arterial elastance and its impact on intrinsic right ventricular function in palliated hypoplastic...
TRANSCRIPT

International Journal of Cardiology 168 (2013) 5385–5389
Contents lists available at ScienceDirect
International Journal of Cardiology
j ourna l homepage: www.e lsev ie r .com/ locate / i j ca rd
Arterial elastance and its impact on intrinsic right ventricular functionin palliated hypoplastic left heart syndrome
Jana Schlangen a,⁎, Gunther Fischer a, Colin Petko a, Jan Hinnerk Hansen a, Inga Voges a, Carsten Rickers a,Hans-Heiner Kramer a, Anselm Uebing a,b
a Department of Congenital Heart Disease and Paediatric Cardiology, University Hospital of Schleswig-Holstein, Campus Kiel, Arnold-Heller-Str.3, Haus 9, 24105 Kiel, Germanyb Adult Congenital Heart Disease Centre, Royal Brompton Hospital, Sydney Street, London SW3 6NP, UK
⁎ Corresponding author. Tel.: +49 431 597 1728; fax: +E-mail address: [email protected] (J
0167-5273/$ – see front matter © 2013 Elsevier Ireland Lhttp://dx.doi.org/10.1016/j.ijcard.2013.08.052
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 13 May 2013Received in revised form 24 July 2013Accepted 18 August 2013Available online 27 August 2013Keywords:Hypoplastic left heart syndromeArterial elastanceVentricular functionCoarctation
Background: Systemic right ventricular (RV) function is a major determinant of long-term outcome in patientswith palliated hypoplastic left heart syndrome (HLHS). Abnormal elastic properties of the reconstructed aortamay negatively impact on ventricular function. We therefore aimed to assess arterial elastance and its relation-ship to systemic RV function in these patients.Methods: Fifty-sixHLHSpatients (median age 5.4 years; range 2.9–14.2 years)were studied at amedianof 2.6 years(range 0.8–12.7 years) after completion of the Fontan circulation with the pressure–volume conductance system.Results: Arterial elastance (Ea) was abnormally high and correlated inversely with RV ejection fraction (r = −0.42,P = 0.001). However, end systolic elastance (Ees) – a load independent measure of intrinsic systolic ventricularfunction – and more so end diastolic stiffness (Eed) were positively correlated with Ea (Ees vs. Ea: r = 0.44,P = 0.001: Eed vs. Ea: r = 0.62, P b 0.0001).
Patients who were treated for significant aortic arch obstruction after surgical palliation showed higher Ea andEed even four years after successful treatment compared to the remainder of the group (Ea: 3.4 ± 1.2 vs.2.8 ± 1.0 mm Hg/ml, P = 0.04 and Eed: 0.67 ± 0.44 vs. 0.45 ± 0.3 mm Hg/ml, P = 0.04).Conclusions: Arterial elastance is abnormally high in palliated HLHS patients and negatively impacts on ejectionfraction but not on intrinsic systolic RV function early after completion of the Fontan circulation. Increased arterialelastance, however, is associatedwith increased RV diastolic stiffness with potential adverse effects on long-termoutcome. Furthermore, arterial elastance and diastolic stiffness are particularly high inpatientswhoneeded treat-ment for aortic arch obstruction.© 2013 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
The right ventricle (RV) is not built to permanently withstand sys-temic afterload and fails prematurely when working as the systemicventricle [1]. Arterial vascular load is the major determinant of ventric-ular afterload and reflects the properties of the vascular bed mainly thedistensibility of the great arteries and peripheral vascular resistance.Arterial vascular load can be measured in a simplified way as arterialelastance (Ea), the steady-state ratio of end systolic pressure and strokevolume obtained from the pressure–volume loop [2]. Ea has beenshown to be a useful marker to assess the impact of arterial vascularload on the human ventricle [3].
Extensive reconstructive surgery to the aortic arch using patch mate-rial is part of the first step of surgical palliation of hypoplastic left heartsyndrome (HLHS) and data from non-invasive imaging studies suggestincreased stiffness with decreased distensibility of the neo-aorta [4,5].We therefore thought to assess Ea in palliatedHLHS patients and to relate
49 431597 1828.. Schlangen).
td. All rights reserved.
this marker of ventricular afterload to ventricular function, especially tointrinsic, load independent function of the systemic RV. Furthermore, be-cause aortic arch obstruction can complicate surgical palliation of HLHSand has been shown to acutely affect RV function we paid particular at-tention to this patient group [6].
2. Materials and methods
2.1. Patients
72 consecutive patients with HLHS after the fenestrated lateral tunnel Fontan proce-dure were recruited to be studied with the pressure–volume conductance system be-tween January 2005 and March 2011. Conductance data should be obtained during aroutine cardiac catheterisation procedure. In 16 patients conductance data could not beanalysed due to either poor signal quality or failure to correctly place the catheter in theRV. Therefore, functional data are available in 56 patients.
All except 3 patients had all their palliative surgical procedures performed at ourcentre by a single surgeon. As stage one the modified Norwood operation was performedusing homograft or bovine pericardial patchmaterial to build the neo-aorta in 14 and 86%of patients, respectively. As stage two a superior cavo-atrio-pulmonary anastomosis (hemiFontan) was created followed by a fenestrated intra-atrial lateral tunnel modification ofthe Fontan operation as stage three. Only two patients received a RV to pulmonary artery

Fig. 1. Pressure–volume loops of a patientwithHLHS after Fontan palliation recorded duringpreload reduction manoeuvre. End systolic elastance (Ees) is described by the slope of theend systolic pressure–volume relationship (Ees: ESP vs. ESV), whilst arterial elastance (Ea)is defined as end systolic pressure divided by stoke volume (Ea = ESP / SV). Diastolic stiff-ness (Eed) is the slope of the end diastolic pressure–volume relationship (Eed: EDP vs. EDV).
Table 1Patient demographics.
Patient characteristics, surgery and aortic arch characteristics
Age, median (range), years 5.4 (2.9–14.2)Gender, male, n (%) 37 (66)Time from TCPC, median (range), years 2.6 (0.8–12.7)NYHA class, I/II/III 43/12/1Medication, D/ACE/BB 7/26/4Number of operation, 3/4/5/6 43/10/1/2Number of patients with treated AAO, n (%) 18 (32)Treatment of aortic arch obstruction
Balloon dilation, 0/1/2/3 39/10/6/1Redo surgery, n (%) 4 (8)Time from last aortic arch intervention, median (range), years 3.9 (1.1–13.0)
Aortic arch measurementsDoppler echocardiographyPeak Doppler velocity, m/s 1.9 ± 0.5
CMRPeak flow velocity, m/s 1.3 ± 0.3
CatheterisationPeak-to-peak gradient, mm Hg 2.5 ± 3.8Coarctation index 0.83 ± 0.13
AAO, aortic arch obstruction; ACE, angiotensin-converting enzyme inhibitors; BB, beta-blocker; CMR, cardiac magnetic resonance; D, diuretics; TCPC, total cavopulmonaryconnection.
5386 J. Schlangen et al. / International Journal of Cardiology 168 (2013) 5385–5389
conduit at the time of the modified Norwood procedure; the remainder received a modi-fied Blalock-Taussig shunt.
In our patient cohort any recurrent aortic arch obstruction with a systolic peak-to-peak gradient≥20 mm Hg or significant anatomical narrowing regardless of the gradientwas treatedwith either balloondilatation or reconstructive surgery. Balloondilatationwasgenerally considered the first-line therapy for coarctation [7].
Informed consent was obtained for each patient. The local research ethics committeeapproved the study protocol.
2.2. Clinical, echocardiographic and angiographic data
Pertinent patient data were collected and included age, gender, follow up time sinceFontan completion and treatment of aortic arch obstruction, New York Heart Association(NYHA) functional class, medication, number of cardiac operations and number ofoperations/interventions to the aortic arch.
Maximal flow velocity in the aortic arch/descending aorta was measured in eachpatient by Doppler echocardiography prior to cardiac catheterisation.
The peak-to-peak pressure gradient between the ascending and descending aortawas measured during the catheter study and the coarctation index was calculated fromangiography by dividing the narrowest diameter of the distal aortic arch by the diameterof the descending thoracic aorta at the level of the diaphragm.
2.3. Cardiac catheterisation and conductance study
Cardiac catheterisation was performed under general anaesthesia and included fullhaemodynamic assessment and biplane (posterior–anterior and lateral) RV angiocardiogra-phy. To acquire RV pressure–volume loops a 4 F combined pressure–conductance catheterwith 12 electrodes (CD Leycom, Zoetermeer, The Netherlands) was placed in the RV via theaorta. Pressure–volume signals were displayed online and digitised at a sample rate of250 Hz (CFL 512, CDLeycom, TheNetherlands) using a value of blood resistivity determinedbefore data acquisition. The pressure signal was calibratedwith a standard calibration pulsefrom the amplifier (Sentron, Roden, TheNetherlands). Conductance derivedRV volumewascalibrated for parallel conductance and gain factorα using the end diastolic (EDV) and endsystolic volume (ESV) obtained frombiplane angiocardiography as previously described [8].Finally, a 25-mm Latex balloon catheter (NuMED, Hopkinton, NY) was placed in the intra-atrial lateral tunnel and prepared to modify preload.
Pressure volume data were recorded for 10–15 s with the respirator temporarilyinterrupted at end expiration during steady state conditions and progressive venousocclusion to generate pressure–volume loops over a wide range of filling pressures.Measurements of pressure and volume relationships were repeated after infusion of10 μg/kg/min of dobutamine for 10 min. All data acquisition runs were repeated intriplicate and all runs containing premature ventricular contractions were excludedfrom analysis.
2.4. Data analysis
Analysis of pressure–volume loops (PV loops) was performedwith custommade soft-ware (Circlab 2011, LUMC, Leiden, the Netherlands). Steady state haemodynamic datawere calculated frompressure–volume loop recordings at baseline and during dobutamineinfusion as means of all beats during a 10-second period.
RV pressure and volume data and derived indices such as cardiac index and ejectionfraction (EF) were assessed. Stroke work (SW) was calculated as the area enclosed by thepressure–volume loop, pressure-volume area (PVA) calculated as the area circumscribedby the end systolic pressure–volume line, the end diastolic pressure–volume relation curve,and the systolic pressure–volume trajectory. The SW/PVA ratio was defined as mechanicalefficiency (EFF).
Indices of intrinsic systolic and diastolic ventricular function were derived frompressure–volume loops recorded during the preload reduction manoeuvre. For systolicventricular function,wedetermined end systolic elastance (Ees) as the slopeof the end sys-tolic pressure–volume relationship (Ees: end systolic pressure; ESP vs. end systolic volume;ESV) the optimal load-independent index of intrinsic systolic function. For diastolic func-tion, diastolic stiffness (Eed), the slope of the end diastolic pressure–volume relationship(Eed: end diastolic pressure; EDP vs. end diastolic volume; EDV) was determined (seeFig. 1).
Arterial elastance (Ea) was calculated as ESP divided by stoke volume; SV(Ea =ESP / SV). Ventriculo-arterial couplingwas described by the quotient of Ea and Ees.
In addition, systemic vascular resistance (SVR)was calculated asmean aortic pressure(mAoP) minus mean right atrial pressure (mRAP) divided by cardiac index (CI) (SVR =(mAoP − mRAP) / CI). Pressures weremeasured directly and cardiac indexwas obtainedfrom conductance data.
A single investigator blinded to the clinical and anatomical data evaluated all functionaldata.
2.5. Statistical analysis
Data are expressed as mean ± SD or median (range) as appropriate. Results for eachvariable were tested for normality using the Kolmogorov–Smirnov method. Comparisonsbetween baseline and dobutamine dataweremadewith Student's t-test for paired samples.Comparisons between patients with and without a history of aortic coarctation were made
with Student's t-test or Mann–Whitney U test as appropriate. Strength of association be-tween variables was measured by linear regression analysis.
For all analyses a P b 0.05 was considered statistically significant. Statistical analysiswas performed with MedCalc, version 11.2 (MedCalc Software, Mariakerke, Belgium).
3. Results
3.1. Patient characteristics
Patient characteristics, surgical data and data on the functional resultof aortic arch reconstruction are summarised in Table 1. Patients werestudied at a median of 2.6 years after Fontan completion. There wasno significant stenosis at the site of the reconstructed aortic arch atthe time of the conductance catheter study.
3.2. Conductance derived data on ventriculo-arterial coupling
Data on RV function at baselinemeasurement and during dobutamineinfusion are given in Table 2.
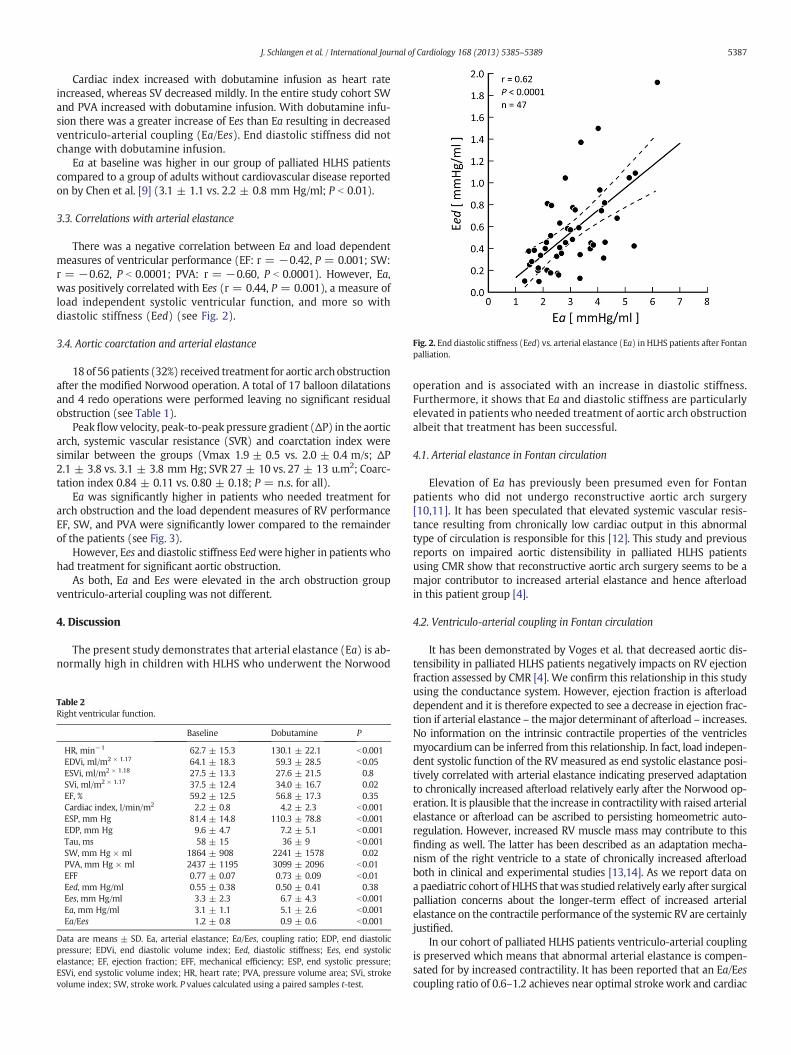
Fig. 2. End diastolic stiffness (Eed) vs. arterial elastance (Ea) in HLHS patients after Fontanpalliation.
5387J. Schlangen et al. / International Journal of Cardiology 168 (2013) 5385–5389
Cardiac index increased with dobutamine infusion as heart rateincreased, whereas SV decreased mildly. In the entire study cohort SWand PVA increased with dobutamine infusion. With dobutamine infu-sion there was a greater increase of Ees than Ea resulting in decreasedventriculo-arterial coupling (Ea/Ees). End diastolic stiffness did notchange with dobutamine infusion.
Ea at baseline was higher in our group of palliated HLHS patientscompared to a group of adults without cardiovascular disease reportedon by Chen et al. [9] (3.1 ± 1.1 vs. 2.2 ± 0.8 mm Hg/ml; P b 0.01).
3.3. Correlations with arterial elastance
There was a negative correlation between Ea and load dependentmeasures of ventricular performance (EF: r = −0.42, P = 0.001; SW:r = −0.62, P b 0.0001; PVA: r = −0.60, P b 0.0001). However, Ea,was positively correlated with Ees (r = 0.44, P = 0.001), a measure ofload independent systolic ventricular function, and more so withdiastolic stiffness (Eed) (see Fig. 2).
3.4. Aortic coarctation and arterial elastance
18 of 56 patients (32%) received treatment for aortic archobstructionafter the modified Norwood operation. A total of 17 balloon dilatationsand 4 redo operations were performed leaving no significant residualobstruction (see Table 1).
Peakflowvelocity, peak-to-peak pressure gradient (ΔP) in the aorticarch, systemic vascular resistance (SVR) and coarctation index weresimilar between the groups (Vmax 1.9 ± 0.5 vs. 2.0 ± 0.4 m/s; ΔP2.1 ± 3.8 vs. 3.1 ± 3.8 mm Hg; SVR 27 ± 10 vs. 27 ± 13 u.m2; Coarc-tation index 0.84 ± 0.11 vs. 0.80 ± 0.18; P = n.s. for all).
Ea was significantly higher in patients who needed treatment forarch obstruction and the load dependent measures of RV performanceEF, SW, and PVA were significantly lower compared to the remainderof the patients (see Fig. 3).
However, Ees and diastolic stiffness Eedwere higher in patients whohad treatment for significant aortic obstruction.
As both, Ea and Ees were elevated in the arch obstruction groupventriculo-arterial coupling was not different.
4. Discussion
The present study demonstrates that arterial elastance (Ea) is ab-normally high in children with HLHS who underwent the Norwood
Table 2Right ventricular function.
Baseline Dobutamine P
HR, min−1 62.7 ± 15.3 130.1 ± 22.1 b0.001EDVi, ml/m2 × 1.17 64.1 ± 18.3 59.3 ± 28.5 b0.05ESVi, ml/m2 × 1.18 27.5 ± 13.3 27.6 ± 21.5 0.8SVi, ml/m2 × 1.17 37.5 ± 12.4 34.0 ± 16.7 0.02EF, % 59.2 ± 12.5 56.8 ± 17.3 0.35Cardiac index, l/min/m2 2.2 ± 0.8 4.2 ± 2.3 b0.001ESP, mm Hg 81.4 ± 14.8 110.3 ± 78.8 b0.001EDP, mm Hg 9.6 ± 4.7 7.2 ± 5.1 b0.001Tau, ms 58 ± 15 36 ± 9 b0.001SW, mm Hg × ml 1864 ± 908 2241 ± 1578 0.02PVA, mm Hg × ml 2437 ± 1195 3099 ± 2096 b0.01EFF 0.77 ± 0.07 0.73 ± 0.09 b0.01Eed, mm Hg/ml 0.55 ± 0.38 0.50 ± 0.41 0.38Ees, mm Hg/ml 3.3 ± 2.3 6.7 ± 4.3 b0.001Ea, mm Hg/ml 3.1 ± 1.1 5.1 ± 2.6 b0.001Ea/Ees 1.2 ± 0.8 0.9 ± 0.6 b0.001
Data are means ± SD. Ea, arterial elastance; Ea/Ees, coupling ratio; EDP, end diastolicpressure; EDVi, end diastolic volume index; Eed, diastolic stiffness; Ees, end systolicelastance; EF, ejection fraction; EFF, mechanical efficiency; ESP, end systolic pressure;ESVi, end systolic volume index; HR, heart rate; PVA, pressure volume area; SVi, strokevolume index; SW, stroke work. P values calculated using a paired samples t-test.
operation and is associated with an increase in diastolic stiffness.Furthermore, it shows that Ea and diastolic stiffness are particularlyelevated in patients who needed treatment of aortic arch obstructionalbeit that treatment has been successful.
4.1. Arterial elastance in Fontan circulation
Elevation of Ea has previously been presumed even for Fontanpatients who did not undergo reconstructive aortic arch surgery[10,11]. It has been speculated that elevated systemic vascular resis-tance resulting from chronically low cardiac output in this abnormaltype of circulation is responsible for this [12]. This study and previousreports on impaired aortic distensibility in palliated HLHS patientsusing CMR show that reconstructive aortic arch surgery seems to be amajor contributor to increased arterial elastance and hence afterloadin this patient group [4].
4.2. Ventriculo-arterial coupling in Fontan circulation
It has been demonstrated by Voges et al. that decreased aortic dis-tensibility in palliated HLHS patients negatively impacts on RV ejectionfraction assessed by CMR [4]. We confirm this relationship in this studyusing the conductance system. However, ejection fraction is afterloaddependent and it is therefore expected to see a decrease in ejection frac-tion if arterial elastance – themajor determinant of afterload – increases.No information on the intrinsic contractile properties of the ventriclesmyocardium can be inferred from this relationship. In fact, load indepen-dent systolic function of the RV measured as end systolic elastance posi-tively correlated with arterial elastance indicating preserved adaptationto chronically increased afterload relatively early after the Norwood op-eration. It is plausible that the increase in contractilitywith raised arterialelastance or afterload can be ascribed to persisting homeometric auto-regulation. However, increased RV muscle mass may contribute to thisfinding as well. The latter has been described as an adaptation mecha-nism of the right ventricle to a state of chronically increased afterloadboth in clinical and experimental studies [13,14]. As we report data ona paediatric cohort of HLHS thatwas studied relatively early after surgicalpalliation concerns about the longer-term effect of increased arterialelastance on the contractile performance of the systemic RV are certainlyjustified.
In our cohort of palliated HLHS patients ventriculo-arterial couplingis preserved which means that abnormal arterial elastance is compen-sated for by increased contractility. It has been reported that an Ea/Eescoupling ratio of 0.6–1.2 achieves near optimal stroke work and cardiac

Fig. 3. Arterial elastance (Ea), load dependent (ejection fraction, EF; stroke work, SW; pressure volume area, PVA) and load independent measures of ventricular function (end systolicelastance, Ees; diastolic stiffness, Eed) in HLHS patients with aortic arch obstruction vs. the remainder of the study cohort.
5388 J. Schlangen et al. / International Journal of Cardiology 168 (2013) 5385–5389
cycle efficiency [15]. Our data are supported by Tanoue et al. who re-ported a simultaneous increase of Ea and Ees six weeks after Fontanoperation using an approximation method from cardiac catheterisationdata but it contradicts the concept of ventricular–vascular mismatch inthe Fontan circulation proposed by Nogaki and colleagues using a theo-retical model [10,11].
Preservation of ventriculo-arterial coupling early after completion ofsurgical HLHS palliation does not necessarily imply absence of ventricu-lar disease in this patient group. Kass coined the term ‘coupling disease’for combined ventriculo-arterial stiffening that occurs with age [16]. Inthe elderly, the combination of increased arterial stiffness and Ees is as-sociated with a limitation of exercise capacity and diastolic dysfunction[17]. We clearly demonstrated in this study that diastolic ventriculardysfunction relates closely to increased arterial elastance in paediatricHLHS patients. Diastolic ventricular dysfunction may well precedesystolic ventricular dysfunction in these patients — a phenomenonwell described for the ageing patient with arterial hypertension [18].Dissociation betweendiastolic and systolic dysfunction is also suggestedby data from the Paediatric Heart Network study that reports echocar-diographic evidence for diastolic dysfunction in 72% of children afterthe Fontan procedurewhilst ejection fractionwas normal in 73% of sub-jects [19]. Longer-term follow up data reporting a period of 15 yearsafter the Fontan operation also support the notion that diastolic functiondeclines earlier than systolic function in this delicate patient group [20].
Increased arterial elastance is unlikely to be the only cause for earlydiastolic dysfunction in palliated HLHS even though this report suggeststhat it is an important contributor.We could recently show that diastolicstiffness is higher in the subgroup of HLHS patients with a large left ven-tricular remnantmaybe because of the impact of the non-ejecting LV onthe stiffness of the interventricular septum that both ventricles share [8].
4.3. The effect of aortic arch obstruction
The deleterious effect of aortic coarctation on ventricular function inHLHS has frequently been reported. Larrazabal et al. recently showedthat timely intervention on recurrent coarctation results in recovery ofRV function, when this is assessed by echocardiography prior to theFontan palliation [6]. Our study is the first to show that even 4 yearsafter successful treatment of aortic arch obstruction arterial elastanceremains elevated with the associated elevation in end systolic and enddiastolic elastance. This is in keeping with data on repaired isolated
coarctation where increased arterial stiffness coupled with increasedventricular elastance has been observed in patients 3 years after suc-cessful surgery [21].
There is evidence that early pathological adjustment of autonomiccardiovascular function with reduced baroreflex sensitivity is alreadyestablished in neonates and infants with isolated coarctation and thatthis may have a causative role in the later development of systemic hy-pertension, as an impairment of baroreceptor sensitivity will result inchronic adrenergic activation [22,23]. It can be speculated that similarpathophysiological mechanisms are initiated in HLHS patients whodevelop aortic arch obstruction. Higher arterial elastance in these patientsmay therefore reflect not only lower aortic compliance but also chronicalterations of the autonomic regulation of the vascular tone. Furtherstudies are required to assess HLHS patients for cardiovascular autonomicdysfunction as this may predispose to the development of systemic hy-pertension. Cardiovascular autonomic dysfunction also carries prognosticinformation in a variety of cardiac diseases [24].Whatever the underlyingmechanism, high arterial elastance and ventricular stiffness are concernsfor the long term outlook of palliatedHLHS patients as any impairment ofdiastolic ventricular function can be expected to be unfavourable particu-larly in the Fontan circulation.
4.4. Study limitations
The fact that arterial elastance and intrinsic ventricular functionneed to be studied invasively meant that we did not obtain similardata in healthy controls. Data on arterial elastance therefore had to becomparedwith published data on adultswithout cardiovascular disease[9].
The conductance method was developed to obtain PV-loops in themore elliptically shaped LV and may be less accurate in the RV. How-ever, several validation studies have shown that it can be applied accu-rately in the RV [25,26].
Angiographic volumes were calculated using cardiac phase and pro-jection specific correction factors obtained from cast studies of sub-pulmonary right ventricles [27]. Whether these correction factors areappropriate for the variably abnormally shaped ventricles of operatedHLHS patients in this study is questionable. However, as we havepreviously reported on a good correlation between RV volumesmea-sured by angiocardiography and cardiac magnetic resonance imaging inthis patient population angiocardiographic volumetry seems sufficiently

5389J. Schlangen et al. / International Journal of Cardiology 168 (2013) 5385–5389
accurate for a methodological study on these patients [8]. Furthermore,any potential error in volume calculation should be consistent withinthe patient population.
5. Conclusion
Arterial elastance, the major determinant of ventricular afterload, isabnormally high in palliated HLHS patients and negatively impacts onejection fraction but not on load independent systolic myocardialfunction. Diastolic stiffness, however, is increased when aortic elastanceis high.
The effects of abnormal arterial elastance on intrinsic systolic func-tion and diastolic stiffness were more pronounced in patients whounderwent successful treatment for aortic coarctation. Thus, prevention,early detection and immediate treatment of aortic arch obstruction areparamount to limit the degree of diastolic dysfunction in HLHS patientundergoing surgical palliation to establish a Fontan circulation.
Funding
This work and the Department of Paediatric Cardiology, Kiel, weresupported by the Fördergemeinschaft Deutsche Kinderherzzentren e.V.
Acknowledgement
The expert technical assistance of T. Hansen and A. Wegmann isgratefully acknowledged.
References
[1] Lopez L, Cohen MS, Anderson RH, et al. Unnatural history of the right ventricle inpatientswith congenitallymalformedhearts. Cardiol Young2010;20(Suppl. 3):107–12.
[2] Sunagawa K, Maughan WL, Burkhoff D, Sagawa K. Left ventricular interaction witharterial load studied in isolated canine ventricle. Am J Physiol 1983;245:H773–80.
[3] Kelly RP, Ting CT, Yang TM, et al. Effective arterial elastance as index of arterial vascularload in humans. Circulation 1992;86:513–21.
[4] Voges I, Jerosch-Herold M, Hedderich J, et al. Maladaptive aortic properties in childrenafter palliation of hypoplastic left heart syndrome assessed by cardiovascularmagneticresonance imaging. Circulation 2010;122:1068–76.
[5] Cardis BM, Fyfe DA, MahleWT. Elastic properties of the reconstructed aorta in hypo-plastic left heart syndrome. Ann Thorac Surg 2006;81:988–91.
[6] Larrazabal LA, Selamet Tierney ES, Brown DW, et al. Ventricular function deterio-rates with recurrent coarctation in hypoplastic left heart syndrome. Ann ThoracSurg 2008;86:869–74 [discussion 869–874].
[7] Hansen JH, Furck AK, Petko C, et al. Use of surveillance criteria reduces interstagemortality after the norwood operation for hypoplastic left heart syndrome. Eur JCardiothorac Surg 2012;41:1013–8.
[8] Schlangen J, FischerG, Steendijk P, et al. Does left ventricular size impact on intrinsic rightventricular function in hypoplastic left heart syndrome? Int J Cardiol 2013;167:1305–10.
[9] Chen CH, Nakayama M, Nevo E, Fetics BJ, Maughan WL, Kass DA. Coupled systolic-ventricular and vascular stiffening with age: implications for pressure regulationand cardiac reserve in the elderly. J Am Coll Cardiol 1998;32:1221–7.
[10] Tanoue Y, Sese A, Imoto Y, Joh K. Ventricular mechanics in the bidirectional glennprocedure and total cavopulmonary connection. Ann Thorac Surg 2003;76:562–6.
[11] Nogaki M, Senzaki H, Masutani S, et al. Ventricular energetics in Fontan circulation:evaluation with a theoretical model. Pediatr Int 2000;42:651–7.
[12] Redington A. The physiology of the Fontan circulation. Prog Pediatr Cardiol2006;22:179–86.
[13] Lorenz CH, Walker ES, Graham Jr TP, Powers TA. Right ventricular performance andmass by use of cine mri late after atrial repair of transposition of the great arteries.Circulation 1995;92:II233–9.
[14] Leeuwenburgh BP, Helbing WA, Steendijk P, Schoof PH, Baan J. Biventricular systolicfunction in young lambs subject to chronic systemic right ventricular pressureoverload. Am J Physiol Heart Circ Physiol 2001;281:H2697–704.
[15] De Tombe PP, Jones S, Burkhoff D, HunterWC, Kass DA. Ventricular stroke work andefficiency both remain nearly optimal despite altered vascular loading. Am J Physiol1993;264:H1817–24.
[16] Kass DA. Ventricular arterial stiffening: integrating the pathophysiology. Hypertension2005;46:185–93.
[17] Kass DA. Age-related changes in ventricular–arterial coupling: pathophysiologicimplications. Heart Fail Rev 2002;7:51–62.
[18] Galderisi M. Diagnosis and management of left ventricular diastolic dysfunction inthe hypertensive patient. Am J Hypertens 2011;24:507–17.
[19] Anderson PA, Sleeper LA, Mahony L, et al. Contemporary outcomes after theFontan procedure: a pediatric heart networkmulticenter study. J Am Coll Cardiol2008;52:85–98.
[20] Nakamura Y, Yagihara T, Kagisaki K, Hagino I, Kobayashi J. Ventricular performancein long-term survivors after Fontan operation. Ann Thorac Surg 2011;91:172–80.
[21] Senzaki H, Iwamoto Y, Ishido H, et al. Ventricular–vascular stiffening in patients withrepaired coarctation of aorta: integrated pathophysiology of hypertension. Circulation2008;118:S191–8.
[22] Polson JW, McCallion N, Waki H, et al. Evidence for cardiovascular autonomic dys-function in neonates with coarctation of the aorta. Circulation 2006;113:2844–50.
[23] Kirchheim HR. Systemic arterial baroreceptor reflexes. Physiol Rev 1976;56:100–77.[24] La Rovere MT, Pinna GD, Raczak G. Baroreflex sensitivity: measurement and clinical
implications. Ann Noninvasive Electrocardiol 2008;13:191–207.[25] Steendijk P. Right ventricular function and failure: methods, models, and mecha-
nisms. Crit Care Med 2004;32:1087–9.[26] White PA, Redington AN. Right ventricular volume measurement: can conductance
do it better? Physiol Meas 2000;21:R23–41.[27] Lange PE, Onnasch D, Farr FL, Heintzen PH. Angiocardiographic right ventricular
volume determination. Accuracy, as determined from human casts, and clinicalapplication. Eur J Cardiol 1978;8:477–501.