approach to the newborn with thrombocytopenia dr. lourdes asiain nov 2004
TRANSCRIPT
Approach to the newborn with thrombocytopenia
Dr. Lourdes AsiainNov 2004
Objectives
Define mild, moderate and severe thrombocytopenia
List most common causes for the condition
List dysmorphic features assoc with Thrombocytopenia
Description and management of neonatal alloimmune thrombocytopenia
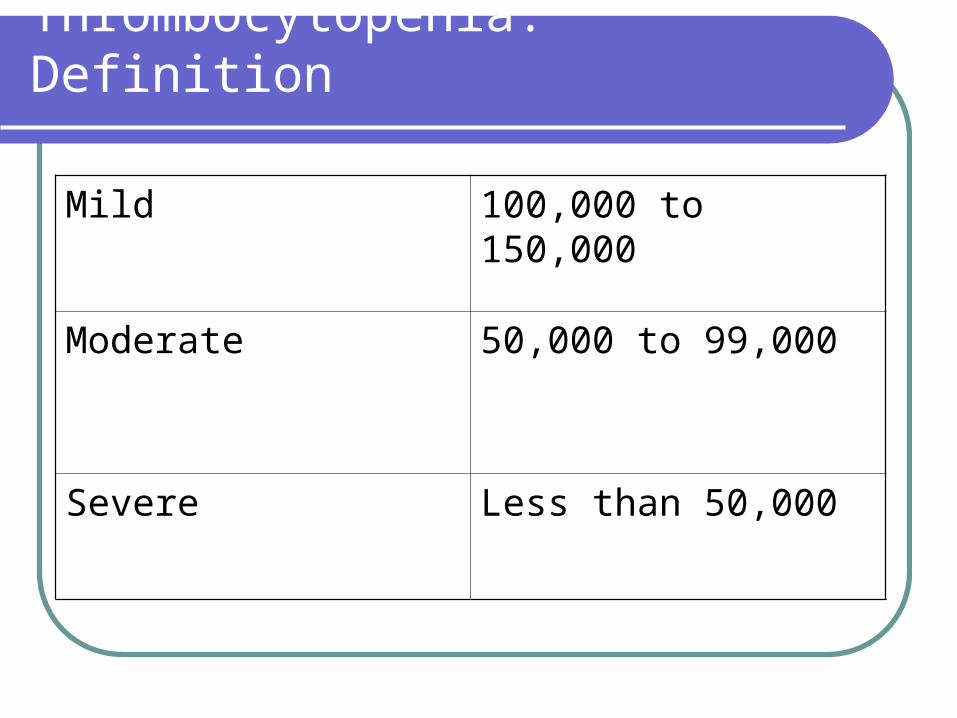
Thrombocytopenia: Definition
Mild 100,000 to 150,000
Moderate 50,000 to 99,000
Severe Less than 50,000
Thrombocytopenia: Epidemiology
Up to 25 % of infants admitted to NICU have the condition.
Mild asymptomatic thrombocytopenia occurs in 1% healthy term infants
Severe thrombocytopenia in term infants rare

Thrombocytopenia
Thrombocytopenia
Increased plateletconsumption
ImpairedMegakaryopoiesis

Thrombocytopenia: assesment
Term or preterm?Other medical conditionsAre there features suggestive of
congenital infection?Congenital anomalies/dysmorphism

Differential Diagnosis
Sick Neonates, Preterm infants, other medical complications.
Hypoxia and acidosis after birth Chronic hypoxia from placental insufficiency Hypothermia Pre-eclampsia Sepsis Congenital viral infections (CMV, rubella) DIC NEC Thrombosis Exchange transfusions
Differential diagnosis
Neonates with physical abnormalities/dysmorphismThrombocytopenia with absent radius SyndFanconi anemiaChromosomal disorders (13,18,21, Turner)Kasabach-Merritt Syndrome
Differential diagnosis
Healthy-appearing infant Occult infectionMaternal autoimmune thrombocytopeniaNeonatal alloimmun thrombocytopeniAmegakaryocytic thrombocytopeniaHereditary macrothrombocytopeniaWiskott-Aldrich Sydrome
Common causes
Pre-eclampsia Magnitude usually correlates with severity of HTN Often have associated neutropenia Nadir at 3-4 days of life, recovering to normal levels
by day 7-10 Rarely severe thrombocytopenia Possible etiology is disruption of hematopoietic
progenitor cell commitment to megakaryopoiesis Assoc conditions from prematurity may exacerbate
condition
Common causes
Bacterial Sepsis
Several mechanisms that include endothelial damage, immune mediated destruction, platelet aggregation and decreased platelet production.
Common causes
Viral infectionsViral neuraminidase causes sialic acid loss
from platelet membranes
Intravascular platelet aggregation
Congenital infections + Splenomegaly
Assoc with Physical abnormalities or dysmorphism
TAR SyndromeAutosomic recessiveSevere thrombocytopenia and skeletal
abnormalities Can be associated with congenital heart
diseasePlatelet nadir during first week generally
improve by 1-3 years of age.

TAR Syndrome
Anomalies/Dysmorphism
Fanconi anemiaAplastic anemia
Thumb anomalies
Anomalies of GU system
Abnormalities/Dysmorphism
Kasabach-Merrit SyndromeHemangiomaCoagulation is activated locally and platelets
are sequestered in the vascular malformation
May not be apparent
Maternal autoimmune Thrombocytopenia
ITP, autoimmune diseasesMaternal antibodies vs. platelet antigens
Glycoprotein IIb/IIIa and Ib/IX
Antibodies cross placenta and bind to these antigens on fetal platelets.
Determine the mother’s platelet count
Neonatal alloimmune thrombocytopenia
A mother lacks a platelet antogen that her fetus inherited from father.
Maternal IgG vs “foreign” antigen on fetal platelets cross the placenta and destroy them.
Most common platelet antigen HPA-1a
Management of immune mediated Thrombocytopenia
IVIG In cases of severe thrombocytopenia or
clinical bleeding1gram/Kg In cases of NAIT Head US and platelet
transfusion with platelets that are free on HPA1 antigen.
Less common etiologies
Congenital amegakarocitic thrombocytopenia (AR)
Heredetary macrothrmbocytopenias (AD)
Wiskott Aldrich Syndrome (WAS protein X)
ImmunedefiencyEczemaThrombocytopenia
Conclusions
Thrombocytopenia is often encountered in newborns, specially sick preterm infants
Initial assessment should consider gestational age, co-morbid conditions, congenital-physical anomalies and dysmorphism.
Thank You
ReferencesNeoReviews.org: Approach to the Newborn
who has thrombocytopenia. Vol.5 2004Curr opinion Obst Gynecol: Platelet
disorders in pregnancy. 2001;13:115-119Avery’s Diseases of the Newborn. Taesch
et Ballard.