appendix a, part 2 - home - axon resourcing · 7 – appendix a, part 2 . 2 1. ... (cc, nrsr,...
TRANSCRIPT
DRAFT Annual Plan 2014/2015
Principal Objectives & KPI’s
7 – Appendix A, part 2
2
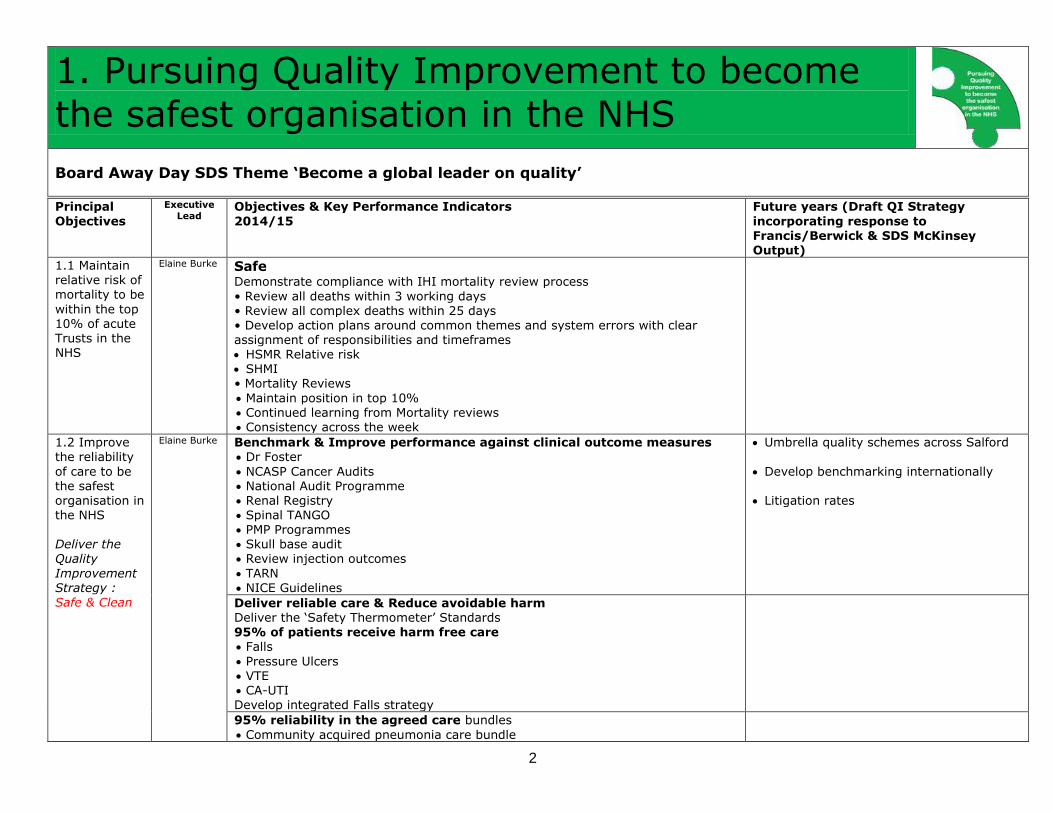
1. Pursuing Quality Improvement to become the safest organisation in the NHS
Board Away Day SDS Theme ‘Become a global leader on quality’
Principal
Objectives
Executive
Lead Objectives & Key Performance Indicators
2014/15
Future years (Draft QI Strategy
incorporating response to Francis/Berwick & SDS McKinsey Output)
1.1 Maintain relative risk of mortality to be
within the top 10% of acute Trusts in the NHS
Elaine Burke Safe
Demonstrate compliance with IHI mortality review process
• Review all deaths within 3 working days • Review all complex deaths within 25 days • Develop action plans around common themes and system errors with clear assignment of responsibilities and timeframes HSMR Relative risk SHMI • Mortality Reviews
Maintain position in top 10% Continued learning from Mortality reviews Consistency across the week
1.2 Improve
the reliability
of care to be the safest organisation in the NHS Deliver the Quality
Improvement Strategy : Safe & Clean
Elaine Burke Benchmark & Improve performance against clinical outcome measures
Dr Foster
NCASP Cancer Audits National Audit Programme Renal Registry Spinal TANGO PMP Programmes Skull base audit Review injection outcomes
TARN NICE Guidelines
Umbrella quality schemes across Salford
Develop benchmarking internationally
Litigation rates
Deliver reliable care & Reduce avoidable harm Deliver the ‘Safety Thermometer’ Standards
95% of patients receive harm free care Falls
Pressure Ulcers VTE CA-UTI Develop integrated Falls strategy
95% reliability in the agreed care bundles
Community acquired pneumonia care bundle

3
Principal Objectives
Executive Lead
Objectives & Key Performance Indicators 2014/15
Future years (Draft QI Strategy incorporating response to Francis/Berwick & SDS McKinsey
Output)
Heart failure care bundle Hip and knee care bundle
Myocardial infarction care bundle AQ bundles (Stroke/SINAP/Sentinel) Intentional rounding Structured ward rounds Infection bundles Sepsis 6
Surgical site infection Dementia & Delirium
Harm Free Collaboratives
Sepsis Collaborative Dementia Collaborative
Theatres WHO Checklist/5 steps to safer surgery Learning Board Days Since Adverse Incidents Briefing using OP SAFE Acronym Governance Away Days
Our Culture Our Commitment Pledge
Medication safety Prescribing error rate
EQUIP Audit
Reduce Readmissions
Review pathways to avoid readmission Outpatient f/u clinics Nurse f/u
Medication f/u texts
Consistently high standards of care across 7 days
• National standards Safety at night • Minimum staff levels Develop business cases to support appropriate 7 day cover Robust cover for Trauma lists Weekend Angiography
ACM in-reach into A&E
Outreach Physician on ANU/C1 Staff staffing levels – hospital wards, Intermediate care, Joint arrangements with CMFT for ENT Consultant cover
Leadership and culture (Doctor involvement, duty of candour, communication and staffing)
Focus on community (Community nursing, collaboration with GP’s and integration)
Capability and measurement (Analytics, real time data, Human Factors, TICKLE, Consultant level data, demand and capacity planning)
Development of learning systems (Listening to & supporting staff,

4
Principal Objectives
Executive Lead
Objectives & Key Performance Indicators 2014/15
Future years (Draft QI Strategy incorporating response to Francis/Berwick & SDS McKinsey
Output)
integrated governance, coaching, prospective thinking)
Collaborative projects supporting key themes
Demonstrate compliance with the ‘Salford Standard’
Patients to be seen & clerked <1hr in A&E & PANDA. All emergency patients to be reviewed by a Consultant <12 hrs of admission Operational Policies (CC, Nrsr, Anaesthesia, Surgery) Radiology specials staff, resident with further on-call tier
Train new junior cadre in EWS, safe handover, end of life care including care of the dying pathway and ceilings of care
Unified clerking document ED/EAU/SAU & agreed surgical handover document Neurosurgery to lead/deliver emergency list Mandatory PTWR document utilisation
Work towards achieving compliance with the Greater Manchester Standards (2012/3) for Emergency Surgical care (including NCEPOD) • Emergency surgical assessments& surgical opinion 24/7
• High risk patients are discussed with the consultants • Consultant Surgeon & Anaesthetic presence in theatre • medical patients have access to surgical opinion 24/7 • Emergency access to theatre as a priority over elective cases
Critical care input is available 24/7 Work to close gaps – 63% compliance at self-assessment Review surgical on-call arrangements
Radiology • Access to appropriately staffed 24/7 plain films, ultrasound, CT & MRI. • Access in emergency to plain film, ultrasound, CT & MRI <30mins • Where immediate treatment plan requires it images to be reported <30mins • Access to interventional radiology 24/7 Pathology
Access to Consultant led Pathology (all subspecialtiess) 24/7
Work towards achieving the Major Trauma Standards • Consultant on call available <30 mins 24/7 • Resident middle grade 24/7
• Consultant in theatre<30mins 24/7 • Immediately available fully staffed & equipped theatre
• Demonstrable plans to make a 2nd theatre available • CT Head to Pelvis available within 60 mins • CT & plain film to be reported within 1 hour • Robust Image sharing/viewing capability with other centres • Adequately staffed lab 24/7 with blood/blood products • Regional Haemorrhage policy

5
Principal Objectives
Executive Lead
Objectives & Key Performance Indicators 2014/15
Future years (Draft QI Strategy incorporating response to Francis/Berwick & SDS McKinsey
Output)
• 24/7 access to Haematology advice • Rehabilitation Planning to start <24 hrs
• Rehabilitation Prescription for every patient • Support TARN submissions
Work towards achieving Specialist Commissioner Standards Intestinal Failure Pain Management
Cancer service specifications
Improve Pathways Trauma pathway Spinal Fracture Pathway
Spinal Trauma pathway to Southport POP (Preoperative optimisation/work up/assessment) CPEX bespoke facility
Post operative optimisation (right place/step down) ERAS Implement Acute abdomen pathway (Hot clinic & Virtual ward. Ring fenced
surgical assessment beds Move LA Cases out of theatre to injection centre/procedure room Implement pathways for Abscess/Lap chole, Appendix, Hernia
Admit regional referrals to neurosciences (within 48 hours) Timely access to Neurorehabiliation
Demonstrate rigorous Governance systems supporting safety for patients & staff Clinical Standards
NAAS/CAAS/TAAS Integrated governance – SUI/Risk/SIARC learning
Reduce Clinical Negligence, Litigation, Claims Reduce harmful events for staff Use the adverse incident/Serious incident reporting system to develop a culture
of reporting harm, with analysis of themes, undertaking root cause analysis and implementing action plans
Undertake Executive safety walk round Learning Boards
Benchmarking
Leadership and culture (Doctor involvement, duty of candour,
communication and staffing) Focus on community (Community nursing,
collaboration with GP’s and integration) Capability and measurement (Analytics,
real time data, Human Factors, TICKLE, Consultant level data, demand and capacity planning)
Development of learning systems (Listening to & supporting staff,
integrated governance, coaching, prospective thinking)
Collaborative projects supporting key
themes Safe use of technology/using
technology for safety
Use electronic health record to be continually building information about what treatments patients receive, to do further research and analysis on outcomes and adherence to best practice care

6
Principal Objectives
Executive Lead
Objectives & Key Performance Indicators 2014/15
Future years (Draft QI Strategy incorporating response to Francis/Berwick & SDS McKinsey
Output)
Clean Reduce healthcare acquired infections including surgical site infections MRSA c Diff MSSA E Coli CA-UTI
Central line bloodstream infections Sepsis Artificial Airway Associated Pneumonia EVD/Craniplasty/Shunt infections
Hip replacement infections Knee replacement infections Repair to neck of femur infections
Long bone infections
1.3 Improve patient experience to maintain indicators in
the top 20% nationally
Deliver the Quality Improvement
Strategy : Personal
Elaine Burke Personal Deliver the Patient Experience Strategy & continue the work of the Patient Experience collaborative Improve Engagement & Openness with Patients & Families
Maintain patient experience indicators in top 20% nationally • Patient Surveys • Patient Experience trackers • ‘Family & Friends’ Test
• Patient Reported Experience Measures (PREM's) • Hospital & Community Nursing Accreditation & Assessment System
Hospital empowering loved-ones & patients (HELP) End of life care Nutrition Intentional rounding • Complaints/PALs feedback • Shared decision making • What matters to you most (individualised care)
• Customer Care • Communicating with patients • Shadow coaching
Experience based design & co-design with patients Development of Care Partners Patient & Family shadowing
Collect “big data” on customers to understand their Learning from customer services in hotels/airlines
Build patient networks so that patients can access information/share information
Provide high quality efficient, patient-centred services by Engaging patients when designing new
services to understand what their true needs are Engaging patients in “co-
production”/expert patient programmes
Patient and carer experience (shared decision making, individualised care, coaching & customer care and communication)
Improve Patient Information Improve the availability of condition & procedure specific patient information

7
2. Safely reducing costs by £20m
Board Away Day SDS Theme : ‘Apply our distinctive quality-management capabilities to drive efficiency in our operational performance’
Principal Themes
Executive
Lead Objectives & Key Performance Indicators 2014/15
Future years (SDS McKinsey Output)
2.1 Improve
productivity and cost
improvements to improve margins
Ian
Moston Income
• Efficiency deliver contract activity & service developments Ensure Service Level Agreements, contracts & leases accurately reflect services
received / provided Delivery of 2013/14 outturn activity including planned growth
Delivery of CQUIN target to secure payments of £7.3m. (£1.4m National, £0.8m Gtr Mcr, £2.3m Local, £2.6m Specialist services)
Deliver of schemes associated with Better Care Fund schemes Delivery of service models to secure best practice tariff Secure income for service developments
Implementation of the Greater Manchester Hyper Acute Stroke model Neurorehabilitation beds
Capacity to meet the impact of Trafford A&E changes
Neuropsychology Urology capacity (Consultant appointment) Orthopaedic capacity (Foot & Ankle Consultant appointment)
Early supported discharge for stroke Increase activity/income in SRS, R&D, Homecare drugs/admin, Private Patients Neuro Legal Surgery
Income
Alliance agreement -2099 hospital admissions (48 beds) over
4 years NW sector Surgical centre Healthier Together reconfiguration CAREUK activity? SRS Income
Tariff Work with Commissioners in review of tariffs to reflect changing service models Impact of tariff changes
Pay & Price pressures CNST adjustments Tariff deflation (4%)
Impact of Education tariffs Renegotiate marginal tariff. Review GPOOH costs and income
Move away from Block contracts New currencies (Assessment/Virtual
wards/telemed/ Assessment tariffs Pain Management
Joint ventures
Costs - People • Review & benchmark workforce plans • Reduce premium workforce costs Safe Staffing levels Pay awards/costs Review of admin support
Costs Salary sacrifice? Change to shift patterns

8
Principal Themes
Executive Lead
Objectives & Key Performance Indicators 2014/15
Future years (SDS McKinsey Output)
Reduce WLI costs Reduce On Call costs Reduce us of Bank & agency/locum staff Review admin support in surgical Neurosciences
Job Planning (all staff groups) Benchmark all support functions and agree improvements
Costs – Productivity/flow • Theatre Improved Utilisation & turnaround times
Template redesign/increased throughput Move LA Cases out of theatre to injection centre/procedure room Beds Reduce Length of stay
Close beds Outpatients Telemedicine
Nurse led clinics Back Office Functions Partnering with Other NHS organisations Running Back Office Functions on behalf of Others Improve utilisation of Theatres, beds & Outpatients • Improve patient flow
• Improve profitability • Develop more collaborative working to identify cost reductions across Divisions,
within the Health Economy & between Trusts
Review back office functions/Outsourcing services
Increased throughput (~20%), reducing LOS, DC rates, theatre productivity
Increased staff & asset utilisation
Apply QI/lean/six sigma capability to productivity
Clinically appropriate care, reducing over investigation and over treatment
Improved community care efficiency (e.g., contacts/nurse)
Realise the benefits of the EPR system;
Patient Flow, A&E, Prescribing, Critical Care Optimisation, Community Services
Close 48 beds associated with integrated care over 4 years
Focus across full patient pathway, to reduce the current 180 medically fit
patients in hospital Rethink physical assets to streamline
flow
Consider how to use step down facilities LOS ward-by-ward/bed pools Introduce alternative models for
outpatient clinics e.g. phone/email
Develop group consultations
Costs – Non Pay • Reduce costs of procurement & Work with SBS Procurement Team Reduce accommodation costs Reduce Penalties associated with readmissions Improve pharmacy cost allocation
Increase remote dispensing Support early discharge TTO's
Reduce costs of Prosthetics/Implants/Procedure pack/SAP stapling, Hip/knee implants, trocars, Power tool consumables
Reduce Waste
Service Line Reporting Improve SLR methodology Implement trading accounts in Radiology, Pathology, AHP’s.

9
3. Supporting high performance and improvement
SDS Themes ‘Engage patients to improve quality and efficiency’
‘Staff are able to deliver the highest standards’
Principal Themes
Executive
Lead Objectives & Key Performance Indicators 2014/15
Future years (SDS McKinsey Output)
3.1 Improve Staff
Contribution to Corporate Objectives and Values
Paul
Renshaw Embed use of the Contribution Framework Agree how outcomes from the contribution framework are implemented
Agree a reward strategy for 2015/16 onwards Implement any revised bonus structures within the RemCo review Develop leaders to drive high performance Embed changes to Consultant CEA awards
Reward appropriate behaviours and allow adjustment of those not in line with core
values by Developing value based performance
management system Linking performance to pay and rewards?
3.2 Improve Employee Well
Being
Paul
Renshaw
Agree & implement a strategy that ensures we improve the health & wellbeing of our staff
Reduce sickness absence to below 3.6% by 2015/16 Reduce reported instances of bullying and harassment
3.3 Develop
Workforce Plans
Paul
Renshaw Agree an affordable 5 year workforce strategy to ensure we have an
sufficient staff with the right skills Safe staffing levels/7 day working
Succession planning Talent Management Develop our own staff including new & extended roles Develop rotational posts for staff to make posts more attractive Align Learning & development strategy & develop capability in specialist areas Reduce staff turnover Agree an ideal set of t&c’s for the future & consider a small trial of these.
Develop our own staff
Develop new roles Review T&C’s
Review shift patterns Develop joint working arrangements with
other organisations
3.4 Improve Culture & Engagement
Paul
Renshaw Implement the Communications Strategy Ensure communication is effective by checking coverage and understanding Support learning within and between organisations Apply for the Times Top 100 places to work
Improve the culture in theatres
3.5 Implement the Membership & Public Engagement Strategy
Paul
Renshaw • Representative Membership • Membership numbers • Engagement activity

10
4. Improving care & services through Integration & Collaboration
Board Away Day SDS Themes ‘Build a great integrated-care organisation, providing population-based care’
‘Lead reconfiguration of "core" acute services across the NW GM sector’ ‘Cement and grow our outstanding specialist services’
‘Work in true partnerships’
Principal Themes
Executive
Lead Objectives & Key Performance Indicators 2014/15
Future years (SDS McKinsey Output)
4.1 Develop Integrated Care in Salford
Simon
Neville Fully implement the new integrated care model for older people and associated contractual arrangements Promotion and increased use of Local Community Assets Establishment of Multi-Disciplinary Groups
Development of an Integrated Contact centre Embed model in Swinton & Eccles Roll out across the city Develop standards for care provision Develop the shared care record
Implement Alliance agreement Integrated working between ED/EAU/CHMP/GP’s & MDG’s
Full-service healthcare excellence for the local population, potentially taking greater control of primary care & maybe integrating with adjacent services such as
social care Improved population health outcomes
especially for people with LTCs Fewer admissions at front-end, better
discharge & LOS at back-end
Implement our "supply chain organisation" vision
Alliance agreement -2099 hospital admissions (48 beds) over 4 years
Explore different governance models e.g. ACO
Leveraging distinctive EPR platform to improve end-to-end patient journeys
Make use of technology to support patients and community clinicians to deliver care remote from hospital setting,
Developing a single Public Sector Asset
Strategy to rationalise & secure best value utilization
Improving coordination & integration of care for specific services e.g. cancer care, renal care, neurology
Develop single front door to hospital with full integration with GP & OOH services/frail elderly services & support to
Develop Integrated Care Pathways Develop Community Nursing Services Collaborate with GP’s Review Community Nursing Model IMC Social care pathways SEP integration
Integrated teams and FACS response CHMP and SRFT development of pathways Cardiac rehabilitation model Explore merging rehab care PR & cardiac rehabilitation Lung Cancer project
Anticoagulation
Home IV service for Bronchiectasis
Explore with partners further opportunities to integrate health and social care for the wider adult population Undertake a review of opportunities to integrate services across partner
organisations by June 2014

11
Principal Themes
Executive Lead
Objectives & Key Performance Indicators 2014/15
Future years (SDS McKinsey Output)
Work with Haelo to improve population health in Salford
nursing/care homes Expanding the acute physician triage
model Supporting paramedics to stream and manage patients in primary/community care settings Exploring use of community diagnostics access needs review
Position services to compete with CAREUK when contract expires
4.2 Integration &
Collaboration within the NW
Sector
Simon
Neville Surgery Provide Leadership to HT Programme/development of North West sector surgical
centre Develop service model/capacity for Emergency & complex surgery with Wigan &
Bolton & consider impact Pennine work Renal SRFT @ WWL Renal clinic Radiology Explore joint working in Radiology Sterile Services Drive improvements in provision of surgical equipment through the SLA
Provide Leadership to HT programme Greater patient care volumes to “load our
factory” – to: Fill the capacity that will be freed up by
greater efficiency in core operations Use scale to operate efficiently and at
high quality Support to partner organisations to
secure their futures, as vital local healthcare providers
4.3 Integration & Collaboration within Greater
Manchester &
beyond
Simon
Neville
Strengthen SRFT position in the provision of specialist services Functional neurosciences Neuro-rehabiliation Implement the hyper acute Stroke model
Spinal services
Renal Dialysis & outreach services Dermatology including Paediatric Dermatology, MOH’s surgery & SRFT at
Stockport Intestinal Failure including home TPN Metabolic Medicine Transitional services for adolescents Cancer surgery
Outreach outpatient services
Spinal centre for Greater Manchester Outreach spinal revision clinics Neuro-rehabilitation provider for Greater
Manchester
Dermatology centre for Greater
Manchester Specialist Pain centre for Greater
Manchester
Implement the Hyper Acute Stroke Model A&E Capacity Additional beds
Medical staffing model
Repatriation model
Open Oldham Dialysis Unit to open Q1 2014/2015
12
Principal Themes
Executive Lead
Objectives & Key Performance Indicators 2014/15
Future years (SDS McKinsey Output)
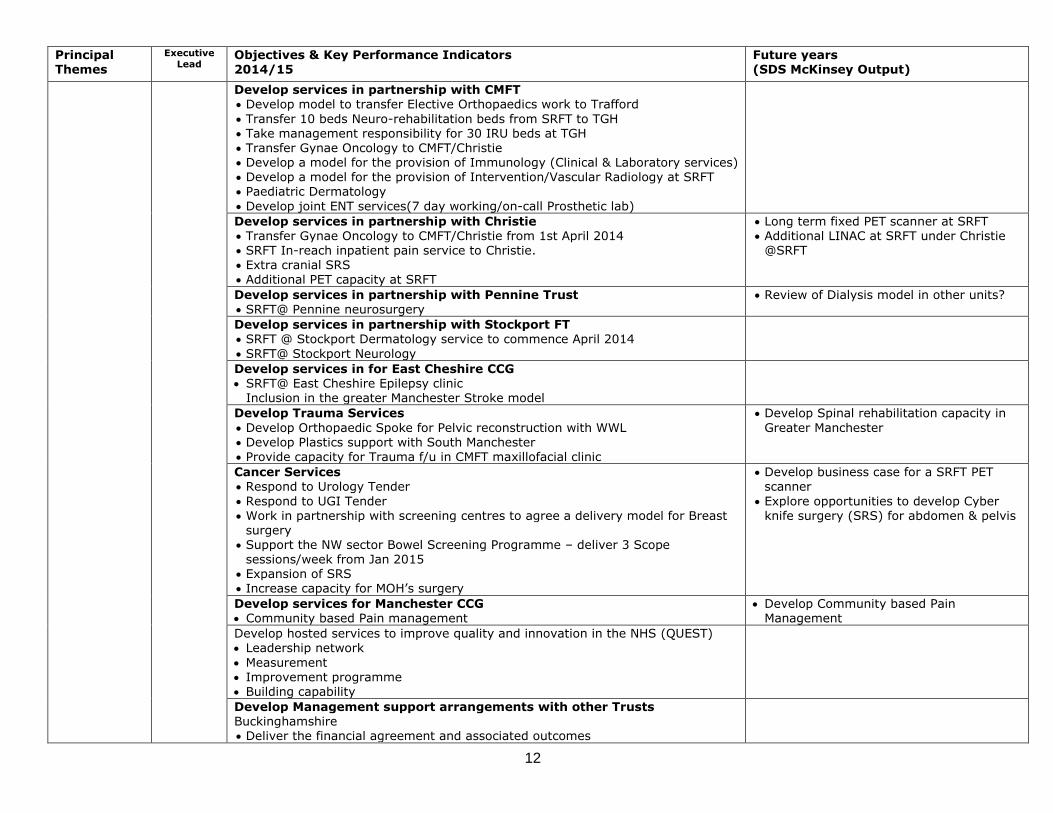
Develop services in partnership with CMFT Develop model to transfer Elective Orthopaedics work to Trafford
Transfer 10 beds Neuro-rehabilitation beds from SRFT to TGH Take management responsibility for 30 IRU beds at TGH Transfer Gynae Oncology to CMFT/Christie Develop a model for the provision of Immunology (Clinical & Laboratory services) Develop a model for the provision of Intervention/Vascular Radiology at SRFT Paediatric Dermatology
Develop joint ENT services(7 day working/on-call Prosthetic lab)
Develop services in partnership with Christie Transfer Gynae Oncology to CMFT/Christie from 1st April 2014 SRFT In-reach inpatient pain service to Christie.
Extra cranial SRS Additional PET capacity at SRFT
Long term fixed PET scanner at SRFT Additional LINAC at SRFT under Christie
@SRFT
Develop services in partnership with Pennine Trust SRFT@ Pennine neurosurgery
Review of Dialysis model in other units?
Develop services in partnership with Stockport FT SRFT @ Stockport Dermatology service to commence April 2014
SRFT@ Stockport Neurology
Develop services in for East Cheshire CCG SRFT@ East Cheshire Epilepsy clinic
Inclusion in the greater Manchester Stroke model
Develop Trauma Services
Develop Orthopaedic Spoke for Pelvic reconstruction with WWL Develop Plastics support with South Manchester
Provide capacity for Trauma f/u in CMFT maxillofacial clinic
Develop Spinal rehabilitation capacity in
Greater Manchester
Cancer Services Respond to Urology Tender
Respond to UGI Tender Work in partnership with screening centres to agree a delivery model for Breast
surgery Support the NW sector Bowel Screening Programme – deliver 3 Scope
sessions/week from Jan 2015 Expansion of SRS Increase capacity for MOH’s surgery
Develop business case for a SRFT PET scanner
Explore opportunities to develop Cyber knife surgery (SRS) for abdomen & pelvis
Develop services for Manchester CCG Community based Pain management
Develop Community based Pain Management
Develop hosted services to improve quality and innovation in the NHS (QUEST) Leadership network
Measurement Improvement programme Building capability
Develop Management support arrangements with other Trusts Buckinghamshire Deliver the financial agreement and associated outcomes

13
Principal Themes
Executive Lead
Objectives & Key Performance Indicators 2014/15
Future years (SDS McKinsey Output)
East Lancashire Explore the offering to East Lancashire to ensure mutual benefit
Explore the benefits of a managed network Explore specific opportunities in respect of back office functions
4.4 Service Development, Redesign &
Innovation
Simon
Neville Develop capacity planning methodology Inpatients Outpatients
Community services Support services
Run the hospital at 85% occupancy not 95%
Improved Logistics
Deliver the Outpatient Improvement Plan Reducing DNAs to less than 10%/text reminders Review of New to follow-up ratios
Roll out managed bookings
Improve customer service through the patient engagement collaborative Reduce waiting times in clinic Implement new Technology(Patient Portals/E-Consultation) Run Rapid Improvement Events
Patient portals Telemedice
Deliver the Radiology Strategy
Explore Joint Venture with Atlas Develop home reporting Develop Business case for 4th MR Scanner
Further MR capacity
Develop business cases for Service Developments Develop Renal self care models Develop Metabolic medicine satellite services (Newcastle/Bradford)
Expand Chronic Fatigue services
Expansion of Sleep services/Thoracic ultrasound Develop and expand GIPU Expand Weight Management services Fracture Clinic redesign Develop NIV model and service Palliative care cover to MDT’s
Increase cell salvage Develop Functional Neuropsychology Develop Neurophysiology capacity Develop Thermal threshold services in Neurophysiology Revisit the Elective Gynaecology Business case with Commissioners including
diagnostic cancer MDT. Move from El to OP service.
Collaborate with CCG to take on EPO Homecare patients Develop Homecare Services Develop Digital Moulding in Oral Surgery
Review setting of Orthodontic clinics Develop Psychology Oncology services/Support to the Chronic fatigue service
3 year plan to move into Community
CBT Clinics in the community
Develop service development/business planning process
Develop an innovation pipestream

14
5. Demonstrate Compliance with Mandatory
Standards
Principal Themes
Executive
Lead Objectives & Key Performance Indicators 2014/15
Future years
5.1 Achieve Clinical & Quality Standards
Pete
Turkington • NHSLA Standards
• Monitor Infection Control Quality Targets
• CQC Standards New inspection format
National CQUIN Standards Friends & Family Test
Safety Thermometer Dementia & delirium
Greater Manchester CQUIN Standards Patient Safety – lessons learned once Ambulatory Care Clinical effectiveness – deteriorating patients hospital
Clinical effectiveness – deteriorating patients community
Local CQUIN Standards • 7 day working Acute medicine & A&E 7 day working Surgical emergencies
Admission avoidance – surgical opinion Clinical communication Advanced care planning Acute – EPaCCS Advanced care planning Community – District Nurse checklist Paediatric Long term conditions – asthma/constipation MDT assessment for Children Medicines safety thermometer
Medicines reconciliation at discharge COPD Integrated care bundle Self care Fracture clinic
5.2 Financial Standards
Ian Moston • Monitor Financial rating • I&E
• Surplus
• EBITDA • Capital • CIP
5.3 IM&T Standards
Ian Moston • Information Governance Standards • Mandatory returns System availability Help desk responsiveness
ICD10/11 in 2015 New ISN/standards (Common CUI Aug 2015)
15
Principal Themes
Executive Lead
Objectives & Key Performance Indicators 2014/15
Future years
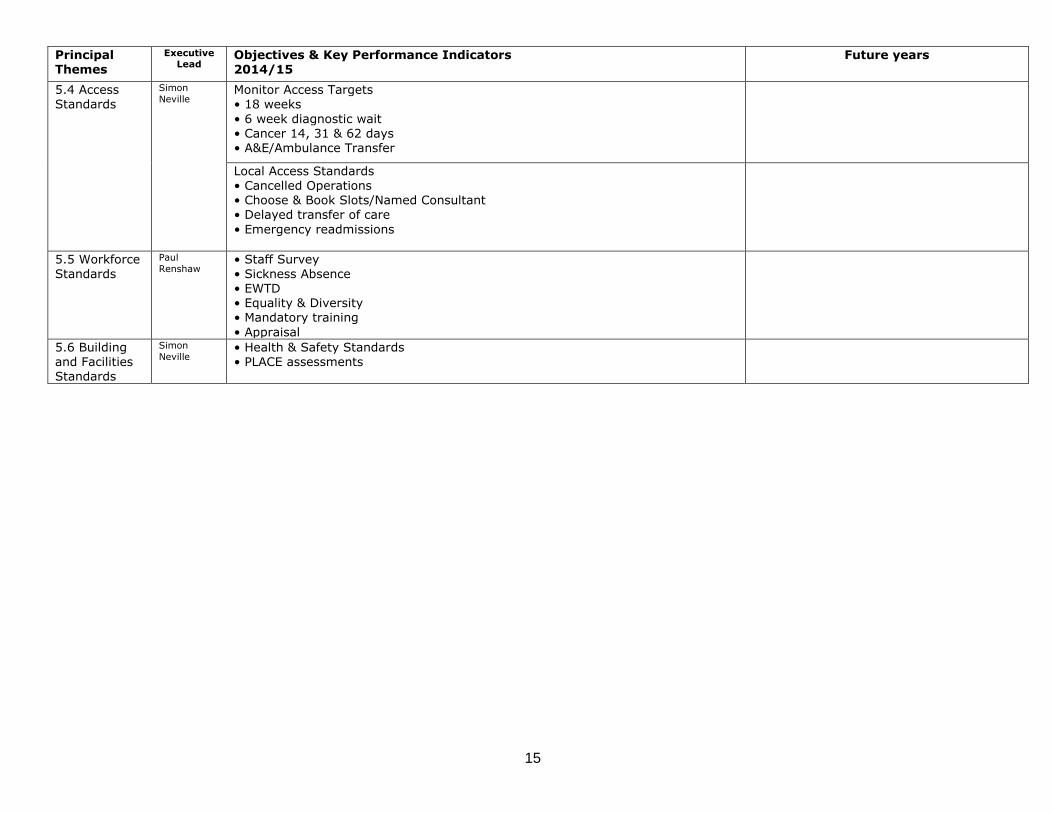
5.4 Access Standards
Simon
Neville Monitor Access Targets • 18 weeks
• 6 week diagnostic wait • Cancer 14, 31 & 62 days • A&E/Ambulance Transfer
Local Access Standards • Cancelled Operations • Choose & Book Slots/Named Consultant • Delayed transfer of care
• Emergency readmissions
5.5 Workforce
Standards
Paul
Renshaw • Staff Survey
• Sickness Absence • EWTD • Equality & Diversity • Mandatory training
• Appraisal
5.6 Building and Facilities Standards
Simon
Neville • Health & Safety Standards • PLACE assessments

16
6. Enabling Strategies Board Away Day SDS Themes
‘Use technology, IT and information to support all themes’
Principal Themes
Executive
Lead Objectives & Key Performance Indicators 2014/15
Future years
6.1 Deliver the Research &
Development Strategy
Define the remit and scope of the role of Research in Salford within MAHSC, AHSN, LCRN Develop a new strategy, building on ETHOS and 5 year plan for Salford R and D
in conjunction with our partners and in alignment to the plans for the Trust & CC Develop understanding of the value & contribution of R&D activity to the
organisation Conduct an impact assessment and evaluation of the public engagement and patient and public involvement in research activity.
Growth in R&D revenue (National Institute of Health Research, Grants, Research Capability Funding & Revenue generated from Commercial Clinical Trials.
Review Governance arrangements
Relocate R&D staff out of CSB Review supporting infrastructure Review supporting financial processes Dementia clinical trials partnership
Further strengthening reputation and proposition through more aggressive research agendas and attracting top
international clinical talent to Salford in chosen specialties
Continue to build world-class quality research and management agenda e.g. Register all patients on arrival for clinical trials and agreement to use data as for research purposes
Formalise reasearch links (eg Pain
Management)
6.2 Under &
Post Graduate Teaching
Pete
Turkington Deliver Undergraduate Medical Education
Deliver Post Graduate Medical Education Health Education North West new tariff funding model/Recharge spoke hospitals Develop multidisciplinary trauma teaching Demonstrate compliance with Deanery Standards
Deliver Student Nursing/clinical placements Fulfil the SHA Learning Contract Demonstrate transparency of funding streams into Divisional budgets
Develop new models of teaching to reflect
service reconfigurations
6.3 Deliver the Hospital Redevelopmen
t/Estates Strategy
Simon
Neville • Demolition of CSB & enabling schemes • Angiography – replacement of 2 rooms HCU – additional 9 beds to co-locate Cardiology beds
Fracture clinic 4th MR/Pad for van
Additional stroke beds Theatre Upgrade programme • Ward Upgrade programme Replacement of the Pharmacy Robot
Additional capacity (A&E/assessment/beds/theatres)
Hot/cold split.
CSB Replacement Helipad
Low tech procedure facility Colocation of services Theatre Upgrade programme Ward Upgrade Programme Swinton Gateway centre – transfer of
community services Work with asset management/design
partners to support leadership in

17
Principal Themes
Executive Lead
Objectives & Key Performance Indicators 2014/15
Future years
environmental space design and reconfiguration of assets to support better
patient flow SRFT PET scanner
6.4 Deliver the IM&T Strategy
Ian Moston Maintaining, Improving Infrastructure & System Upgrades PAS upgrade Upgrade DW/EPR (6.2/14.1)/Prodacapo Patient Flow Implementation
F&FT roll out Current EPR projects – A&E, Chemo, Community App, ED,CC,PP Optimise & consolidate current build ICM within SCM Upgrade & hot fix programme – all systems
Mobile phone project Data centre 2 Ascribe upgrade
DW hardware refresh and migration Medisec hardware upgrade Medisec roll out
Medisec hardware upgrade
Develop QI & Measurement Capability Develop data analysis/IT support
• Develop Real time & prospective quality & safety data • Consultant level data • Demand/capacity measures
Collect patient data to understand what patients appreciate
Better leverage patient data to help clinical decision making
Reduced variation across the organisation by continually reviewing efficiency and
quality metrics by Consultant/ward
Develop EPR & Clinical Systems EPR Prescribing Chemotherapy Stroke capture system • Diabetes Easycare Electronic measurement of 5 steps to safer surgery
EPR Anaesthetic optimisation EPR sunrise surgery module Explore molecular technology in
Microbiology Explore automation opportunities in
Histopathology Pathology results in offsite clinics
Digital slides - NHS Innovation pilot Pathology PAC's/Diagnostic Cloud
Outpatient Improvement • Outpatient appointment text reminder service
• Outpatient Self check in
Partner with other organizations to implement self-service IT system e.g.
patients to book appointments online/fill
in pre-appointments surveys Patients enter all their own data on past
medical history etc prior to consultation Develop self-management /reporting
systems
Supporting Back office Efficiencies
SMART workforce management system
18
Principal Themes
Executive Lead
Objectives & Key Performance Indicators 2014/15
Future years
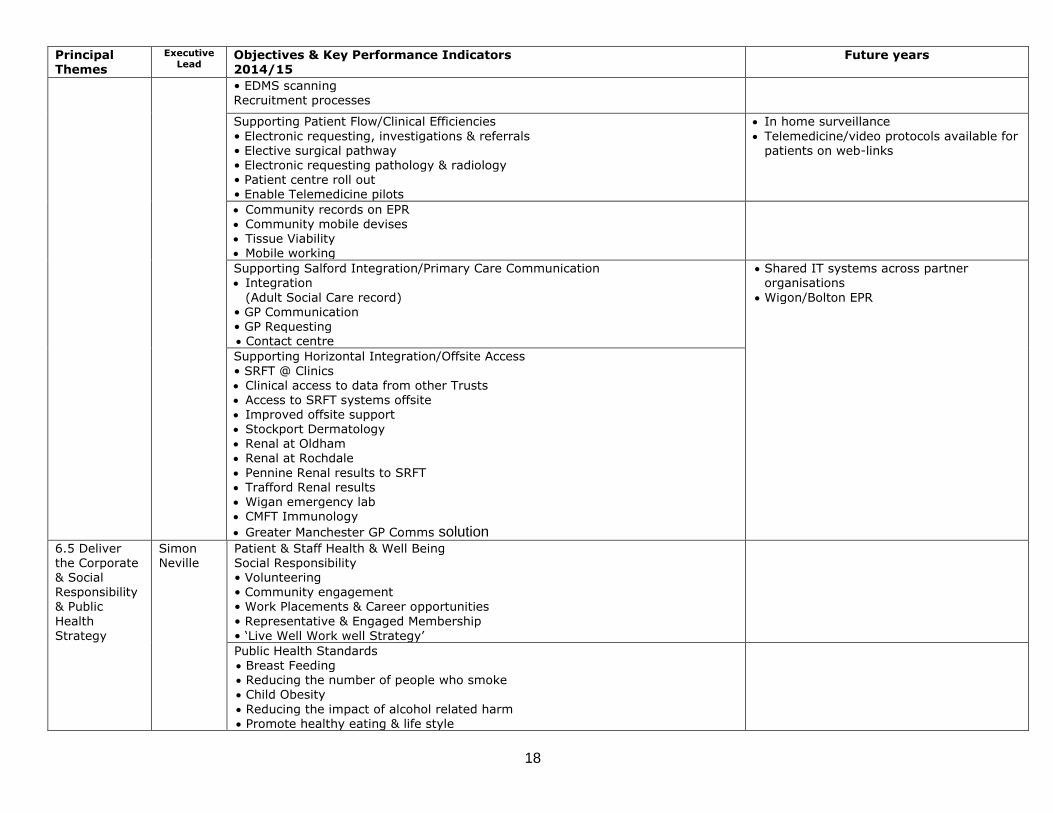
• EDMS scanning Recruitment processes
Supporting Patient Flow/Clinical Efficiencies
• Electronic requesting, investigations & referrals • Elective surgical pathway • Electronic requesting pathology & radiology • Patient centre roll out • Enable Telemedicine pilots
In home surveillance
Telemedicine/video protocols available for patients on web-links
Community records on EPR Community mobile devises Tissue Viability Mobile working
Supporting Salford Integration/Primary Care Communication Integration
(Adult Social Care record) • GP Communication • GP Requesting Contact centre
Shared IT systems across partner organisations
Wigon/Bolton EPR
Supporting Horizontal Integration/Offsite Access
• SRFT @ Clinics Clinical access to data from other Trusts Access to SRFT systems offsite Improved offsite support Stockport Dermatology
Renal at Oldham Renal at Rochdale
Pennine Renal results to SRFT Trafford Renal results Wigan emergency lab CMFT Immunology
Greater Manchester GP Comms solution
6.5 Deliver the Corporate & Social Responsibility & Public
Health
Strategy
Simon Neville
Patient & Staff Health & Well Being Social Responsibility • Volunteering • Community engagement • Work Placements & Career opportunities
• Representative & Engaged Membership
• ‘Live Well Work well Strategy’
Public Health Standards Breast Feeding Reducing the number of people who smoke Child Obesity
Reducing the impact of alcohol related harm Promote healthy eating & life style

19
Principal Themes
Executive Lead
Objectives & Key Performance Indicators 2014/15
Future years
Sustainability & Environmental Impact Minimise Waste/Increase recycling
• Minimise Energy Use • Minimise Carbon emissions • Green travel plan • Procurement – promote use of local goods/fair trade