approach to dyslipidemia among - صفحه اصلیhealth.tums.ac.ir/uploads/final-lipid...
TRANSCRIPT


11/28/2017 2
Approach to Dyslipidemia among
diabetic patients
Farzad Hadaegh, MD,
Professor of Internal Medicine & Endocrinology
Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Shahid Beheshti University of Medical Sciences Tehran, Nov 2017
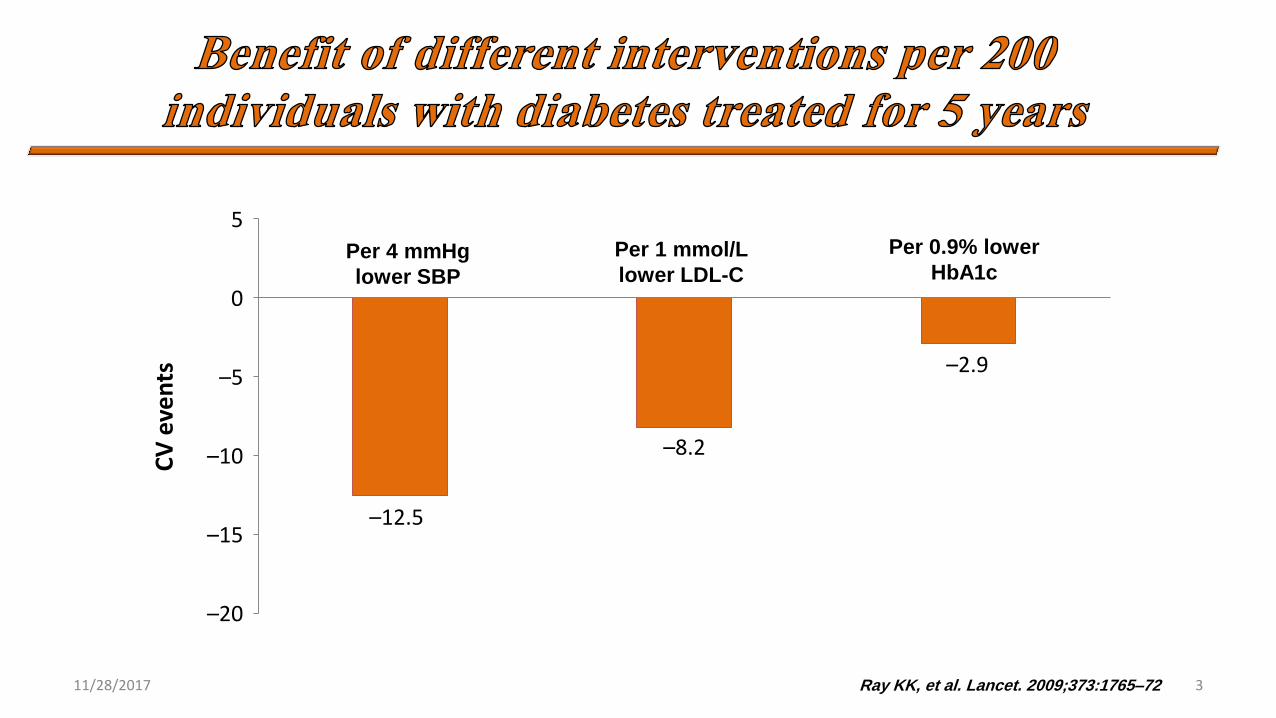
11/28/2017 3 Ray KK, et al. Lancet. 2009;373:1765–72
Per 0.9% lower
HbA1c Per 4 mmHg
lower SBP
Per 1 mmol/L
lower LDL-C
5
0
–5
–10
–15
–20
CV
eve
nts
–12.5
–8.2
–2.9

11/28/2017 4 Cholesterol, 2012, doi:10.1155/2012/861924
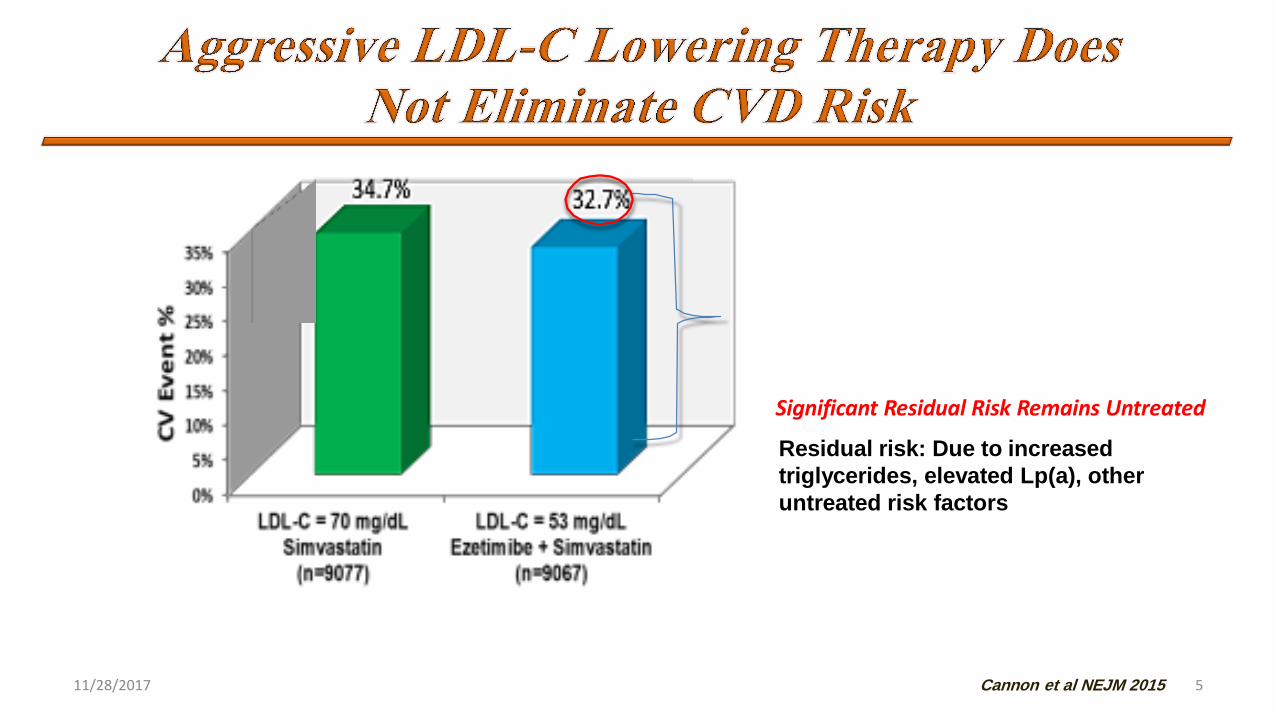
11/28/2017 5
8
Residual risk: Due to increased
triglycerides, elevated Lp(a), other
untreated risk factors
Cannon et al NEJM 2015
Significant Residual Risk Remains Untreated
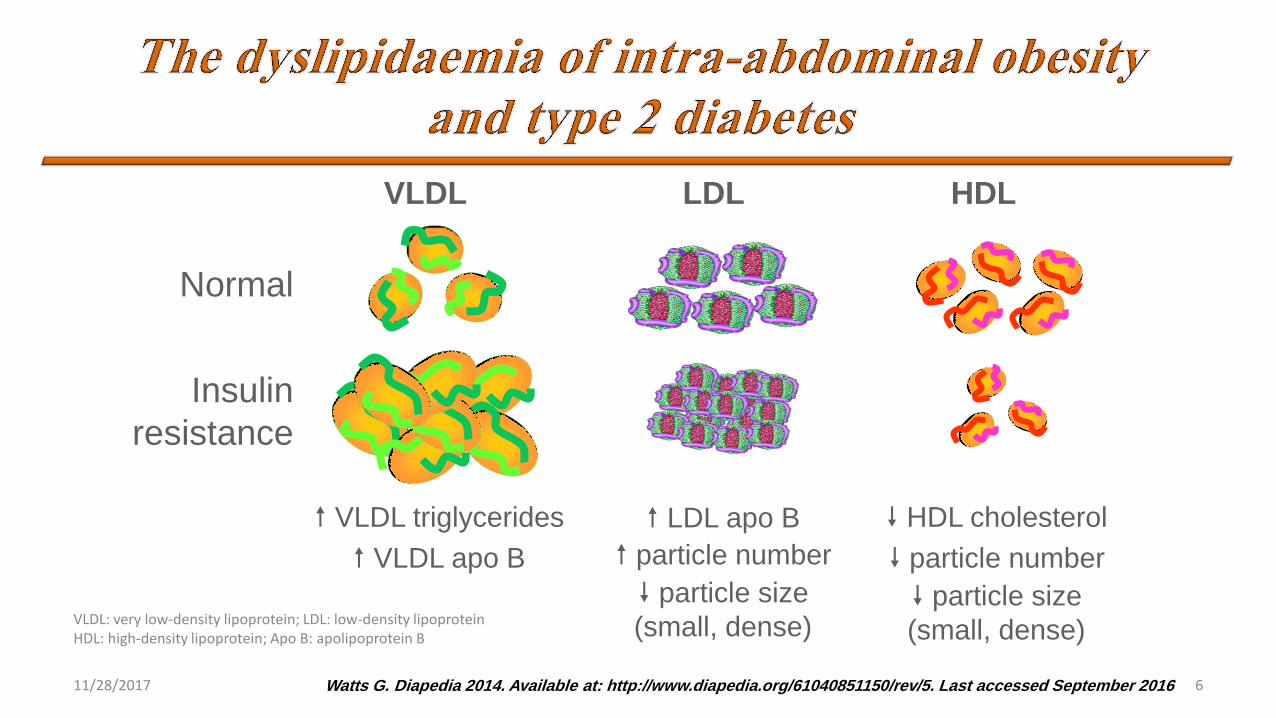
11/28/2017 6
Normal
Insulin
resistance
VLDL
VLDL triglycerides
VLDL apo B
HDL
HDL cholesterol
particle number
particle size
(small, dense)
LDL
LDL apo B
particle number
particle size
(small, dense) VLDL: very low-density lipoprotein; LDL: low-density lipoprotein HDL: high-density lipoprotein; Apo B: apolipoprotein B
Watts G. Diapedia 2014. Available at: http://www.diapedia.org/61040851150/rev/5. Last accessed September 2016
11/28/2017 7
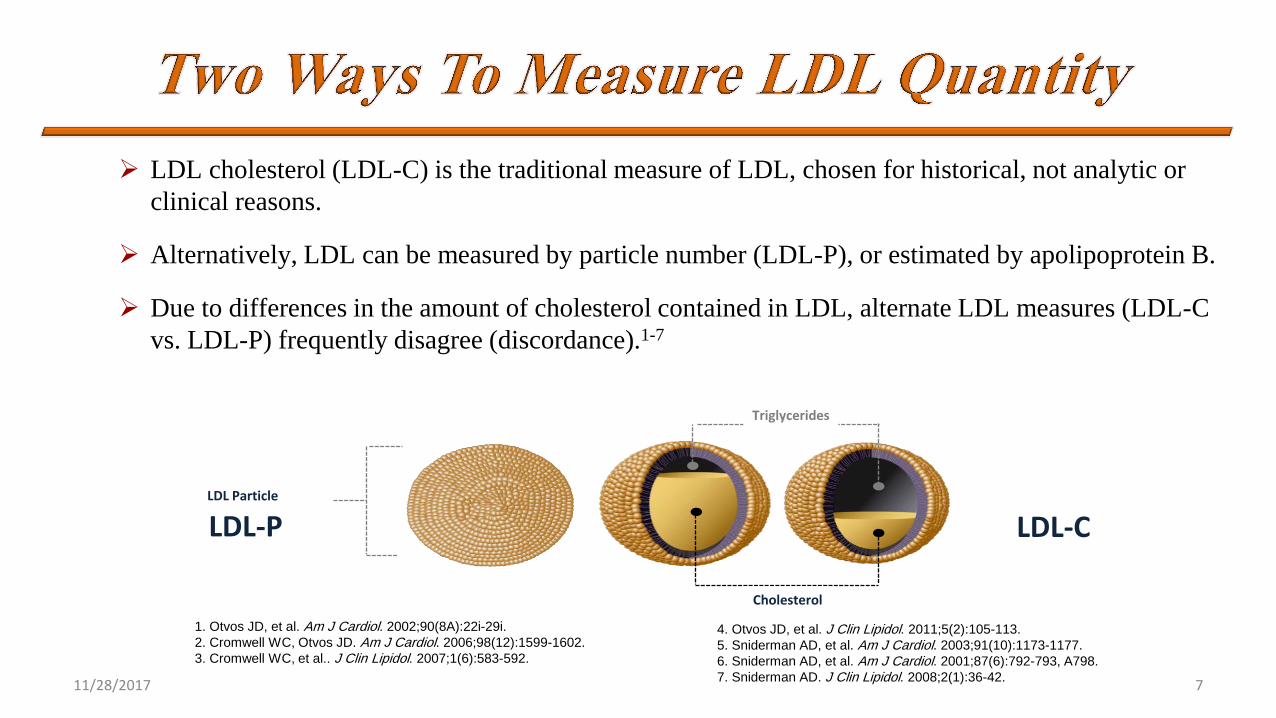
LDL cholesterol (LDL-C) is the traditional measure of LDL, chosen for historical, not analytic or
clinical reasons.
Alternatively, LDL can be measured by particle number (LDL-P), or estimated by apolipoprotein B.
Due to differences in the amount of cholesterol contained in LDL, alternate LDL measures (LDL-C
vs. LDL-P) frequently disagree (discordance).1-7
1. Otvos JD, et al. Am J Cardiol. 2002;90(8A):22i-29i.
2. Cromwell WC, Otvos JD. Am J Cardiol. 2006;98(12):1599-1602.
3. Cromwell WC, et al.. J Clin Lipidol. 2007;1(6):583-592.
4. Otvos JD, et al. J Clin Lipidol. 2011;5(2):105-113.
5. Sniderman AD, et al. Am J Cardiol. 2003;91(10):1173-1177.
6. Sniderman AD, et al. Am J Cardiol. 2001;87(6):792-793, A798.
7. Sniderman AD. J Clin Lipidol. 2008;2(1):36-42.
LDL Particle
Triglycerides
Cholesterol
LDL-P LDL-C
LDL Particle
Triglycerides
Cholesterol
LDL-P LDL-C
Cardiovascular risk tracks with LDL particle number
When alternate LDL measures (LDL-C vs LDL particle number) agree
(concordance) each measure is equally associated with CVD risk.
When alternate measures are discordant (e.g., diabetes, metabolic syndrome,
statin therapy), risk tracks with LDL-P, not LDL-C.
The majority of atherogenic lipoproteins in individuals with insulin resistance,
metabolic syndrome or T2D are smaller, cholesterol-depleted LDL particles.
These compositional changes in LDL particles may lead to a disagreement
between measures of LDL-C and LDL-P resulting in “discordance”
11/28/2017 8
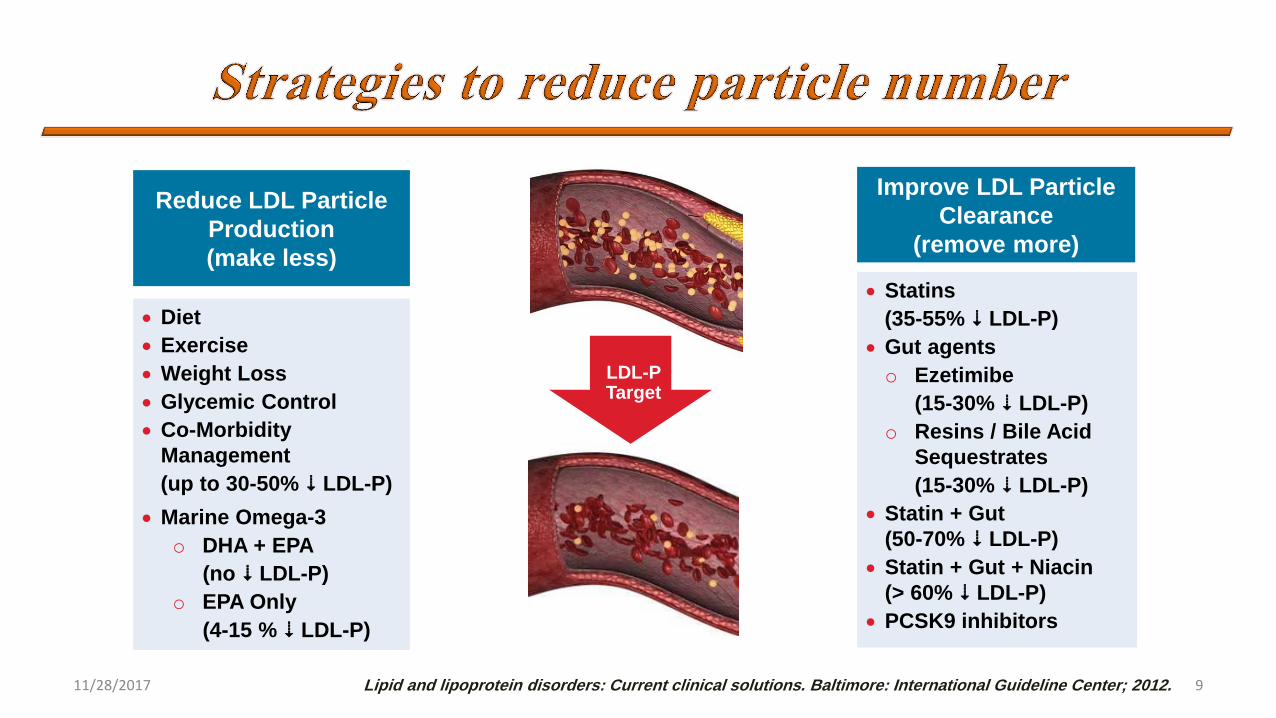
Reduce LDL Particle
Production
(make less)
11/28/2017 9
LDL-P Target
Diet
Exercise
Weight Loss
Glycemic Control
Co-Morbidity
Management
(up to 30-50% 6 LDL-P)
Marine Omega-3
o DHA + EPA
(no 6 LDL-P)
o EPA Only
(4-15 % 6 LDL-P)
Improve LDL Particle
Clearance
(remove more)
Statins
(35-55% 6 LDL-P)
Gut agents
o Ezetimibe
(15-30% 6 LDL-P)
o Resins / Bile Acid
Sequestrates
(15-30% 6 LDL-P)
Statin + Gut
(50-70% 6 LDL-P)
Statin + Gut + Niacin
(> 60% 6 LDL-P)
PCSK9 inhibitors
Lipid and lipoprotein disorders: Current clinical solutions. Baltimore: International Guideline Center; 2012.
11/28/2017 10

• Aim: assess the effects on vascular mortality and morbidity of a substantial LDL-C reduction maintained for several years in a large cohort of diabetic individuals
• Methods : 5963 UK adults (aged 40–80 years) known to have DM, and an additional 14 573 with occlusive arterial disease (but no diagnosed DM), were randomly allocated to receive 40 mg simvastatin daily or matching placebo
Lancet 2003; 361: 2005-16 11/28/2017 11
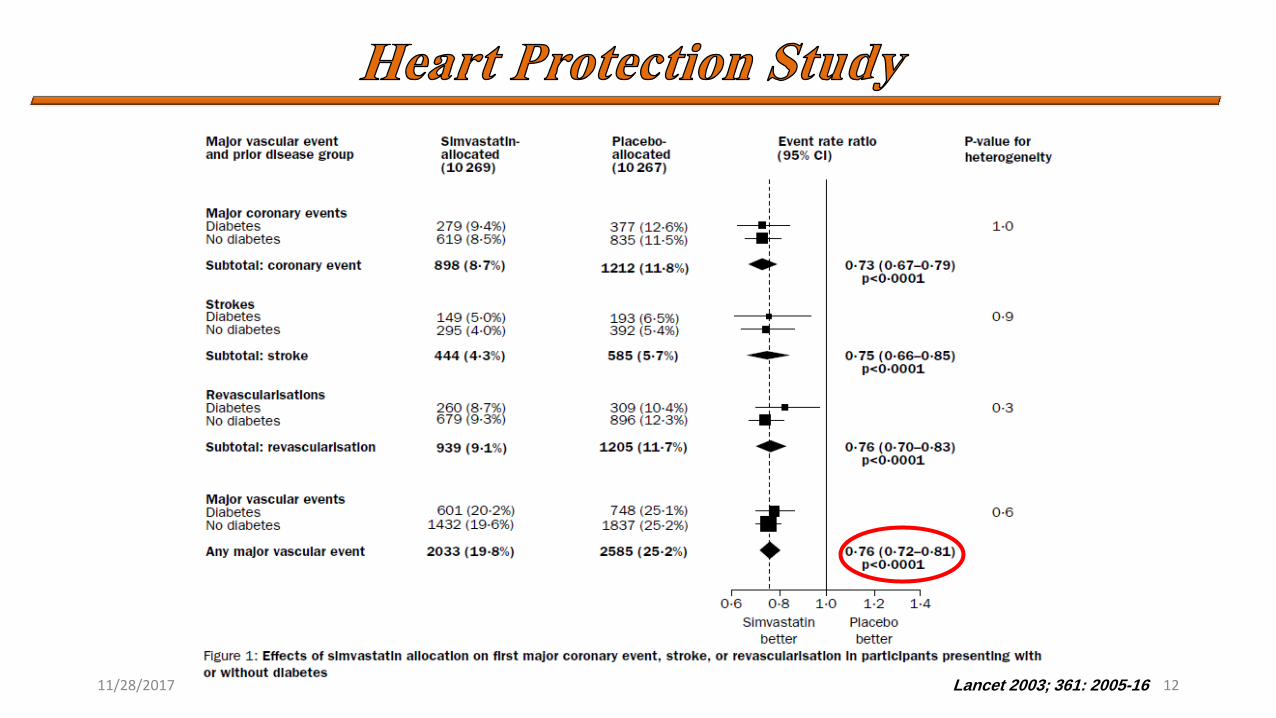
11/28/2017 12 Lancet 2003; 361: 2005-16
11/28/2017 13 Lancet 2003; 361: 2005-16
• Allocation to 40 mg simvastatin daily reduced the rate of first major
vascular events by about a quarter in a wide range of diabetic patients
studied.
• Statin therapy should now be considered routinely for all diabetic
patients at sufficiently high risk of major vascular events, irrespective
of their initial cholesterol concentrations.
• n = 2838
• Age 40-75, no history of CVD
• T2DM plus one or more:
• Retinopathy
• Albuminuria
• Hypertension
• Smoking
• Intervention: Atorvastatin 10 mg vs. Placebo
• Outcome: ACS, revascularization, stroke
Colhoun HM, et al. Lancet 2004;364:685. 11/28/2017 14
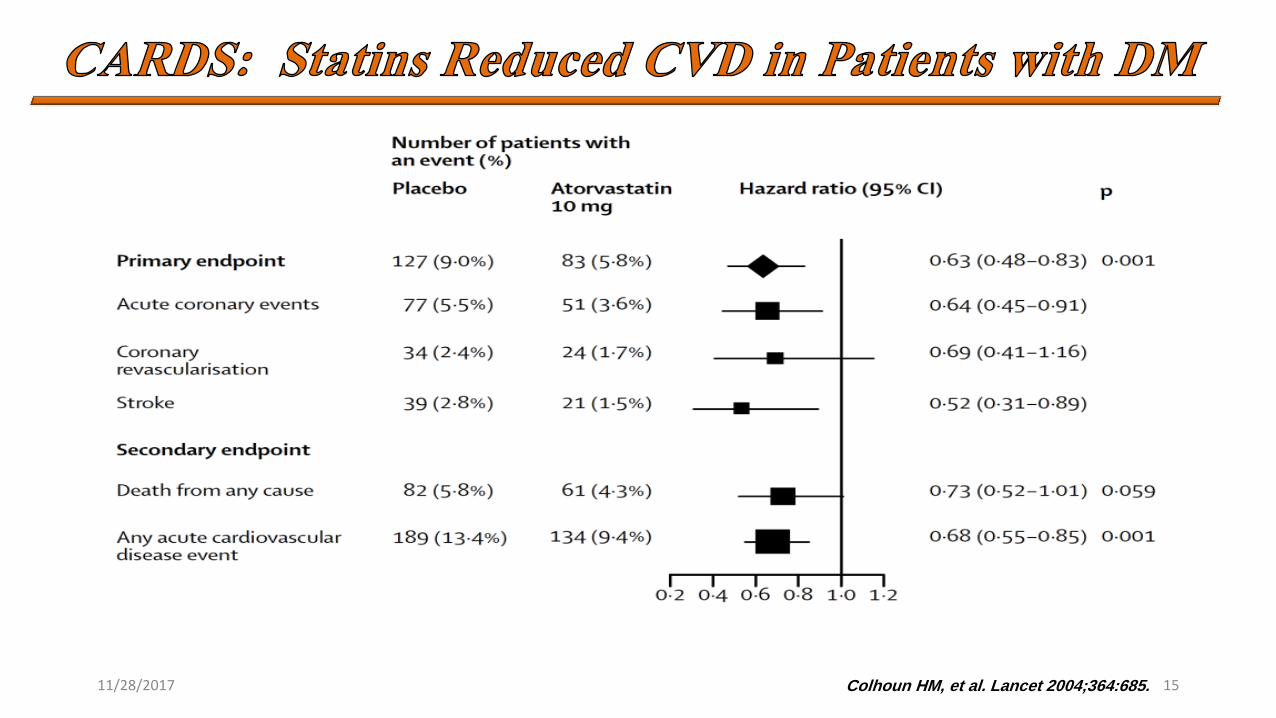
Colhoun HM, et al. Lancet 2004;364:685. 11/28/2017 15
Aim of study:
Although statin therapy reduces the risk of occlusive vascular events in people with DM
There is uncertainty about the effects on particular outcomes and whether such effects depend on the type of diabetes, lipid profile, or other factors.
Methods:
Data from 18686 individuals with diabetes (1466 type 1 and 17,220 type 2) in the context of a further 71,370 without diabetes in 14 randomised trials of statin therapy.
Estimates effects on clinical outcomes per 1.0 mmol/L reduction in LDL cholesterol.
Lancet 2008, Jan 12;371(9607):117-25 11/28/2017 16

• Result in Diabetic patients:
All cause
mortality MI or
Coronary
Death
Coronary
Revasculari
sation
Stroke
Risk
Reduction
%9
RR= 0.87
P<0.0001
22%
RR=0.78
P<0.0001
25%
RR=0.75
P<0.0001
21%
RR=79
P=0.0002
11/28/2017 17
Lancet 2008, Jan 12;371(9607):117-25
After 5 years, 42 (95% CI 30–55) fewer people with diabetes had major
vascular events per 1000 allocated statin therapy.
11/28/2017 18
11/28/2017 19

11/28/2017 20

11/28/2017 21
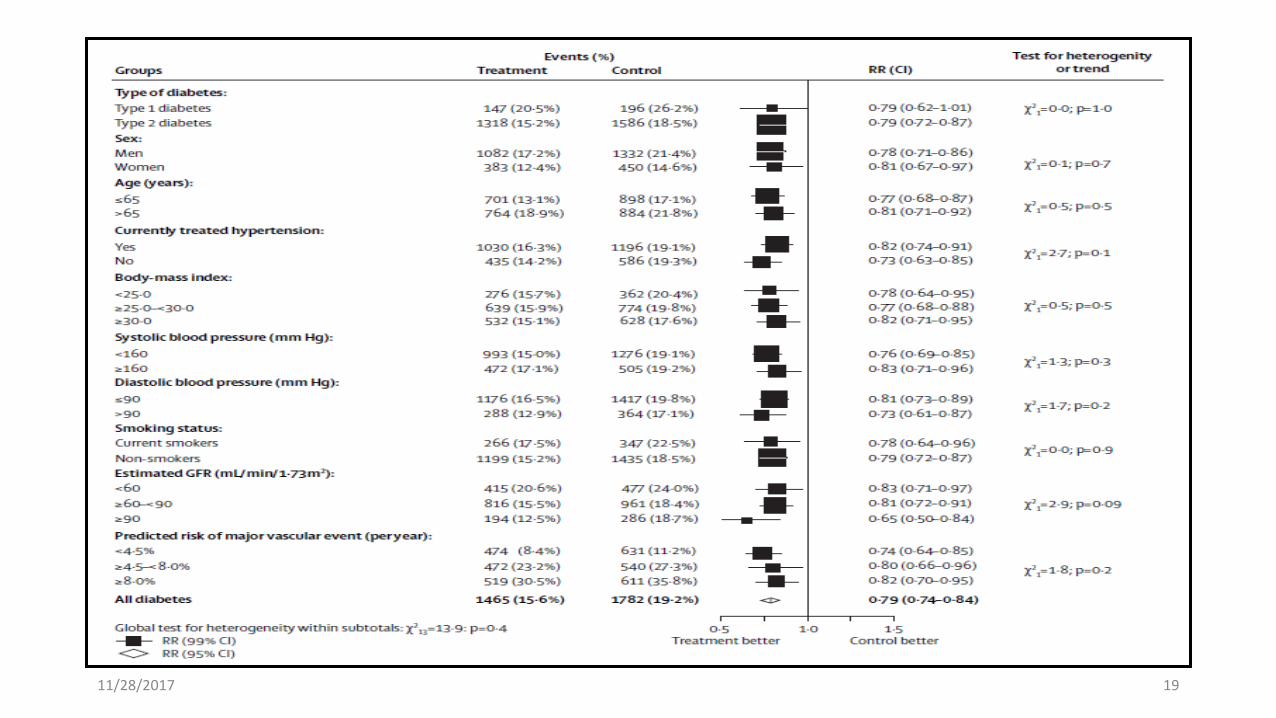
Lancet 2008, Jan 12;371(9607):117-25
Among diabetic patients the proportional effects of statin therapy were similar irrespective of whether there was a :
Prior history of vascular disease
Other baseline characteristics.
Conclusion: Statin therapy should be considered for all diabetic individuals who are at sufficiently high risk of vascular events.

11/28/2017 22
1501 patients with diabetes and CHD, primary end point: time to first major
cardiovascular event*
*CHD death, nonfatal non–procedure-related MI, resuscitated cardiac arrest, fatal
or nonfatal stroke
TNT: Treating to New Target study
Shepherd J, et al. Diabetes Care 2006;29:1220–6
Cu
mu
lati
ve i
ncid
en
ce o
f m
ajo
r card
iovascu
lar
even
ts*
Relative risk reduction = 25%
0.15
HR = 0.75 (95% CI: 0.58, 0.97)
P = 0.026
Atorvastatin 10 mg
Atorvastatin 80 mg
0.20
0.10
0.05
0
0 1 2 3 4 5 6
Years
11/28/2017 23

11/28/2017 24

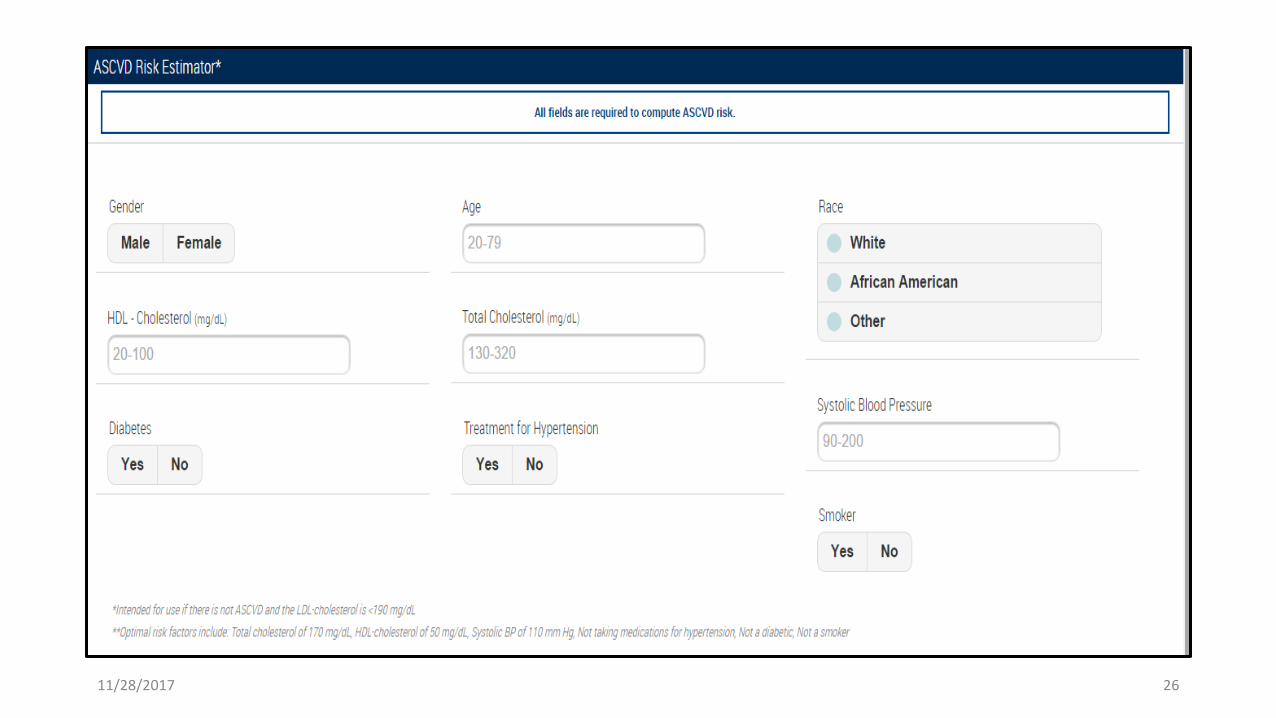
The Risk Calculator.
The American College of Cardiology/American Heart Association
ASCVD risk calculator may be a useful tool to estimate 10-year ASCVD
(http://my .americanheart.org).
11/28/2017 25
11/28/2017 26

11/28/2017 27

11/28/2017 28

11/28/2017 29

11/28/2017 30
Reduce LDL-C 18–55% & TG 7–30%
Raise HDL-C 5–15%
Major side effects
Myopathy
Increased liver enzymes
Contraindications
Absolute: liver disease
Relative: use with certain drugs
11/28/2017 31
Fibric acid derivatives, especially Gemfibrozil
Niacin
Cyclosporine
Azole antifungals
Macrolide antibiotics
HIV protease inhibitors
Nefazodone
Verapamil and diltiazem
Amiodarone
Grapefruit juice, >1 qt/d
11/28/2017 32
A meta-analysis of 13 randomized statin trials with 91,140 participants
showed an odds ratio of 1.09 (9%) for a new diagnosis of diabetes,
On average ,treatment of 255 patients with statins for 4 years resulted in 1
additional case of diabetes,
while simultaneously preventing 5.4 vascular events among those 255
patients
11/28/2017 33

11/28/2017 34
Hypertriglyceridemia should be addressed with dietary and lifestyle changes
including abstinence from alcohol
Severe hypertriglyceridemia (>1,000 mg/dL) may warrant pharmacologic
therapy (fibric acid derivatives and/or fish oil) to reduce the risk of acute
pancreatitis.
Low levels of HDL cholesterol, often associated with elevated triglyceride
levels, are the most prevalent pattern of dyslipidemia in individuals with type
2 diabetes.
11/28/2017 35

Drug Dose
• Gemfibrozil 600 mg BID
• Fenofibrate 200 mg QD
• Clofibrate 1000 mg BID
11/28/2017 36

11/28/2017 37
• Major actions
• Lower LDL-C 5–20% (with normal TG)
• May raise LDL-C (with high TG)
• Lower TG 20–50%
• Raise HDL-C 10–20%
• Side effects: dyspepsia, gallstones, myopathy
• Contraindications: Severe renal or hepatic disease
11/28/2017 38
Combination therapy (statin/fibrate) has not been shown to improve
atherosclerotic cardiovascular disease outcomes and is generally not
recommended. However, therapy with statin and fenofibrate may be
considered for men with both triglyceride level ≥204 mg/dL (2.3 mmol/L)
and HDL cholesterol level ≤ 34 mg/dL (0.9 mmol/L).
Combination therapy (statin/niacin) has not been shown to provide
additional cardiovascular benefit above statin therapy alone and may
increase the risk of stroke and is not generally recommended.

11/28/2017 39
Clinicians should attempt to find a dose or alternative statin that is
tolerable, if side effects occur.
There is evidence for benefit from even extremely low, less than daily,
statin doses .
The addition of Ezetimibe to moderate-intensity statin therapy has been
shown to provide additional cardiovascular benefit compared with
moderate-intensity statin therapy alone and may be considered for
patients :
with a Recent ACS with LDL –C >50 mg/dL or for those patients who
cannot tolerate high intensity statin therapy. A
11/28/2017 40
Individuals were 50 years of age who experienced an ACS within the
preceding 10 days and had an LDL –C level> 50 mg/dL.
In those with diabetes (27%), the combination of moderate intensity
simvastatin (40mg) and ezetimibe (10 mg) showed a significant reduction of
major adverse cardiovascular events with an absolute risk reduction of 5%
(40% vs. 45%) and RR reduction of 14% (RR 0.86 [95% CI 0.78–0.94])
over moderate-intensity simvastatin (40 mg) alone.

11/28/2017 41
11/28/2017 42
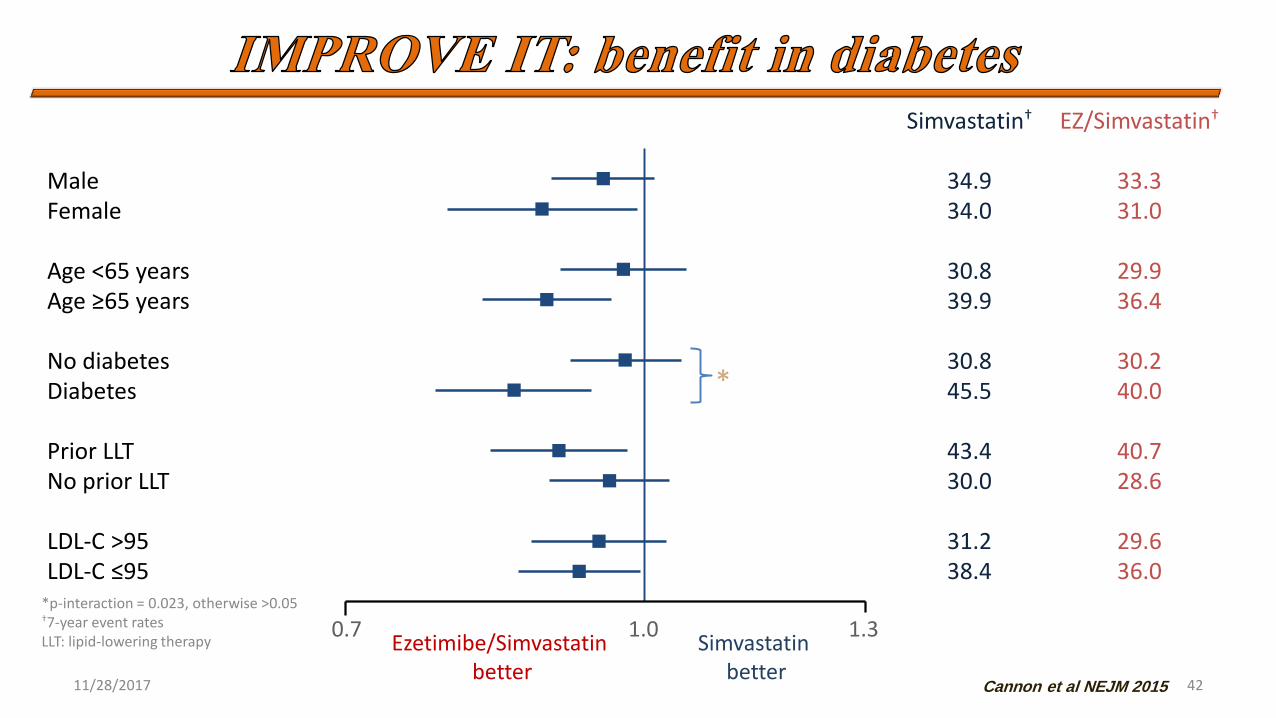
Simvastatin† EZ/Simvastatin†
Male 34.9 33.3 Female 34.0 31.0 Age <65 years 30.8 29.9 Age ≥65 years 39.9 36.4
No diabetes 30.8 30.2 Diabetes 45.5 40.0
Prior LLT 43.4 40.7 No prior LLT 30.0 28.6
LDL-C >95 31.2 29.6 LDL-C ≤95 38.4 36.0
*p-interaction = 0.023, otherwise >0.05 †7-year event rates LLT: lipid-lowering therapy Ezetimibe/Simvastatin
better Simvastatin
better
*
0.7 1.0 1.3
Cannon et al NEJM 2015

The addition of the novel PCSK9 inhibitors, Evolocumab and
Alirocumab,
To maximally tolerated doses of statin therapy in participants who
were at high risk for ASCVD
Decrese the LDL cholesterol ranging from 36% to 59%.
11/28/2017 43

11/28/2017 44

LAPLACE-2: LDL-C Assessment with PCSK9
Monoclonal Antibody Inhibition
Combined With Statin Therapy.
RUTHERFORD-2: Reduction of LDL-C With
PCSK9 Inhibition in Heterozygous Familial
Hypercholesterolemia Disorder Study.
GAUSS-2: Goal Achievement after Utilizing an
Anti-PCSK9 Antibody in Statin
Intolerant Subjects.
11/28/2017 45
11/28/2017 46
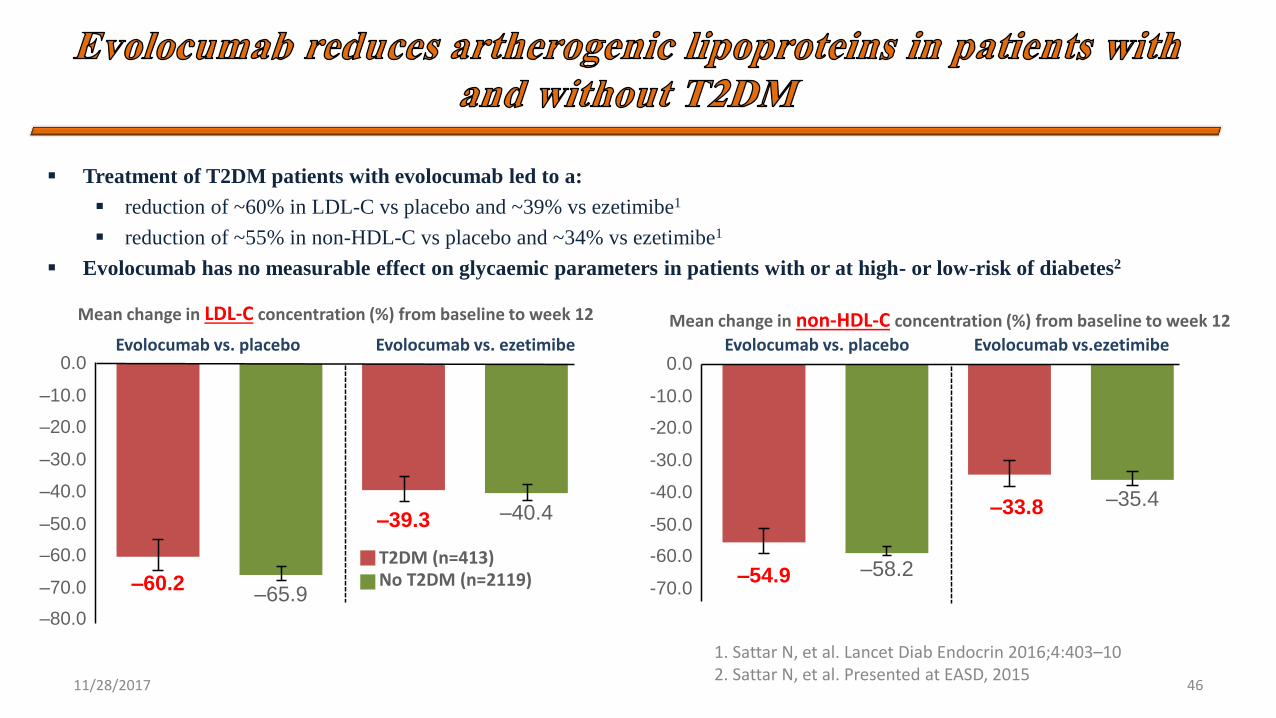
Treatment of T2DM patients with evolocumab led to a:
reduction of ~60% in LDL-C vs placebo and ~39% vs ezetimibe1
reduction of ~55% in non-HDL-C vs placebo and ~34% vs ezetimibe1
Evolocumab has no measurable effect on glycaemic parameters in patients with or at high- or low-risk of diabetes2
1. Sattar N, et al. Lancet Diab Endocrin 2016;4:403–10 2. Sattar N, et al. Presented at EASD, 2015
Mean change in non-HDL-C concentration (%) from baseline to week 12
Evolocumab vs. placebo Evolocumab vs.ezetimibe
Mean change in LDL-C concentration (%) from baseline to week 12
Evolocumab vs. placebo Evolocumab vs. ezetimibe 0.0
-10.0
-20.0
-30.0
-40.0
-50.0
-60.0
-70.0
–33.8 –35.4
–54.9 –58.2 T2DM (n=413) No T2DM (n=2119)
0.0
–10.0
–20.0
–30.0
–40.0
–50.0
–60.0
–70.0
–39.3 –40.4
–60.2 –65.9
–80.0

11/28/2017 47

Evolocumab markedly reduces
atherogenic lipoproteins in patients
with type 2 diabetes, an effect that is
consistent across subgroups and
similar to that seen in patients
without type 2 diabetes
11/28/2017 48
N Engl J Med 2017; 376:1713-1722
11/28/2017 49
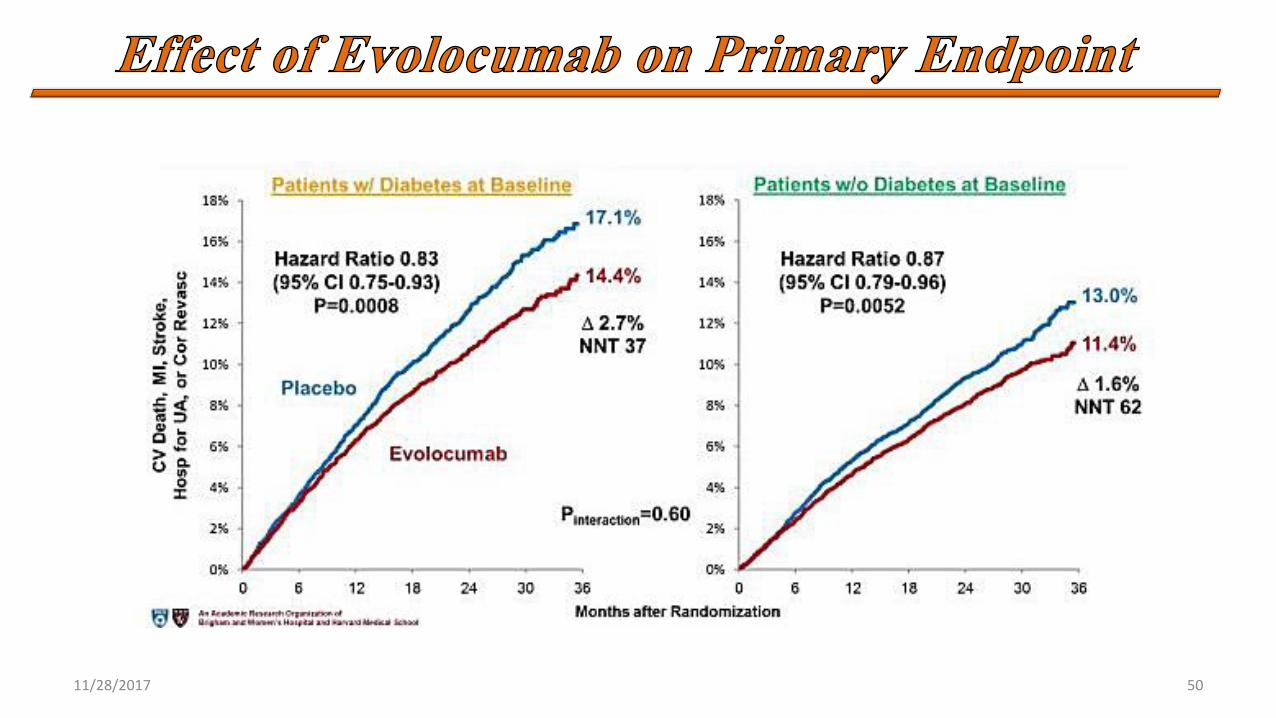
11/28/2017 50
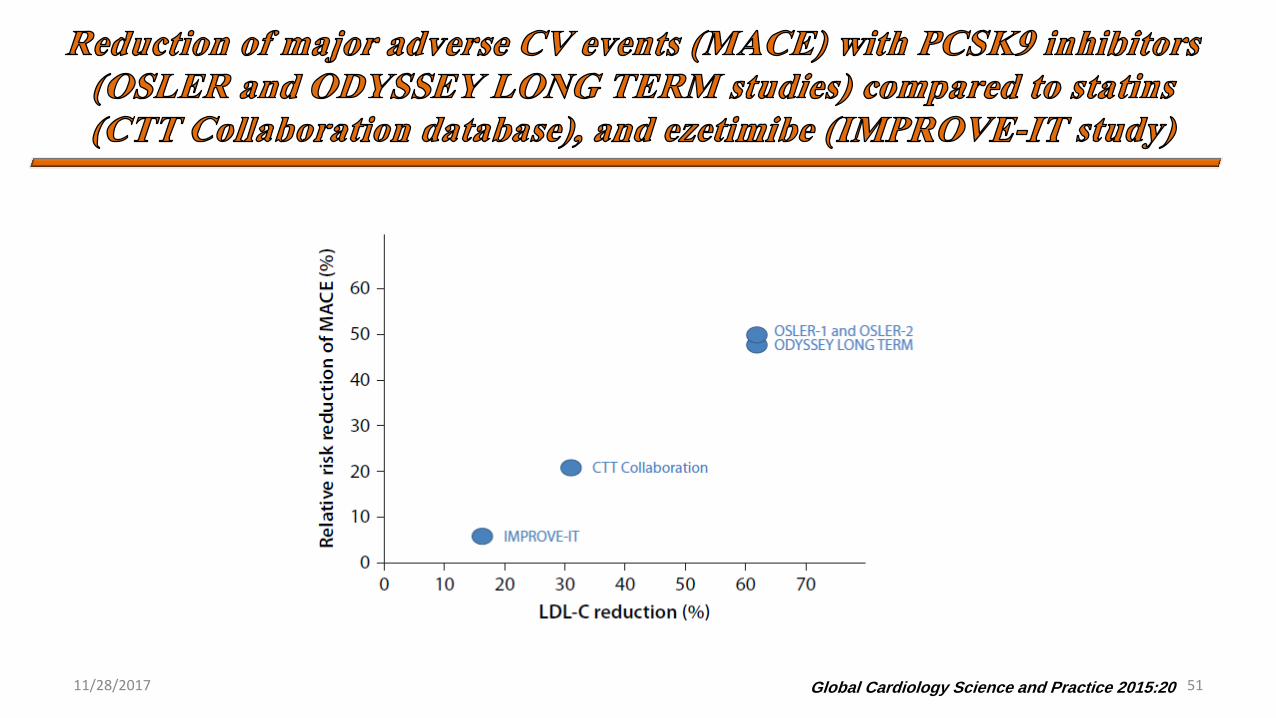
Global Cardiology Science and Practice 2015:20 11/28/2017 51
11/28/2017 52

11/28/2017 53

Patients aged 40-75, without
ASCVD, with DM and
baseline LDLc 70-189 mg/dl
on statin for primary
prevention
11/28/2017 54

11/28/2017 55
Patients with clinical
ASCVD with
comorbidities on statin
for secondary prevention
Patients with diabetes need to look beyond LDL C for better cardiovascular
risk factor stratification as they often have elevated triglycerides, non-HDL
cholesterol/LDL P
PCSK9 inhibitors reduce LDL cholesterol and have favorable safety profile
LDL-C reductions in those with diabetes were similar to those without
diabetes
PCSK9 inhibitors lower non HDL cholesterol , Lp(a) and may be an important
tool in reducing residual risk
All trials of PCKS9 inhibitors have been conducted on top of baseline statin
therapy
PCSK9 inhibitors do not yet have CV outcome data to support their use in
diabetes for primary prevention
11/28/2017 56

11/28/2017 57
Thanks for
your patience,
dear colleagues!