article a decision-making algorithm for initiation and ... para... · a decision-making algorithm...
TRANSCRIPT

Article
A Decision-Making Algorithm for Initiation andDiscontinuation of RRT in Severe AKI
Mallika L. Mendu,* George R. Ciociolo Jr.,† Sarah R. McLaughlin,‡ Dionne A. Graham,‡ Roya Ghazinouri,§
Siddharth Parmar,† Alissa Grossier,† Rebecca Rosen,† Karl R. Laskowski,† Leonardo V. Riella,* Emily S. Robinson,*David M. Charytan,* Joseph V. Bonventre,* Jeffrey O. Greenberg,† and Sushrut S. Waikar*
AbstractBackground and objectives AKI is an increasingly common and devastating complication in hospitalized pa-tients. Severe AKI requiring RRT is associated with in–hospital mortality rates exceeding 40%. Clinical decisionmaking related to RRT initiation for patients with AKI in the medical intensive care unit is not standardized.
Design, setting, participants, & measurements We conducted a 13-month (November of 2013 to December of2014) prospective cohort study in an academic medical intensive care unit involving the implementation of anAKI Standardized Clinical Assessment and Management Plan, a decision-making algorithm to assist front-lineclinicians caring for patients with AKI. The Standardized Clinical Assessment andManagement Plan algorithmsprovided recommendations about optimal indications for initiating and discontinuing RRT on the basis ofvarious clinical parameters; 176 patientsmanaged by nine nephrologistswere included in the study.We capturedreasons for deviation from the recommended algorithm as well as mortality data.
Results Patients whose clinicians adhered to the Standardized Clinical Assessment and Management Planrecommendation to start RRT had lower in-hospital mortality (42% versus 63%; P,0.01) and 60-day mortality(46% and 68%; P,0.01), findings that were confirmed after multivariable adjustment for age, albumin, anddisease severity. There was a differential effect of Standardized Clinical Assessment and Management Planadherence in low (,50% mortality risk) versus high ($50% mortality risk) disease severity on in-hospital mor-tality (interaction term P=0.02). In patients with low disease severity, Standardized Clinical Assessment andManagement Plan adherence was associated with lower in–hospital mortality (odds ratio, 0.21; 95% confidenceinterval, 0.08 to 0.54; P=0.001), but no significant association was evident in patients with high disease severity.
Conclusions Physician adherence to an algorithm providing recommendations on RRT initiation was associatedwith lower in–hospital mortality.
Clin J Am Soc Nephrol 12: 228–236, 2017. doi: 10.2215/CJN.07170716
IntroductionEach year, .0.5 million United States hospitalizationsare complicated by AKI at a cost of approximately$10 billion (1,2). Severe AKI requiring RRT is one ofthe most ominous of clinical complications, associ-ated with in-hospital mortality rates exceeding 40%(3). Several absolute indications for the initiation ofRRT in AKI are widely accepted: refractory hyperka-lemia or metabolic acidosis, volume overload withpulmonary edema, and uremic pericarditis. Delaysin initiating RRT can result in serious preventablecomplications and even death (4). However, early ini-tiation carries the risk of starting RRT (an invasiveprocedure with non-negligible complications, includ-ing infection and hypotension) in a patient who mayrecover renal function without needing RRT.
Studies that have examined timing of RRT initiationin AKI have used varied biochemical and clinicalparameters to define early versus late initiation andshown mixed results (4–9). Four meta-analyses
concluded that earlier institution of RRT may be as-sociated with a survival benefit (10–13). However, thestudies were heterogeneous in design. Two recentrandomized, controlled trials (RCTs) (14,15) showeddisparate results when randomizing patients to earlyversus late initiation; Zarbock et al. (15) showed abenefit to early initiation, whereas Gaudry et al. (14)showed no benefit. Notably, the studies used differ-ent criteria for RRT initiation. The Kidney DiseaseImprove Global Outcomes (KDIGO) AKI practiceguidelines provide the following recommendation:“Initiate RRT emergently, when life-threateningchanges in fluid, electrolyte, and acid-base balanceexist. Consider the broader clinical context, the pres-ence of conditions that can be modified with RRT andthe trends of laboratory tests—rather than singleBUN and creatinine thresholds alone—when makingthe decision to start RRT” (16).Data regarding RRT discontinuation are even more
limited. A post hoc analysis of a prospective,
*Division of RenalMedicine,†Department ofMedicine, and §Centerfor HealthcareDelivery Sciences,Department ofMedicine, Brighamand Women’sHospital, HarvardMedical School,Boston,Massachusetts; and‡Department ofAnalytics, Institute forRelevant Clinical DataAnalytics, Boston,Massachusetts
Correspondence:Dr. Mallika LakshmiMendu, Brigham andWomen’s Hospital,Division of RenalMedicine, 75 FrancisStreet, MRB-4 Boston,MA 02115. Email:[email protected]
www.cjasn.org Vol 12 February, 2017228 Copyright © 2017 by the American Society of Nephrology
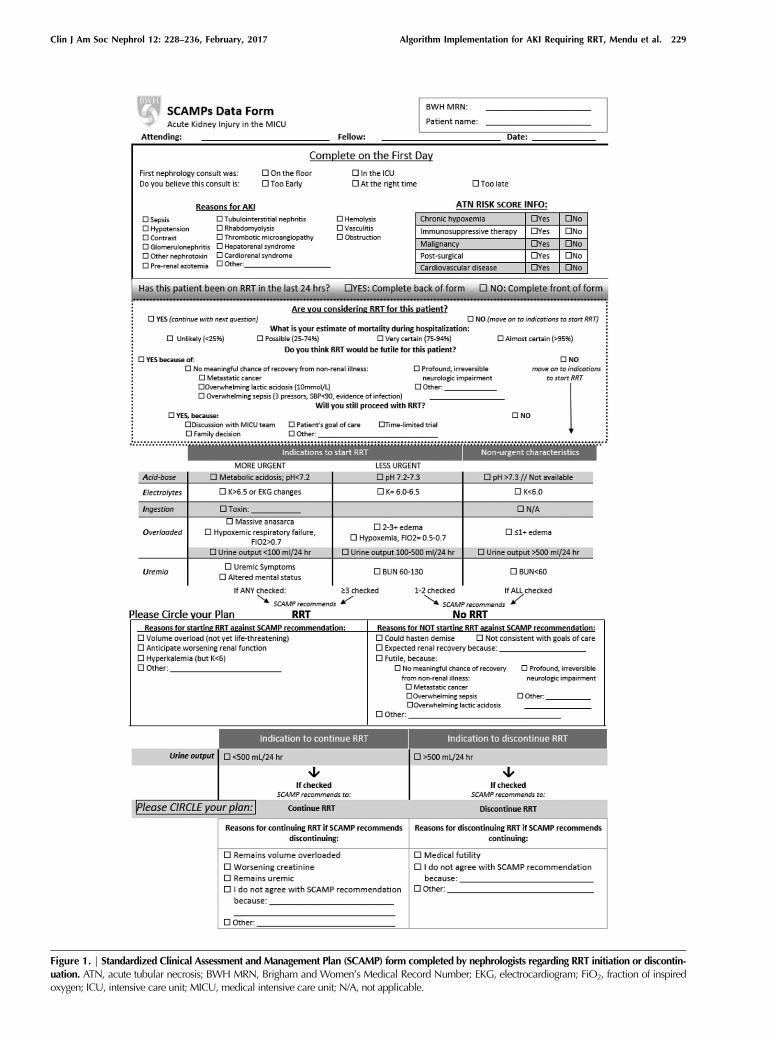
Figure 1. | Standardized Clinical Assessment and Management Plan (SCAMP) form completed by nephrologists regarding RRT initiation or discontin-uation. ATN, acute tubular necrosis; BWH MRN, Brigham and Women’s Medical Record Number; EKG, electrocardiogram; FiO2, fraction of inspiredoxygen; ICU, intensive care unit; MICU, medical intensive care unit; N/A, not applicable.
Clin J Am Soc Nephrol 12: 228–236, February, 2017 Algorithm Implementation for AKI Requiring RRT, Mendu et al. 229

multicenter, observational study of 529 patients who sur-vived RRT showed that urine output at the time of cessa-tion of RRT was the most important predictor of successfuldiscontinuation (17). The KDIGO AKI practice guidelinesprovide the following recommendation: “Discontinue RRTwhen it is no longer required, either because intrinsic kid-ney function has recovered to the point that it is adequateto meet patient needs, or because RRT is no longer consis-tent with the goals of care” (16).To address uncertainties in the care of patients with AKI
requiring RRT, we implemented a structured decision–making algorithm for clinicians managing patients withAKI in the medical intensive care unit (MICU). The algo-rithm prompted clinicians to document criteria relevantfor decisions on RRT initiation and discontinuation. Thealgorithm provided management recommendations,which the clinicians could follow or ignore. We measuredwhether clinicians followed or deviated from the recom-mendations provided, the reasons for deviation, andwhether outcomes differed among patients whose clini-cians adhered versus did not adhere to the algorithm.
Materials and MethodsDescription of the Standardized Clinical Assessment andManagement PlanStandardized Clinical Assessment and Management
Plans (SCAMPs) are a quality improvement approach
that aims to provide insight into undefined areas of careand optimize outcomes through implementation of a stan-dardized care pathway. Oversight of SCAMPs’ productionis provided by the Institute for Relevant Clinical DataAnalytics, a nonprofit, tax-exempt organization that pro-vides the education and resources for the development,implementation, and analysis of SCAMPs at its memberinstitutions. Through an unstructured, iterative process in-volving four intensive care unit (ICU) nephrology attend-ing physicians, we identified several areas of uncertaintyin the care of patients with severe AKI, including criteriafor RRT initiation and discontinuation. Specific criteriawere agreed on by nephrologists on the basis of clinicalexperience and review of existing literature. Structuredforms were developed for clinicians to document decisionmaking. The SCAMP included a phase 1 enrollment periodfrom October 31, 2012 to November 7, 2013, during whichpreliminary data were collected on 142 patients; these dataare not included in this study, because they were incom-plete. Operational issues related to enrollment and datacollection were identified that informed the design ofphase 2. In phase 2, the SCAMP focused specifically onRRT initiation/discontinuation. Figure 1 illustrates theSCAMP form used by clinicians and the criteria included.Figure 2 shows the SCAMP workflow for RRT initiation.
For patients not on RRT, each day, clinicians entered clin-ical data relevant to AKI initiation (4–9) (pH, potassium,suspicion of toxic ingestion, volume overload, fraction of
Figure 2. | Standardized Clinical Assessment and Management Plan (SCAMP) indications to start or not start RRT. N (percentage) refers to thenumber of SCAMP forms (each patient received one SCAMP formper day that he/shewas in themedical intensive care unit andmet criteria for AKI).
230 Clinical Journal of the American Society of Nephrology
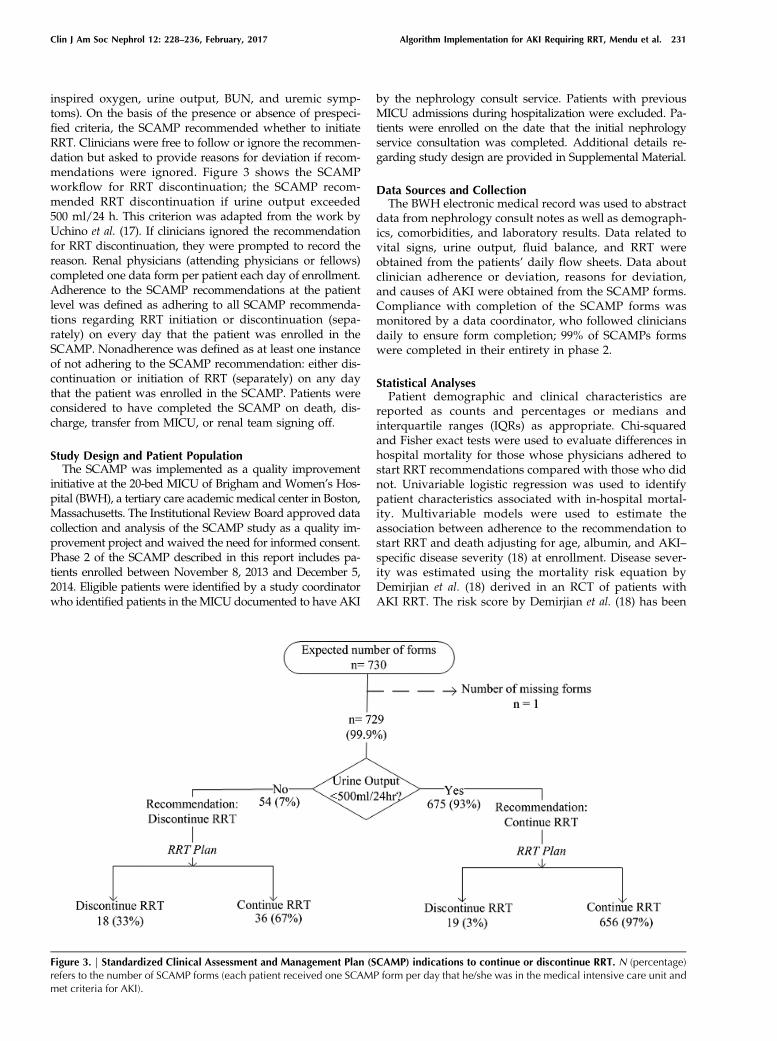
inspired oxygen, urine output, BUN, and uremic symp-toms). On the basis of the presence or absence of prespeci-fied criteria, the SCAMP recommended whether to initiateRRT. Clinicians were free to follow or ignore the recommen-dation but asked to provide reasons for deviation if recom-mendations were ignored. Figure 3 shows the SCAMPworkflow for RRT discontinuation; the SCAMP recom-mended RRT discontinuation if urine output exceeded500 ml/24 h. This criterion was adapted from the work byUchino et al. (17). If clinicians ignored the recommendationfor RRT discontinuation, they were prompted to record thereason. Renal physicians (attending physicians or fellows)completed one data form per patient each day of enrollment.Adherence to the SCAMP recommendations at the patientlevel was defined as adhering to all SCAMP recommenda-tions regarding RRT initiation or discontinuation (sepa-rately) on every day that the patient was enrolled in theSCAMP. Nonadherence was defined as at least one instanceof not adhering to the SCAMP recommendation: either dis-continuation or initiation of RRT (separately) on any daythat the patient was enrolled in the SCAMP. Patients wereconsidered to have completed the SCAMP on death, dis-charge, transfer from MICU, or renal team signing off.
Study Design and Patient PopulationThe SCAMP was implemented as a quality improvement
initiative at the 20-bed MICU of Brigham and Women’s Hos-pital (BWH), a tertiary care academic medical center in Boston,Massachusetts. The Institutional Review Board approved datacollection and analysis of the SCAMP study as a quality im-provement project and waived the need for informed consent.Phase 2 of the SCAMP described in this report includes pa-tients enrolled between November 8, 2013 and December 5,2014. Eligible patients were identified by a study coordinatorwho identified patients in the MICU documented to have AKI
by the nephrology consult service. Patients with previousMICU admissions during hospitalization were excluded. Pa-tients were enrolled on the date that the initial nephrologyservice consultation was completed. Additional details re-garding study design are provided in Supplemental Material.
Data Sources and CollectionThe BWH electronic medical record was used to abstract
data from nephrology consult notes as well as demograph-ics, comorbidities, and laboratory results. Data related tovital signs, urine output, fluid balance, and RRT wereobtained from the patients’ daily flow sheets. Data aboutclinician adherence or deviation, reasons for deviation,and causes of AKI were obtained from the SCAMP forms.Compliance with completion of the SCAMP forms wasmonitored by a data coordinator, who followed cliniciansdaily to ensure form completion; 99% of SCAMPs formswere completed in their entirety in phase 2.
Statistical AnalysesPatient demographic and clinical characteristics are
reported as counts and percentages or medians andinterquartile ranges (IQRs) as appropriate. Chi-squaredand Fisher exact tests were used to evaluate differences inhospital mortality for those whose physicians adhered tostart RRT recommendations compared with those who didnot. Univariable logistic regression was used to identifypatient characteristics associated with in-hospital mortal-ity. Multivariable models were used to estimate theassociation between adherence to the recommendation tostart RRT and death adjusting for age, albumin, and AKI–specific disease severity (18) at enrollment. Disease sever-ity was estimated using the mortality risk equation byDemirjian et al. (18) derived in an RCT of patients withAKI RRT. The risk score by Demirjian et al. (18) has been
Figure 3. | Standardized Clinical Assessment and Management Plan (SCAMP) indications to continue or discontinue RRT. N (percentage)refers to the number of SCAMP forms (each patient received one SCAMP form per day that he/she was in the medical intensive care unit andmet criteria for AKI).
Clin J Am Soc Nephrol 12: 228–236, February, 2017 Algorithm Implementation for AKI Requiring RRT, Mendu et al. 231

shown to have improved performance for mortality pre-diction in patients with AKI compared with SequentialOrgan Failure Assessment and Acute Physiology andChronic Health Evaluation II scores. Laboratory data forthe disease severity score were missing on enrollment in 36of 177 patients (most commonly arterial PO2). In 15 of 36with missing laboratory data, values were available fromthe preceding 48 hours before enrollment and used. In 21of 36 with missing data for laboratory values, we imputednormal values given the likelihood that missing data onvariables, such as pH, indicated low clinical suspicion forabnormal values. All analyses were performed using SAS9.4 (SAS Institute, Cary, NC).
ResultsClinical CharacteristicsTable 1 shows characteristics of the 176 patients included
in the study; one patient was admitted more than once to thehospital, resulting in 177 enrollments. The median age was61 (IQR, 51–70) years old, and 58% were men. Most patientswere white and non-Hispanic (84%). Hypotension (58%),sepsis (51%), and prerenal azotemia (30%) were the mostcommon recorded etiologies of AKI. The median hospitaland MICU lengths of stay were 16.3 (IQR, 7–29.1) daysand 5.9 (IQR, 2.5–13.7) days, respectively.
Indications to Start RRT and Reasons for DeviationFigure 2 depicts clinical decision making regarding initia-
tion of RRT. RRT initiation was recommended in 31% ofSCAMP forms in 176 enrolled patients. In 57% of forms whereRRT was recommended by the SCAMP, clinicians deviatedfrom the suggestions and did not initiate RRT. Table 2 showsthe reasons for these deviations. The most common reason fornot initiating RRT when recommended was expected renalrecovery (48%). Of these patients, 33% ultimately requiredRRT, and 50% died. In 69% of the SCAMP forms, RRT wasnot recommended; virtually all of these recommendations(98%) were followed by the clinicians. The most commonreasons for initiating RRT when not recommended were an-ticipation of worsening renal function and volume overload.
Indications to Discontinue RRT and Reasons for DeviationFigure 3 depicts a flow diagram illustrating clinical de-
cision making regarding discontinuation of RRT. In 7% ofthe SCAMP forms, RRT discontinuation was recom-mended. In 67% of forms where RRT discontinuationwas recommended, clinicians deviated from the sugges-tion and continued RRT. The most common reasons fordeviation were volume overload (69%) and worsening re-nal function or uremia (42%). In 93% of the SCAMP forms,RRT was recommended to continue, and virtually all ofthese recommendations (97%) were followed. The mostcommon reasons for discontinuing RRT against recom-mendations to continue were medical futility (12 of 19)and catheter malfunction (two of 12).
Adherence to and Deviation from the SCAMP Algorithmand OutcomesThe association between adherence to the SCAMP
recommendation to start RRT and in-hospital mortality ispresented in Table 3; 162 patients had SCAMP information
detailed about recommending RRT (of 176 total patients;14 did not). We observed a significantly lower risk of in-hospital mortality in patients whose clinicians adhered toall SCAMP recommendations to start RRT compared withthose whose clinicians did not adhere to the SCAMP on atleast one occasion (42% versus 63%, respectively; P,0.01);the overall mortality of the entire cohort was 50%. There
Table 1. Patient demographics and clinical characteristics
Patient Characteristics,n=177 enrollments N (%)
Men 103 (58)Age, yr, median (IQR) 61 (51–70)RaceWhite 146 (84)Black 16 (9)Hispanic 9 (5)Other 6 (3)
Reasons for AKIa
Hypotension 102 (58)Sepsis 89 (51)Prerenal azotemia 52 (30)Other nephrotoxin 16 (9)Obstruction 7 (4)Contrast 16 (9)Hepatorenal syndrome 7 (4)Thrombotic microangiopathy 6 (3)Cardiorenal syndrome 7 (4)Rhabdomyolysis 6 (3)GN 4 (2)Hemolysis 5 (3)Vasculitis 4 (2)Tubulointerstitial nephritis 4 (2)Other 26 (15)
Chronic health conditionChronic hypoxemia 26 (15)Malignancy 69 (39)Immunosuppresive therapy 57 (32)Cardiovascular disease 47 (27)Postsurgery 15 (8)
Vitals at enrollmentMean arterial pressure, mean+SD 76.8+13.8Serum albumin, mean+SD 2.5+0.6FiO2.0.6 23 (13)Mechanical ventilation 91 (51)
Type (s) of RRTduring enrollmentNone 91 (51)CVVH 44 (25)HD 16 (9)CVVH and HD 26 (15)
Length of stay, median (IQR)MICU, d 5.9 (2.5–13.7)Hospital, d 16.3 (7–29.1)
Probability of 60-d mortality,bmedian (IQR)
0.48 (0.04–0.96)
Values represent N (%) unless otherwise stated. IQR,interquartile range; FiO2, fraction of inspired oxygen; CVVH,continuous venovenous hemofiltration; HD, hemodialysis;MICU, medical intensive care unit.aClinical diagnosis of AKI specified by clinicians caring for thepatient.bRisk equation by Demirjian et al. (18).
232 Clinical Journal of the American Society of Nephrology
was a higher prevalence of cardiovascular disease, me-chanical ventilation, and predicted 60-day mortality inthe nonadherence cohort at baseline (Supplemental Tables1–3). We performed prespecified subgroup analyses usingmultivariable analyses (adjusted for age, albumin, and dis-ease severity at enrollment) in those with higher ($50%predicted mortality) versus lower disease severity (#50%predicted mortality) to account for observed baseline dif-ferences. In multivariable analyses in the lower–diseaseseverity group, adherence to the SCAMP recommendationwas associated with a 79% lower odds of death (95% con-fidence interval [95% CI], 46% to 92%; P=0.001). The re-sults were nearly identical after excluding 32 patients in
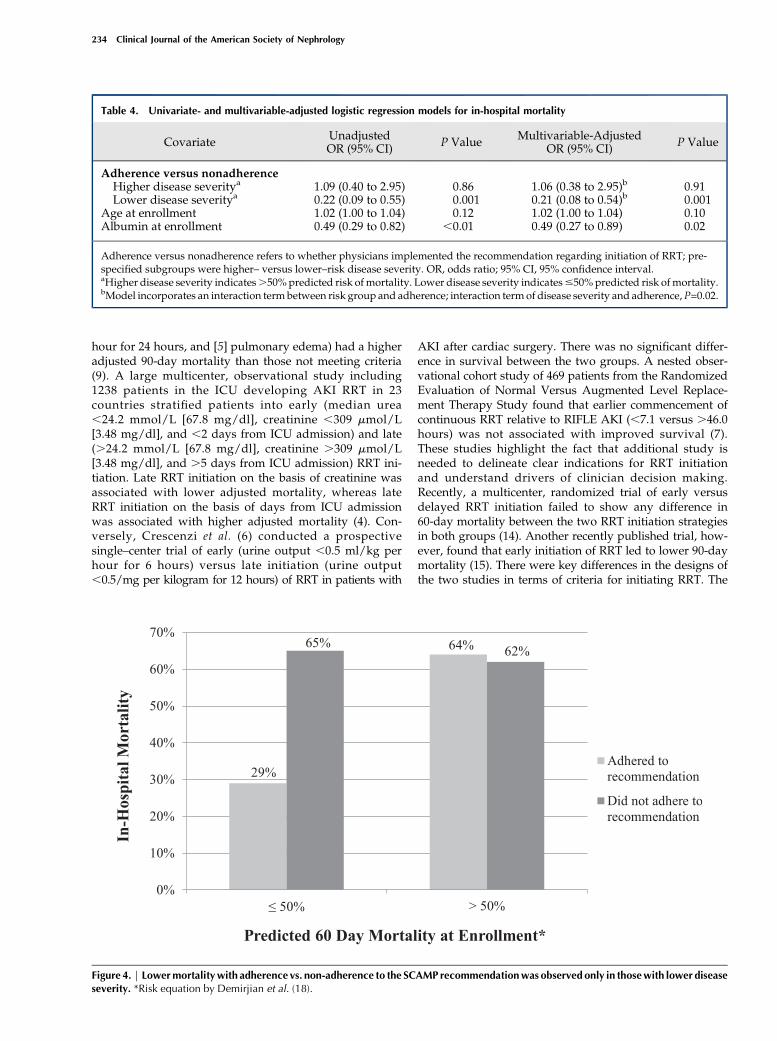
whom futility or goals of care were documented as reasonsfor deviation (odds ratio, 0.21; 95% CI, 0.11 to 0.85;P=0.02). In the higher–disease severity group, we foundno difference in odds of death according to SCAMP adher-ence (odds ratio, 1.06; 95% CI, 0.38 to 2.95; P=0.91) (Table 4).In-hospital mortality according to disease severity andSCAMP adherence are shown in Figure 4. Results weresimilar with adjustment for propensity scores for adher-ence versus nonadherence (data not shown). The meanserum creatinine concentration at enrollment was similaramong patients whose physicians adhered versus did notadhere to the SCAMP recommendation on RRT initiation(3.662.7 and 3.161.5 mg/dl, respectively; P=0.14). Ofnote, the overall in–hospital mortality rate of a separatehistorical control cohort from October of 2010 to July of2012 captured using SCAMP entry criteria and matched byacute tubular necrosis risk score severity was not statisti-cally significantly different (48% in n=183 historical con-trols versus 50% in this study; P=0.56, [data not shown]).There were no differences in outcomes among patients
whose nephrologists adhered or did not adhere to recom-mendations for discontinuing RRT. Our analyses werelimited by sample size, because there were few patientswhose nephrologists deviated from RRT discontinuationrecommendations.
DiscussionThe primary finding of this study on the implementation
of an AKI RRT decision–making algorithm (SCAMP) wasthat mortality was lower among patients whose cliniciansadhered to SCAMP recommendations on RRT initiationcompared with those whose clinicians did not adhere tothe recommendations; this difference was observed in pre-specified analyses of those with lower severity of illness.Our study is unique in that it examines the issue of RRTtiming on the basis of clinical decision making and shedslight on actual clinical practice.Few small observational studies have examined the
timing of RRT for AKI on the basis of varying clinicalparameters. Some have found that earlier initiation resultsin improved outcomes. The Finnish Acute Kidney InjuryStudy found that patients meeting at least one indicationof five ([1] potassium .6 meq/L, [2] pH,7.15, [3]urea .100.8 mg/dl, [4] urine output ,0.3 ml/kg per
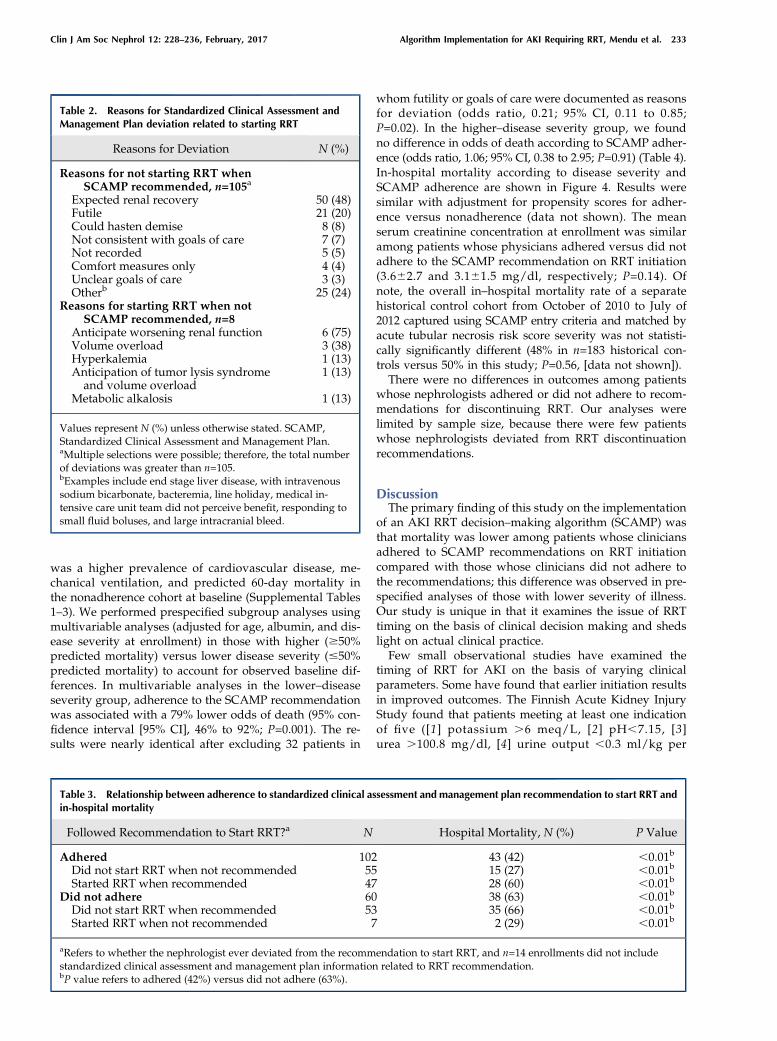
Table 2. Reasons for Standardized Clinical Assessment andManagement Plan deviation related to starting RRT
Reasons for Deviation N (%)
Reasons for not starting RRT whenSCAMP recommended, n=105a
Expected renal recovery 50 (48)Futile 21 (20)Could hasten demise 8 (8)Not consistent with goals of care 7 (7)Not recorded 5 (5)Comfort measures only 4 (4)Unclear goals of care 3 (3)Otherb 25 (24)
Reasons for starting RRT when notSCAMP recommended, n=8
Anticipate worsening renal function 6 (75)Volume overload 3 (38)Hyperkalemia 1 (13)Anticipation of tumor lysis syndromeand volume overload
1 (13)
Metabolic alkalosis 1 (13)
Values represent N (%) unless otherwise stated. SCAMP,Standardized Clinical Assessment and Management Plan.aMultiple selections were possible; therefore, the total numberof deviations was greater than n=105.bExamples include end stage liver disease, with intravenoussodium bicarbonate, bacteremia, line holiday, medical in-tensive care unit team did not perceive benefit, responding tosmall fluid boluses, and large intracranial bleed.
Table 3. Relationship between adherence to standardized clinical assessment and management plan recommendation to start RRT andin-hospital mortality
Followed Recommendation to Start RRT?a N Hospital Mortality, N (%) P Value
Adhered 102 43 (42) ,0.01b
Did not start RRT when not recommended 55 15 (27) ,0.01b
Started RRT when recommended 47 28 (60) ,0.01b
Did not adhere 60 38 (63) ,0.01b
Did not start RRT when recommended 53 35 (66) ,0.01b
Started RRT when not recommended 7 2 (29) ,0.01b
aRefers to whether the nephrologist ever deviated from the recommendation to start RRT, and n=14 enrollments did not includestandardized clinical assessment and management plan information related to RRT recommendation.bP value refers to adhered (42%) versus did not adhere (63%).
Clin J Am Soc Nephrol 12: 228–236, February, 2017 Algorithm Implementation for AKI Requiring RRT, Mendu et al. 233
hour for 24 hours, and [5] pulmonary edema) had a higheradjusted 90-day mortality than those not meeting criteria(9). A large multicenter, observational study including1238 patients in the ICU developing AKI RRT in 23countries stratified patients into early (median urea,24.2 mmol/L [67.8 mg/dl], creatinine ,309 mmol/L[3.48 mg/dl], and ,2 days from ICU admission) and late(.24.2 mmol/L [67.8 mg/dl], creatinine .309 mmol/L[3.48 mg/dl], and .5 days from ICU admission) RRT ini-tiation. Late RRT initiation on the basis of creatinine wasassociated with lower adjusted mortality, whereas lateRRT initiation on the basis of days from ICU admissionwas associated with higher adjusted mortality (4). Con-versely, Crescenzi et al. (6) conducted a prospectivesingle–center trial of early (urine output ,0.5 ml/kg perhour for 6 hours) versus late initiation (urine output,0.5/mg per kilogram for 12 hours) of RRT in patients with
AKI after cardiac surgery. There was no significant differ-ence in survival between the two groups. A nested obser-vational cohort study of 469 patients from the RandomizedEvaluation of Normal Versus Augmented Level Replace-ment Therapy Study found that earlier commencement ofcontinuous RRT relative to RIFLE AKI (,7.1 versus .46.0hours) was not associated with improved survival (7).These studies highlight the fact that additional study isneeded to delineate clear indications for RRT initiationand understand drivers of clinician decision making.Recently, a multicenter, randomized trial of early versusdelayed RRT initiation failed to show any difference in60-day mortality between the two RRT initiation strategiesin both groups (14). Another recently published trial, how-ever, found that early initiation of RRT led to lower 90-daymortality (15). There were key differences in the designs ofthe two studies in terms of criteria for initiating RRT. The
Table 4. Univariate- and multivariable-adjusted logistic regression models for in-hospital mortality
Covariate UnadjustedOR (95% CI) P Value Multivariable-Adjusted
OR (95% CI) P Value
Adherence versus nonadherenceHigher disease severitya 1.09 (0.40 to 2.95) 0.86 1.06 (0.38 to 2.95)b 0.91Lower disease severitya 0.22 (0.09 to 0.55) 0.001 0.21 (0.08 to 0.54)b 0.001
Age at enrollment 1.02 (1.00 to 1.04) 0.12 1.02 (1.00 to 1.04) 0.10Albumin at enrollment 0.49 (0.29 to 0.82) ,0.01 0.49 (0.27 to 0.89) 0.02
Adherence versus nonadherence refers to whether physicians implemented the recommendation regarding initiation of RRT; pre-specified subgroups were higher– versus lower–risk disease severity. OR, odds ratio; 95% CI, 95% confidence interval.aHigher disease severity indicates.50%predicted risk of mortality. Lower disease severity indicates#50%predicted risk of mortality.bModel incorporates an interaction term between risk group and adherence; interaction termof disease severity and adherence,P=0.02.
Figure 4. | Lowermortalitywith adherence vs. non-adherence to the SCAMP recommendationwas observed only in thosewith lower diseaseseverity. *Risk equation by Demirjian et al. (18).
234 Clinical Journal of the American Society of Nephrology

discordance in the findings of these two well-designedRCTs highlights the need for a standardized approach toclinical decision support regarding dialysis initiation.In our study, we implemented a decision-making algo-
rithm on the basis of aggregated findings in the establishedliterature (4–9). On the basis of the limitations of previousstudies and the absence of clear guidelines about RRT ini-tiation and discontinuation, we recognized the importanceof allowing nephrologists to deviate from the SCAMP rec-ommendations and sought to capture these reasons fordeviation. Deviations from the algorithm shed light onthe practical decisions that face nephrologists caring forcritically ill patients with AKI. Notably, in the majorityof patients (57%), the clinicians did not follow the recom-mendation to start RRT when recommended. The mostcommon reason for not starting RRT when clinical param-eters indicate need for initiation was a clinician’s sense ofanticipated renal recovery, which suggests that clinicaljudgement should be balanced with recommended guide-lines. Conversely, the most common reason for continuingRRT when the SCAMP algorithm suggested discontinua-tion was volume overload, implying that our discontinu-ation criterion was ineffective and could be morecomprehensive by incorporating other factors, includingvolume status and creatinine clearance.In addition to shedding light on clinical decision making,
SCAMPs may lead to improved clinical care by providingclinicians with specific recommendations for patient-levelcare at the locus of patient contact and reducing variabilityin clinical practice. Real-time prompts through the SCAMPfor implementation of evidence-based practice may guideclinicians to make the best evidence–based decisions. Ourfinding of improved survival among patients whose clini-cians adhered to the SCAMP recommendation for RRTinitiation is a promising piece of evidence in support ofthe ability of SCAMPs to improve patient care.There are a number of limitations that should temper
enthusiasm about the finding of improved outcomes. First,the most important limitation is residual confounding bydisease severity (measured or unmeasured) or factorsrelated to futility of care: it is possible that lower survivalamong those whose nephrologists declined to initiate RRTwhen recommended reflects higher severity of illness and/or perceived futility of care rather than a beneficial effect ofinitiating RRT. A cluster–stepped wedge RCT of SCAMPimplementation versus usual care would shed light oncausality. Future iterations of the algorithm incorporating,for example, a clear definition of futility are needed. No-tably, outcomes appeared to be improved only amongthose with lower predicted risk of mortality. This suggeststhat high severity of illness may negate benefit of a struc-tured algorithm. Second, the study involved a single aca-demic medical center with a relatively small sample size,and single-center trials, such as this, often find exagger-ated effect sizes. Clinical shared decision making in AKIcan vary on the basis of site of practice and often involvesnon-nephrology intensivists, which further limits the gen-eralizability of this study, particularly to institutions inregions where RRT is prescribed by non-nephrologists.On the basis of these factors, we believe an expansion ofour study to multiple, diverse clinical sites is warrantedbefore general adoption. Third, a potential confounding
factor is that nephrologists who chose to adhere to theSCAMP recommendation may have been inherently betterclinicians and therefore, had better patient outcomes com-pared with those that did not adhere to the SCAMP.Fourth, the possibility of the Hawthorne effect, in whichknowledge of study participation leads to behaviorchanges affecting the outcome of interest, should not beignored. Fifth, implementation of the SCAMP requiredtracking of patients and reminders to clinicians to usethe decision-making algorithm, calling into question thefeasibility of implementation outside of a quality improve-ment study. Implementation of the SCAMP algorithminto an electronic medical record template may facilitateclinical use.In conclusion, our study provides preliminary evidence
that an RRT decision–making algorithm may lead to im-proved outcomes in severe AKI. Additional study isneeded to elucidate the benefit that clinical decision sup-port for RRT initiation could provide in improving clinicaloutcomes.
AcknowledgmentsM.L.M. and S.S.W. take responsibility for the integrity of the data
and the accuracy of the data analysis.
DisclosuresNone.
References1. Chertow GM, Burdick E, Honour M, Bonventre JV, Bates DW:
Acute kidney injury, mortality, length of stay, and costs in hos-pitalized patients. J Am Soc Nephrol 16: 3365–3370, 2005
2. Waikar SS, Curhan GC, Wald R, McCarthy EP, Chertow GM:Declining mortality in patients with acute renal failure, 1988 to2002. J Am Soc Nephrol 17: 1143–1150, 2006
3. Waikar SS, Liu KD, Chertow GM: Diagnosis, epidemiology andoutcomes of acute kidney injury. Clin J Am Soc Nephrol 3: 844–861, 2008
4. Bagshaw SM, Uchino S, Bellomo R, Morimatsu H, Morgera S,Schetz M, Tan I, Bouman C, Macedo E, Gibney N, Tolwani A,Oudemans-van StraatenHM, RoncoC, Kellum JA; Beginning andEnding Supportive Therapy for the Kidney (BEST Kidney) Inves-tigators: Timing of renal replacement therapy and clinical out-comes in critically ill patients with severe acute kidney injury.J Crit Care 24: 129–140, 2009
5. ChouYH,HuangTM,WuVC,WangCY, ShiaoCC, Lai CF, TsaiHB,Chao CT, Young GH, WangWJ, Kao TW, Lin SL, Han YY, Chou A,Lin TH, Yang YW, Chen YM, Tsai PR, Lin YF, Huang JW, ChiangWC,ChouNK,KoWJ,WuKD,Tsai TJ;NSARFStudyGroup: Impactof timing of renal replacement therapy initiation on outcome ofseptic acute kidney injury. Crit Care 15: R134, 2011
6. CrescenziG, Torracca L, PierriMD, Rosica C,MunchC, CapestroF: ‘Early’ and ‘late’ timing for renal replacement therapy in acutekidney injury after cardiac surgery: A prospective, interventional,controlled, single-centre trial. Interact Cardiovasc Thorac Surg20: 616–621, 2015
7. Jun M, Bellomo R, Cass A, Gallagher M, Lo S, Lee J; RandomizedEvaluation of Normal Versus Augmented Level of ReplacementTherapy (RENAL) Study Investigators: Timing of renal re-placement therapy and patient outcomes in the randomizedevaluation of normal versus augmented level of replacementtherapy study. Crit Care Med 42: 1756–1765, 2014
8. Lee J, Cho JH, Chung BH, Park JT, Lee JP, Chang JH, Kim DK, KimS: Classical indications are useful for initiating continuous renalreplacement therapy in critically ill patients. Tohoku J Exp Med233: 233–241, 2014
9. Vaara ST, ReinikainenM,Wald R, Bagshaw SM, Pettila V; FINNAKIStudyGroup: Timing of RRT based on the presence of conventionalindications. Clin J Am Soc Nephrol 9: 1577–1585, 2014
Clin J Am Soc Nephrol 12: 228–236, February, 2017 Algorithm Implementation for AKI Requiring RRT, Mendu et al. 235

10. Wang X, Jie Yuan W: Timing of initiation of renal replacementtherapy in acute kidney injury: A systematic review and meta-analysis. Ren Fail 34: 396–402, 2012
11. Pannu N, Klarenbach S, Wiebe N, Manns B, Tonelli M; AlbertaKidneyDiseaseNetwork: Renal replacement therapy in patientswithacute renal failure: A systematic review. JAMA 299: 793–805, 2008
12. Seabra VF, Balk EM, Liangos O, Sosa MA, Cendoroglo M, JaberBL: Timing of renal replacement therapy initiation in acute renalfailure: A meta-analysis. Am J Kidney Dis 52: 272–284, 2008
13. Karvellas CJ, Farhat MR, Sajjad I, Mogensen SS, Leung AA, WaldR, Bagshaw SM: A comparison of early versus late initiation ofrenal replacement therapy in critically ill patients with acutekidney injury: A systematic review and meta-analysis. Crit Care15: R72, 2011
14. Gaudry S, Hajage D, Schortgen F, Martin-Lefevre L, Pons B,Boulet E, Boyer A, ChevrelG, LerolleN, CarpentierD, de Prost N,Lautrette A, Bretagnol A,Mayaux J, Nseir S,Megarbane B, ThirionM, Forel JM, Maizel J, Yonis H, Markowicz P, Thiery G, Tubach F,Ricard JD, Dreyfuss D,; AKIKI Study Group: Initiation strategiesfor renal-replacement therapy in the intensive care unit. N Engl JMed 375: 122–133, 2016
15. Zarbock A, Kellum JA, Schmidt C, Van Aken H, Wempe C,Pavenstadt H, Boanta A, Gerß J, Meersch M: Effect of early vsdelayed initiation of renal replacement therapy on mortality incritically ill patients with acute kidney injury: The ELAIN ran-domized clinical trial. JAMA 315: 2190–2199, 2016
16. KDIGO: KDIGO Clinical Practice Guideline for Acute KidneyInjury, 2015. Available at: http://www.kdigo.org/clinical_practice_guidelines/pdf/KDIGO%20AKI%20Guideline.pdf. AccessedJuly 2, 2015
17. Uchino S, Bellomo R, Morimatsu H, Morgera S, Schetz M, Tan I,BoumanC,Macedo E, GibneyN, Tolwani A, StraatenHO,RoncoC, Kellum JA: Discontinuation of continuous renal replacementtherapy: A post hoc analysis of a prospective multicenter obser-vational study. Crit Care Med 37: 2576–2582, 2009
18. Demirjian S, Chertow GM, Zhang JH, O’Connor TZ, Vitale J,Paganini EP, Palevsky PM; VA/NIH Acute Renal Failure TrialNetwork: Model to predict mortality in critically ill adults withacute kidney injury. Clin J Am Soc Nephrol 6: 2114–2120, 2011
Received: July 6, 2016 Accepted: November 1, 2016
Published online ahead of print. Publication date available at www.cjasn.org.
See related editorial, “Guiding Physician Decisions for InitiatingDialysis for AKI: Is Progress on the Horizon?,” on pages 217–219.
This article contains supplemental material online at http://cjasn.asnjournals.org/lookup/suppl/doi:10.2215/CJN.07170716/-/DCSupplemental.
236 Clinical Journal of the American Society of Nephrology