assessing postoperative pain after endodontic therapy · pdf filepain after endodontic therapy...
TRANSCRIPT

Opinions expressed by CE authors are their own and may not reflect those of Dentistry Today. Mention ofspecific product names does not infer endorsement by Dentistry Today. Information contained in CE articlesand courses is not a substitute for sound clinical judgment and accepted standards of care. Participants areurged to contact their state dental boards for continuing education requirements.
Continuing Education
Assessing PostoperativePain After Endodontic
TherapyAuthored by David A. Beach, DDS, MS
Upon successful completion of this CE activity 1 CE credit hour will be awarded
Volume 32 No. 10 Page 90
ABOUT THE AUTHORDr. Beach graduated magna cum laudefrom the University of Florida College ofDentistry in 2003. He completed hisendodontic residency there in 2005. Dr.Beach is currently a Dip lomate of theAmerican Board of Endodontics and
maintains a private practice in Wesley Chapel, Fla. Dr.Beach frequently provides continuing educational lecturesat local, state, and national study clubs and conventions.Hevcan be reached at [email protected] or atendodonticeducators.com.
Disclosure: Dr. Beach reports no disclosures.
INTRODUCTIONEndodontic therapy has a high degree of success.1 In spiteof this, some pa tients will experience varying de grees ofpostoperative problems. The following article addressessome of the types of postoperative problems that can beencountered in endodontics, as well as how to minimizeand manage them.
ENDODONTIC FLARE-UPS A flare-up, whether after completion of endodontic therapyor in between appointments of a multiple-visit treatment,can result in an exacerbation of clinical symptoms. If aclinician treats enough necrotic teeth endodontically inone’s practice, one will eventually have a patientexperience a flare-up.2 It is a simple statistical fact. Since avariety of factors can contribute to or cause a flare-up, it isimpossible to prevent this situation 100% of the time.
Some etiological factors that can cause a flare-up are:1. Inadequate debridement of the root canal system,
leaving bacteria behind to continue the infection.
2. Extruding debris out of the apex during cleaning andshaping, causing the host immune system to react. This canbe done by excessive air pressure with an air/water syringe,incorrect irrigation technique, or errors in working length.
3. Over instrumentation leading to tissue damage, ordebris extrusion in the apical area.
4. A poor host response. Poor systemic health, loweredimmune defenses, allergic reactions, and a geneticpredisposition can all contribute to a flare-up even if theclinician does not accidentally have any procedural errorsoccur. Endodontics, like anything in medicine or dentistry, isreally a 2-way street. The clinician can do his or her part, butthe patient’s body must do its part as well to heal.
When a flare-up occurs, the patient can experiencevarying degrees of pain and swelling in minor to moderatecases, and additional systemic symptoms like fever andmalaise in more severe cases. To treat a flare-up, theclinician can prescribe antibiotics when necessary,prescribe analgesics, and perform an incision and drainageif needed. Fortunately, the occurrence of a flare-up doesnot lower the prognosis of endodontic treatment.
While flare-ups cannot be totally avoided, the followingsuggestions can help minimize their occurrence:
l Avoid blowing air from the air/water syringe devicedown the canals during ac cess. While accessing anecrotic tooth, re move debris with irrigation andsuction only. If visibility is impaired in a deep chamberby residual water, blot dry the chamber with a cottonpellet held in cotton pliers.
l Thoroughly clean the canal(s).l Maintain good working length control.l Prescribe appropriate medications. If the patient hasclinical symptoms or issues in their medical historythat warrant the use of antibiotics, prescribe themresponsibly.
l Perform an incision and drainage if the swelling doesnot have a sinus tract or does not drain from thecanal when the tooth is accessed.
SHORT-TERM POSTOPERATIVE PAIN Short-term postoperative pain can be de fined as discomfortlasting one to 2 weeks after treatment. It is normal for a patient
Continuing Education
1
Assessing Postoperative PainAfter Endodontic TherapyEffective Date: 10/1/2013 Expiration Date: 10/1/2016

to experience some discomfort after endodontic therapy. Rootcanal therapy (RCT) itself involves poking, filing, cuttingnerves, removing tissue, etc. A lot occurs that can causesome soreness. If the tooth was inflamed, the periodontalligament (PDL) has to heal. If the tooth was infected, thedestruction from the bacteria must be cleared. A key point toremember in en dodontics is preoperative pain is the mostreliable predictor of postoperative pain.3 If a patient presentswith significant pain, chances are they will not feel 100%better immediately after the procedure is completed and theanesthesia wears off.
In order to avoid unnecessary concerns and phone callsfrom a patient, expectations during the recovery periodneed to be managed by the clinician. Advise the patient thathealing will take time. A “root canal” is not a 100% quick fix.The analogy of a splinter in a finger often helps the patientunderstand. When a splinter is re moved from a finger, thefinger still has to heal. Like the finger, the tooth andeverything around it must heal once the infection and/orinflammation is removed. If the patient has pain whilechewing, this will likely take a week to resolve. Tell thepatient the ligament around the tooth in the socket needs toheal. If an ankle is sore, staying off it allows the ligamentsand tendons to heal. Similarly, the more the patient avoidschewing on the tooth, the quicker it will heal. Writtenpostoperative in structions emphasizing the possibility ofdiscomfort for one or 2 weeks and how to manage pain withover-the-counter medications can help patients rememberany verbal advice they may forget once they leave thedental office.
PERSISTENT PAINAfter the average healing period of one to 2 weeks followingendodontic therapy, some patients can continue toexperience problems. There are more than 16.4 million rootcanal procedures performed each year in the UnitedStates. The frequency of persistent tooth pain after RCT isestimated to be 5.3%.4 Some possible causes of persistentpain include:
1. Is another tooth involved? Per haps the tooth treatedwas not the only tooth involved in causing the symptoms.Or, perhaps, was the wrong tooth diagnosed and treated?
2. Is there a missed canal? Angled radiographs cansometimes help determine this.
3. Is the tooth cracked? If it is, RCT can be performedrepeatedly without any hope of resolving the problem.
4. Does the patient have a sinus infection? If thesymptoms are in the maxillary arch, sometimes sinus issuescan mimic odontogenic pain. The tooth or teeth may actuallybe fine.
5. Are there periodontal issues? Is an open contactcausing trauma and inflammation to the marginal gingiva?Is a periodontal pocket infected or inflamed?
6. Is the patient having a poor host response? As statedearlier, the clinician can provide the best therapy in theworld, but if the patient’s body is unable to heal, then theprocedure will not work. Nothing in dentistry or medicine is100% guaranteed. If it were, a majority of consent formswould probably not be needed.
7. Does the occlusion need to be adjusted? When thePDL becomes inflamed, the tooth can be raised in thesocket. Likewise, a significant infection in the periapicalarea can cause tenderness to occlusal loading. If a largerestoration or carious area is removed during access, thegeneral occlusal pattern of the tooth is altered. Excessivecontact concentrated on one area can cause pain.
8. Does the patient have a history of bruxism or otherparafunctional occlusal habits? If the patient is puttingexcessive occlusal force on the tooth, it will delay thehealing by prolonging inflammation in the PDL.
When attempting to sort through the possible causes ofpersistent pain with a tooth, the clinician should always startwith a conservative ap proach. Often, occlusion is thesolution. Check for occlusal interferences or excessivecontacts and adjust or relieve accordingly. A short-termsteroid, such as a medrol dose pack, can be given to speedup the reduction of inflammation in the PDL after treating avital tooth. The prescription of antibiotics may be necessaryin cases of severe or persistent infections. Retest theadjacent teeth to rule out the presence of anothersymptomatic tooth. If sensitivity to cold temperature is stillbothering the patient, the involvement of another toothshould be high on the list of considerations.
Despite the best efforts of the clinician, sometimes
Continuing Education
2
Assessing Postoperative Pain After Endodontic Therapy
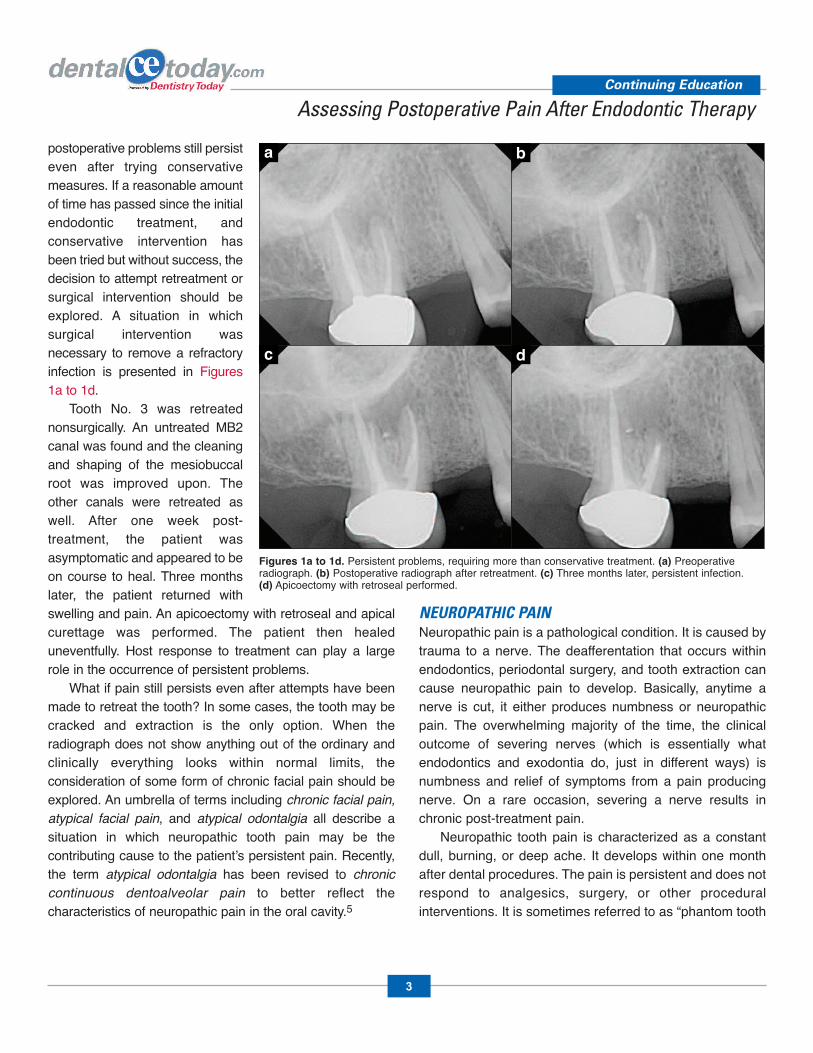
postoperative problems still persisteven after trying conservativemeasures. If a reasonable amountof time has passed since the initialendodontic treatment, andconservative intervention hasbeen tried but without success, thedecision to attempt retreatment orsurgical intervention should beexplored. A situation in whichsurgical intervention wasnecessary to remove a refractoryinfection is presented in Figures1a to 1d.
Tooth No. 3 was retreatednonsurgically. An untreated MB2canal was found and the cleaningand shaping of the mesiobuccalroot was improved upon. Theother canals were retreated aswell. After one week post-treatment, the patient wasasymptomatic and appeared to beon course to heal. Three monthslater, the patient returned withswelling and pain. An apicoectomy with retroseal and apicalcurettage was performed. The patient then healeduneventfully. Host response to treatment can play a largerole in the occurrence of persistent problems.
What if pain still persists even after attempts have beenmade to retreat the tooth? In some cases, the tooth may becracked and extraction is the only option. When theradiograph does not show anything out of the ordinary andclinically everything looks within normal limits, theconsideration of some form of chronic facial pain should beexplored. An umbrella of terms including chronic facial pain,atypical facial pain, and atypical odontalgia all describe asituation in which neuropathic tooth pain may be thecontributing cause to the patient’s persistent pain. Recently,the term atypical odontalgia has been revised to chroniccontinuous dentoalveolar pain to better reflect thecharacteristics of neuropathic pain in the oral cavity.5
NEUROPATHIC PAINNeuropathic pain is a pathological condition. It is caused bytrauma to a nerve. The deafferentation that occurs withinendodontics, periodontal surgery, and tooth extraction cancause neuropathic pain to develop. Basic ally, anytime anerve is cut, it either produces numbness or neuropathicpain. The overwhelming majority of the time, the clinicaloutcome of severing nerves (which is essentially whatendodontics and exodontia do, just in different ways) isnumbness and relief of symptoms from a pain producingnerve. On a rare occasion, severing a nerve results inchronic post-treatment pain.
Neuropathic tooth pain is characterized as a constantdull, burning, or deep ache. It develops within one monthafter dental procedures. The pain is persistent and does notre spond to analgesics, surgery, or other proceduralinterventions. It is sometimes referred to as “phantom tooth
Continuing Education
3
Assessing Postoperative Pain After Endodontic Therapy
Figures 1a to 1d. Persistent problems, requiring more than conservative treatment. (a) Preoperative radiograph. (b) Postoperative radiograph after retreatment. (c) Three months later, persistent infection. (d) Apicoectomy with retroseal performed.
a b
c d

pain.”6 It tends to develop in patients who experience eitherchronic or intense pain before a procedure, or in patientswho undergo a procedure under inadequate anesthesia.The mechanisms of neuropathic tooth pain include centralsensitization in the brain, ectopic impulses generated froma neuroma at the injury site, neuroplasticity, decreasedaction of the descending inhibitory system, and Aß fibersthat cause mechanical allodynia.
Treatment of neuropathic tooth pain involves the off-label use of tricyclic antidepressants or antiepileptics.These drugs have many possible side effects. Referral to aneurologist is the best option for a clinician not comfortablein prescribing these medications and managing asuspected case of neuropathic tooth pain.
Luckily, in dentistry, the incidence of chronic pain after aprocedure is low compared to other procedures performedelsewhere on the human body. Chronic pain following toothextraction or endodontic therapy ranges from 3% to 5%.Other procedures, such as amputation of a limb or coronaryartery by pass surgery, can have incidences of chronic painfrom 30% to 50%! Even a C-section or inguinal hernia repaircan leave a patient with chronic pain around 10% of thetime.7 While postoperative pain prob lems are a headache todeal with at times, we don’t seem to have it so bad indentistry after all if you look at it from a medical perspective.
IN SUMMARYEndodontics has a high de gree of success when donecorrectly (Figures 2a to 2c). Many of the complications that
can occur after RCT have been presented. Methods andideas to manage and avoid these complications have beendescribed. It is now up to you to put the knowledge intopractice.
REFERENCES1. Setzer FC, Boyer KR, Jeppson JR, et al. Long-termprognosis of endodontically treated teeth: aretrospective analysis of preoperative factors in molars.J Endod. 2011;37:21-25.
2. Naidorf IJ. Endodontic flare-ups: bacteriological andimmunological mechanisms. J Endod. 1985;11:462-464.
3. Kalkman CJ, Visser K, Moen J, et al. Preoperativeprediction of severe postoperative pain. Pain.2003;105:415-423.
4. Nixdorf DR, Moana-Filho EJ, Law AS, et al. Frequencyof persistent tooth pain after root canal therapy: asystematic review and meta-analysis. J Endod.2010;36:224-230.
5. Greene CS, Murray GM. Atypical odon tal gia: an oralneuropathic pain phe nom enon. J Am Dent Assoc.2011;142:1031-1032.
6. Oshima K, Ishii T, Ogura Y, et al. Clinical investigationof patients who develop neuropathic tooth pain afterendodontic procedures. J Endod. 2009;35:958-961.
7. Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgicalpain: risk factors and prevention. Lancet.2006;367:1618-1625.
Continuing Education
4
Assessing Postoperative Pain After Endodontic Therapy
Figures 2a to 2c. Successful endodontic treatment of tooth No. 30. (a) Preoperative radiograph. Note the large periradicular lesion. (b) Postoperative radiograph. (c) One-year postoperative radiograph, showing resolution of the periradicular lesion.
a b c

POST EXAMINATION INFORMATION
To receive continuing education credit for participation inthis educational activity you must complete the programpost examination and answer 4 out of 5 questions correctly.
Traditional Completion Option:You may fax or mail your answers with payment to DentistryToday (see Traditional Completion Information on followingpage). All information requested must be provided in orderto process the program for credit. Be sure to complete your“Payment,” “Personal Certification Information,” “Answers,”and “Evaluation” forms. Your exam will be graded within 72hours of receipt. Upon successful completion of the post-exam (answer 4 out of 5 questions correctly), a letter ofcompletion will be mailed to the address provided.
Online Completion Option:Use this page to review the questions and mark youranswers. Return to dentalcetoday.com and sign in. If youhave not previously purchased the program, select it fromthe “Online Courses” listing and complete the onlinepurchase process. Once purchased the program will beadded to your User History page where a Take Exam linkwill be provided directly across from the program title.Select the Take Exam link, complete all the programquestions and Submit your answers. An immediate gradereport will be provided. Upon receiving a passing grade,complete the online evaluation form. Upon submitting the form, your Letter Of Completion will be providedimmediately for printing.
General Program Information:Online users may log in to dentalcetoday.com any time inthe future to access previously purchased programs andview or print letters of completion and results.
POST EXAMINATION QUESTIONS
1. If a clinician treats enough necrotic teethendodontically in their practice, they will eventuallyhave a patient experience a flare-up. a. True b. False
2. The occurrence of a flare-up does not lower theprognosis of endodontic treatment. a. True b. False
3. Preoperative pain is the most reliable predictor ofpostoperative pain. a. True b. False
4. The frequency of persistent tooth pain after rootcanal therapy is estimated to be 15.3% a. True b. False
5. Neuropathic tooth pain is characterized as a constantdull, burning, or deep ache, usually developing withinone month after dental procedures.a. True b. False
Continuing Education
5
Assessing Postoperative Pain After Endodontic Therapy
This CE activity was not developed in accordance withAGD PACE or ADA CERP Standards.CEUs for this activity will not be accepted by the AGDfor MAGD/FAGD credit.
PROGRAM COMPLETION INFORMATION
If you wish to purchase and complete this activitytraditionally (mail or fax) rather than online, you mustprovide the information requested below. Please be sure toselect your answers carefully and complete the evaluationinformation. To receive credit you must answer 4 of the 5questions correctly.
Complete online at: dentalcetoday.com
TRADITIONAL COMPLETION INFORMATION:Mail or fax this completed form with payment to:
Dentistry TodayDepartment of Continuing Education100 Passaic AvenueFairfield, NJ 07004Fax: 973-882-3622
PAYMENT & CREDIT INFORMATION:
Examination Fee: $20.00 Credit Hours: 1Note: There is a $10 surcharge to process a check drawn on any bank other than a US bank. Should you have additionalquestions, please contact us at (973) 882-4700.
o I have enclosed a check or money order.o I am using a credit card.
My Credit Card information is provided below.o American Express o Visa o MC o Discover
Please provide the following (please print clearly):
Exact Name on Credit Card
Credit Card # Expiration Date
Signature
PROGRAM EVAUATION FORMPlease complete the following activity evaluation questions.Rating Scale: Excellent = 5 and Poor = 0Course objectives were achieved. Content was useful and benefited your clinical practice. Review questions were clear and relevant to the editorial. Illustrations and photographs were clear and relevant.Written presentation was informative and concise.How much time did you spend reading the activity and completing the test?What aspect of this course was most helpful and why?
What topics interest you for future Dentistry Today CE courses?
Continuing Education
Assessing Postoperative Pain After Endodontic Therapy
ANSWER FORM: VOLUME 32 NO. 10 PAGE 90Please check the correct box for each question below.1. o a. True o b. False2. o a. True o b. False3. o a. True o b. False4. o a. True o b. False5. o a. True o b. False
PERSONAL CERTIFICATION INFORMATION:
Last Name (PLEASE PRINT CLEARLY OR TYPE)
First Name
Profession / Credentials License Number
Street Address
Suite or Apartment Number
City State Zip Code
Daytime Telephone Number With Area Code
Fax Number With Area Code
E-mail Address
/
6
This CE activity was not developed in accordance withAGD PACE or ADA CERP Standards.CEUs for this activity will not be accepted by the AGDfor MAGD/FAGD credit.