applications of real time fmri: pain treatment and
TRANSCRIPT

APPLICATIONS OF REAL TIME FMRI:PAIN TREATMENT AND SUBSTANCE ABUSE TREATMENT
MARCH 2007
THIS WORK SUPPORTED BY NIH:
MH067290-01 NS050642-03 DA-4-7748 DA-4-7748 NS049673-01 DA021877-01A1
Applications of Real Time fMRI
Applications of Real Time fMRI - Phase II
Virtual Reality and Real Time fMRI
Virtual Reality and Real Time fMRI - Phase II
Novel Methods for Functional Brain Imaging
Measurement and Control of Patterned Brain Activation U i R l Ti fMRI
SPECIAL THANKS FOR HELP AND GUIDANCENora Volkow, NIDARo Nemeth, NIDADave Thomas, NIDALarry Stanford, NIDALinda Porter, NINDS

1
COLLABORATIVE TEAM
SEAN MACKEY–Axel Lucca–Deepak Soneji
JOHN GABRIELI
–Fumiko Maeda
–Alison Adcock
GARY GLOVER
JOHN PAULY
CHRISTOPHER DECHARMS–Chloe Hutton–Susan Landau–Brett Mensh–Kristen Lutomski–Saxon MacLeod–Debbie Scacco–Dave Hagewood
AFFILIATION

2
TALK OUTLINE
OVERVIEW OF REAL TIME FMRI
LEARNED CONTROL OVER BRAIN ACTIVATION AND PAIN
RTFMRI IN CHRONIC PAIN
SUBSTANCE ABUSE - PRELIMINARY EXPERIENCES

3
DESCARTES VIEW OF BRAIN, AND PAIN

4
IS IT POSSIBLE TO VISUALIZE THE MECHANISMS UNDERLYING PERCEPTION IN REAL TIME?
fMRI

5
CAN MRI BECOME A THERAPEUTIC MODALITY?
Today3TMRI
Diagnostic Radiology
DIAGNOSTIC
• MRI provides answer
• Very broad application
DIAGNOSTIC
• MRI provides answer
• Very broad application

6
CAN MRI BECOME A THERAPEUTIC MODALITY?
Today3TMRI
DIAGNOSTIC
• MRI provides answer
• Very broad application
DIAGNOSTIC
• MRI provides answer
• Very broad application
THERAPEUTIC
• MRI provides patient improvement
• Application in areas of severe need
THERAPEUTIC
• MRI provides patient improvement
• Application in areas of severe need
Tomorrow?
Diagnostic Radiology Neuroimaging Therapy

7
RTFMRI AS A POTENTIAL NEW INTERFACE TO THE NERVOUS SYSTEM
+•Control of screen cursor demonstrated in monkeys•Potential to control prosthetics
Multi-electrode recording
•Used in epilepsy and elsewhere•EEG Neurofeedback•Control of screen cursor demonstrated in people
EEG-based measurement
•Drive centers in the brain that control global functioning in order to remediate disease•Currently applied in Parkinson’s disease, efforts underway in others
Deep brain stimulation
•Restore hearing through direct stimulation of the nervous system in the profoundly deaf•Potential to move on to vision as well
Cochlear implant
+
Wires
Wires
Wires
Wires
+
+

8
RTFMRI AS A POTENTIAL NEW INTERFACE TO THE NERVOUS SYSTEM
+•Control of screen cursor demonstrated in monkeys•Potential to control prosthetics
Multi-electrode recording
•Used in epilepsy and elsewhere•Used in anesthesia monitoring•Control of screen cursor demonstrated in people
EEG-based measurement
•Non-Invasive•No tissue damage•Reasonable localization
Neuroimaging/Cognitive
•Drive centers in the brain that control global functioning in order to remediate disease•Currently applied in Parkinson’s disease, efforts underway in others
Deep brain stimulation
•Restore hearing through direct stimulation of the nervous system in the profoundly deaf•Potential to move on to vision as well
Cochlear implant
+
Wires
Wires
Wires
Wires
+
+
+
Photons
9
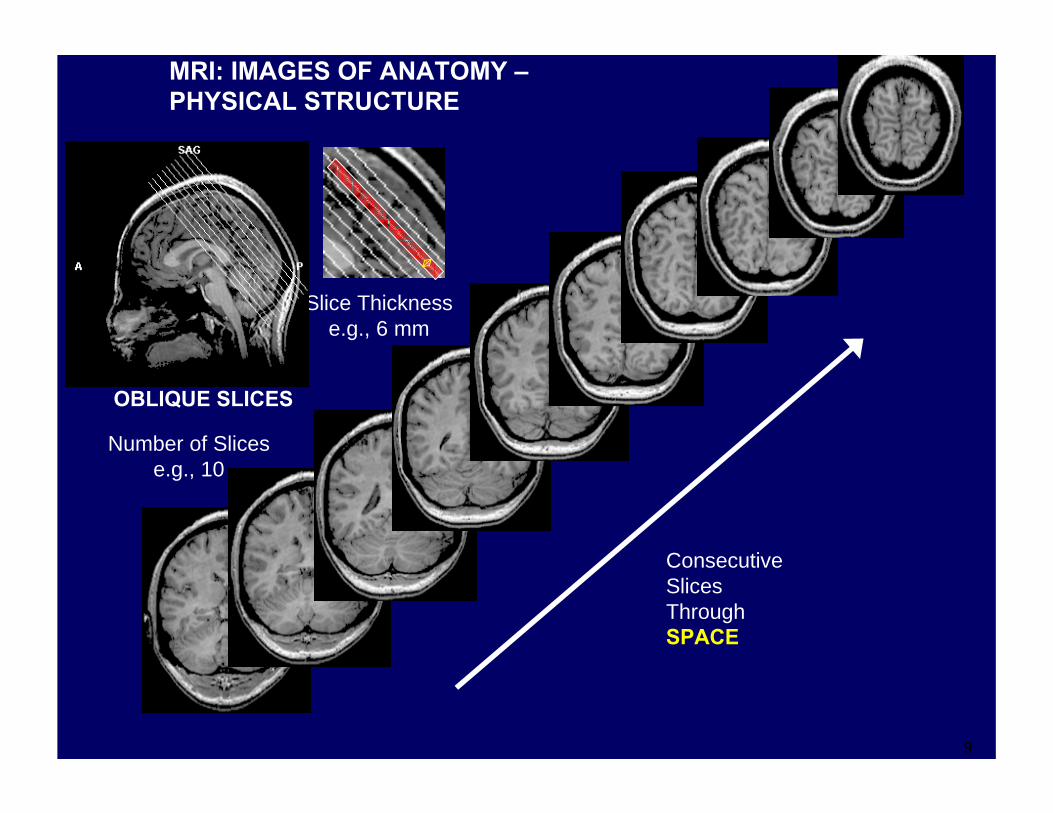
Slice Thicknesse.g., 6 mm
Number of Slicese.g., 10
OBLIQUE SLICES
MRI: IMAGES OF ANATOMY –PHYSICAL STRUCTURE
ConsecutiveSlicesThroughSPACE

10
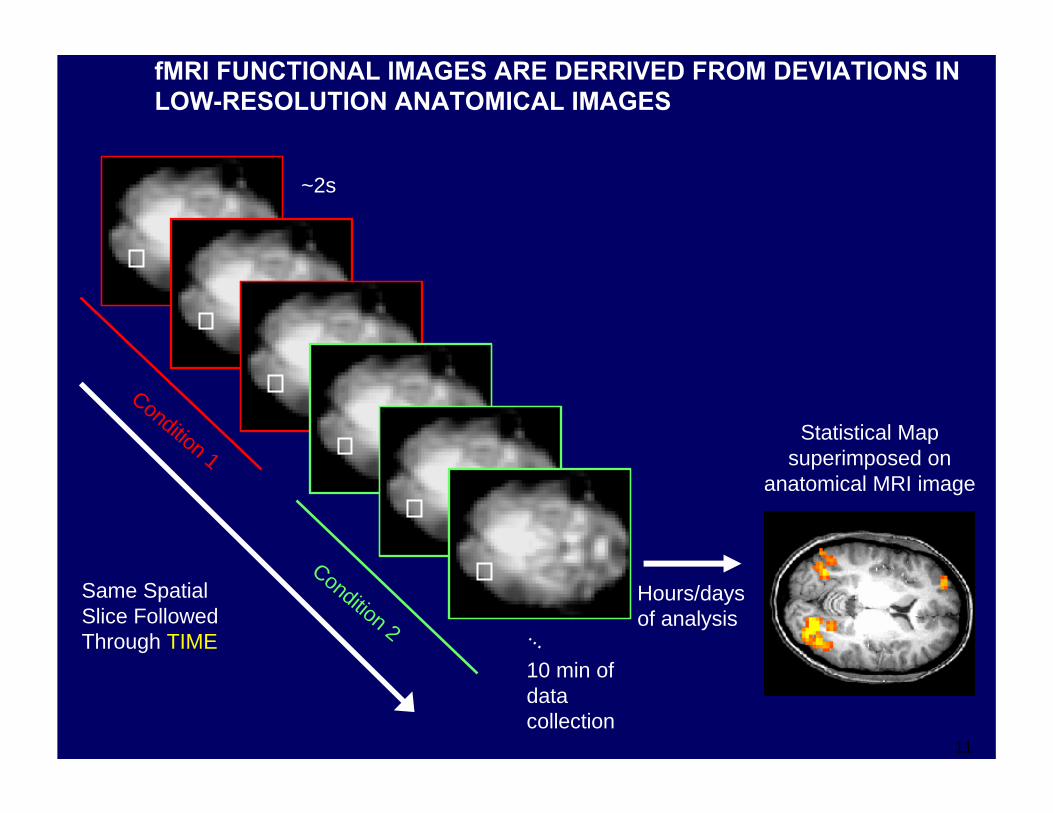
~2s
Same SpatialSlice FollowedThrough TIME ...
fMRI: IMAGES OF PHYSIOLOGY –FUNCTION
10 min ofdata collection
fMRI FUNCTIONAL IMAGES ARE DERRIVED FROM CHANGES IN T2*-SENSITIVE LOW-RESOLUTION IMAGES OVER TIME
11
Statistical Mapsuperimposed on
anatomical MRI image
~2s
Same SpatialSlice FollowedThrough TIME
Condition 1
Condition 2 ...
fMRI FUNCTIONAL IMAGES ARE DERRIVED FROM DEVIATIONS IN LOW-RESOLUTION ANATOMICAL IMAGES
10 min ofdata collection
Hours/daysof analysis

12
Statistical Mapsuperimposed on
anatomical MRI image
~2s
Same SpatialSlice FollowedThrough TIME
Condition 1
Condition 2 ...
Hours/daysof analysis
Region of interest (ROI)
fMRI FUNCTIONAL IMAGES ARE DERRIVED FROM DEVIATIONS IN LOW-RESOLUTION ANATOMICAL IMAGES
10 min ofdata collection

13
Statistical Mapsuperimposed on
anatomical MRI image
~2s
Same SpatialSlice FollowedThrough TIME
Condition 1
Condition 2 ...
Hours/daysof analysis
Region of interest (ROI)
fMRI FUNCTIONAL IMAGES ARE DERRIVED FROM DEVIATIONS IN LOW-RESOLUTION ANATOMICAL IMAGES
10 min ofdata collection
Time
fMRISignal
(% change)
ROI Time Course
Condition

14
OVERVIEW OF METHOD
MRI acquires real time fMRI data (spiral or EPI)
MRI acquires real time fMRI data (spiral or EPI)
Real time fMRI analysis•Motion correction•Temporal filtering•Spatial filtering•Event-related averages•Pattern comparison
Real time fMRI analysis•Motion correction•Temporal filtering•Spatial filtering•Event-related averages•Pattern comparison
Subjects (or patients or clinicians) watch their cognitive processes unfold ‘live’, depicted as simulated displays
Subjects (or patients or clinicians) watch their cognitive processes unfold ‘live’, depicted as simulated displays
Image from story courtesy

15
RTFMRI SETUP

16
RTFMRI-BASED TRAINING – A MORE PRECISE, ANATAMICALLY TARGETED MEASURE THAN TRADITIONAL AUTONOMIC ‘BIOFEEDBACK’
60’s Predominantly measures of global arousal.
Most useful if you want to teach relaxation
AUTONOMIC FUNCTIONHeart RateBreath RateSkin ConductanceSkin Temperature
CONSEQUENCESMEASURES

17
RTFMRI-BASED TRAINING – A MORE PRECISE, ANATAMICALLY TARGETED MEASURE THAN TRADITIONAL AUTONOMIC ‘BIOFEEDBACK’
TODAY
60’s
Can measure the very specific neurophysiological functions associated with the >100 individual brain areas.
Can measure patterns of activation evolving across multiple brain areas.
Potential to train subjects to produce very specific neurophysiological effects.
BRAIN FUNCTION
Predominantly measures of global arousal.
Most useful if you want to teach relaxation
AUTONOMIC FUNCTIONHeart RateBreath RateSkin ConductanceSkin Temperature
CONSEQUENCESMEASURES

18
CHALLENGES WITH fMRI AS A MEASURE OF BRAIN FUNCTION
Patient care costs can easily run into $100k/yr/patient for many CNS diseases. Invasive CNS procedures can easily cost this much for a single procedure.
Isn’t MRI way too expensive to really be practical?
$$
SPATIALSCALE
TIMESCALE
It may not be necessary to control individual neurons to achieve important applications: eg drugs, deep brain stimulation.
There may be ~107 neurons in the areas that fMRI is measuring – that’s no way to measure the code.
Cognitive processing is closer to the seconds timescale. We’ll use better temporal methods as soon as they come along.
Neural activation is on a msec timescale, diseases lead to long-term changes in brain function. fMRIsignals evolve over a few seconds.
POTENTIAL RESOLUTIONPROBLEM
“Neurophysiologist reaction”

19
CHALLENGES WITH fMRI AS A MEASURE OF BRAIN FUNCTION
Patient care costs can easily run into $100k/yr/patient for many CNS diseases. Invasive CNS procedures can easily cost this much for a single procedure.
Isn’t MRI way too expensive to really be practical?
$$
OVER TIME, IMAGING
TECHNOLOGY WILL EVOLVE TO
NEW USES:
SPATIALSCALE
TIMESCALE
It may not be necessary to control individual neurons to achieve important applications: eg drugs, deep brain stimulation.
There may be ~107 neurons in the areas that fMRI is measuring – that’s no way to measure the code.
Cognitive processing is closer to the seconds timescale. We’ll use better temporal methods as soon as they come along.
Neural activation is on a msec timescale, diseases lead to long-term changes in brain function. fMRIsignals evolve over a few seconds.
POTENTIAL RESOLUTIONPROBLEM

20
RTFMRI AND COGNITIVE TRAINING TAKE-HOME EXERCISE
Next WedProduce 1% modulation in rACC activation
DUE DATEASSIGNMENTPOSSIBLE CREDIT

21
RTFMRI AND COGNITIVE TRAINING TAKE-HOME EXERCISE
??Take control over your own reward and endorphin systems…
Next WedProduce 1% modulation in rACC activation
DUE DATEASSIGNMENTPOSSIBLE CREDIT

22
RTFMRI AND COGNITIVE TRAINING TAKE-HOME EXERCISE
FutureDecrease pain and suffering
??Take control over your own reward and endorphin systems…
Next WedProduce 1% modulation in rACC activation
DUE DATEASSIGNMENTPOSSIBLE CREDIT

23
REAL TIME FMRI TRAINING OF BRAIN FUNCTION
Pre Post
R L R LActivation target
Learned regulation of spatially localized brain activation using real-time fMRI. NeuroImage (2004) 21, 436-443deCharms, R. C., Christoff, K., Glover, G. H., Pauly, J. M., Whitfield, S., and Gabrieli, J. D.

24
IMPACT OF RTFMRI TRAINING ON BRAIN ACTIVATION
A) Pre-Training BOLD Individual
B) Post-Training BOLD Individual
0 60s
60 120 180 240s
C) Average
D) Average
E) Concurrent EMG
0Time (s)
% s
igna
l ∆%
sig
nal ∆
mV
2
1
-1
-2
2
1
-1
-2
-101
.6
0
.2
.4
.6
.2
.4
0

25
TIME COURSE OF TRAINING EFFECT AND CONTROLS
B)A) C) D) E)
Training,ROI
Whole brain control
ShamTraining,ROI
MotorTask,ROI
Post-TrainingTest,ROI
Sess
ion
I
0
.5
Sess
ion
IISe
ssio
n III
Sess
ion
ISe
ssio
n II
Sess
ion
III
Sess
ion
ISe
ssio
n II
Sess
ion
III
Expe
rimen
tal
Sham
+ Fe
edba
ck
-Fee
dbac
k
% s
igna
l ∆

26
CAN THIS APPROACH BE USED IN CLINICALLY IMPORTANT AREAS?

27
TRANSLATING BASIC RESEARCH IN PAIN INTO A NEW POTENTIAL THERAPEUTIC APPLICATION AREA: NEUROIMAGING
APPLIED QUESTIONBASIC RESEARCH
…and subjects with different pain sensitivities show differences in a similar group of brain regions
CAN NEURAL PLASTICITY BE ANATOMICALLY TARGETED?
Pain, and brain, can be changed substantially by mechanisms of plasticity
CAN SUBJECTS SHIFT THEIR PAIN TOLERANCE OR PERCEPTION?
There are large individual differences in pain perception…
CAN SUBJECTS BE TRAINED TO MORE EFFECTIVELY COGNITIVELY CONTROL PAIN?
Pain can be powerfully modulated by cognitive processes including attention, placebo effect, hypnosis, and many others involving a matrix of brain regions
012345678910
0 2 4 6 8 10stimulus
pain
Rainville…Bushnell, Science 1997

28
POTENTIAL TARGETS IN THE PAIN CONTROL SYSTEM
DCN
ThalamusVPL/VPM
SI/SII
MI/SMA
Insula
LateralOrbito-Frontal
AnteriorCingulate
Rostral ACC
Amygdala
PeriaqueductalGray
Pons/Parabrachial
nucleus
RostralVentromedial
Medulla
Spinal CordDorsal Horn
Ascending Pain
Perception System
Descending Pain Control
System
Invasive Electrical NeurostimulationProvides Pain Relief
Internal capsule
Potential Target

29
RTFMRI TRAINING PROTOCOL IN HEALTHY SUBJECTS
Decrease60s
Rest30s
Increase60s
CYCLE, (3 blocks, 150s total)
BLOCK DESIGNPain Pain
Control over brain activation and pain learned by using real-time functional MRI.Proceedings of the National Academy of Sciences (2005)deCharms, R. C., Maeda, F., Glover, G. H., Ludlow, D., Pauly, J. M., Soneji, D., Gabrieli, J. D., and Mackey, S. C.

30
RTFMRI TRAINING PROTOCOL IN HEALTHY SUBJECTS
Decrease60s
Rest30s
Increase60s
CYCLE, (3 blocks, 150s total)
RUN, (5 cycles + ratings, 13min). 1-5 RUNS per TRAINING DAY)
BriefingPre-TestsAnatomicals
Cycle 1150s
Cycle 2150s
Cycle 3150s
Cycle 4150s
Cycle 5150s
After ScanRatings Debrief
BLOCK DESIGNPain Pain
Control over brain activation and pain learned by using real-time functional MRI.Proceedings of the National Academy of Sciences (2005)deCharms, R. C., Maeda, F., Glover, G. H., Ludlow, D., Pauly, J. M., Soneji, D., Gabrieli, J. D., and Mackey, S. C.

31
RTFMRI TRAINING PROTOCOL IN HEALTHY SUBJECTS
Decrease60s
Rest30s
Increase60s
CYCLE, (3 blocks, 150s total)
RUN, (5 cycles + ratings, 13min). 1-5 RUNS per TRAINING DAY)
BriefingPre-TestsAnatomicals
Cycle 1150s
Cycle 2150s
Cycle 3150s
Cycle 4150s
Cycle 5150s
After ScanRatings Debrief
BLOCK DESIGN
ROI TARGET: rostral Anterior Cingulate Cortex
Pain Pain

32
RTFMRI TRAINING PROTOCOL IN HEALTHY SUBJECTS
Decrease60s
Rest30s
Increase60s
CYCLE, (3 blocks, 150s total)
RUN, (5 cycles + ratings, 13min). 1-5 RUNS per TRAINING DAY)
BriefingPre-TestsAnatomicals
Cycle 1150s
Cycle 2150s
Cycle 3150s
Cycle 4150s
Cycle 5150s
After ScanRatings Debrief
BLOCK DESIGN
ROI TARGET: rostral Anterior Cingulate Cortex
Pain Pain
SUBJECT INSTRUCTIONS: Written text describing cognitive modulation of pain
•Attend to pain vs. attend away•Perceive the pain as more intense vs. less intense•Perceive the pain as harmful vs. only a tactile sensation

33
RTFMRI TRAINING PROTOCOL IN HEALTHY SUBJECTS
Decrease60s
Rest30s
Increase60s
CYCLE, (3 blocks, 150s total)
RUN, (5 cycles + ratings, 13min). 1-5 RUNS per TRAINING DAY)
BriefingPre-TestsAnatomicals
Cycle 1150s
Cycle 2150s
Cycle 3150s
Cycle 4150s
Cycle 5150s
After ScanRatings
0 50 100s
-101234
fMR
I BO
LD d
iffer
ence
Debrief
BLOCK DESIGN
ROI TARGET: rostral Anterior Cingulate Cortex
Pain Pain
SUBJECT INSTRUCTIONS: Written text describing cognitive modulation of pain
•Attend to pain vs. attend away•Perceive the pain as more intense vs. less intense•Perceive the pain as harmful vs. only a tactile sensation
SUBJECT DISPLAYS

34
rtfMRI-BASED TRAINING LEADS TO SPATIALLY-SPECIFIC CHANGES IN BRAIN ACTIVATION
MEASURE: Thresholded T-statistic, (INCREASE – DECREASE) last run VS. (INCREASE – DECREASE) first run

35
HEALTHY SUBJECTS LEARN INCREASED CONTROL OVER BRAIN ACTIVATION THROUGH THE COURSE OF TRAINING
Training run 1
Trainingrun 2
Training run 3
Final testrun 4
0
0.1
0.2
0.3
0.4
0.5
0.6
rAC
Cac
tivat
ion
(BO
LD) * †
MEASURE: Brain Activation, BOLD % Signal Change,(Increase Period – Decrease Period) from each pair of blocks,
Averaged over N=8 Subjects

36
HEALTHY SUBJECTS LEARN INCREASED CONTROL OVER PAINTHROUGH THE COURSE OF TRAINING
Training run 1
Training run 2
Training run 3
Final testrun 4
-10
0
10
20
30
40
50
Pain
inte
nsity
ratin
g (%
diff
eren
ce)
** †
MEASURE: Pain Intensity Rating % Difference,(Increase Period Rating – Decrease Period Rating)/Average from each pair of blocks,
Averaged over N=8 Subjects

37
THE TIMECOURSE OF LEARNING OF CONTROL OVER BRAIN ACTIVATION MIRRORS THE TIME COURSE FOR CONTROL OVER PAIN
Training run 1
Training run 2
Training run 3
Final testrun 4
-10
0
10
20
30
40
50
Pain
inte
nsity
ratin
g (%
diff
eren
ce)
** †
Training run 1
Trainingrun 2
Training run 3
Final testrun 4
0
0.1
0.2
0.3
0.4
0.5
0.6
rAC
Cac
tivat
ion
(BO
LD) * †

38
LEARNED CONTROL OVER BRAIN ACTIVATION IN RACC LEADS TO CORRESPONDING CHANGES IN PAIN INTENSITY RATINGS FOR A CONCURRENT THERMAL STIMULUS
-0.5 0 0.5 1 1.5-40
-20
0
20
40
60
80
100
rACC activation (BOLD)
Pain
inte
nsity
(% d
iffer
ence
)
y=28.167x + 7.013 R=0.368 p<0.00076

39
FOUR CONTROL GROUPS WERE TRAINED USING SIMILAR OR IDENTICAL PROCEDURES BUT IN THE ABSENCE OF RACC RTFMRI INFORMATION
BLIND CONTROLControl for cognitive effects.
Received identical training to the experimental group, but unknown to them the rtfMRI displays that they saw corresponded to activation from a previously-tested experimental subject’s rACC, rather than their own rACC.
GROUP IV
BLIND CONTROLControl for spatial and physiological specificity
Received identical training to the experimental group, but using rtfMRI information derived from a posterior cingulate cortex region not involved in pain processing, to examine spatial and physiological specificity.
GROUP III
Control for identical training without rtfMRI
Received identical instructions to the experimental group, and the same period of training, but with no rtfMRI information, to test the effect of identical practice alone.
GROUP II
Control for effects of extended attention training
Received purely behavioral training for twice as long as the experimental group, but they had no rtfMRI feedback. They were additionally instructed to focus attention on the thermal stimuli during “increase” periods.
GROUP I

40
THE LEARNED CONTROL OVER PAIN REQUIRES SPATIALLY-SPECIFIC RTFMRI INFORMATION
rACCexper.group
-40
-30
-20
-10
0
10
20
30
40
50C
hang
e in
pai
n ra
ting
(% d
iffer
ence
)Pain Intensity

41
THE LEARNED CONTROL OVER PAIN REQUIRES SPATIALLY-SPECIFIC RTFMRI INFORMATION
rACCexper.group
Attention controlgroup I
– rtfMRIcontrolgroup II
PCC control
group III
Yoked control
group IV
-40
-30
-20
-10
0
10
20
30
40
50C
hang
e in
pai
n ra
ting
(% d
iffer
ence
)
† † † *** * ** ***† †
Pain Intensity
p<.01† †p<.001† † †p<.05 vs. experimental*p<.01 vs. experimental **p<.001 vs. experimental***
CONTROL GROUPS,NO EFFECT
EFFECT

42
THE LEARNED CONTROL OVER PAIN REQUIRES SPATIALLY-SPECIFIC RTFMRI INFORMATION
rACCexper.group
Attention controlgroup I
– rtfMRIcontrolgroup II
PCC control
group III
Yoked control
group IV
-40
-30
-20
-10
0
10
20
30
40
50C
hang
e in
pai
n ra
ting
(% d
iffer
ence
)
† † † *** * ** ***† † *** * *** **
UnpleasantnessPain Intensity
p<.01† †p<.001† † †p<.05 vs. experimental*p<.01 vs. experimental **p<.001 vs. experimental***
CONTROL GROUPS,NO EFFECT
EFFECT

43
CAN THE PICTURES OF YOUR HEAD PROVIDE RELIEF?

44
RTFMRI TRAINING PROTOCOL IN PAIN PATIENTS
Decrease60s
Rest30s
Increase60s
CYCLE, (3 blocks, 150s total)
RUN, (5 cycles + ratings, 13min). 1-5 RUNS per TRAINING DAY)
BriefingPre-TestsAnatomicals
Cycle 1150s
Cycle 2150s
Cycle 3150s
Cycle 4150s
Cycle 5150s
After ScanRatings
0 50 100s
-101234
fMR
I BO
LD d
iffer
ence
Debrief
BLOCK DESIGN
ROI TARGET: rostral Anterior Cingulate Cortex
SUBJECT INSTRUCTIONS: Written text describing cognitive modulation of pain
•Attend to pain vs. attend away•Perceive the pain as more intense vs. less intense•Perceive the pain as harmful vs. only a tactile sensation
SUBJECT DISPLAYS
NO PAINFULEXTERNAL STIMULI
45
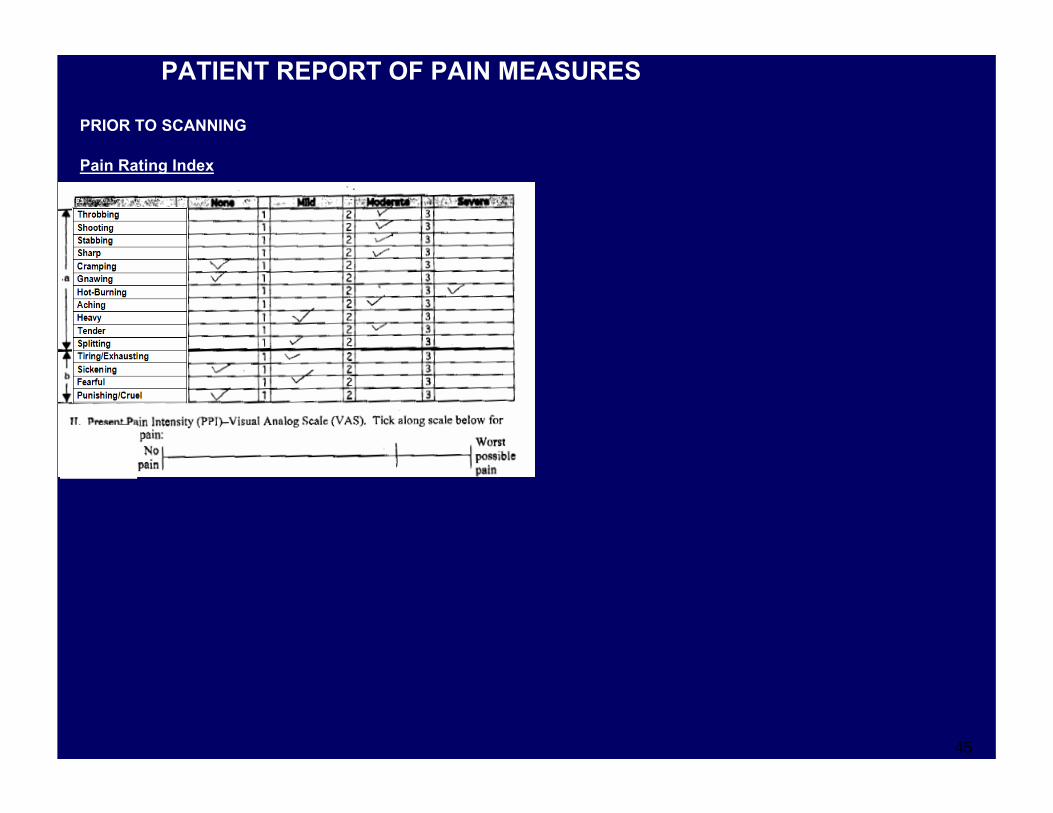
PATIENT REPORT OF PAIN MEASURES
PRIOR TO SCANNING
Pain Rating Index

46
PATIENT REPORT OF PAIN MEASURES
PRIOR TO SCANNING
Pain Rating Index
AFTER SCANNING
Pain Rating Index

47
CHANGE IN PAIN RATINGS FOLLOWING RTFMRI TRAINING IN CHRONIC PAIN PATIENTS
MPQVAS
rACC rtfMRIexperimental
group
Cha
nge
in p
ain
ratin
g (%
)
10
20
30
40
50
60
70
80
p<.001
† † †
† † †

48
PATIENTS WHO LEARNED TO CONTROL RACC ACTIVATION SHOWED A CHANGE IN PAIN, OTHERS DID NOT
--0.20.2 00 0.20.2 0.40.4 0.60.6 0.80.8 11 1.21.2 1.41.4 1.61.6 1.81.8rACCrACC change in activation (BOLD)change in activation (BOLD)
y=0.422x + 0.085. R=0.9170. y=0.422x + 0.085. R=0.9170. p<0.01p<0.01
--101000
10102020303040405050606070708080
Cha
nge
in V
AS
(%)
Cha
nge
in V
AS
(%)
00 0.20.2 0.40.4 0.60.6 0.80.8 11 1.21.2 1.41.4 1.61.6 1.81.8
y=0.376x +0.392. R=0.9173. y=0.376x +0.392. R=0.9173. p<0.01p<0.01
3030404050506060707080809090
100100
Cha
nge
in M
PQ (%
)C
hang
e in
MPQ
(%)
2020
rACCrACC change in activation (BOLD)change in activation (BOLD)

49
A CONTROL GROUP, TRAINED USING AUTONOMIC BIOFEEDBACK, DID NOT SHOW THE SAME CHANGES IN PAIN
p<.02p<.02
MPQVAS
rACC rtfMRIexperimental
group
Autonomic feedbackcontrol group
Cha
nge
in p
ain
ratin
g (%
)
10
20
30
40
50
60
70
80
p<.001† † †
† † †
† † †
EFFECTCONTROL GROUP,
NO EFFECT

50
MOTIVATIONS FOR NEUROIMAGING THERAPY IN CHRONIC PAIN TREATMENT
No surgery.No physical intervention required.
NON-INVASIVE
Technology grows to meet need:Less expensivePHYSICIAN’S OFFICE IMAGING MAY BECOME FEASIBLE
REVERSIBLE
NON-PHARMACOLOGIC
Potentially low risk.Can be terminated if unsuccessful.
No drug-related side effects.Uses endogenous physiological, neurotransmitter systems
RATIONALEIMPLICATION

51CAN THIS APPROACH COOL THE FIRES OF CHRONIC PAIN?

52
INTERFACE FOR CHRONIC PAIN PATIENTS
A Better View of Brain Disorders Science 313, 1377-1379 (8 Sept, 2006)Miller, G

53
CAN REAL TIME FMRI LEAD TO A NEW, MECHANISTICALLY-BASED, COMPUTER GUIDED FORM OF COGNITIVE INTERVENTION?

54
ONGOING STUDY: LONG-TERM RTFMRI TRAINING PROTOCOL IN PAIN PATIENTS
Decrease60s
Rest30s
Increase60s
CYCLE, (3 blocks, 150s total)
RUN, (5 cycles + ratings, 13min). 1-5 RUNS per TRAINING DAY)
BriefingPre-TestsAnatomicals
Cycle 1150s
Cycle 2150s
Cycle 3150s
Cycle 4150s
Cycle 5150s
After ScanRatings Debrief
BLOCK DESIGN
ROI TARGETS: (Two groups) 1. rostral Anterior Cingulate Cortex2. Training using rACC and bilateral insula
PROTOCOL: Training over 6 consecutive sessions, approximately 6 weeks
SUBJECT DISPLAY
NO PAINFULEXTERNAL STIMULI

55
WILL NEUROIMAGING THERAPY PRODUCE LONG-TERM DECREASES IN CHRONIC PAIN?
3
3.5
4
4.5
5
5.5
6
6.5
7
1 6
Training Week
VAS
Pain
Rat
ing
Training Group (N=21)21% decreaseDecrease seen in 16/21
NOTE:Preliminary, Unpublished Data!No Control Group to DatePlacebo Effects Are Likely

56
WILL NEUROIMAGING THERAPY PRODUCE LONG-TERM DECREASES IN CHRONIC PAIN?
Training Group (N=21)21% decreaseDecrease seen in 16/21
3
3.5
4
4.5
5
5.5
6
6.5
7
1 6Training Week
VAS
Pain
Rat
ing
Waiting List Control (N=24)5% decrease
3
3.5
4
4.5
5
5.5
6
6.5
7
1 6Training Week
VAS
Pain
Rat
ing
EFFECT CONTROL, NO EFFECT
NOTE:Preliminary, Unpublished Data!No Control Group to DatePlacebo Effects Are Likely

57
COMPARISON OF EFFECT ACROSS TWO TRAINING SITES/SCANNERS
Comparison Across Training Sites (N=10/11)
3
3.5
4
4.5
5
5.5
6
6.5
7
1 6
Training Week
VAS
Pain
Rat
ing
Together Stanford Omneuron
NOTE:Preliminary, Unpublished Data!No Control Group to DatePlacebo Effects Are Likely

58
CAN RTFMRI-BASED TRAINING BE USED IN SUBSTANCE ABUSE?PROTOCOL DETAIL
SELF-INDUCED CRAVINGTASK
REST 30s
RATE 20s
DECREASE 30s
REST 30s
RATE 20s
INCREASE 30s
RTFMRI TRAININGTASK
STIMULUS-INDUCEDCRAVING TASK
OVERVIEW OF DISPLAY TO SUBJECTS
INCREASE CRAVING
INCREASE CRAVING
DECREASE CRAVING
DECREASE CRAVING
GRAPH UP GRAPH DOWN
0 50 100s-101234
fMR
I BO
LD
0 50 100s-101234
fMR
I BO
LD
0 50 100s-101234
fMR
I BO
LD
0 50 100s-101234
fMR
I BO
LD
REST
REST
REST
REST
REST REST

59
SOME REFERENCES
Control over brain activation and pain learned by using real-time functional MRI.Proceedings of the National Academy of Sciences (2005) deCharms, R. C., Maeda, F., Glover, G. H., Ludlow, D., Pauly, J. M., Soneji, D., Gabrieli, J. D., and Mackey, S. C.
Learned regulation of spatially localized brain activation using real-time fMRI. NeuroImage (2004) 21, 436-443deCharms, R. C., Christoff, K., Glover, G. H., Pauly, J. M., Whitfield, S., and Gabrieli, J. D.
Functional brain imaging using a blood oxygenation sensitive steady state. Magn Reson Med (2003) 50, 675-683Miller, K. L., Hargreaves, B. A., Lee, J., Ress, D., deCharms, R. C., and Pauly, J. M.
WE ARE ACTIVELY ENROLLING CHRONIC PAIN PATIENTS FOR OUR CURRENT TRIAL
WE ARE INITIATING NEW COLLABORATIVE STUDY SITES
WE ARE ADDING RESEARCHERS TO OUR TEAM
THANK YOU…