artificial skin and artificial cartilage
TRANSCRIPT
ARTIFICIAL SKIN
PRESENTED BYPWADUBASAHIYI COSTON PWAVODI 20143883 MSC.
FELIX CHIBUZO OBI 20144610 MSC.MICHAEL OLABOYE AMUSAN 20103181
ARTIFICIAL ORGANSDEPARTMENT OF BIOMEDICAL
ENGINEERING..
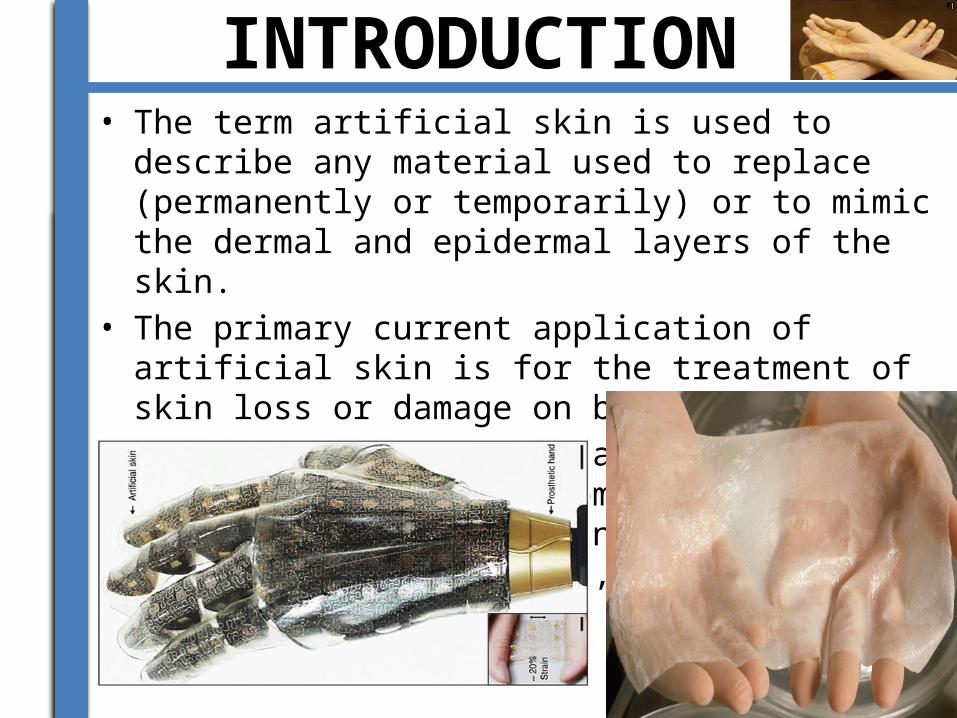
INTRODUCTION• The term artificial skin is used to describe any material used
to replace (permanently or temporarily) or to mimic the dermal and epidermal layers of the skin.
• The primary current application of artificial skin is for the treatment of skin loss or damage on burn patients.
• Alternatively however, artificial skin is now being used in some places to treat patients with skin diseases, such as diabetic foot ulcers, and severe .[1]
ANATOMICAL OVERVIEW OF THE SKIN
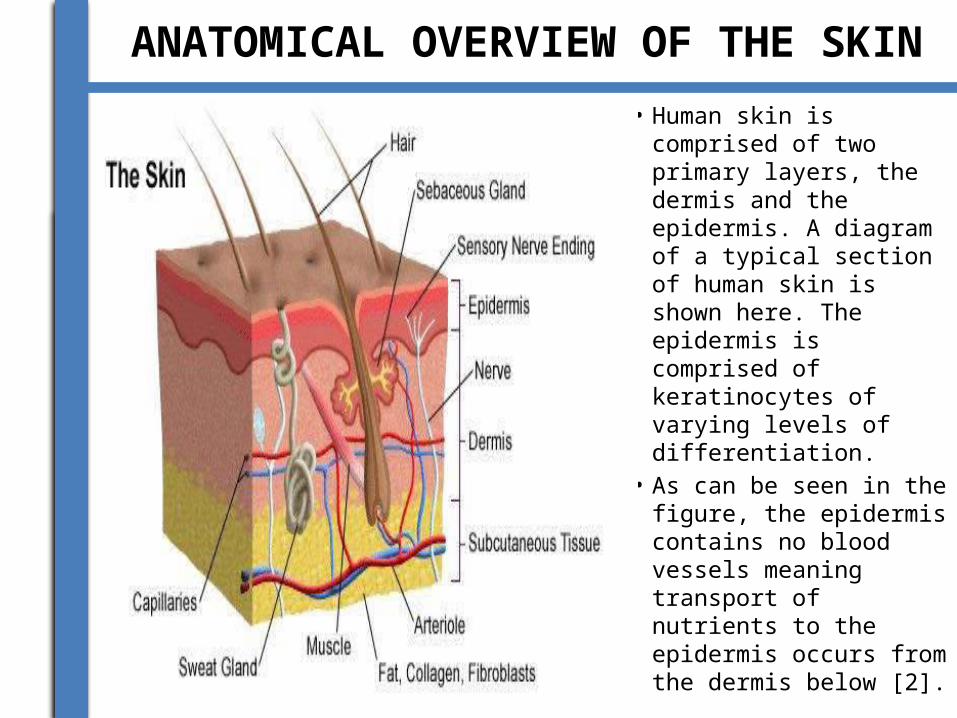
• Human skin is comprised of two primary layers, the dermis and the epidermis. A diagram of a typical section of human skin is shown here. The epidermis is comprised of keratinocytes of varying levels of differentiation.
• As can be seen in the figure, the epidermis contains no blood vessels meaning transport of nutrients to the epidermis occurs from the dermis below [2].
BRIEF HISTORY OF THE ARTIFICIAL SKIN
• 3000-2500BC, India: Skin is allegedly transplanted by Hindus from the buttocks to repair mutilated ears and noses.
• 1442, Italy: An allogenous skin graft was performed by Branca de Branca who used a man’s arm skin to transplant the nose of the man’s slave onto himself.
• 1871, England: Pollock proposes skin grafts for burn treatment.
• 1998, United States: First tissue engineered skin (Apligraf) is approved by the FDA.
• 2001, United States: Dermagraft, Orcel, Composite Cultured Skin are FDA approved [4].
• 2002, United States: Integra is FDA approved for treatment of severe burns [4].
PROCESSES INVOLVED IN THE MANUFACTURE OF THE ARTIFICIAL SKIN
Skin is usually donated by other donors. • Fibroblasts are removed from the donated skin and
are frozen until they are needed. • The fibroblasts are placed on a polymeric mesh
scaffolding, gather oxygen, and grow new cells. • The cells are then transferred to a culture
system.After 4 weeks the polymer mesh dissolves and leaves behind a new layer of dermal skin.
• When the growth cycle is completed, they add more nutrients. Keratinocytes are added to the collagen and are
exposed to air to form epidermal layers. • The skin is now completed and is stored in
sterile contains until ready to use.
Skin Grafts • Skin grafts are required for patients with skin damage that is
too significant for self-repair. As stated before, one of the primary requirements for artificial skin is for the treatment of severe burn victims. [2
• Skin grafts are also often done on patients with ulcers, skin loss from cancer removal, and plastic surgery [1]
• The skin required for a skin graft can be obtained from three sources; the patient themselves (autograft), another human (allograft), or from animals such as pigs or cows (xenografts)[2]. Allografts and xenografts can only be used as temporary wound coverings as they are typically rejected within 7 to 10 days or 3 to 5 days respectively [2].
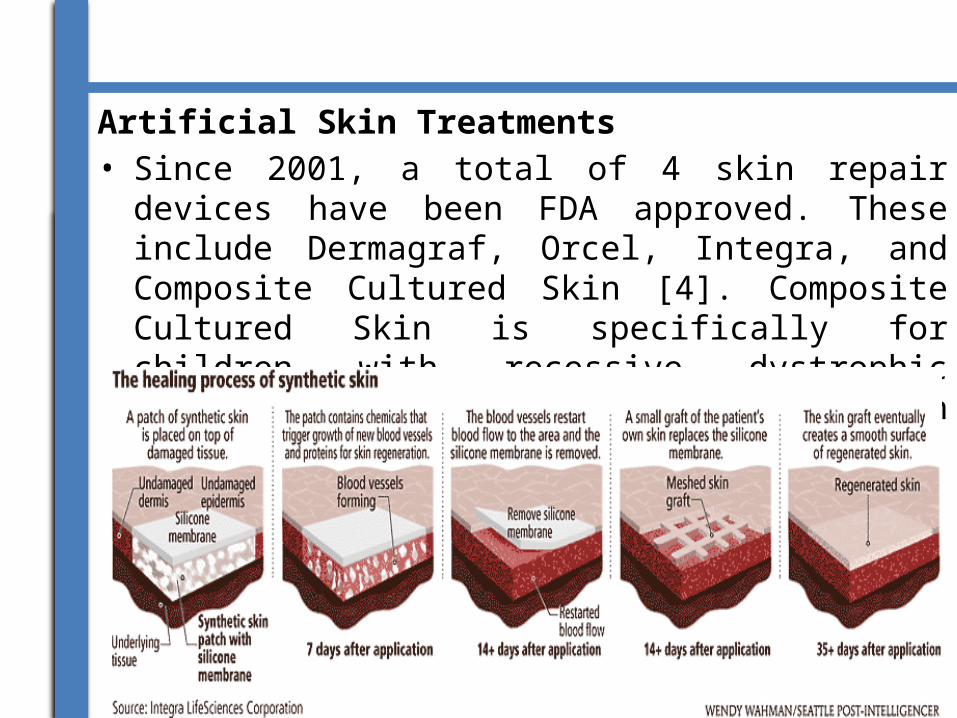
Artificial Skin Treatments • Since 2001, a total of 4 skin repair devices have been FDA
approved. These include Dermagraf, Orcel, Integra, and Composite Cultured Skin [4]. Composite Cultured Skin is specifically for children with recessive dystrophic epidermolysis bullosa and also contain living cells.
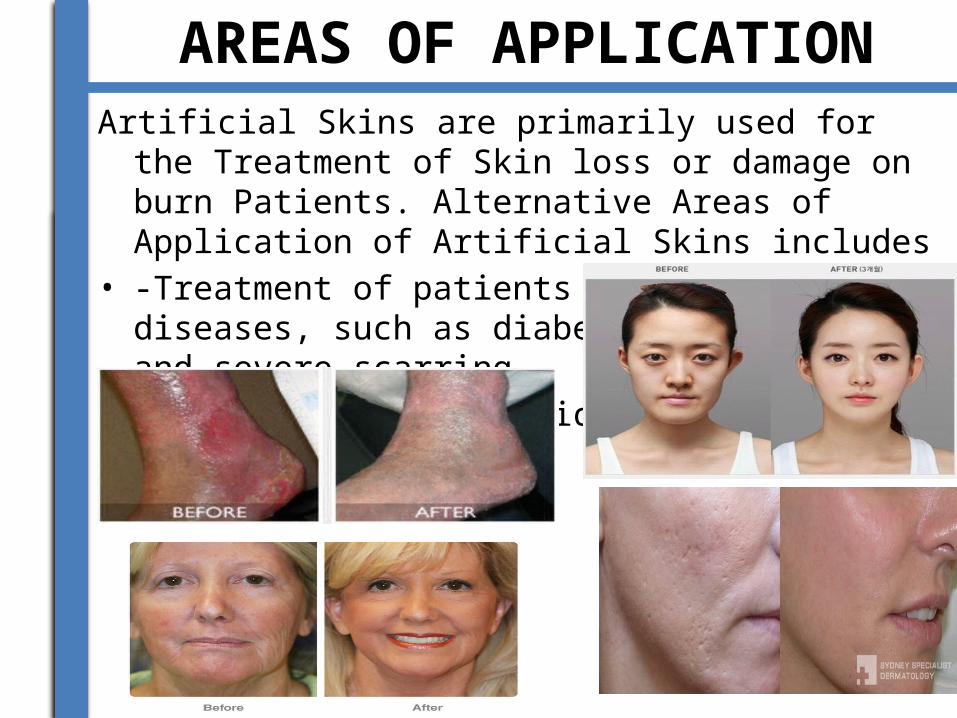
AREAS OF APPLICATIONArtificial Skins are primarily used for the Treatment of Skin
loss or damage on burn Patients. Alternative Areas of Application of Artificial Skins includes
• -Treatment of patients with skin diseases, such as diabetic foot ulcers, and severe scarring.
• - Plastics and Cosmetic Surgery.

ADVANTAGES AND DISADVANTAGES
ADVANTAGES• -Chances of survival for burn patients.• -Artificial skin seals the wound preventing fluid loss and bacteria
from entering through the wound.• - The fear of Stigmatization of the Patient is eliminated
DISADVANTAGES• -Risks of Infection and Rejection by the Patients
• -Lack of vascularization to the implanted skin or skin cells can lead to cell death which provides a breeding ground for bacteria.
• -Loss of Sensitivity• -Cut of Blood Supply.• -Complication could arise due to Skin Adhesion and/or fluid
buildup between the wounded site and the transplanted skin.• - Artificial Skins are very expensive.
RECENT DEVELOPMENTS OF THE ARTIFICIAL SKIN/ONGOING RESEARCH
• Though artificial skin has aided significantly in skin regeneration, there remain several areas for improvement. Ongoing Research attempt to produce bacteria-resistant skin cell cultures that can be used in artificial skin. Ideally, this would allow in vitro replication of a patient’s own genetically modified skin cells. These cells could then be put into the artificial matrix for bacteria-free growth.
• Another current trend in Artificial is the creation of Electronic Skin. Scientist are working towards the Incorporation of flexible pressure transducers and Bioreceptors to the Artificial Skin, these will give a sense of Touch to the Patients.
• Outside of artificial biological skin, synthetic skin is being developed in hopes of enabling the sensation of touch to non-living structures. Flexible pressure transducers may eventually allow us to create an electronic “skin” with signals to mimic the sense of touch. This has applications in robotics including advanced prosthetic limbs [8].
RECENT DEVELOPMENTS OF THE ARTIFICIAL SKIN/ONGOING RESEARCH
• Other advances have been made in the application of cells to the matrices. Dr. Fiona Woods has produced a “spray on skin” called Cellspray. This method takes healthy cells from the patient and creates a suspension culture of the cells. The cells are then distributed by spraying them evenly across the matrix. It is believed that this method will be beneficial because the suspension cell culture can be produced much faster (5 days) than traditional methods which require formation of a sheet of cells (21 days). Though this procedure has not been through clinical trials, it was controversially used on burn victims in conjunction with traditional methods in the Bali bombings in 2004. Further testing is required before this treatment can officially be deemed successful.

CONCLUSION• The ultimate goals of current artificial skin
technologies are to provide protection from infection, dehydration, and protein loss after severe skin loss or damage.
REFERENCES
• [1] Dantzer, E., Queruel, P., Salinier, L., Palmier, B., & Quinot, J. F. (2001). Integra, a new surgical alternative for the treatment of massive burns. Clinical evaluation of acute and reconstructive surgery: 39 case. Annales De Chirurgie Plastique Esthétique, 46(3), 173-189. http://www.ncbi.nlm.nih.gov/pubmed/11447623
• [2] Roos, D. (2012). Skin grafts. Retrieved 02/29, 2012, from http://health.howstuffworks.com/skin-care/information/anatomy/skin-graft.htm
• [3] Heman, A. R. (2002). The history of skin grafts. Retrieved 02/29, 2012, from http://findarticles.com/p/articles/mi_m0PDG/is_3_1/ai_110220336/
ARTIFICIAL CARTILAGE
INTRODUCTION• Articular cartilage is a highly organized avascular tissue
composed of chondrocytes embedded within an extracellular matrix of collagens, proteoglycans and noncollagenous proteins. Its primary function is to enable the smooth articulation of joint surfaces, and to cushion compressive, tensile and shearing forces. Hyaline cartilage has one of the lowest coefficients of friction known for any surface to surface contact.
• Cartilage is unique as it is an avascular, aneural tissue, in which cells survive for a lifetime, without intercellular connections.Owing to its sophisticated composition, its high water content and its ability to withstand hydrostatic pressurization, cartilage is capable of transferring enormous forces relatively evenly from one subchondral bone plate to the other.

OVERVIEW OF THE ANATOMY OF THE CARTILAGE
• Cartilage is a flexible connective tissue found in many areas in the bodies of humans and other animals, including the joints between bones, the rib cage, the ear, the nose, the bronchial tubes and the intervertebral discs. It is not as hard and rigid as bone but is stiffer and less flexible than muscle.
• ARTICULAR CARTILAGE?
Hyaline articular cartilage is a complex structure, developed and progressively refined over hundreds of millions of years. Articular cartilage provides smooth articulation under variable loads and impaction for very long periods of time. It serves as the load-bearing material of joints, which has excellent friction, lubrication and wear characteristics. The cartilage thickness varies significantly across articular surfaces of the same joint. Normal hyaline cartilage has a glossy, bluish white, homogenous appearance, firm consistency and some elasticity. .
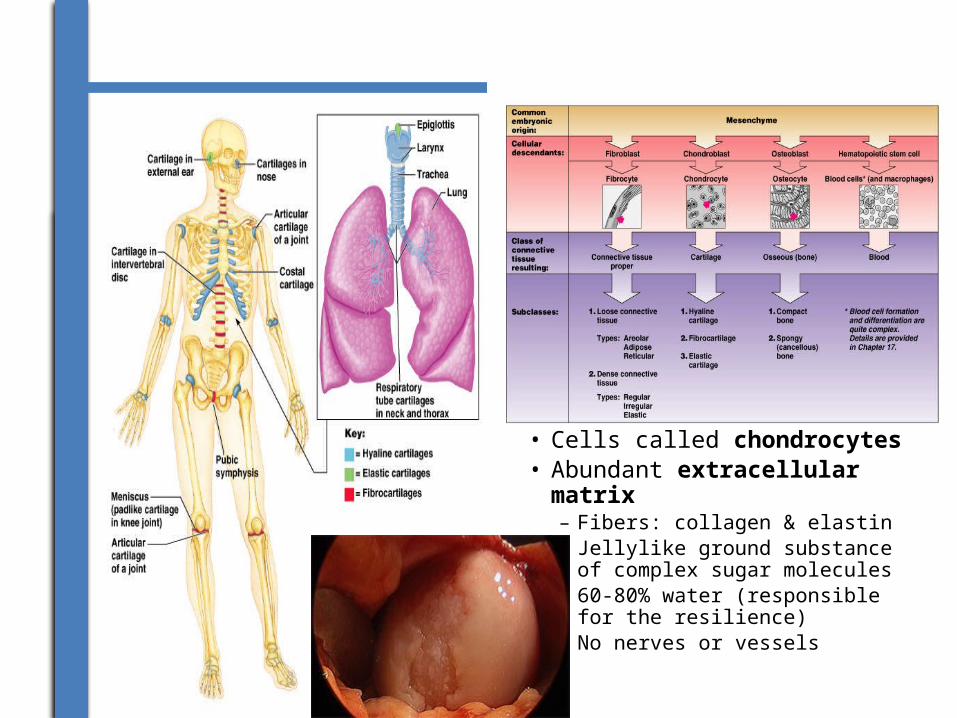
• Cells called chondrocytes• Abundant extracellular
matrix– Fibers: collagen & elastin– Jellylike ground substance of
complex sugar molecules– 60-80% water (responsible
for the resilience)– No nerves or vessels
BRIEF HISTORY OF THE ARTIFICIAL CARTILAGE
• The history up to 1900 is told chronologically, divided into (1) recognition of the tissue, (2) structure, and (3) chemistry. The twentieth century is sketched with a timeline of discoveries that at the time were important and a bibliography of journal review articles.
• By 1900 the avascular, aneural state and fibrillar composition have been accepted. The nutrition of articular cartilage remained in dispute. The composition of the binding substance and its relation to collagen remained unknown. Research in the first half of the twentieth century continued to be impeded by lack of technology. The advent of electron microscopy, isotopic tracer technics and enzymology rapidly accelerated the understanding of hyaline cartilage beginning in the 1950s.
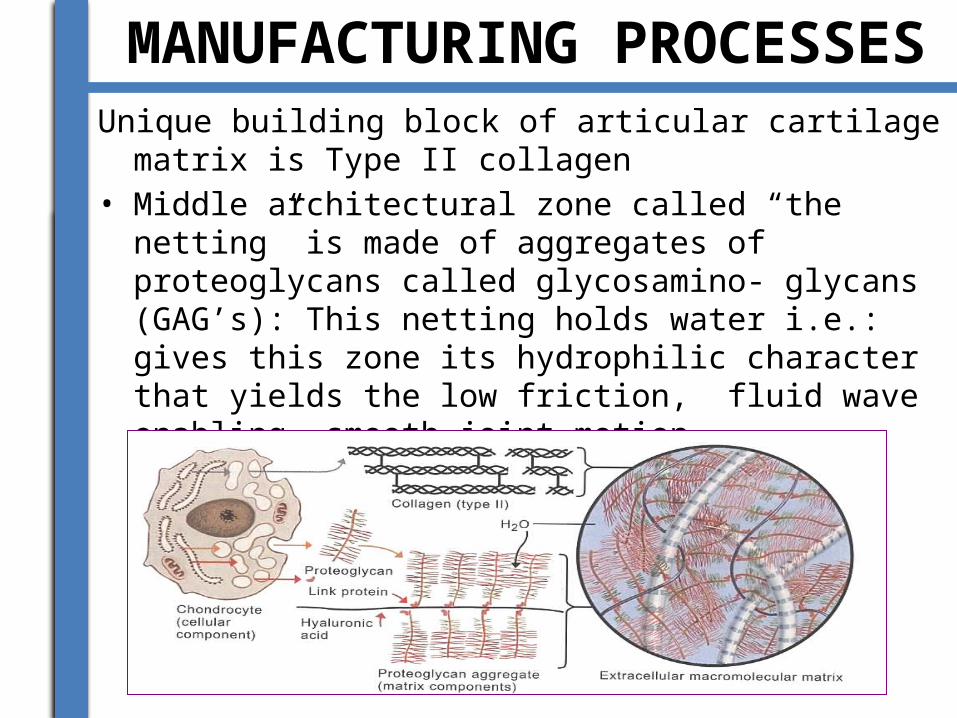
MANUFACTURING PROCESSESUnique building block of articular cartilage matrix is Type II
collagen• Middle architectural zone called “the netting” is made of
aggregates of proteoglycans called glycosamino- glycans (GAG’s): This netting holds water i.e.: gives this zone its hydrophilic character that yields the low friction, fluid wave enabling smooth joint motion
• Restore smooth articular cartilage surface• Relieve patient symptoms and improve function • Match biomechanical/biochemical properties of normal hyaline
cartilage• Prevent or slow progression of focal chondral injury to end-
stage arthritis• Scaffolds to enhance Micr0-fx marrow cell stimulation• 2nd Generation Cell Techniques• Minced Cartilage ( One stage techniques)• 3rd Generation cell techniques • Concurrent Use of Growth factors/ BMP’s • Enhanced Stem cell derived:
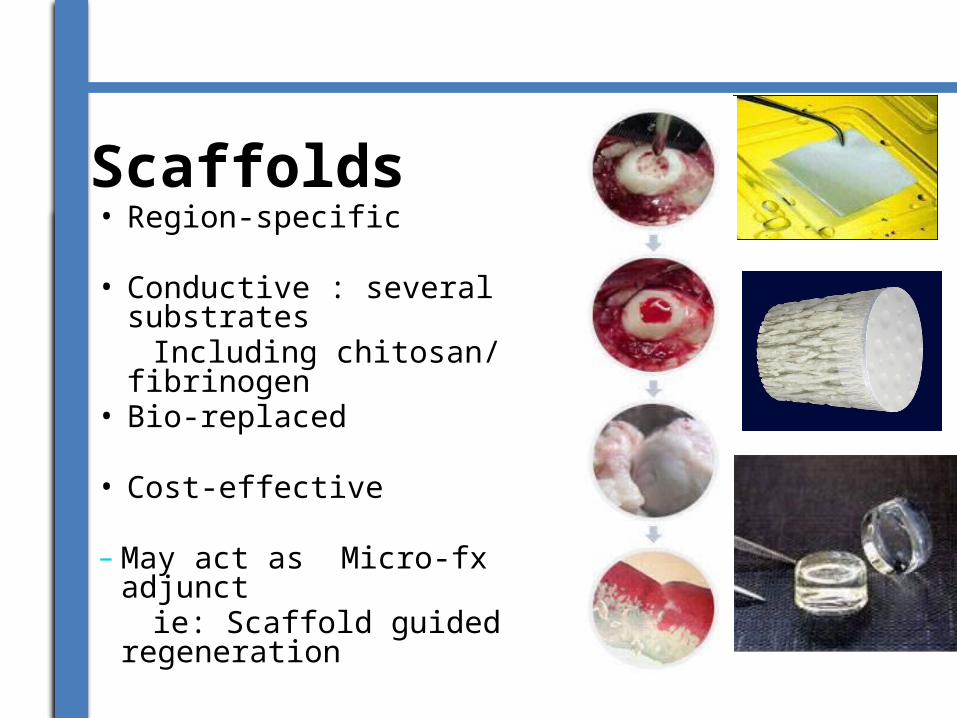
Scaffolds• Region-specific
• Conductive : several substrates Including chitosan/ fibrinogen• Bio-replaced
• Cost-effective
–May act as Micro-fx adjunct ie: Scaffold guided
regeneration
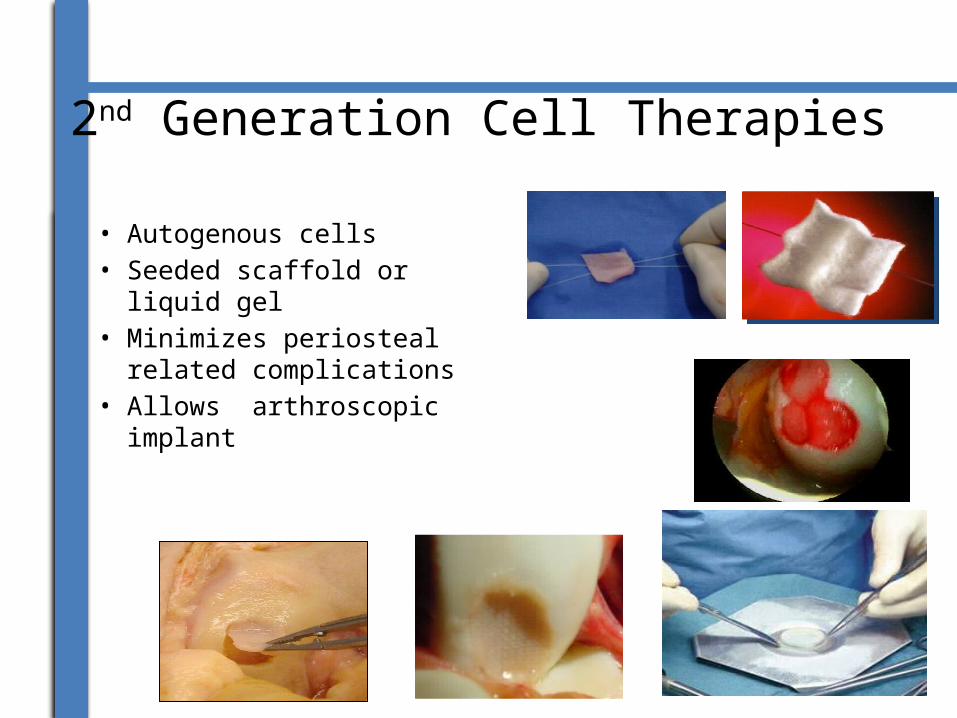
2nd Generation Cell Therapies
• Autogenous cells• Seeded scaffold or liquid
gel• Minimizes periosteal
related complications • Allows arthroscopic
implant
3rd Generation Cell Based
• Autogenous• Allogeneic• 3-D Cartilage graft• Technical ease might allow
arthroscopic insertion with
bioadhesive
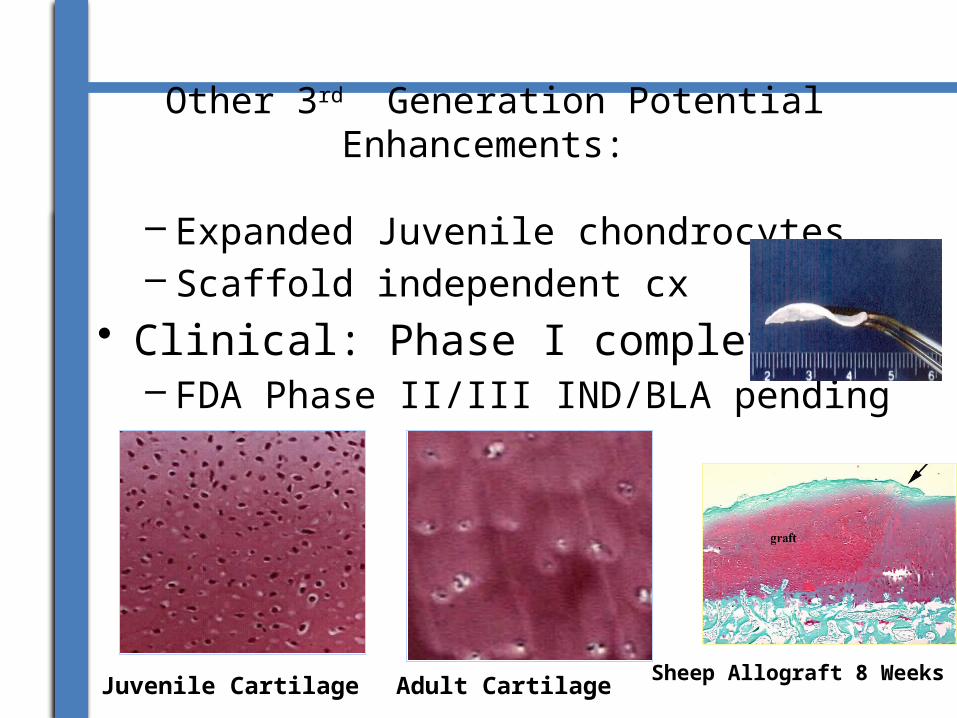
Other 3rd Generation Potential Enhancements:
– Expanded Juvenile chondrocytes– Scaffold independent cx
• Clinical: Phase I completed:– FDA Phase II/III IND/BLA pending
Sheep Allograft 8 WeeksJuvenile Cartilage Adult Cartilage
CURRENT TRENDS/RESENT DEVELOPMENT OF THE ARTIFICIAL CARTILAGE
• A resent development of the Artificial Cartilage is it use in the treatment of knee Injury. Studies have shown that almost half of all running injuries are knee injuries, tears could sometimes occur. For instance, Meniscus (the cartilage pad between the thigh and shin bones) tears can occur when a runner takes a misstep or twists, pivots or compresses the knee joint in the wrong way.
• Biomedical Engineers are now able to implant Artificial Cartilage into patient’s knee that could restore much of the function to the damaged meniscus.
• Another recent Application of the Artificial Cartilage is in Allograft Osteochongraph Transplantation (AOT). This is the process whereby the Cartilage is obtained from a recently deceased donor. It is then tested in the Laboratory to make sure it is free from Infection before been transplanted to the Patient.
•

ONGOING RESEARCH IN THE ARTIFICIAL CARTILAGES
• A number of ongoing research projects are currently investigating more efficient and effective ways of repairing cartilage.
• Examples of current research projects include:• investigating ways of using different sources of stem
cells to generate new cartilage (for example, bone marrow or fat)
• using donor stem cells to regenerate cartilage • combining cartilage and stem cells to improve repair • Although these projects are still in the early stages,
researchers are optimistic they will lead to new kinds of treatment.
AREAS OF APPLICATIONS OF THE ARTIFICIAL CARTILAGE
• The Treatment of knee Injury• Articular Cartilage: the smooth, white tissue
that covers the ends of bones where they come together to form joints
• Nose, Ear etc
ADVANTAGES OF THE ARTIFICIAL CARTILAGE.
• It can protect runners from arthritis and total knee replacement• It can be use to correct birth defects• It brings hope and confidence to Patients• • DISADVANTAGES OF THE ARTIFICIAL CARTILAGE• The Risk of complication and Infection• It could be rejected the patient’s body• It’s expensive
