approach to limb pain in children/osteomyelitis mr 7/17/09 j.chen
TRANSCRIPT

APPROACH TO LIMB PAIN IN CHILDREN/OSTEOMYELITISMR 7/17/09J.Chen

Approach to Limb Pain in Children

Approach to Child with Limb Pain History History History PE Labs/Imaging

History
Important aspects: Area involved # of joints involved Nature of the pain Presence of systemic symptoms (fever, rash, weight
loss, fatigue) Presence of limp Weight bearing status Morning stiffness History of past medical illneses Travel Family History (Arthritis, Bleeding Disorders, Sickle
Cell Disease, IBD)

Physical Exam
Important Aspects Joint Exam
Swelling Erythema Warmth Tenderness Deformity ROM

Physical Exam Continue
Adjacent Structures Bones Tendons Muscles Skin
Gait Leg length discrepancy Full Neurologic Examination

Basic Screening
CBC with Diff Blood Smear ESR CRP Radiographs

Imaging
Plain Radiograph and Bone Scan (Technetium-99 scan) have long been the mainstay for joint and bone problems
CT useful in diagnosing: Osseus Tumors Pelvic and acetabular fractures Intraarticular Extension of Femoral Fractures
US: Joint effusions Developmental dysplasia of the hip
Imaging Continued
MRI-useful in evaluating Soft tissue Joint spaces Suspected joint infection Soft tissue tumors Muscle injuries Early avasular necrosis

Approach to Limb Pain in Children

Osteomyelitis
Cause: Most commonly results from Hematogenous spread May be from direct invasion of Pathogens into the
bone. May be precipitated by trauma
Pathogens: Staph aureus: 90% Non-group A beta-hemolytic streptococci Hib now less prevalent Salmonella-Sickle Cell Anemia Pseudomonas aeruginosa-puncture wound Neisseria gonorrhacae-sexually active GBS-neonates

Clinical Presentation
Sudden onset Localized pain Swelling Fever +/- trauma Limp/refusal to bear weight Previous infection

Physical Exam
Erythema Swelling Point tenderness Decreased ROM
Most commonly involves femur>tibia>humerous>fibula>radius>calcaneus>ilium

Imaging
X-Ray-not helpful in early diagnosis Findings appear after 7 days
Soft tissue swelling Subperiosteal changes Bone destruction
Bone Scan-85-100% sensitive MRI-equal sensitivity, better specificity
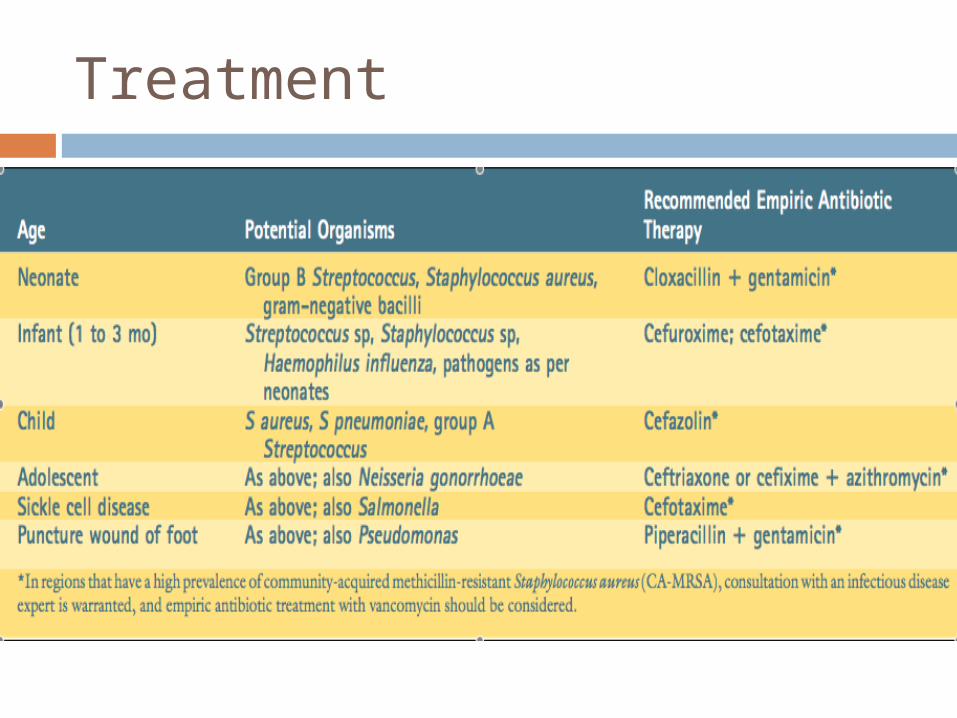
Treatment