ash 2015 nhl clinical update
TRANSCRIPT


PCYC-1125-Ca trial: Ibrutinib Plus Rituximab in Treatment-Naive Patients With Follicular Lymphoma
Nathan Fowler, Department of Lymphoma and Myeloma, The University
of Texas MD Anderson Cancer Center, Houston, TX

Follicular Lymphoma

Ibrutinib in FL
• Ibrutinib :phase 1, first-in-human, dose-escalation trial in patients with relapsed/refractory FL
overall response rate (ORR) 38%
Complete Response (CR) 20% --(Advani, JCO 2013).

Frontline Ibrutinib Plus Rituximab in FL: Study Design
• Multicenter phase II study of combination ibrutinib plus rituximab therapy in previously untreated FL pts
• Primary endpoint: ORR
• Secondary endpoints: DoR, PFS, OS, and safety
Treatment naive,
stage II, III, or IV FL
pts with at least
1 measurable lesion
≥ 2 cm; ECOG PS ≤
2
(N = 60)
Ibrutinib
560 mg PO QD +
Rituximab
375 mg/m2 IV weekly x 4
Continued
until
disease
progression
or toxicity

Frontline Ibrutinib Plus Rituximab in FL:
Response
ORR of 82% (49 of 60); CR of 30%
– Median follow-up: 13.8 mos with a median time to best response of 2.7 mos
– Median duration of ibrutinib treatment: 12.55 mos

Frontline Ibrutinib Plus Rituximab in FL: DoR and PFS
• At a median follow-up of 13.8 mos:• Median PFS not reached; 12-mo PFS rate of 86%
• Median OS not reached; 12-mo OS rate of 98%
100
90
80
70
60
50
40
30
20
10
0
Do
R (
%)
Mos From Initiation of Study Treatment0 123 6 9
Pts at
Risk, n: 49 45 34 9 0
100
90
80
70
60
50
40
30
20
10
0
PF
S (
%)
Mos From Initiation of Study Treatment0 123 6 9
Pts at
Risk, n: 60 56 53 41 12
15
1
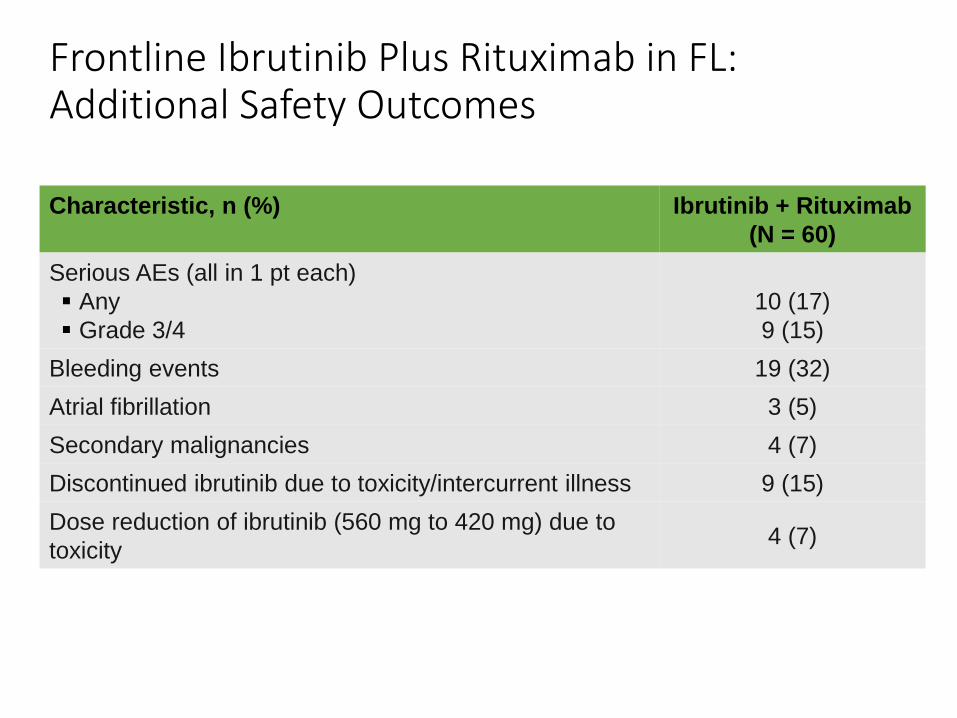
Frontline Ibrutinib Plus Rituximab in FL: Additional Safety Outcomes
Characteristic, n (%) Ibrutinib + Rituximab
(N = 60)
Serious AEs (all in 1 pt each)
Any
Grade 3/4
10 (17)
9 (15)
Bleeding events 19 (32)
Atrial fibrillation 3 (5)
Secondary malignancies 4 (7)
Discontinued ibrutinib due to toxicity/intercurrent illness 9 (15)
Dose reduction of ibrutinib (560 mg to 420 mg) due to
toxicity4 (7)

Frontline Ibrutinib Plus Rituximab in FL: Conclusions
“Ibrutinib addition to rituximab in treatment-naive FL pts is highly active with 82% ORR and 30% CR”
“Combination chemotherapy-free treatment well tolerated with few grade 3/4 serious Aes”

PYRAMID: Frontline R-CHOP ± Bortezomib in Non-GCB DLBCL
Leonard et al, Weill Cornell Medical College, New York, NY

PYRAMID: Background
In retrospective analyses, non-GCB DLBCL pts display less favorable outcomes with R-CHOP chemotherapy than those with GCB DLBCL
Non-GCB DLBCL dependent on NF-κB pathways
Randomized phase II study in non-GCB DLBCL pts investigates efficacy and safety of frontline R-CHOP vs R-CHOP + bortezomib[8]
Meyer PN, et al. J Clin Oncol. 2011;29:200-207./Davis RE, et al. J Exp Med. 2001;194:1861-1874./Ngo VN, et al. Nature.
2006;441;106-110.

PYRAMID: Study Design• Prospective randomized, open-label phase II study
• Primary endpoint: PFS
• Secondary endpoints: OS, ORR, CR, toxicity• Evaluated response, disease progression by CT and FDG-PET at end of cycles 2 and 6• Follow-up scans every 3 mos until disease progression
Treatment-naive,
centrally confirmed
non-GCB DLBCL by
Hans IHC method with
measurable disease,
ECOG PS 0-2
(N = 183)
Bortezomib 1.3 mg/m2 IV Days 1, 4 +
R-CHOP* 21 days x 6 cycles
(n = 92)
R-CHOP* 21 days x 6 cycles
(n = 91)

PYRAMID: Baseline Characteristics
CharacteristicVR-CHOP
(n = 92)
R-CHOP
(n = 91)
Median age, yrs (range)
Age > 65 yrs, %
65 (20-83)
46
62 (24-85)
44
Male, % 49 58
IPI risk group, %
Low
Low/intermediate
High/intermediate
High
28
27
34
11
24
25
38
12
ECOG PS, %
0
1
2
59
40
1
44
44
12
LDH > ULN, % 54 55

PYRAMID: Drug Exposure and Response
• 85% VR-CHOP and 86% R-CHOP pts completed ≥ 6 treatment cycles• Median relative dose intensity: > 98% in both arms for all drugs
• Median duration of follow-up: 34 mos in both arms
Characteristic, %VR-CHOP
(n = 90)
R-CHOP
(n = 86)
CR 56 49
CR/PR 96 98
Negative FDG-PET at EOT visit 59 53

PYRAMID: Survival Outcomes
Outcome, %VR-CHOP
(n = 92)
R-CHOP
(n = 91)HR (95% CI) P Value
2-yr PFS rate 82 780.73
(0.43-1.24).611
2-yr PFS rate by IPI risk group
Low and Low/Intermediate 89 (n = 51) 90 (n = 45)0.85
(0.35-2.10).958
Intermediate/High and
High72 (n = 41) 65 (n = 46)
0.67
(0.34-1.29).606
2-yr OS rate 93 880.75
(0.38-1.45).763

PYRAMID: Safety
• Any grade AE in ≥ 25% pts in either arm
• Hematologic: neutropenia, thrombocytopenia,‡ anemia
• Non-hematologic: fatigue,§ nausea,§
peripheral neuropathy,‡ alopecia,§
constipation, insomnia, diarrhea, peripheral edema,‡ decreased appetite
• Grade ≥ 3 AEs in ≥ 10% pts in either arm
• Hematologic: neutropenia, thrombocytopenia,‡ anemia,‡
decreased WBC, leukopenia,§
decreased platelet count, febrile neutropenia
• Nonhematologic: hypokalemia
Event, %VR-CHOP
(n = 101)
R-CHOP
(n = 100)
Any AE
Grade ≥ 3
99
79
100
71
Drug-related AE
Grade ≥ 3
95
68
88
55
Serious AE 34 31
AEs leading to
discontinuation6 4
Death < 1* 1†
PYRAMID: Conclusions
“Similar survival outcomes with VR-CHOP and R-CHOP in treatment-naive pts with non-GCB DLBCL”

S1106: R-Bendamustine vs R-HyperCVADInduction Therapy Followed by ASCT in MCL

S1106: Background
• Best treatment for MCL still undefined
• R-hyperCVAD effective; but combination with high-dose cytarabine and methotrexate important
–ASCT possible after short course of R-hyperCVAD
• In a phase III trial, R-bendamustine demonstrated greater efficacy than R-CHOP
Romaguera JE, et al. J Clin Oncol. 2005;23:7013-7023. 2. Khouri IF, et al. J Clin Oncol. 1998;16:3803-3809. 3. Till BG, et al. Leuk Lymphoma.
2008;49:1062-1073. 4. Rummel MJ, et al. Lancet. 2013;38:1203-1210. 5. Dreyling M, et al. Blood. 2005;105:2677-2684. 6.

S1106: Study Design
• Randomized phase II US Intergroup trial
• Primary endpoint: 2-yr PFS rate
• Secondary endpoints: ORR, OS, toxicity, prognostic value of MRD monitoring
Adult pts 18-65 yrs of age
with untreated stage III,
IV, or bulky stage II MCL;
CD19+ or CD20+;
cyclin D1 IHC or t(11;14);
2-dimensional
measurable disease,
adequate organ function
(N = 52)
R-Bendamustine
4 cycles
(n = 35)
R-HyperCVAD
Cycle 1
R-MTX/Cytarabine
Cycle 2
(n = 17)
R-HyperCVAD
Cycle 3
Stem cell collection
R-MTX/Cytarabine
Cycle 4
R-Bendamustine
2 cycles
R-Cyclophosphamide
1 cycle
Stem cell collection
Stratified by MIPI Restaging:* ≥ PR Restaging: age
< 61 yrs: CBV,
BEAM, or
TBI/VP16/Cy
61-65 yrs:
CBV or BEAM
*< PR off study.

S1106: Baseline Characteristics
CharacteristicR-Bendamustine
(n = 35)
R-HyperCVAD
(n = 17)P Value
Age, yrs 57 (33-64) 59 (44-66) .23
Male, n (%) 32 (91) 9 (53) .003
ECOG PS, n (%)
0
1
26 (74)
9 (26)
11 (65)
6 (35)
.52
Disease stage, n (%)
III
IV
3 (8.5)
32 (91.4)
1 (5.9)
16 (94.1)
1.00
Bulky disease, n (%) 3 (8) 1 (6) 1.00
B symptoms, n (%) 10 (29) 6 (35) .75
Bone marrow involvement, n (%) 30 (86) 14 (82) 1.00
Extranodal involvement, n (%) 32 (91) 15 (88) 1.00Elevated LDH, n (%) 9 (26) 5 (29) 1.00
MIPI score, n (%)
Intermediate/high risk
Low risk
13 (37)
22 (63)
6 (35)
11 (65)
1.00

S1106: Outcomes
Outcome, n = 52 evaluable ptsR-Bendamustine
(n = 35)
R-HyperCVAD
(n = 17)
Median follow-up, mos (range) 27.3 (1.0-39.5) 34 (10.0-41.0)
Response, %
ORR
CR
PR
Inadequate
82.9
40
43
17
94.1
35
59
6
Survival, %
2-yr PFS
2-yr OS
81
87
82
88

S1106: Induction Phase Grade 3/4 AEsEvent, %
R-Bendamustine(n = 35)
R-HyperCVAD(n = 17)
Thrombocytopenia 17 71
Neutropenia Febrile neutropenia
3414
6529
Anemia 8.6 59
Hypokalemia 5.7 29
Hypophosphatemia 2.9 24
Hyperglycemia 0 12
Increased ALT 0 5.9
Increased AST 0 5.9
Catheter infection 2.9 5.9
Dehydration 0 5.9
Diarrhea 0 5.9
Epistaxis 0 5.9
Nausea 0 5.9
Rash 2.9 5.9
Syncope 0 5.9

S1106: Progression-Free Survival
100
80
60
40
20
00 12 24 36 48
Months After Registration
%
R-Bendamustine
R-HCVAD
Failed
8
4
At Risk
35
17
2-year
Estimate
81%
82%

S1106: Overall Survival
100
80
60
40
20
00 12 24 36 48
Months After Registration
%
R-Bendamustine
R-HCVAD
Failed
4
2
At Risk
35
17
2-year
Estimate
87%
88%

S1106: Conclusions
“R-bendamustine exhibited similar response rates, 2-yr PFS, and 2-yr OS compared with R-hyperCVAD”
• R-bendamustine:–2-yr PFS rate of 81%
–89% MRD-negative rate on paired samples
–Exhibited less hematologic and marrow toxicity than R-hyperCVAD
Chen R, et al. ASH 2015. Abstract 518.

Bendamustine Treatment in Refractory or Relapsed T Cell Lymphomas: A Retrospective
Multicenter Study
Reboursiere et al, CHU, Caen, France

Background
• Peripheral T-cell lymphoma :aggressive disease with poor outcome.
• First line therapies are usually unsatisfactory with frequent need for second-line therapies.
• Median progression free survival (PFS) and overall survival (OS) for relapse PTCL patients are very short with few available therapeutic options.
• Bendamustine has been shown to be active in phase 1 studies.

Study Method
• median age was 64y (range 28-89)
• Histology : AILT=63, PTCL-NOS =44), ALCL=13, NK/TCL (n=3), mycosis fungoides (MF=7), subcutaneous panniculitis-like-TCL (n=2), hepato-splenic-TCL (n=1) and others (n=9).
• The majority of patients (96%, n=130) had stage-disseminated disease and 72% (n=102) of them had extranodal localisations.
• The median number of chemotherapy lines prior to bendamustine was 2 (range 0-8). Seven patients (5%) had SCT and 16 autoSCT (11%)
• The median duration of response prior to bendamustine 4.3m and 50% of patients had refractory disease.

Result
• Overall, they received a median of 2 cycles (range 1-8) with a median dose of 90mg/m2 (range 50-150).
• The best overall response rate (ORR) was 32% ,complete response of 24% (CR=34). The median DoR was 3.3 months (1-39).
• For AITL patients, ORR was 52% (33/63) with CR of 41%, whereas it was 18% (8/44) with 11% of CR,

“Bendamustine as single agent must be considered as a therapeutic option for relapsed or refractory PTCL, particularly in patients with AITL”
