aortic emergencies moritz haager sept 19, 2002. objectives define aortic dissection + aaa, and why...
TRANSCRIPT
Aortic Emergencies
Moritz HaagerSept 19, 2002

Objectives
• Define aortic dissection + AAA, and why its important
• Review pathophysiology and classification
• Discuss diagnostic modalities• Discuss management options

What is Dissection?
• Aortic dissection dissecting aortic aneurysm
• “longitudinal cleavage of the aortic media created by a dissecting column of blood”Rosen’s Emergency Medicine

Relevance
• Underreported• Incidence 5-10/ 1,000,000 and rising• Mortality 1-2%/hour (33% in 1st 24 hrs)• High rate of misdiagnosis ~28%• One study suggests EP’s suspect AD in
<50% of cases » Sullivan et al. Am J Emerg Med 18: 46-50. 2000
• Variable presentation including MI• Lack of suspicion for AD is #1 cause of
misdiagnosis

Sad but true..• 42 yo M presents c/o pain in R groin + leg• Also atypical CP/back pain preceding• Sniffed coke ~2 hrs ago + popped viagra ~1
hr ago at a “sex party”• PMHx: HTN, smoker• O/E: 92/ 160/100 /16; pale, diaphoretic,
unwell looking; 2/6 SEM at apex, clear lungs, soft non-tender belly w/ Ø masses, R foot/ leg cool w/ Ø femoral, popliteal or tibial pulses
• ECG: isolated ventricular beats• B/W: normal except +ve tox for cocaine• CT: Stanford Type B dissection• TEE: 3.5 cm intimal tear, Ø AR
Famularo et al. J Emerg Med 21(1): 78-9. 2001
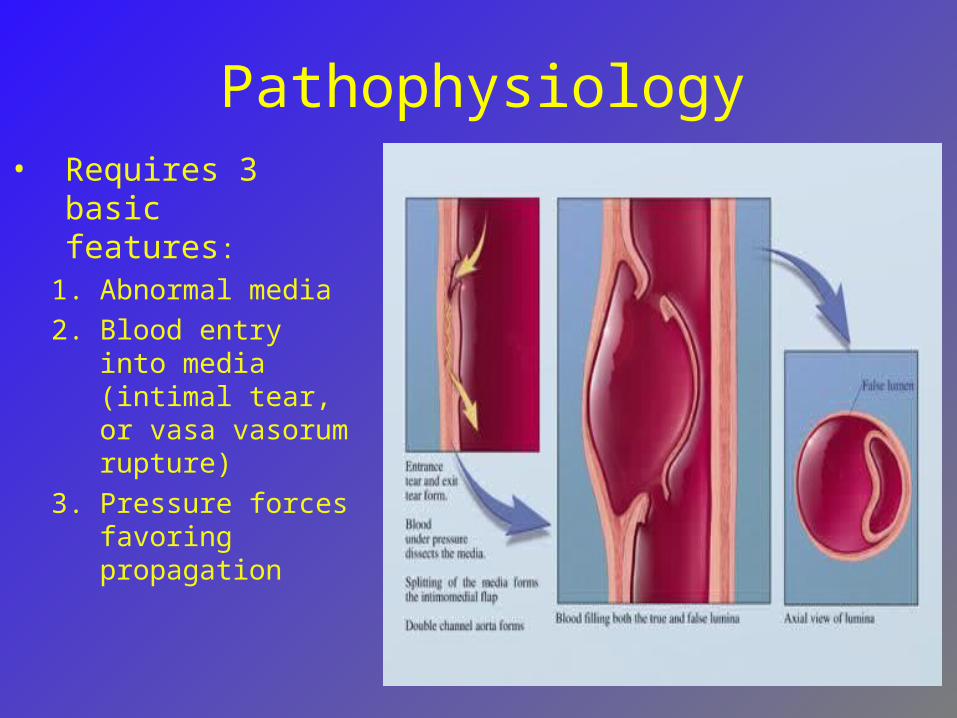
Pathophysiology• Requires 3
basic features:
1. Abnormal media
2. Blood entry into media (intimal tear, or vasa vasorum rupture)
3. Pressure forces favoring propagation

Pathophysiology• Peripheral complications: expanding
hematoma dissects into, or compresses branches, or fistulizes into adj. structures
– Cerebral CVA, syncope, – Spinal Neuro deficits– Cardiac MI, tamponade– Respiratory Hemoptysis, pleural effusion– GI Hematemesis, dysphagia, mesenteric
ischemia– Renal ARF, HT N– Limbs Extremity ischemia

• Intimal tears occur in 96% of all AD cases
• Felt to occur 2o to shearing forces and hemodynamic stresses
• Propagation factors:– Degree of HTN– Slope of pulse wave
(dP/dT)
• Spontaneous cure = rupture back into true lumen (rare)
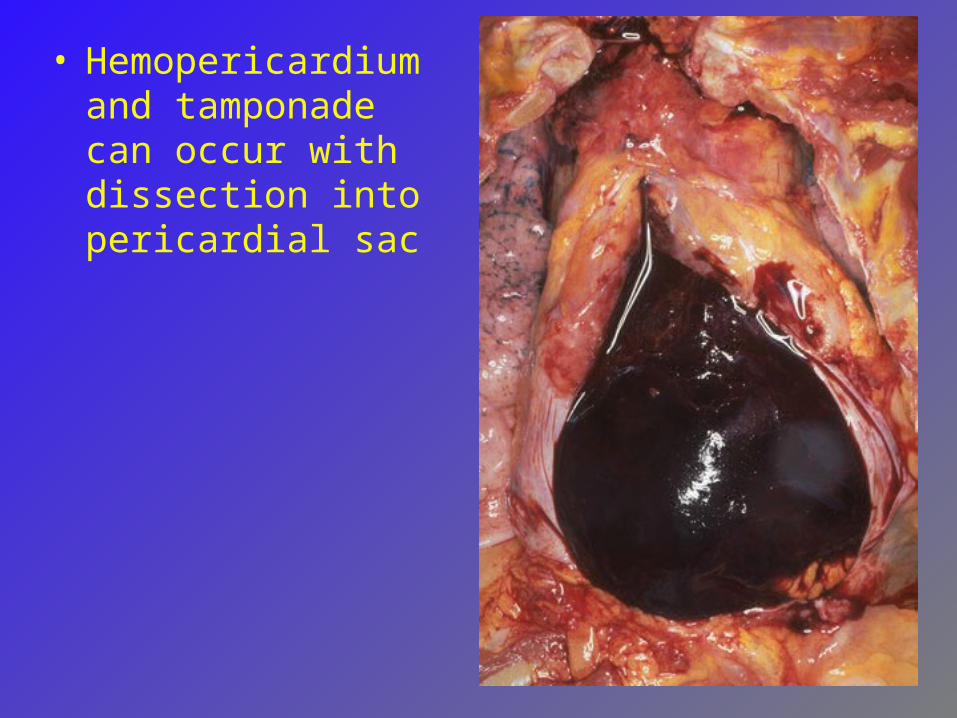
• Hemopericardium and tamponade can occur with dissection into pericardial sac

-Coronary artery involvement in ~1% presents as MI-0.1-0.2% of MI’s are complicated by admin of lytics in setting of AD
Clinical Presentation
• Sudden, severe chest pain (~76-90%)• Migratory CP is highly specific (~71%)• Back pain (~53%), abd pain• Other Sx depending on site of
involvement– Syncope (~9%)– Neuro Sx (~6-13%)– GI Sx– Resp Sx
• Can be painless in up to 15% (chronic)Moore et al. Am J Card. 89:1235-1238 2002Hals. Emerg Med Reports 2000

Risk Factors for AD• Hypertension (60-90%)• Age 50-70 yo• Male (3:1)• CTD’s (Marfans ~5%, Ehlers-Danlos)• Turners, Coarctation, Ebstein’s Anomaly• Congenital bi-/tricuspid AV• Family Hx or previous dissection• Cocaine, metamphetamine• Iatrogenic• Trauma
Hals. Emerg Med Reports 2000

Classification
• DeBakey:– Type I: involve ascending aorta, arch, and
descending aorta– Type II: ascending aorta proximal to L
subclavian artery– Type IIIa: descending aorta only; above
diaphragm only– Type IIIb: descending aorta only;
extension below diaphragm
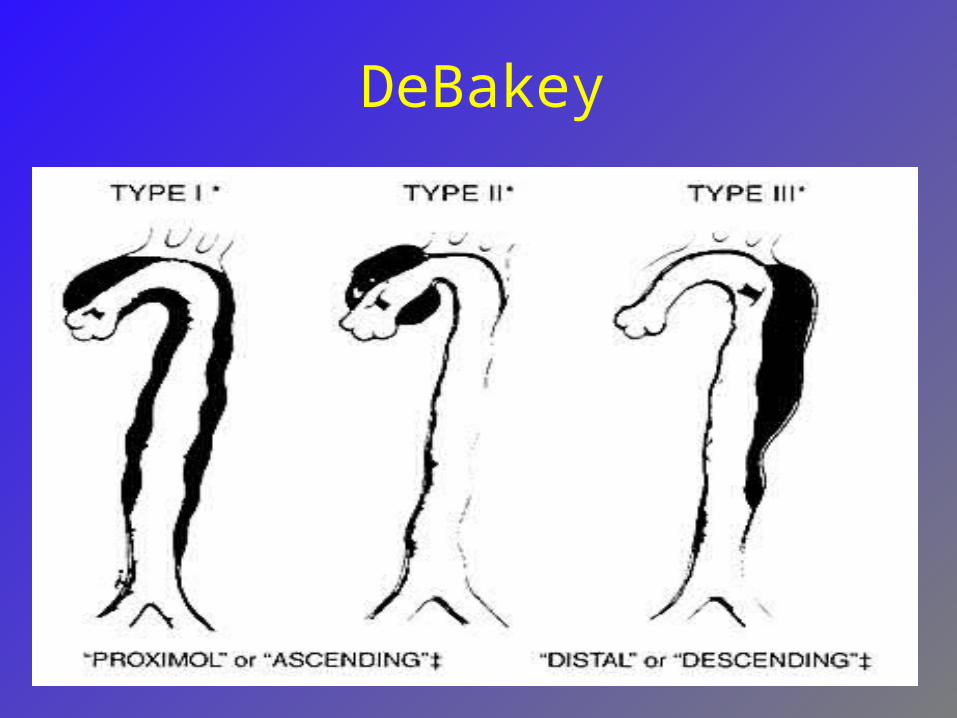
DeBakey

Stanford
• Type A: involvement of ascending aorta
• Type B: no involvement of ascending aorta
• ~62.5% of pts w/ AD have a Type A• Involvement of ascending aorta is of
prognostic and therapeutic importance

Classification

How to diagnose AD
• Clinical suspicion above all• 3 clinical variables shown to be useful:
• Aortic pain (immediate onset, tearing, ripping)• Mediastinal widening / aortic widening on CXR• Pulse or BP differentials
– Likelihood of AD:• Ø of above variables 7% risk of AD• Pain or widening alone 31 + 39% risk of AD respectively• > 2 variables or isolated BP / pulse diff > 83% risk of AD
» Von Kodolitsch et al. Arch Intern Med. 160: 2977-82. 2000
• Diagnostic modalities• ECG, CXR, CT, TEE, Angiogram, MRI

ECG findings in AD
• ~85% will be abnormal• LVH • Non-specific ST-T wave changes• MI (RCA most common)• Bottom line:
– not sensitive or specific– beware thrombolysis until AD excluded

CXR findings in AD• 80-90% will be abnormal• Most findings non-specific:
– Mediastinal widening (~59-75%)– Calcium sign (pathognomonic)– Double density aorta– Obliteration of aortic knuckle– Loss of PA window– Tracheal deviation to right– Depressed left main stem bronchus– New left pleural effusion– Apical cap– Size disparity of ascending + descending aorta


TEE• Rosen: 98% sensitive, 77% specific• Moore et al: 88% sensitive• 1st test in Europe and Japan• Advantages:
– Can differentiate Type A + B dissections– Rapid, can be done at bedside– No contrast or radiation– Can detect AR and pericardial effusion
• Disadvantages– Availability, operator dependence– Limited info on distal aorta
Moore et al. Am J Card. 89:1235-1238. 2002


CT scanning
• Dynamic helical CT nearly 100% sensitive and specific (dye) (Moore et al: 93% sens)
• Advantages:– Availability, can differentiate Type A + B – Able to identify sealed-off false lumens– Able to identify other pathology (eg PE)
• Disadvantages:– Dye reactions (1/10,000 fatal)– No info on AV function or intimal tear location– No info about extension into other arteries



Angiography
• 81-87% sensitive, 96% specific• Previous gold standard• Advantages:
– Anatomical delineation of aortic tree– Ability to demonstrate AR– Can differentiate Type A + B dissections
• Disadvantages:– False –ves due to false lumen thrombosis– Invasive, time consuming, expensive


MRI
• Near 100% sensitivity and specificity• No role in critical pts but good for serial
follow-up• Advantages:
– Excellent anatomical delineation, info on AR, intimal tear location, type and extent of AD
• Disadvantages:– Time-consuming– Unable to monitor pt


Intravascular U/S
• New technique – intravascular U/S probe
• Currently evolving uses include– Identification of unstable plaques in CAD– Diagnostic and therapeutic use in AD
• 3-D imaging of aorta + surrounding structures• Guidance of intra-vascular stent placement –
less invasive procedure than classic surgery• Fenestration of intimal flap
– Not available at most centers at this timeChavan et al. Circulation 96: 2124-2127. 1997

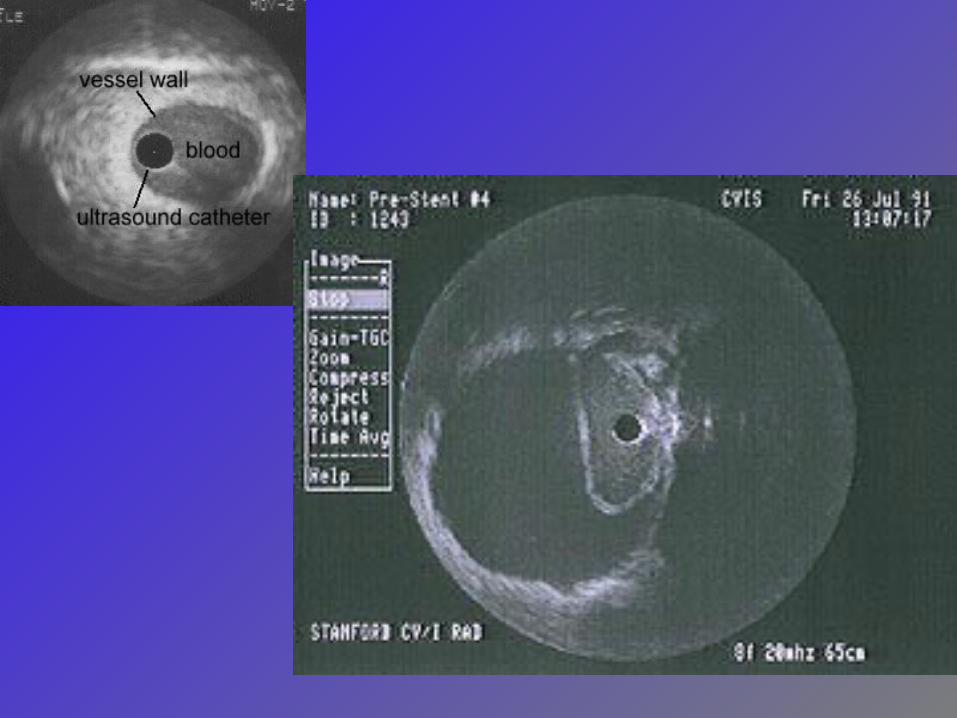

3-D IVUS
So what test do I order 1st?
• Moore et al: CT is initial test of choice followed by TEE to clarify Dx or better delineate surrounding anatomy + AR
» Moore et al. Am J Card. 89:1235-1238. 2002
• In Calgary, TEE is considered highly accurate and available, and should be considered a 1st line test
» Peter Giannacarro, personal communication
Can we predict outcomes?
• Pulse deficit is independent predictor of 5-day mortality RR 2.73, 95% CI 1.7-4.4
• Stat sig trend of increasing mortality with increasing number of pulse deficits
– Bosssone et al. Am J Card 89: 851-855. 2002
• Mortality predictors:– Age > 70 (OR 1.7, 95% CI 1.05-2.77)– Abrupt onset CP (OR 2.6, 95% CI 1.22-5.54)– Hypotension/shock/tamponade (OR 2.97, 95% CI 1.25-
3.29)– ARF (OR 1.77; 95% CI 1.80-12.6)– Pulse deficit (OR 2.03; 95% CI 1.25-3.29)– Abnormal ECG (OR 1.77; 95% CI 1.06-2.95)
– Rajendra et al. Circulation. 105: 200-206. 2002

Management
• ABC’s and then 2 basic principles:– Control dP/dT
• 1st control your HR, then lower the pressure
– Surgery if indicated• All Type A dissections need urgent OR
• Controversies + New Ideas– Surgery for Type B dissections– Intravascular repair
Medical Tx• Control HR
– IV BB’s – aim for HR 60-80 bpm• Propranolol 1mg IVP q5min• Esmolol 500 mcg/kg bolus, then titrate
infusion 50-200 mcg/kg/min• Metoprolol 5 mg IVP q5min • Diltiazem 20 mg IV bolus, then 5-15 mg/hr if
BB contraindicated (heart block, asthma, COPD, CHF)

Medical Tx
• Control BP •aim for BP 100-120 mmHg sys or min BP
req’d to maintain end-organ perfusion•Nitroprusside 0.5 mcg/kg/min – titrate up
prn
• Monotherapy•Labetalol 20 mg IVP, then 20-80 mg q5-
10 min until in target HR, then 1-2 mg/hr
Surgical Tx
• Indicated for:– All Type A dissections– Type B w/ complications:
• Aortic rupture• Severe distal ischemia• Refractory HTN• Progressive dissection despite Tx• Intractable pain
• Mortality for Type A repair is ~7-12%• Co-morbidities increase mortality• 5 yr survival is 77% Type A + 88% Type B


Why not operate on all?
• Medical Tx of Type B has ~20% mortality
• Surgical Tx of Type B has 10-15% mortality, and 3.5-36% risk of paraplegia
• This may be changing with advent of endovascular repair, fenestration procedures, and IVUS.

New Surgical Methods
• IVUS-guided fenestration of intimal flap» Chavan et al. Circulation 96: 2124-2127. 1997
• Intravascular stent placement– Cover intimal flap reducing flow to false
lumen clotting of false lumen– 1.6 hrs vs 8 hrs for conventional Sx– One recent series of 70 Type B AD pts tx’d
w/ stent-grafts reported 92.9% success and 9.6% all cause mortality at 29 months
» Palma et al. Ann Thorac Surg 73: 138-42. 2002


AAA: some facts
• Incidence rising: 2% >65 yo• 9 men for every 1 female• Most have no antecedent Sx • 50-80% mortality rate• Misdiagnosed in 30-60% of cases
Definitions
• Aneurysm = irreversible localized dilatation of an artery to > 1.5 original diameter (~3cm in abd aorta)
• Types of aneurysms:– True = involves intima, media, and
adventitia– Pseudoaneurysm = only intact + bulging
layer is adventita– Inflammatory aneurysm = surrounding
fibrosis and adhesions


Pseudoaneurysm
• Damged intima + media
• Adventitia prevents rupture

Anatomy1. Aorta2. Inf phrenic3. R hepatic4. Common
hepatic5. Gastroduodenal6. Inf pancreatico-
duodenal7. L common iliac8. L renal9. Splenic10.L gastric

Anatomy

Risk Factors for AAA
• Age 50-70• Male (9:1)• White• Atherosclerosis• HTN• Smoking• Family Hx• Loss of elastin / CTD’s (Marfans)

Clinical presentation
• Unruptured vs. Ruptured– Unruptured:
• Vague abd pain / back pain / pulsations / fullness
• SMA syndrome (wt loss, vomiting)• Renal colic, radicular Sx, embolic phenomena
– Ruptured:• Classic: abd pain, pulsatile mass, hypotension• Atypical:
– Back or flank pain + hematuria– LLQ pain + GI bleeding– Sx of high-output failure
Physical Findings
• Pulsatile abd mass– Palpate each sid of aorta; if >2.5 cm w/u– PPV ~43%
• Other findings neither sensitive or specific

How do to Diagnose AAA
• Clinical suspicion• Diagnostic imaging
– Abd U/S– CT abd– Angiography– MRI
• What test, when, and for whom?

Plain Films• Initial screening• Findings in 60-75%
– Calcified wall– Paravertebral soft
tissue mass– Loss of psoas
shadow– Loss of renal
silhouette– Erosion of vertebral
bodies
• Negative study does NOT exclude Dx

Ultrasound
• Test of choice, esp in unstable pts• Advantages:
– 100% sensitive + specific for AAA– Rapid (~5 min vs. ~80 min for CT) – can be done at bedside– non-invasive
• Disadvantages– Poor at identifying rupture – Technically difficult in obesity / bowel gas


Computed Tomography
• 100% sensitive + specific for AAA• Advantages
– Able to detect ruptures– Obesity + bowel gas don’t limit study– Surrounding anatomy
• Disadvantages– Unstable pts– Time– IV contrast (can do without)– Not 100% sensitive for rupture



Angiography
• NOT a ED screening tool• Tends to underestimate AAA size• May aid in planning of surgery (e.g.
renal a. stenosis)• Helical CT can produce 3-D images +
may replace angiography


MRI
• Not useful in acute setting• Excellent anatomical delineation• Used primarily prior to elective repair

ED Management
• Depends on context:– Incidental Dx of AAA– Ruptured AAA in “stable” pt– Unstable pt with ruptured AAA
• Basic principles:– ABC’s– Surgical referral for all
• Elective surgery has ~5% mortality• Emergent surgery in non-ruptured AAA ~25%
mortality• Emergent surgery for RAAA ~50% mortality
• Controversies:– Role of volume resuscitation

Fluid Resuscitation
• Evidence in penetrating trauma for forgoing aggressive volume resusitation
– Bickell et al. N Eng J Med 1994 (331): 1105-1109
• Fluids can cause dilutional coagulopathy• Ø studies compare ED resus strategies in
AAA• Recent Cochrane Review: no evidence to
support any specific fluid resus strategy in setting of traumatic hypovolemic shock
» Kwan et al. Coch Data Sys Rev. 2002
• Recommendations are to aim for min BP necessary to maintain end-organ perfusion + use blood products early

Natural Hx
• Formation enlargement rupture DEATH
• How can we intervene?– Primary prevention– Early management + observation– Elective surgery– Emergency surgery

Risk of Rupture
• Risk factors– Size of AAA– COPD– HTN– smoking
• What is the risk of rupture?– <4 cm: ~1-1.2%– 4-5 cm: 1-3%
• One study suggests surgeons estimate risk of rupture >2x published risk
» Lederle. Arch Intern Med 156: 1007-009. 1996

Current Surgical Indications
• All symptomatic aneurysms• All saccular aneurysms• Poor risk pt w/ AAA >6 cm• Good risk pt w/ AAA >5 cm• Young, good risk pt w/ AAA 4-5 cm
» Sternbergh et al. Surg Clin NA 78: 827-834. 1998
Elective repair of small AAA’s
• 5 yr survival ~76% vs ~30% for emergent
• 2 recent RCT’s suggest no survival benefit from immediate surgery for AAA’s 4-5.4 cm– RR 1.21; 95% CI 0.95-1.54
» Lederle et al. N Eng J Med 346: 1437-44. 2002
– RR 0.94; 95% CI 0.75-1.17» UK Small Aneurysm Trial Participants. Lancet
352: 1649-55. 1998


Traditional vs Endovascular• ELG repair advantages:
– Less invasive– Dec’d blood loss, procedure times, ICU stays,
hospitalization time, and recovery time– Dec’d morbidity but not mortality
• Disadvantages– Expense, limited long-term experience but may
be less durable than conventional repair
• Utility– Clear morbidity advantage in elderly, high risk
pts demonstrated in recent observational study» Sicard et al. Ann Surg 234: 427-37. 2001
– No good evidence to support use in small AAA’s or younger pts
» Brewster. Surgery 131: 363-7. 2002

Late complications• Graft infection
– Early or late (up to years after)– ~30-50% mortality– Staphylococcus epidermidis– Present w/ sepsis +/- AEF– Tx is abx, graft excision, + bypass
• Aorto-enteric fistula (AEF)– Can form anywhere (usually duodenum)– Acute or chronic GIB– Tx is graft replacement
Questions?1 hour boy!!..all you had to do is talk for 1 lousy hour! I could be drunk by now!!