application of the nhsn 2015 definitions - texas society ... · pdf fileapplication of the...
TRANSCRIPT

Application of the NHSN 2015
Definitions
Joan N. Hebden RN, MS, CIC
Clinical Program Manager – Infection Prevention
Wolters Kluwer Health

The pessimist complains about the wind; the optimist
expects it to change; the realist adjusts the sails.“
William Arthur Ward
American writer
Surveillance – A fast moving trajectory
1

Application of the NHSN Surveillance
Definitions
How well are we doing?
2

3
AJIC Case Studies
Am J Infect Control 40 (2012) S32-S40

AJIC Supplement Findings
• 297 unique respondents
First 8 case studies published separately gathered 523 respondents on
average
9 case studies at once; shortened time frame
•Eighty-three (83/297 or 27.9%) passed on the first attempt:
passing score 80%
•Overall: 64.6% (5,567/8,613) correct responses (range: 13.8%-
100%)
• Those with 10+ years of healthcare experience answered correctly
(69.7%) more often than those with fewer years of experience (64.8%
p<0.001)
• Those with a Master’s degree were more likely to pass (36.7%) than
those with an associate or bachelor’s degree (23.8% p=0.02)

• Cross-sectional study: sample of US-based members of the
SHEA Research Network; non-pediatric hospitals
• Objective: Using clinical vignettes, characterize variations
in the interpretation of NHSN definitions
• 113 responses from at least 61 unique hospitals
• Respondents:
79.2% infection preventionists
79.4% worked in academic hospitals
• 6 clinical vignettes were used – piloted and vetted through
two NHSN surveillance experts and experienced IPs
Keller SC, Linkin DR, Fishman NO, Lautenbach E. Variations in Identification of Healthcare-
Associated Infections. Infect Control Hosp Epidemiol 2013;34(7):678-686.
Variation in Application of NHSN Definitions
5

Variation in Application of NHSN Definitions
6

Clinical Vignette – CLABSI
7

Variation in Application of NHSN Definitions
8
#2 – Negative control- response of NO
#6 – Positive control – response of YES
Correct respond bolded

• Results:
Mean percentage of correct responses = 61.1% with low inter-
rater reliability between respondents. Correct responses
ranged from a high of 87.5% (CLABSI) to a low of 27.4% (C.
difficile)
No differences identified in HAI reporting characteristics based
on:
State-mandated reporting requirements
Hospital characteristics
IPC program characteristics
Respondents with clinical background were more likely to have
higher scores
Variation in Application of NHSN Definitions
9

Conclusion:
Substantial disparateness exists in the application of HAI
surveillance definitions
“ more reproducible definitions of HAIs – or even new
approaches to HAI surveillance, such as electronic surveillance –
are urgently needed”
Variation in Application of NHSN Definitions
10

11
• Goal: “deliver a reliable source of high quality data for
analysis and action at the facility, local, state and national
levels”
• Decrease subjectivity
• Maintain epidemiologic standardization and clinical
relevance
• NO near-term plans for further revisions
• 2015 data will provide the baseline for calculating the SIRs
for 2016 and subsequent years
• Future changes – “move to fully electronic capture of
required data and determination of events”: 3-5 years
NHSN 2015 Definition Changes

General NHSN HAI Changes
Acknowledgement: Some slides are from the
Utah Department of Health
12

13
• NHSN Infection Window Period
• No more “gap” day for defining site-specific infection criterion
• Window is defined as the 7-day period during which all site-
specific infection criterion must be met
• Day 1: first positive diagnostic test was obtained, the 3
calendar days before and the 3 calendar days after.
• If diagnostic testing is not part of the definition, use the first
date that localized signs/symptoms developed
• Does NOT apply to SSI, VAE, or LabID Event surveillance
• Site-specific criterion: laboratory specimen collection date,
imaging test date, procedure or exam date, physician diagnosis,
initiation of treatment
General NHSN HAI Changes

14

15
• NHSN Date of Event
• Changed from the date of the LAST to the FIRST element of
infection criteria being met
• Does NOT apply to VAE or LabID event surveillance
• Occurs for the first time within the 7-day infection window
period
• Date of event within the POA timeframe: day of admission, 2
days prior and 1 day after
• Date of event on or after hospital day 3 = HA
General NHSN HAI Changes

16

17

18

19
• Repeat Infection Timeframe (RIT)
• 14-day period during which repeat infections of the SAME
infection type cannot be reported
• Day 1 of the RIT is the date of the event for the first infection
• Does NOT apply to SSI, VAE or LabID events
• If additional site-specific specimens are collected within the
RIT and NEW pathogens are detected, ADD to the original
infection documentation
General NHSN HAI Changes

20

21
Adding an additional pathogen to event forms in
NHSN

22

23
NHSN Supporting Materials
http://www.cdc.gov/nhsn/acute-care-hospital/CAUTI/index.html
24
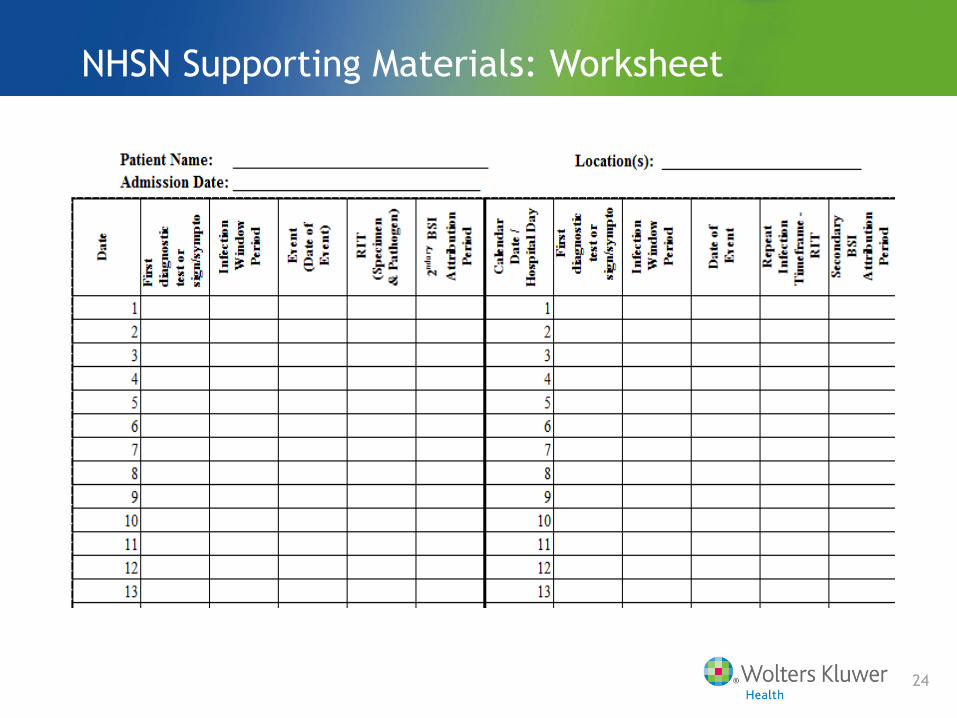
NHSN Supporting Materials: Worksheet

25
Example Worksheet

26
• Secondary Bloodstream Attribution
• Time period will include the 17 days that make up the infection
window for the primary infection as well as that infection’s RIT
• Length of the attribution period will vary from 14-17 days
depending on where the date of event falls within the infection
window period
• Does NOT apply to SSI, VAE, or LabID event surveillance
• The entire chapter of NHSN definitions has been updated to
include ALL changes – Chapter 17 of the NHSN Manual
General NHSN HAI Changes

27

Utilizing NHSN 2015 Definitions
• Clinical scenarios
Acknowledgement: Some of the slides represent material
presented at the NHSN Training Conference: Feb 17-19,
2015
28

Is it a CLABSI?
29

30
• 9/1: Mr. Jones is admitted for a COPD exacerbation and has
a central line inserted
• 9/6: He is hypotensive and has a slightly elevated WBC. BP
responds to fluids
• 9/7 Hypotensive with further increase in WBC- two sets of
blood cultures are drawn
• 9/9: Blood cultures are positive from both sets: 1st set grew
CNS and the 2nd set grew Staph epidermidis. No other source
of infection is identified
BSI Case Study

31
BSI Case Study:

32
• Does this patient have a LCBSI? If so, what criterion?
1. Yes
2. No
BSI Case Study: Polling Question

33
• Does this patient have a LCBSI? YES
BSI Case Study: Polling Question

CLABSI Reporting in Dialysis Patients
34

CLABSI Reporting in Dialysis Patients
35

Is it a CAUTI?
36

Is it a CAUTI?
37

38
• UTI
Is it a CAUTI?

39
• 4/1: Mr. Smith is a 66 yo admitted to the CCU with a
diagnosis of CHF and ventricular fibrillation. Urinary
catheter and RIJ central line inserted
• 4/5: Temperature of 38.40 C. Fever work-up performed -
urine and blood cultures sent
• 4/6: Temperature remains 38.40 C. Repeat urine and blood
cultures sent
• 4/8: Urine and blood culture from 4/5 reported as
negative; 4/6 urine culture + 100,000 cfu E. coli, blood
negative. Urinary catheter and central line remains in
place
• 4/10: Blood culture obtained for mental status change: +
for E.coli
UTI Case Study

40
• Does this patient meet SUTI 1a criteria?
1. Yes
2. No
• If so, what is the date of the event?
1. 4/6
2. 4/5
UTI Case Study: Polling Questions

41
• Does this patient meet SUTI 1a criteria?
1. Yes
2. No
• If so, what is the date of the event?
1. 4/6
2. 4/5 – Date of first element of infection criteria met within the
infection window period
UTI Case Study: Polling Questions

42
4/6
4/5 –
T 384

43
• Does this patient meet the criteria for secondary BSI
attribution?
1. Yes
2. No
UTI Case Study: Polling Questions

44
• Does this patient meet the criteria for secondary BSI
attribution?
1. Yes – Bloodstream infection with the same pathogen responsible for
the SUTI occurred within the 17 day time period
2. No
UTI Case Study: Polling Questions

45
• Is this a CAUTI?
1. Yes
2. No
UTI Case Study: Polling Questions

46
• Yes
• Rationale: Catheter was in place for > 2 calendar days and
the date of event – day 9 – was the day after catheter
removal
UTI Case Study: Polling Questions

47
Is it a CAUTI?

48

49
• 4/4: Patient admitted for emergent colectomy. Urinary
catheter inserted in the OR.
UTI Case Study

50
• Does this patient meet SUTI 1a. Criteria?
1. Yes
2. No
• If NO, why?
UTI Case Study: Polling Question

51
• NO – Candida not an acceptable pathogen
UTI Case Study: Polling Question

52
• SSI
• Infection Present at Time of Surgery (PATOS)
• New field on the SSI event form
• Infection is present PREOPERATIVELY
• There must be a surgeon notation of evidence of an infection or
abscess present at the time of surgery
• These cases will be analyzed separately and excluded from the
SIRs beginning with the 2016 data
SSI Surveillance Changes

53
• Revision hip and knee procedures: will require review of specific
ICD-9 diagnosis or procedure codes in the 90 days prior to and
including the index revision
• If present, mark YES to “ was the revision associated with prior
infection at index joint”
• Data will be used in risk factor analysis
•
SSI Surveillance Changes

SSI Surveillance : Reminder
Courtesy of Janet Brooks RN, BSN, CIC – NHSN Nurse Consultant

55
BSI Secondary to an SSI

56
SSI Case Study

57
• Which is the site-specific organ space definition that should
be reviewed for this case?
1. PJI – periprosthetic joint infection
2. JNT - joint
What is the date of the event?
1. Jan 15
2. Mar 8
3. Mar 9
Does the patient have a BSI secondary to the SSI-PJI?
1. Yes
2. No
SSI Case Study: Polling Questions

• PJI
• In 2014, NHSN adopted the
Musculoskeletal Infection
Society’s definition of
Periprosthetic Joint Infection
• Mar 9
• First element used to meet the
SSI infection criterion occurs for
the first time during the
surveillance period
• Yes
• The secondary attribution period
for SSI is a17-day period which
includes the date of event, 3
days prior and 13 days after
58
SSI Case Study: Polling Question

SSI Case Study: Polling Question
A patient presents with an acute abdomen. During the
exploratory laparotomy, the appendix is noted to be purulent.
Despite antibiotics and irrigation, the patient develops an SSI.
Would this be considered an HAI since the patient had an
existing infection at the time of the operation?
1. Yes
2. No
59

SSI Case Study: Polling Question
• YES
For procedure-based surveillance, the POA definition does
not apply. This case would have a wound class of IV which is a
data element for SSI risk-adjustment.
SSI form will include YES to the question “Is infection present
at time of procedure”.
60

61
• VAE
• Third tier consolidated into PVAP – Probable Ventilator-
Associated Pneumonia
VAE Surveillance Change

Is it a VAC?
62
http://www.cdc.gov/nhsn/VAE-calculator/

Is it a IVAC?
63

Is It a IVAC?
64
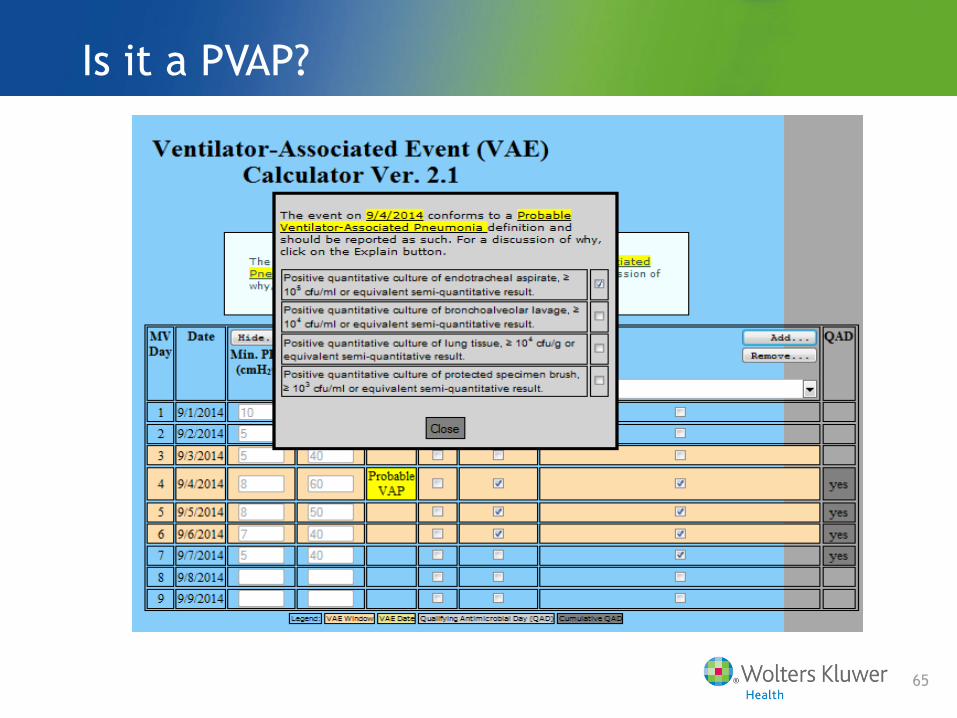
Is it a PVAP?
65

66
• LabID event reporting
• FacWideIN reporting: If the laboratory specimen is collected in
the Emergency Department or a 24-hour observation area, the
assignment of location will be for these areas and NOT the
admitting location if admission is on the same day; allows the
facility to capture CO cases
MDRO Reporting Changes

67
• Facilities reporting on HA-CDI
• New specific infection type: GI-CDI Gastrointestinal System
Clostridium difficile infection
• Does not impact CDI-LabID event reporting
MDRO Reporting Changes

68
• CRE
• New CRE organism added: CRE-Enterobacter
• In-plan reporting must include all CRE organisms: E. coli,
Klebsiella pneumoniae/oxytoca, Enterobacter
MDRO Reporting Changes

69
• http://www.cdc.gov/nhsn/labid-calculator/index.html#
MDRO & CDI LabID Event Calculator

70
MDRO & CDI LabID Event Calculator

NHSN Support
71

Thank you
Great Job!
72