifying increased CVD risk and effect of therapeutic agents to achieve these targets
Tsimikas JACC 2017;69:692-711 42

43

NHLBI Recommendations
• Explore mechanisms by which NHLBI could facilitate basic, mechanistic, preclinical, and clinical research on Lp(a).
• Foster collaborative research and resource sharing, leverage expertise of different groups and centers with complementary skills, methods, and knowledge, and leverage existing resources such as NHLBI cohorts.
• Support assignment of an ICD-10 code for the diagnosis of elevated Lp(a).
• Organize focused working groups comprised of wide array of stakeholders, including regulatory agencies, to standardize Lp(a) measurements.
• Educate the public, physicians, regulatory agencies, and funding agencies on the role of Lp(a) in CVD and CAVD.
• Develop evidence-based management plans for patients.
44
✓
✓

Specific Research Priorities and Recommendations
• To fully define mechanisms of Lp(a) synthesis, assembly, clearance and other influences on circulating levels.
• To understand the mechanisms underpinning Lp(a) and its associated oxidized phospholipids in mediating risk of CVD and aortic stenosis
• To develop a globally standardized measurement of Lp(a) applicable to commercial laboratories and to define population risk among different ethnic/racial groups
• To understand the mechanisms through which therapeutic regimens affect Lp(a) levels
• Focused populations at risk for CVD with high Lp(a) requiring special research emphasis (FH, CAVD, ESRD, high thrombosis risk, refractory angina, lipoprotein apheresis, children with CVA)
45
✓
✓

New Lp(a) ICD-10 codes
New ICD-10 codes effective Oct. 2018
E78.41 Elevated lipoprotein(a)
Z83.430 Family history of elevated lipoprotein(a)
46

What are the mechanisms through which Lpa) mediates CVD and CAVS?
Tsimikas JACC 2017;69:692-711 47

OxPL-apoB Levels and CVD Outcomes CAD, PAD, CVA
Byun et al JACC 2015;65:1286-95
2,40
1,66
2,55
1,50
2,58
1,90
1,45
4,40
0,0
1,0
2,0
3,0
4,0
5,0
Bruneck EPIC-Norfolk NHS HPFS MAYO TNT Atorva10 mg
TNT Atorva80 mg
SPARCL
OxP
L-a
po
B, O
R/H
R
Study
Hazard/Odds ratio for primary endpoint,
highest tertile/quartile comp
No Prior CVD Prior CVD
48

Association of Aortic stenosis and Lp(a)-OxPL Six Recent Studies
49

Association of Aortic Stenosis and Lp(a)-OxPL Seven Recent Studies
50

Elevated Lp(a) and OxPL-apoB Predict Progression of CAVS and
Need for AVR
Potential explanation of the failure of statins in aortic stenosis
51J Am Coll Cardiol 2015;66:1236-46

Progression of aortic stenosis according to Lp(a) and
OxPL levels
Capoulade et al JAMA Cardiol 2018;3:1212-17 52

Statins increase Lp(a) levels UCSD Lp(a) data from clinical trials in 5256 patients
Tsimikas et al Eur Heart J 2019
53

In whom should Lp(a) be measured?
• Since it’s a genetic risk factor whose levels change minimally over a lifetime, everyone should have an Lp(a) measured when they get their first lipid panel.mIt is likely cost-effective is test is ~$50. If levels are low (in >75% of patients) it never has to be checked again
• UCSD EPIC ordering options
• “lipid panel”• ’lipid panel with Lp(a)”
• Intermediate or high risk• Premature CVD• FH• Family history• Non-responsive to statins• Recurrent events≥3% 10-year
risk of fatal CVD• ≥10% 10-year risk of
fatal/nonfatal CHD
My opinion Guidelines
54

UCSD is a Center of Excellence in Research and Patient Care in Lp(a)Created World’s First Dedicated “Lp(a) Clinic” in 2014
5
5
Tsimikas Vascular Medicine Clinic
(n=150)
Physician members of the UCSD Lp(a) Clinic:Michael Wilkinson, MD
Calvin Yeang, MD
Joseph Witztum, MD
Sotirios Tsimikas, MD
UCSD Hospitals 2010-2015
55

Acknowledgments
56
UCSD
Calvin YeangXiaohong Yang
Kim WeldyPhuong Miu
Joseph Witztum
Ionis
Nick VineyRosanne Crooke
Mark GrahamMichelle Fugett
Joseph TamiPatricia Wu
Lynnetta WattsRichard GearyStanley Crooke
Ionis/Akcea
Ewa ProkopczukJonathan Guerriero
Chelsey JansenPhil Piscitelli
Victoria BartlettLouis O’Dea
Collaborators
Peter WilleitSantica Marcovina
Erik StroesJ. C. van CapelleveenF. M. Van der WalkRomain Capoulade
Patrick MoriartyPhil Pibarot
Pia KamstrupBorge Nordestgaard
Novartis
Anastasia LesogorYoung-Min Kim
Tom Thuren