arterial trauma
TRANSCRIPT

Extremity Vascular Injuries
Popliteal Arterial InjuriesJoel Arudchelvam
Consultant Vascular and Transplant SurgeonTeaching Hospital Anuradhapura

Extremity Vascular InjuriesInjury to the vessels of the limbs
Common (at THA – 95% of vascular injuries)
Results in limb loss at times loss of life
Economic burden

Causes Road Traffic injuries – 60%Trap GunIatrogenic - 25%
Penetrating / SharpBlunt
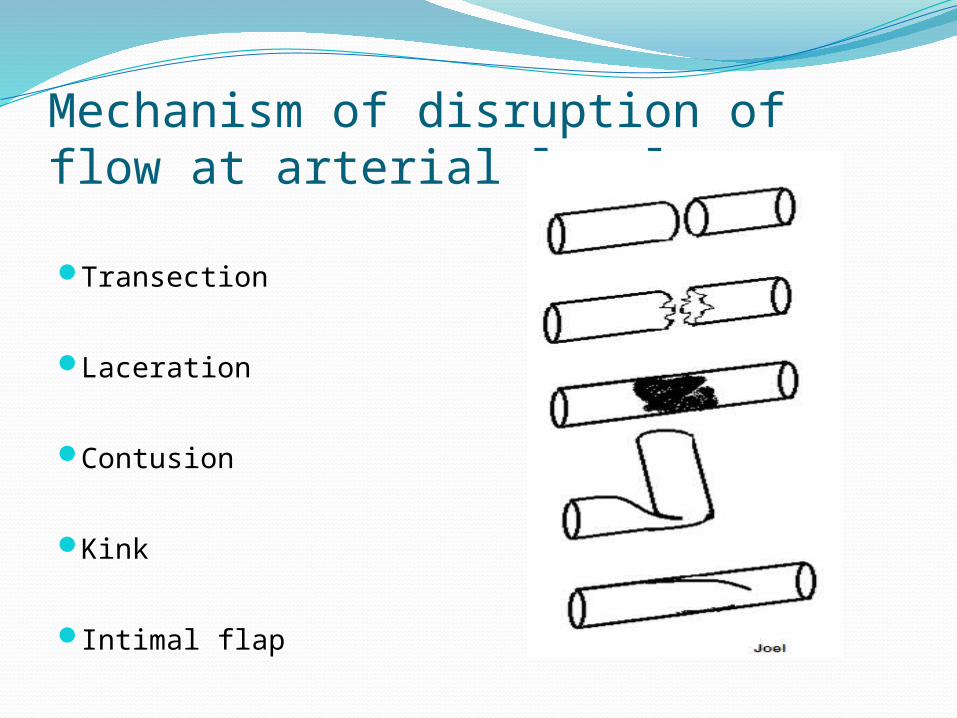
Mechanism of disruption of flow at arterial level
Transection
Laceration
Contusion
Kink
Intimal flap

Clinical featuresHard signs
Active bleeding Thrills, Bruits Distal ischemia
Pain Pallor Pulse – absent Perishing cold Paresthesia /anaesthesia Paresis / paralysis
Expanding hematoma
Soft signs
Hematoma Injury close to a known neurovascular bundle
Injury to Popliteal VesselsCommon
Amputation rates are high.
Our experience At NHSL
Popliteal arterial injury – 32.5% of all injuries –commonest

Vascular injuryVessel Number Mechanism
Iliac artery 2 Blunt
Femoral artery 5 Iatrogenic – 3blunt (RTA) – 2
Femoral vein 1 Penetrating
Popliteal artery 5 blunt (RTA) -4
Popiteal vein 1 Penetrating
Tibial arteries 4 blunt (RTA)
Brachial artery 2 blunt (RTA)

Vascular injuryVessel Number Mechanism
Iliac artery 2 Blunt
Femoral artery 5 Iatrogenic – 3blunt (RTA) – 2
Femoral vein 1 Penetrating
Popliteal artery 5 (25%) blunt (RTA) -4
Popiteal vein 1 Penetrating
Tibial arteries 4 blunt (RTA)
Brachial artery 2 blunt (RTA)
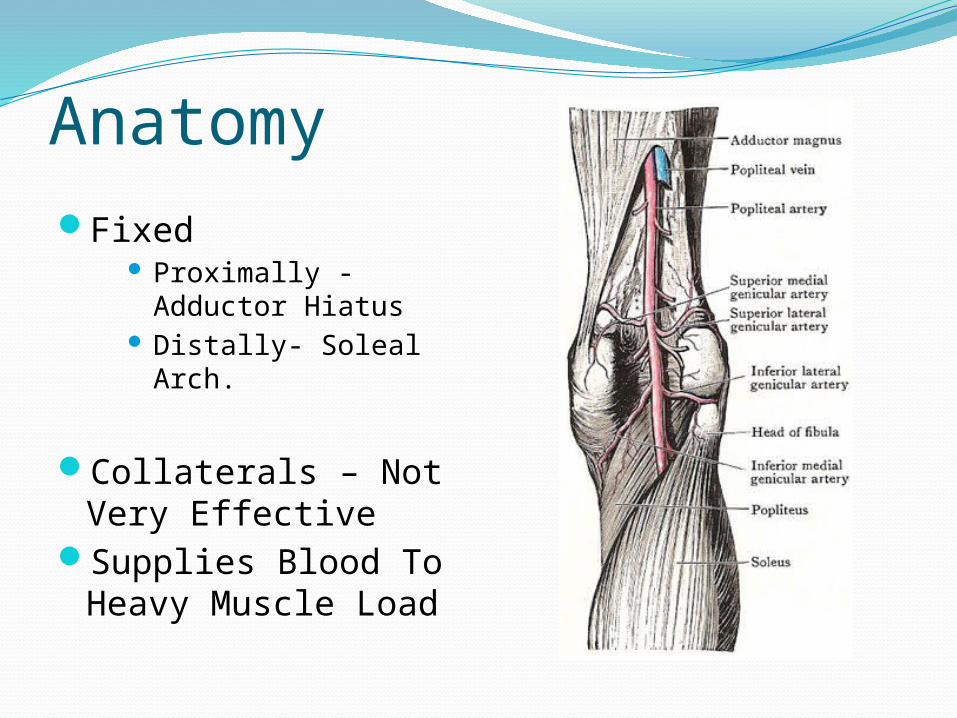
AnatomyFixed
Proximally - Adductor Hiatus
Distally- Soleal Arch.
Collaterals – Not Very Effective
Supplies Blood To Heavy Muscle Load

HISTORY
Ligation – common practice during world War I /
II
Amputation Rate – 72.5%
Korean War / Vietnam Conflict -32%

Reasons givenLack of
Transport Sterility Conditions / Antibiotics Lack of Blood For Transfusion Anesthesia
Prevented Repair on a Large Scale.

PROGNOSTIC FACTORSTime Interval – Common Cause Of Limb Loss In Most
Series In Our Series – THA – 8.2 Hours
MechanismPenetrating Wounds Better Outcomes Than From Blunt
Injury Because Surrounding Tissue Damage To Be Less Severe. Difficult To Diagnose Because Associated Organ And
Tissue Injuries
Associated Injuries - Skeletal Injuries (Knee Dislocation , Popliteal Vein, Nerve, And Soft Tissue And Tendon)

Clinical featuresHard signs
Active bleeding Thrills, Bruits Distal ischemia
Pain Pallor Pulse – absent Perishing cold Paresthesia /anaesthesia Paresis / paralysis
Expanding hematoma
Soft signs
Hematoma Injury close to a known neurovascular bundle

Clinical features Hard signs
Active bleeding Thrills, Bruits
Distal ischemiaPainPallorPulse – absentPerishing coldParesthesia /anaesthesiaParesis / paralysis
Expanding hematoma
Soft signs
Hematoma Injury close to a known neurovascular bundle

Investigations Investigations
• Hard signs • urgent intervention
• Soft signs • Observe• Investigate
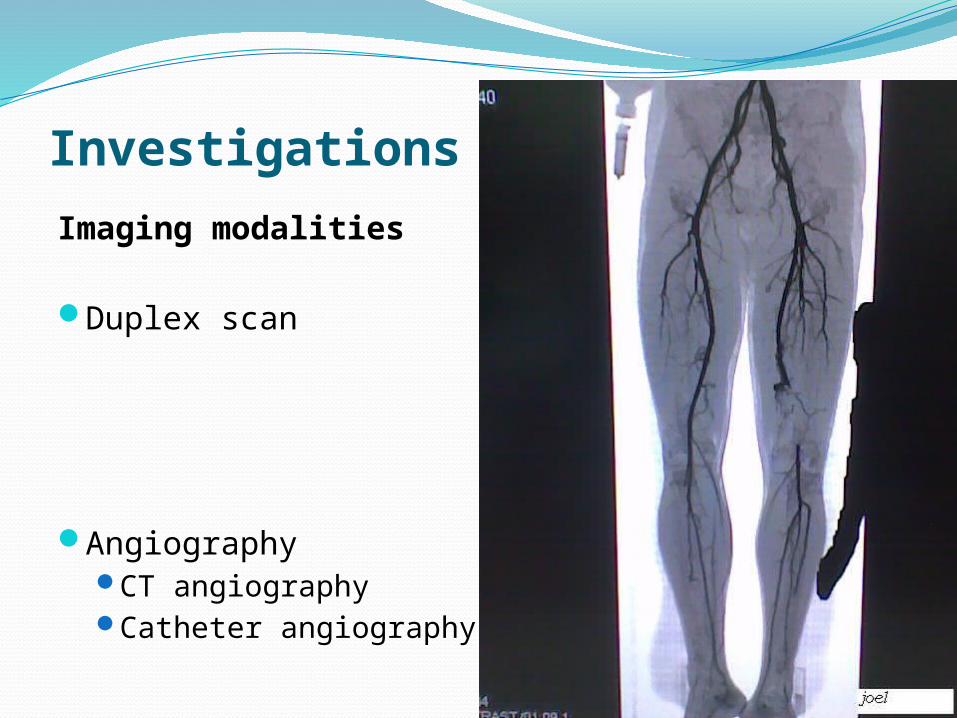
Investigations Imaging modalities
Duplex scan
AngiographyCT angiographyCatheter angiography

Investigations Imaging modalities
Duplex scanDifficult in trauma due to
pain, dressing, wound, patient not cooperating
AngiographyCT angiographyCatheter angiography

Investigations Arteriography
On table

TREATMENTSurgical RepairABCD / resuscitation
Repair as soon as possible
General anesthesia
Cleaning entire leg and be able to visualize the foot and palpate distal pulses.
Contra lateral limb – for venous harvest
Fasciotomy
Medial approach

Surgical RepairArterial Ends TrimmedBalloon ThrombectomySystemic And Distal
HeparinisationInterposition Graft
Unit Experience NHSL - 93.3% RSVG ANP– RSVG Upto Now
? Prosthesis InfectionLower Patency

Surgical Repairlateral injury – patch angioplasty
Our series – none underwentExtra-anatomic bypass
Severe soft tissue injuryOur series – none underwent
Skeletal fixationWhen to fix depends on the urgency of
vascular repair, generally skeletal fixation first is preferred

Compartment SyndromeReduced organ perfusion due to increased
compartment pressure.
Causes,Vascular injuryReperfusionHaematomacontusion

Compartment Syndrome
Treatment – Fasciotomy
Who should do it?

Reperfusion effectsLocal
Reperfusion injury – paradoxical death of already dying muscles after reperfusion
SystemicReperfusion syndrome;
Hypotension ARDS Lactic acidosis Hyperkalemia Kidney shut down

Reperfusion effectsMangement
Fasciotomy
Hydration Mannitol, allopurinolO2InotropesLigation of vessel if not responding to above
measures

Primary Amputation
Extensive soft tissue damage / multiple skeletal
fractures with bone loss “Mangled limb”

Summary
Vascular injury;
ResuscitateAssess viability and extent of injuryAssess need for fasciotomyEarly intervention and post intervention monitoringRehabilitation

Thank You