assessment and management of patients with hypertension
TRANSCRIPT

Assessment and Management of Patients
With Hypertension
Assessment and Management of Patients
With Hypertension
Hypertension • High blood pressure• Defined by the Seventh Report of the Joint
National Commission on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) as a systolic pressure greater than 140 mm Hg and a diastolic pressure greater than 90 mm Hg. based on the average of two or more accurate blood pressure measurements taken during two or more contacts with a health care provider

Classification of Blood Pressure for Adults Age 18 and Older

Incidence of Hypertension— “The Silent Killer”
• Primary hypertension.• Secondary hypertension.• 28–31% of the adult population of the U.S. has
hypertension. • 90–95% of this population with hypertension
has primary hypertension.• Incidence is greater in southeastern U.S. and
among African-Americans.
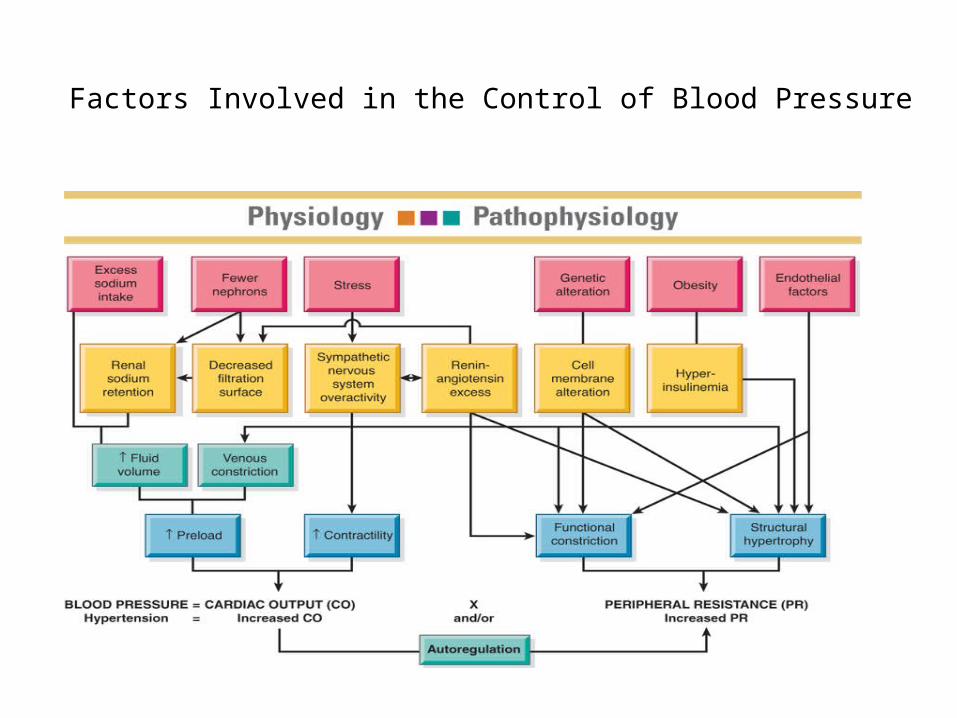
Factors Involved in the Control of Blood Pressure

Common Peripheral Vascular
• Primary Hypertension– Pathophysiologic causes• Sympathetic nervous system overstimulation• Alterations of the renin-angiotensin-aldosterone system• Chemical mediators of vasomotor tone and blood
volume• Interaction between insulin resistance,
hyperinsulinemia and endothelial function

Common Peripheral Vascular

Common Peripheral Vascular
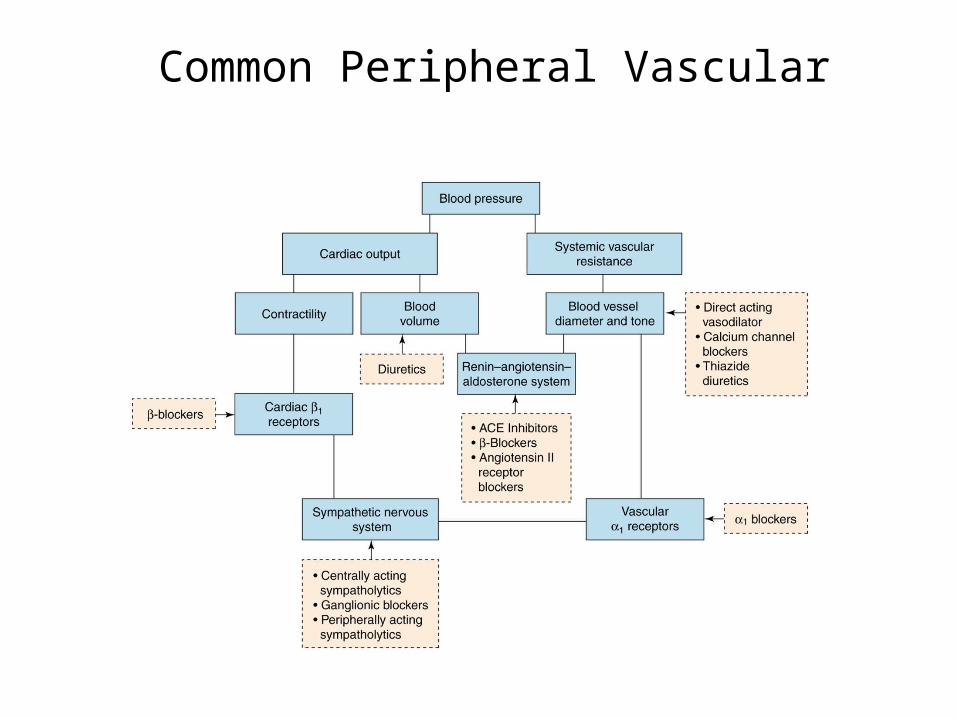
Common Peripheral Vascular
Manifestations of Hypertension
• Usually NO symptoms other than elevated blood pressure
• Symptoms seen related to organ damage are seen late and are serious – Retinal and other eye changes– Renal damage – Myocardial infarction– Cardiac hypertrophy– Stroke
Common Peripheral Vascular
– Manifestations• Initially asymptomatic• Headache, confusion• Nocturia• Nausea and vomiting• Visual disturbances
– Complications• Cardiovascular• Neurologic• Renal systems.

Common Peripheral Vascular
• Secondary Hypertension– Related to a specific underlying cause• Kidney disease• Coarctation of the aorta• Endocrine disorders• Neurologic disorders• Drug use• Pregnancy
Major Risk Factors
• Hypertension• Smoking• Obesity• Physical inactivity• Dyslipedemia• Diabetes mellitus• Microalbuminuria or GFR < 60• Older age• Family history
Patient Assessment
• History and Physical• Laboratory tests– Urinalysis– Blood chemistry– Cholesterol levels
• ECG

JNC 7 Treatment Algorithm
Refer to fig. 32-2
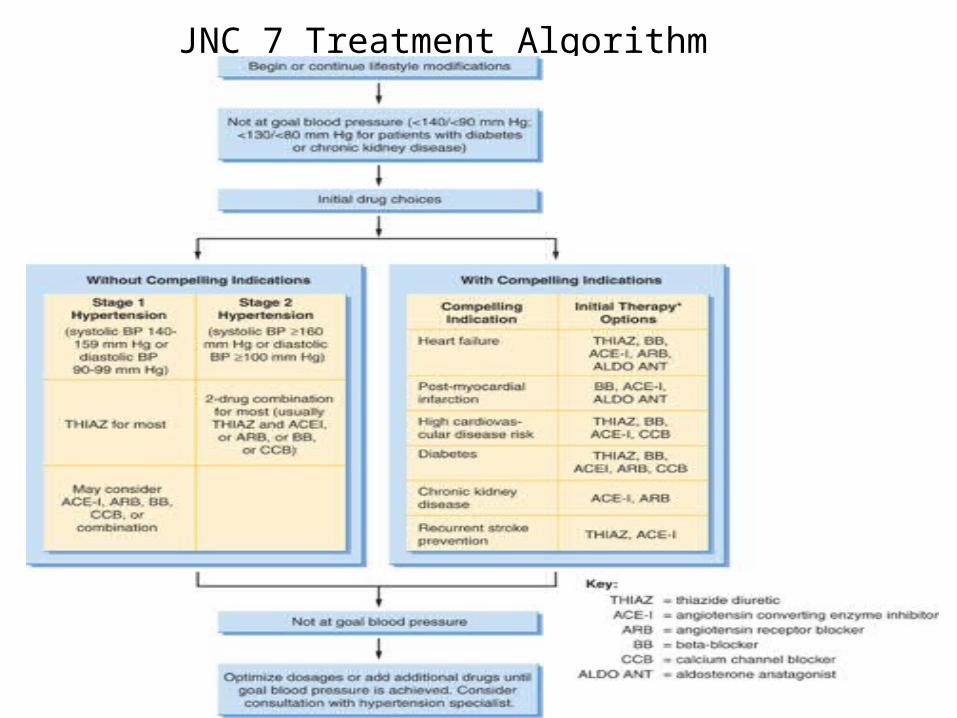
JNC 7 Treatment Algorithm
• Persons with diabetes mellitus or chronic renal disease as evidenced by a reduced GFR or an elevated serum creatinine have a lower goal pressure of 130/80 (JNC 7).

Lifestyle Modifications
• Weight loss• Reduced alcohol intake• Educed sodium intake• Regular physical activity• Diet: high in fruits, vegetables, and low-fat
dairy• DASH diet

Medication Treatment• Usually initial medication treatment is a thiazide
diuretic.• Low doses are initiated and the medication dosage
is increased gradually if blood pressure does not reach target goal.
• Additional medications are added if needed.• Multiple medications may be needed to control
blood pressure.• Lifestyle changes initiated to control BP must be
maintained.
Medication Therapy for Hypertension
• Diuretic and related drugs– Thiazide diuretics– Loop diuretics– Potassium sparing diuretics– Aldosterone receptors blockers
• Central alpha2-agonists and other centrally acting drugs• Beta-blockers• Beta-blockers with intrinsic sympathomimetic activity• Alpha and beta blockers

Medication Therapy for Hypertension (continued)
• Vasodilators• Angiotensin-converting enzyme (ACE)
inhibitors• Angiotenisin II antagonists• Calcium channel blockers
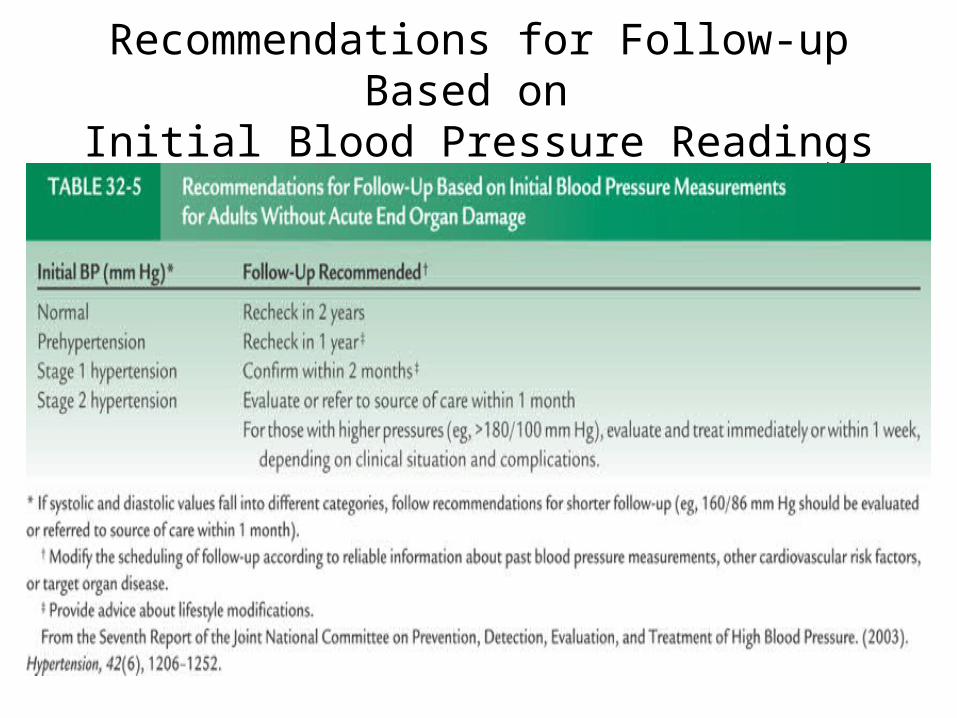
Recommendations for Follow-up Based on Initial Blood Pressure Readings

Nursing History and Assessment
• History and risk factors• Assess potential symptoms of target organ damage– Angina, shortness of breath, altered speech, altered
vision, nosebleeds, headaches, dizziness, balance problems, nocturia
– Cardiovascular assessment: apical and peripheral pulses• Personal, social, and financial factors that will
influence the condition or its treatment

Goals:
• Patient understanding of disease process• Patient understanding of treatment regimen• Patient participation in self-care• Absence of complications

Nursing Diagnoses
• Knowledge deficit regarding the relation of the treatment regimen and control of the disease process
• Noncompliance with therapeutic regimen related to side effects of prescribed therapy

Interventions
• Patient teaching• Support adherence to the treatment regimen• Consultation/collaboration • Follow-up care• Emphasize control rather than cure • Reinforce and support lifestyle changes• A lifelong process
Gerontologic Considerations
• Noncompliance• Include family• Understanding of therapeutic regimen– Reading instructions– Monotherapy
Hypertensive Crises• Hypertensive emergency– Blood pressure > 180/120 and must be lowered
immediately to prevent damage to target organs• Hypertensive urgency – Blood pressure is very high but no evidence of
immediate or progressive target organ damage
Hypertensive Emergency• Reduce BP 25% in first hour.• Reduce to 160/100 over 6 hours.• Then gradual reduction to normal over a period of
days.• Exceptions are ischemic stroke and aortic dissection.• Medications
– IV vasodilators: sodium nitroprusside, nicardipine, fenodopam mesylate, enalaprilat, nitrogylcerin
• Need very frequent monitoring of BP and cardiovascular status.
Hypertensive Urgency
• Patient requires close monitoring of blood pressure and cardiovascular status.
• Assess for potential evidence of target organ damage.
• Medications– Fast-acting oral agents: beta adrenergic blocker—
labetalol; angiotensin-converting enzyme inhibitor— captopril; or alpha2-agonist—clonidine