aspirin exacerbated respiratory disease diagnosis and desensitization sandra c christiansen md...
TRANSCRIPT
Aspirin Exacerbated Respiratory DiseaseDiagnosis and Desensitization
Sandra C Christiansen MD
Kaiser Permanente & UCSD

Aspirin/NSAID Sensitivity• Pseudoallergic reactions:
- urticaria/angioedema- Respiratory, including naso-ocular and/or asthma
• Rarely: anaphylactoid reaction with laryngeal or GI sx• Prevalence:
- 0.2% general population- 8-19% asthmatics- 30-40% polyps & sinusitis
• AERD (ASA quatrad): - asthma, sinusitis, ASA sensitivity, nasal polyps
Clinical AERD presentation (1)• Sequence of symptoms
– Rhinitis at an average age of 30 years, related to a flu-like infection in half of patients; possibility of ETS or diesel particulate exposure
– Asthma (2 years later)– Aspirin intolerance and nasal polyposis (4 years later)
with anosmia or hyposmia• Women
– Outnumber men by 2.3:1– More progressive and severe
• Atopy – one third to two thirdsSzczeklik et al Eur Respir J 2000

Clinical AERD presentation (2)
• Most patients with AERD have moderate or severe persistent asthma.– Inhaled corticosteroids; 80%– Oral steroids; 51%
Szczeklik et al Eur Respir J 2000

Szczeklik et al Eur Respir J 2000

Clinical AERD presentation (3)
• After ingestion – acute asthma attack occurs within 3 hours, usually accompanied by profuse rhinorrhea, conjunctival injection, periorbital edema, and sometimes a scarlet flushing of head and neck
Szczeklik et al J Allergy Clin Immunol 1999
• AERD is a common precipitant of life-threatening attack of asthma (7 out of 92 asthmatics who underwent mechanical ventilation)
Picado et al Eur Respir J 1989
• 25% of asthmatic patients requiring emergency mechanical ventilation – AERD (147 asthmatics)
Marquette et al Am Rev Respir Dis 1992

Prevalence of AERD according to severity of bronchial hyperresponsiveness
P < .01

Prevalence of AERD according to sputum eosinophil count
P < .05
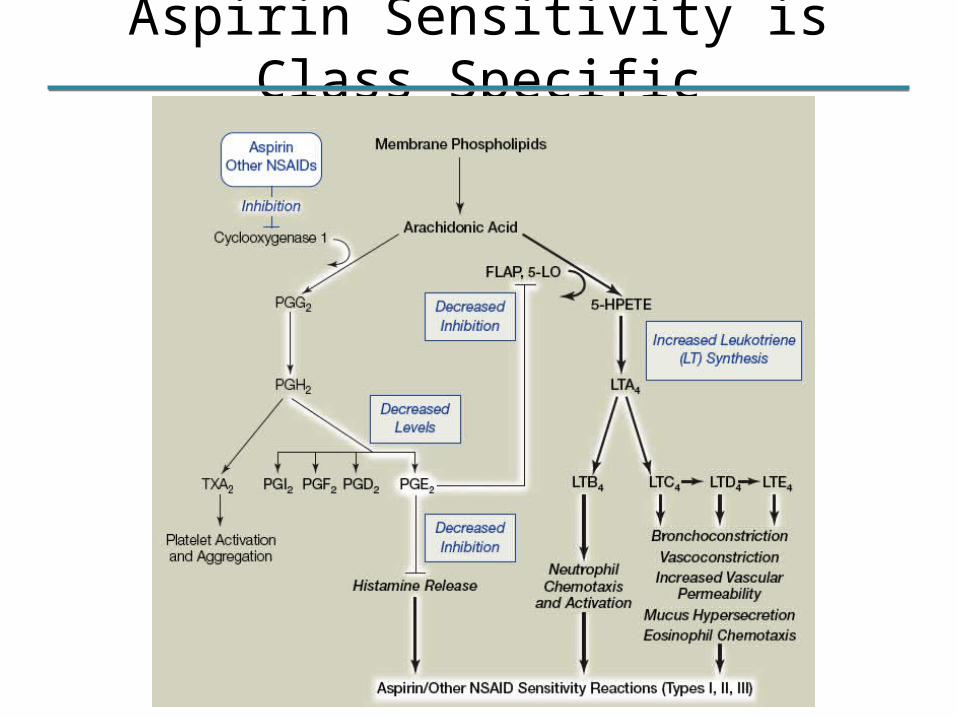
Aspirin Sensitivity is Class Specific
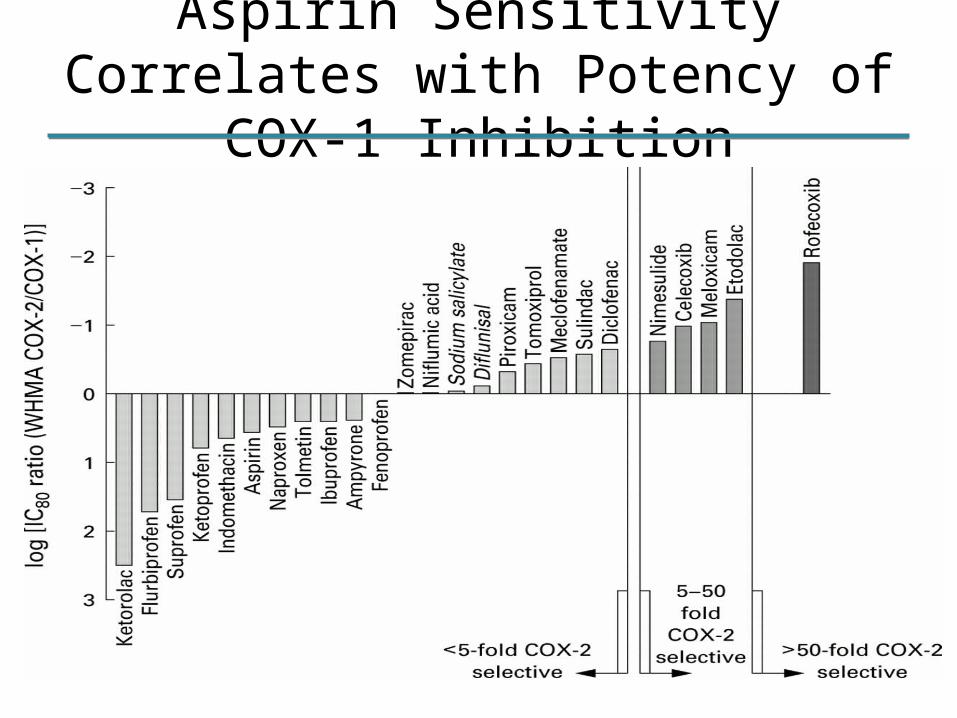
Aspirin Sensitivity Correlates with Potency of COX-1 Inhibition
Cyclooxygenase pathway
• COX-1 and COX-2 have molecular weights of 71 kd and 60% homology
• COX-1 constitutive form• COX-2 induced during inflammation
and enhances synthesis of inflammatory prostanoids
• PGE2
– Reduce LT biosynthesis through inhibition of 5-LO
– Inhibits cholinergic transmission– Prevents discharge of granular
mediators from mast cells– Prevents ASA-precipitated
bronchoconstriction and the expected rise in urinary LTE4
• PGE2 administration by inhalation inhibits aspirin induced bronchoconstriction
Sestini et al AJRCCM 1996
• Selective COX-2 inhibitor(celecoxib, rofecoxib) – preserve PGE2 and do not cross-react with ASA
Stevenson et al J Allergy Clin Immunol 2001Szczeklik et al Clin Exp Allergy 2001

Fig. 3. Counts of cells immunostaining for 5-LO pathway enzymes in bronchial mucosal biopsies from patients with AIA (n = 10), with ATA (n = 10), and N subjects (n = 9), taken 20 min after bronchoscopic challenge with placebo solution. Enzymes are 5-LO, FLAP, LTA4
hydrolase (LTA4H), and LTC4 synthase (LTC4S). Horizontal bars, mean±SEM. All significant comparisons between subject groups (P
< 0.05 Mann-Whitney) are indicated.
Cowburn et al J Clin Invest 1998
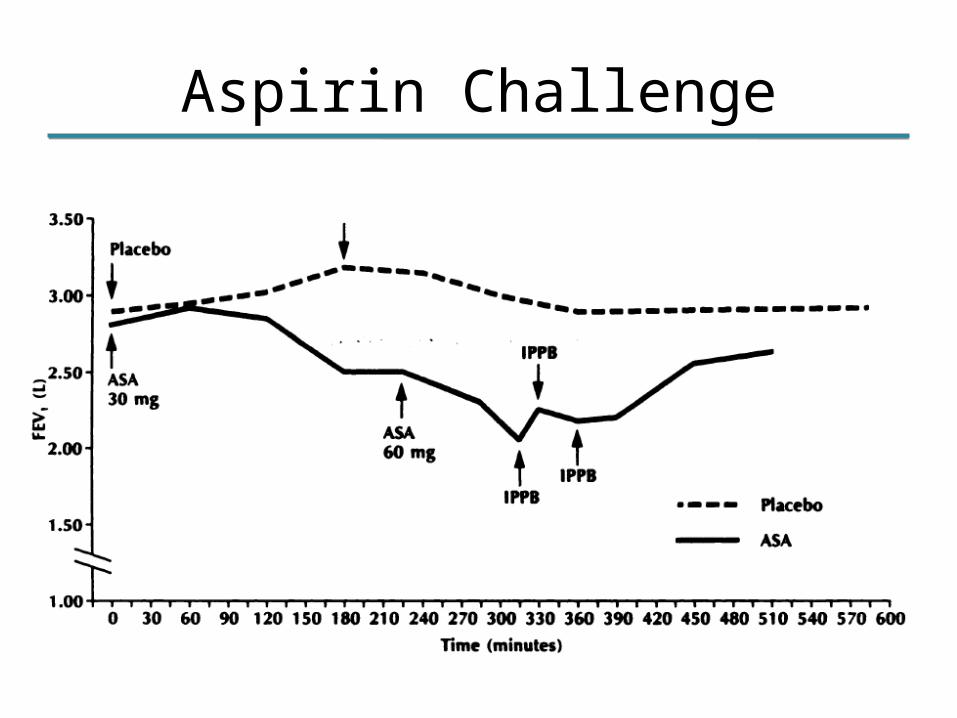
Aspirin Challenge

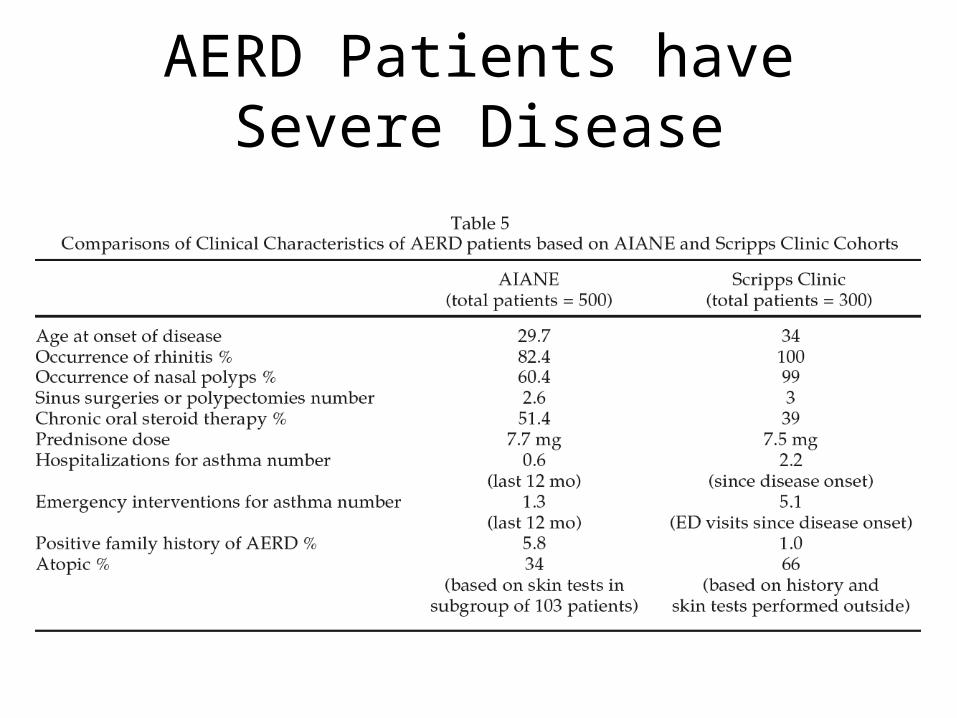
AERD Patients have Severe Disease
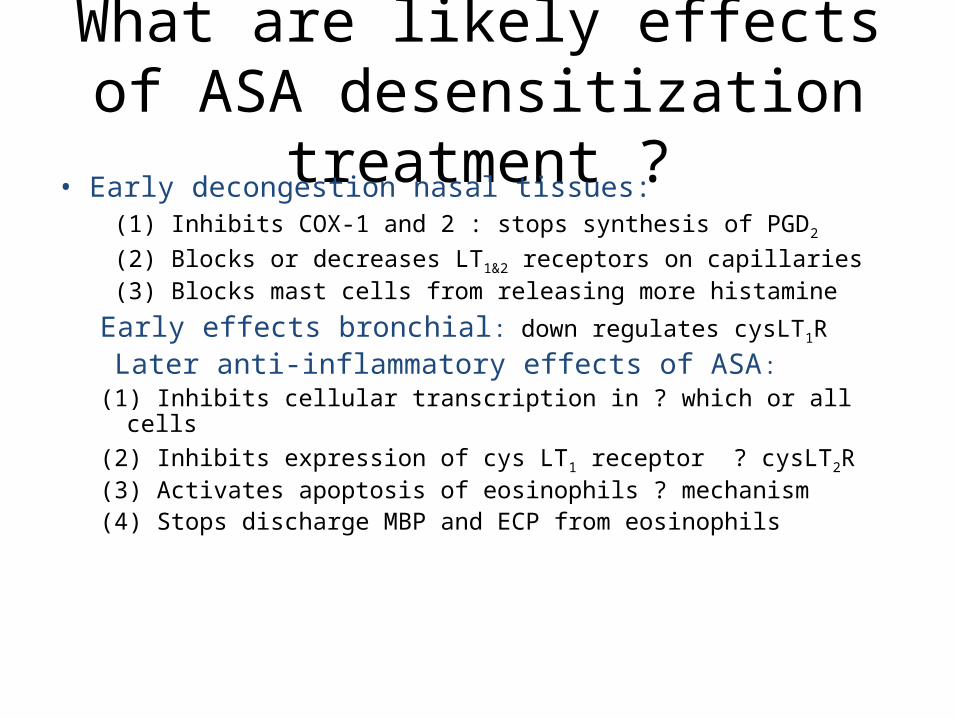
What are likely effects of ASA desensitization treatment ?
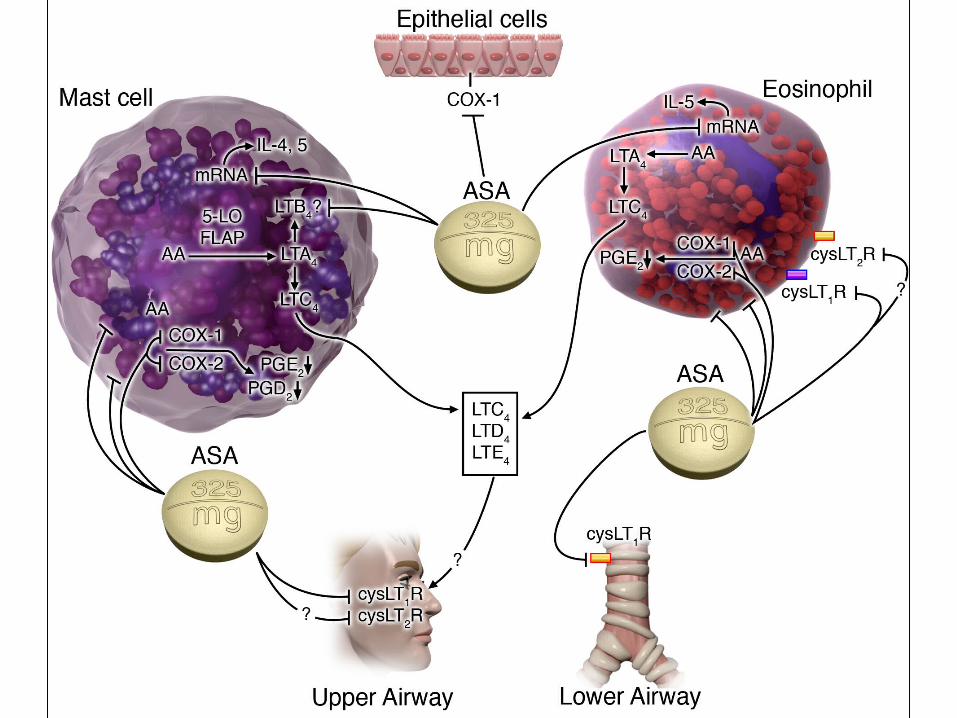
• Early decongestion nasal tissues: (1) Inhibits COX-1 and 2 : stops synthesis of PGD2
(2) Blocks or decreases LT1&2 receptors on capillaries (3) Blocks mast cells from releasing more histamine
Early effects bronchial: down regulates cysLT1R
Later anti-inflammatory effects of ASA:(1) Inhibits cellular transcription in ? which or all cells(2) Inhibits expression of cys LT1 receptor ? cysLT2R(3) Activates apoptosis of eosinophils ? mechanism(4) Stops discharge MBP and ECP from eosinophils

Polyp sinus surgery before and after ASA desensitization
• AERD patients average one sinus/ polyp operation every 3 years:
• After ASA desensitization:– Average revision operation: one every 10 years– Majority stopped or slowed growth of polyps– With decrease in polyps, decrease infections– Decrease in need for prednisone bursts
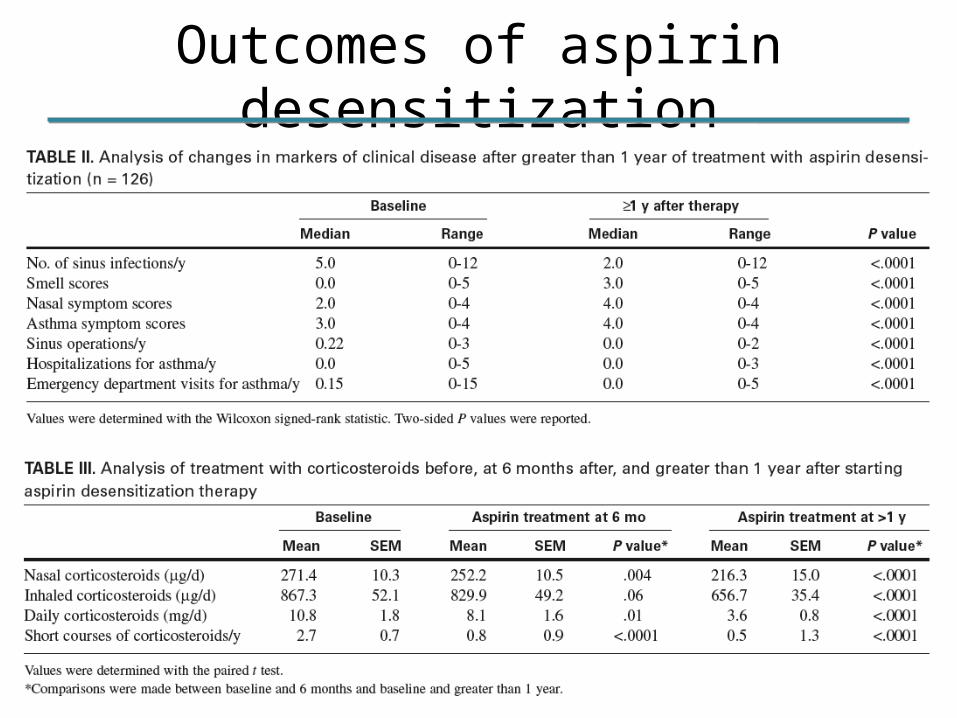
Outcomes of aspirin desensitization
‘How We Do It’Preparation for ASA
Challenge• Consult for AERD• 2 week prechallenge nursing
checklist, review medications (singulair, prednisone dose, frequency of SABA)
• Advise MD if changes required• Hold antihistamine 48 hours prior,
SABA after midnight pre challenge
Toradol Challenge
• Nasacort spray vial soln 8mg Toradol/cc
• Monitor spirometry, symptom scores, VAS, PIF
• IV, one on one nursing• Dosing 30”intervals, NS, 1spray
(1.04mg) to 6 sprays each nostril (12.48mg)

ASA Challenge/Desensitization
• FEV1 >70%• Monitor spirometry, symptom scores,
VAS,PIF• IV, one on one nursing• Dosing 3’ intervals, usual mg 20.25,
40.5, 81, 162.5, 325, 650• Maintenance 650 bid for 6-12 months
then 325 bid

Risk Factors for Severe Reaction
• Drop in FEV1>30%• Lack of LT modifier• Baseline FEV1 <80%• Prior asthma related ED visit• 75% threshold dose 45 or 60mg• 3% initial reactions 150-325, no reactions at 650 for threshold dose
A. Hope et al JACI 2009;
123:406-10
ASA Reaction Treatment• Ocular, topical antihistamine• Nasal antihistamine, topical decongestant• Laryngeal, racemic epinephrine (2.5mg/2cc) • Bronchial, Nebulized Albuterol• GI, IV Ranitidine• Urticarial, IV Benadryl 50mg• Shock, Epinephrine IM Epipen
Long Term AERD Tx Outcomes
• 1995-2000 Scripps Clinic GCRC, 172 enrolled, written and telephone f/u• 14% dropout, 78% of remaining 148 improved, 87% for 110 with >1 year f/u• Onset of improvement 6mo,# sinus infections, prednisone bursts, smell score, nasal-sinus and asthma symptoms • 1-5 year ED, Hospitalization, ESS p<.0001
M Pilar Berges-Gimeno et al JACI 2003;111:180-6

Economics of ASA Treatment for AERD
• Ambulatory desensitization for AERD cost $6768 per quality-adjusted life year (QALY)• Saved $18.54 per additional symptom-free day• Remained cost effective across a wide range of assumptions (<$50,000 per QALY saved)
M. Shaker et al JACI 2008;121:81-7