assessment, interviewing, & observation in clinical psychology dr. kline florida state...
TRANSCRIPT
Assessment, Interviewing, & Assessment, Interviewing, & Observation in Clinical PsychologyObservation in Clinical Psychology
Dr. KlineDr. Kline
Florida State UniversityFlorida State University
I. Clinical Assessment: QuestionsI. Clinical Assessment: Questions 1. What are goals of assessment?1. What are goals of assessment?
2. How is assessment carried out?2. How is assessment carried out?
3. What types of data are obtained?3. What types of data are obtained?
4. How does assessment allow us to make 4. How does assessment allow us to make inferences regarding treatment?inferences regarding treatment?

Why do Clinicians make assessments?Why do Clinicians make assessments? While most individuals speculate why people behave the way While most individuals speculate why people behave the way
they do, they do, they aren’t formally trained to make assessments they aren’t formally trained to make assessments regarding others’ actions & motivesregarding others’ actions & motives. .
Clinical psychologists are trained to systematically & formally Clinical psychologists are trained to systematically & formally examine behaviors of peopleexamine behaviors of people to determine if there are mental to determine if there are mental problems, behavior problems, family dysfunctions, & evidence problems, behavior problems, family dysfunctions, & evidence of of psychopathologypsychopathology..
By conducting assessments, Clinicians can determine an By conducting assessments, Clinicians can determine an individual’s individual’s diagnosisdiagnosis and the best course of action to and the best course of action to treattreat the the disorder/problem.disorder/problem.
Unfortunately, while Clinicians may be more objective than lay Unfortunately, while Clinicians may be more objective than lay individuals, individuals, they have their biases as wellthey have their biases as well which effect the which effect the assessment tools they use to examine an individual & possibly assessment tools they use to examine an individual & possibly the treatment plan as well.the treatment plan as well.
The Clinical Assessment ProcessThe Clinical Assessment Process Clinicians gather information (data) on individuals in a formal Clinicians gather information (data) on individuals in a formal
systematic fashion to determine the problem & subsequent treatment systematic fashion to determine the problem & subsequent treatment plan.plan.
At each stage in the assessment process, the Clinician faces At each stage in the assessment process, the Clinician faces challenges such aschallenges such as::
How do we gather the data?How do we gather the data? How much information is enough?How much information is enough? What kinds of data are important (valuable)?What kinds of data are important (valuable)? How can we eliminate inaccurate/useless information?How can we eliminate inaccurate/useless information? How do we put the information together to form a diagnosis?How do we put the information together to form a diagnosis? How do we avoid our own biases coming into the picture?How do we avoid our own biases coming into the picture? Who gets to see the results of the assessment & for what purposes?Who gets to see the results of the assessment & for what purposes? How will the assessment results effect the clients?How will the assessment results effect the clients? How do we ensure confidentiality of the assessment?How do we ensure confidentiality of the assessment?
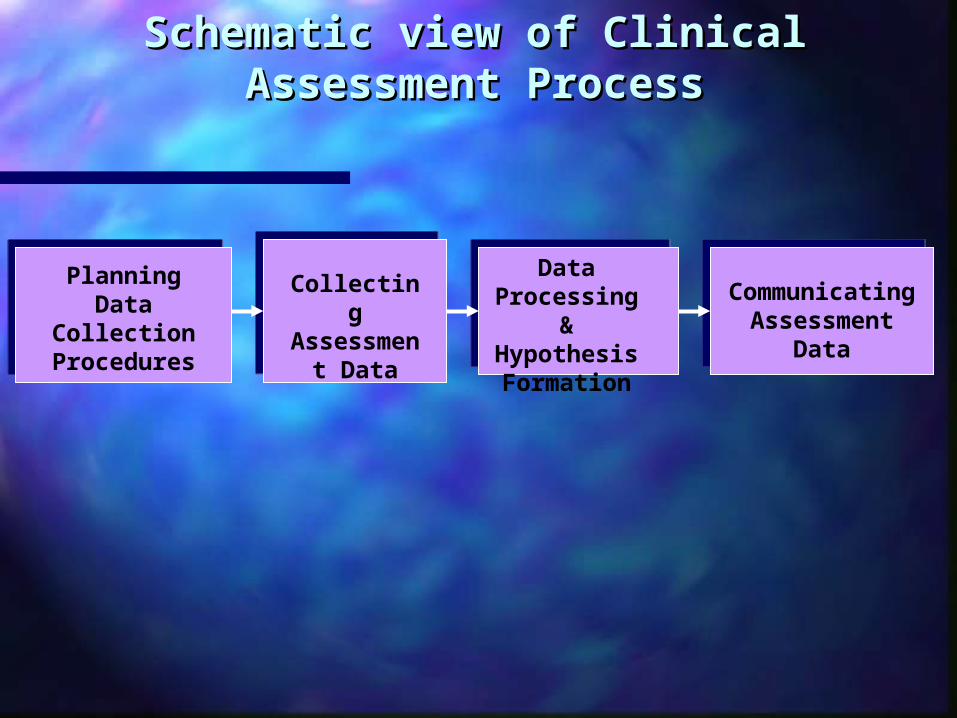
Schematic view of Clinical Assessment ProcessSchematic view of Clinical Assessment Process
Planning Data Collection Procedures
Collecting Assessment
Data
Data Processing & Hypothesis Formation
Communicating Assessment Data
A. Clinical Assessment Issues:A. Clinical Assessment Issues: 1. 1. Planning for AssessmentPlanning for Assessment Before conducting a clinical assessment, we have to two issues Before conducting a clinical assessment, we have to two issues
to address.to address. a. a. What do we want to knowWhat do we want to know?? b. b. How do we find out about itHow do we find out about it??
The answer to both questions hinges largely on the The answer to both questions hinges largely on the specific specific approachapproach (psychodynamic, behavioral, humanistic, etc.) the (psychodynamic, behavioral, humanistic, etc.) the Clinician is likely to adopt.Clinician is likely to adopt.
The Clinician’s approach may have a large impact on the type of The Clinician’s approach may have a large impact on the type of data they want to gather for their assessment. data they want to gather for their assessment.
Furthermore, the amount of data that could be obtained is vast Furthermore, the amount of data that could be obtained is vast (from biological to life record) & so it would be difficult to know (from biological to life record) & so it would be difficult to know just how much data is necessary to make an accurate assessment.just how much data is necessary to make an accurate assessment.

Case Study Guide-provides a general overview of the clientCase Study Guide-provides a general overview of the client
Levels of Assessment & Some Representative Data from EachLevels of Assessment & Some Representative Data from Each
1. Somatic- Blood type, RH factor, autonomic stress response pattern, kidney & liver function, genetic data, basal metabolism, vision, toxicology,
neuroimaging data (fMRI, Cat, Pet).
2. Physical- Ht, wt, sex, eye color, hair color, body type
3. Demographic- Name, age, address, phone#, occupation, education, income, marital status, # of children.
4. Overt Behavioral- Reading speed, eye-hand coordination, frequency of fighting with others, conversational skill, interpersonal assertiveness,
occupational competence, smoking habits.
5. Cognitive- Response to intelligence test items, reports on thoughts, performance on tests of information processing or cognitive complexity, response
to tests of reality perception and structuring.
6. Emotional- Reports of feelings, responses to tests measuring mood states, physiological responsiveness.
7. Environmental- Location& characteristics of housing; # & description of cohabitants, job requirements & characteristics; physical & behavioral
characteristics of family, friends, & coworkers; nature of specific cultural or subcultural standards & traditions; general economic conditions; geographical location.
Factors Guiding Assessment ChoicesFactors Guiding Assessment Choices
1. 1. Often Case Study Guides are associated with a particular Often Case Study Guides are associated with a particular theoretical approach to clinical psychologytheoretical approach to clinical psychology..
This influences the kinds of questions & data the Clinician will pursueThis influences the kinds of questions & data the Clinician will pursue. .
E.g., a Clinician with a heavy biological orientation, will want to obtain biological data E.g., a Clinician with a heavy biological orientation, will want to obtain biological data (fMRI, Pet, toxicology, etc.) to see if the behavior is related to an organic cause (brain (fMRI, Pet, toxicology, etc.) to see if the behavior is related to an organic cause (brain infection, tumor, stroke, dementia, drug use, etc.). infection, tumor, stroke, dementia, drug use, etc.).
2. 2. Diagnoses are also influenced by the theoretical approach Diagnoses are also influenced by the theoretical approach the Clinician is adopting.the Clinician is adopting.
E.g., A Clinician with a E.g., A Clinician with a cognitive-behavioral approachcognitive-behavioral approach will not only make assessments will not only make assessments regarding client’s thinking skills, thought patterns, & the maladaptive thoughts, but will regarding client’s thinking skills, thought patterns, & the maladaptive thoughts, but will tend to make diagnoses based on this paradigm as well (changing the client’s tend to make diagnoses based on this paradigm as well (changing the client’s maladaptive thoughts to reduce the problem behaviors.) maladaptive thoughts to reduce the problem behaviors.)
3. 3. Research on the reliability & validity of assessment methods Research on the reliability & validity of assessment methods are used to determine which types of data are gathered.are used to determine which types of data are gathered.
Issues in Testing:Issues in Testing:
A. Reliability—consistency with which a A. Reliability—consistency with which a test measures what it purports to measure.test measures what it purports to measure.
Types of reliability:Types of reliability: *inter-rated reliability*inter-rated reliability *test-retest reliability*test-retest reliability
B. ValidityB. Validity
Types of validity:Types of validity:
**content validitycontent validity-does test measure content -does test measure content area?area?
**face validityface validity—on surface does test —on surface does test measure what it’s supposed to.measure what it’s supposed to.

Validity contd.Validity contd.
Concurrent validityConcurrent validity-does the index being -does the index being used to measure a type of abnormal used to measure a type of abnormal behavior agree with another index used to behavior agree with another index used to measure the same behavior.measure the same behavior.
Predictive validityPredictive validity-does measure -does measure accurately predict the occurrence of some accurately predict the occurrence of some event.event.
Goals of Clinical Assessment: 3 goalsGoals of Clinical Assessment: 3 goals
1. 1. Diagnostic Classification-Diagnostic Classification- Determining the Determining the diagnosis for the problem behavior. What is it?diagnosis for the problem behavior. What is it?
2. 2. DescriptionDescription- understanding the social, - understanding the social, cultural, & physical context of behavior.cultural, & physical context of behavior.
3. 3. PredictionPrediction- What will people do in a variety - What will people do in a variety of settings based on their past behavior?of settings based on their past behavior?

Why an “accurate diagnosis” is so Why an “accurate diagnosis” is so important in Clinical psychology?important in Clinical psychology?
1. The appropriate treatment plan cannot be implemented 1. The appropriate treatment plan cannot be implemented until we have an until we have an accurate definition of what is wrong accurate definition of what is wrong with the client.with the client.
2. 2. Research into causes of psychological disorders Research into causes of psychological disorders requires reliable & valid identification of disorders & requires reliable & valid identification of disorders & accurate differentiation of one disorder from anotheraccurate differentiation of one disorder from another (Nietzel et al., 2003).(Nietzel et al., 2003).
3. 3. Classification allows multiple Clinicians to discuss Classification allows multiple Clinicians to discuss a client’s case or cases based on a given disorder a client’s case or cases based on a given disorder accurately & efficientlyaccurately & efficiently (i.e., standardized of (i.e., standardized of diagnosis). diagnosis).

Diagnostic standard in Clinical PsychologyDiagnostic standard in Clinical Psychology In In 19521952, The American Psychiatric Association published its first , The American Psychiatric Association published its first
official classification system, the “official classification system, the “Diagnostic and Statistical Diagnostic and Statistical Manual of mental disorders.Manual of mental disorders.” Several revisions have been made ” Several revisions have been made to the DSM over the years.to the DSM over the years.
Clinicians currently use the fourth edition of the DSM or The Clinicians currently use the fourth edition of the DSM or The DSM-IVDSM-IV. This version was published in 1994 and revised in . This version was published in 1994 and revised in 2000. Plans for a DSM-V are in the works!! 2000. Plans for a DSM-V are in the works!!
The DSM-IV is based on a multi-axial classification system. The DSM-IV is based on a multi-axial classification system.
Each individual is rated on 5 separate dimensions or axes. Each individual is rated on 5 separate dimensions or axes.
Axis IAxis I: Psychiatric disorders, excludes : Psychiatric disorders, excludes personality disorders & mental retardation.personality disorders & mental retardation.
Axis IIAxis II: Personality disorders & mental : Personality disorders & mental retardation.retardation.
Axis IIIAxis III: General medical conditions: General medical conditions
Axis IV:Axis IV: Psychosocial & environmental Psychosocial & environmental problems. problems.
Axis VAxis V: Current level of functioning: Global : Current level of functioning: Global Assessment ScaleAssessment Scale
Axes I & II comprise the classification of Axes I & II comprise the classification of abnormal behavior.abnormal behavior.
Most individuals consult a clinician for an Most individuals consult a clinician for an Axis I condition (e.g., depression).Axis I condition (e.g., depression).
Clinician must examine if Axis II disorder Clinician must examine if Axis II disorder is also present. is also present.
Axis II disorders make treating Axis I Axis II disorders make treating Axis I disorders more complicated.disorders more complicated.

Axis I DisordersAxis I Disorders
1. Disorders Usually First Diagnosed in 1. Disorders Usually First Diagnosed in Infancy, Childhood, or AdolescenceInfancy, Childhood, or Adolescence
*separation anxiety*separation anxiety *attention-deficit/hyperactivity disorder*attention-deficit/hyperactivity disorder *autism*autism

2. Mood disorders-disturbances 2. Mood disorders-disturbances in emotion and behavior.in emotion and behavior.
*Major Depression (unipolar depression)*Major Depression (unipolar depression) *Mania*Mania *Bipolar disorder (Manic Depression)*Bipolar disorder (Manic Depression) *Cyclothymia (Chronic mood disorder)*Cyclothymia (Chronic mood disorder) DysthymiaDysthymia
3. Schizophrenia-disturbances of 3. Schizophrenia-disturbances of thought, emotions, and behavior.thought, emotions, and behavior.
Different types:Different types:
Paranoid SchizophreniaParanoid Schizophrenia Catatonic SchziophreniaCatatonic Schziophrenia Undifferentiated SchizophreniaUndifferentiated Schizophrenia
4. Anxiety disorders4. Anxiety disorders
Generalized anxiety disorder (GAD)Generalized anxiety disorder (GAD) PhobiasPhobias Panic DisorderPanic Disorder Obsessive-compulsive disorder (OCD)Obsessive-compulsive disorder (OCD) Post-traumatic stress disorder (PTSD)Post-traumatic stress disorder (PTSD) Acute Stress DisorderAcute Stress Disorder
5. Sexual disorders5. Sexual disorders
Gender Identity disorderGender Identity disorder TransvestismTransvestism PedophiliaPedophilia VoyeurismVoyeurism ExhibitionismExhibitionism Sadism/MasochismSadism/Masochism Rape traumaRape trauma

Axis II: personality disordersAxis II: personality disorders Schizoid PD—person is aloof, has few friends, Schizoid PD—person is aloof, has few friends,
& is indifferent to praise/criticism.& is indifferent to praise/criticism.
Borderline PD—erratic behavior, impulsivity, Borderline PD—erratic behavior, impulsivity, and instability in relationships/ mood, & self-and instability in relationships/ mood, & self-image.image.
Narcissistic PD—people who have malignant Narcissistic PD—people who have malignant grandiosity of their own self-importance.grandiosity of their own self-importance.

Axis II (contd.)Axis II (contd.)
Histrionic PD- marked by an overly Histrionic PD- marked by an overly dramatic display of behavior that is for dramatic display of behavior that is for show (no real substance underneath).show (no real substance underneath).
Antisocial PD—marked by violent acts & Antisocial PD—marked by violent acts & lack of empathy for others. lack of empathy for others.

2. Collecting Assessment Data: Four main 2. Collecting Assessment Data: Four main sourcessources
1. 1. Interviews- Interviews- Clinicians may simply ask the client questions to Clinicians may simply ask the client questions to find out what is happening in his or her life. find out what is happening in his or her life.
Advantages of interviewsAdvantages of interviews: : *Allows Clinician to obtain a sample of the client’s verbal & non-*Allows Clinician to obtain a sample of the client’s verbal & non-
verbal behavior in a social interaction.verbal behavior in a social interaction.
*No equipment is necessary to conduct an interview.*No equipment is necessary to conduct an interview.
*Interviews are flexible.*Interviews are flexible.
2. 2. Observations –Observations –Clinicians may want to Clinicians may want to observe non-verbal behaviors in a variety of observe non-verbal behaviors in a variety of situations.situations.
The goal here is to look at what the client is The goal here is to look at what the client is “doing” rather than what he/she is saying.“doing” rather than what he/she is saying.
Clinicians may observe:Clinicians may observe: client’s eye contactclient’s eye contact how distractible is the clienthow distractible is the client Does the client seem comfortable or agitatedDoes the client seem comfortable or agitated Is the client coherent or ramblingIs the client coherent or rambling Does client keep changing topic in social Does client keep changing topic in social
interaction?interaction?

3. 3. Tests- Tests- Clinicians may administer tests to Clinicians may administer tests to assess a variety of abilities, functions, traits, assess a variety of abilities, functions, traits, & aptitudes.& aptitudes. Advantage of testsAdvantage of tests
*Tests may be more reliable than interviews.*Tests may be more reliable than interviews.
*Tests that have been standardized, allow Clinicians to *Tests that have been standardized, allow Clinicians to obtain data on a client or multiple clients that can be obtain data on a client or multiple clients that can be compared with individuals in the general population.compared with individuals in the general population.
*Responses on tests can be *Responses on tests can be quantified, providing quantified, providing more objective datamore objective data with which to make a more with which to make a more accurate assessment. accurate assessment.
4. 4. Life Records Life Records – Clinicians obtain data – Clinicians obtain data about a client from this life history.about a client from this life history.
Our life history may provide useful information about our Our life history may provide useful information about our past behavior.past behavior.
Examples of life records:Examples of life records: Academic transcripts, driving record, financial records, Academic transcripts, driving record, financial records,
diaries/journals, occupational history, etcdiaries/journals, occupational history, etc..
Advantages of Life recordsAdvantages of Life records:: *Easy to obtain*Easy to obtain *You don’t have to worry about memory problems or biases *You don’t have to worry about memory problems or biases
in obtaining this type of data.in obtaining this type of data. *Allows you to summarize a client’s behavior over a long *Allows you to summarize a client’s behavior over a long
span of time. span of time.
3. Processing Assessment Data3. Processing Assessment Data Once the Clinician has obtained data on a client, Once the Clinician has obtained data on a client,
they have to make an inference regarding the they have to make an inference regarding the client’s diagnosis & subsequent treatment plan.client’s diagnosis & subsequent treatment plan.
This is easier said than done, as clinical This is easier said than done, as clinical inference can be tricky.inference can be tricky.
Again, the theoretical approach of the Again, the theoretical approach of the clinician plays a large role in how they clinician plays a large role in how they interpret the assessment data they’ve interpret the assessment data they’ve obtained. obtained.
Three main ways Clinicians view Assessment Three main ways Clinicians view Assessment Information:Information: 1. 1. SamplesSamples- Clinicians may examine the raw behavior - Clinicians may examine the raw behavior
of the client (E.g., What the client did?)of the client (E.g., What the client did?)
2. 2. Correlates-Correlates- The sample of a client’s raw behavior The sample of a client’s raw behavior may be viewed as a correlate to other aspects of their may be viewed as a correlate to other aspects of their life (Neitzel et al., 2003).life (Neitzel et al., 2003).
3. 3. Signs-Signs- The raw behavior sample may be viewed as The raw behavior sample may be viewed as a sign of other less obvious client traits a sign of other less obvious client traits (characteristics). (characteristics).

1. Sample behavior1. Sample behavior ““A person overdoses on pain medication in a hotel room one night before A person overdoses on pain medication in a hotel room one night before
going to bed. Fortunately, the individual is saved after being discovered by going to bed. Fortunately, the individual is saved after being discovered by the hotel maid and is rushed to the hospital.”the hotel maid and is rushed to the hospital.”
The The incidentincident is the is the samplesample in this case. On this data alone the Clinician might in this case. On this data alone the Clinician might infer the following:infer the following:
*Conclude the client had access to lethal meds.*Conclude the client had access to lethal meds. *Client did not wish to be saved as no one was warned of the suicide attempt.*Client did not wish to be saved as no one was warned of the suicide attempt. *Under similar situations, the client may attempt suicide again.*Under similar situations, the client may attempt suicide again.
Problems—No effort is made by the Clinician to Problems—No effort is made by the Clinician to ascertain “why” the client made the attempt in the first ascertain “why” the client made the attempt in the first placeplace. .
2. Correlates- The client’s behavior may be 2. Correlates- The client’s behavior may be viewed for its correlation with other viewed for its correlation with other individuals’ behaviors.individuals’ behaviors. *The client is likely to be elderly, single, divorced, or widowed and lives alone *The client is likely to be elderly, single, divorced, or widowed and lives alone
with a physical ailment.with a physical ailment.
*The client is or has been depressed.*The client is or has been depressed.
*The client has little support from family & friends.*The client has little support from family & friends.
With the correlates method, the Clinician may look at the facts related to the With the correlates method, the Clinician may look at the facts related to the client’s individual behavior as well as the how this behavior is related to the client’s individual behavior as well as the how this behavior is related to the Clinician’s knowledge base of factors associated with suicide attempts. Clinician’s knowledge base of factors associated with suicide attempts.
Inferences are more accurate when more information is known about the Inferences are more accurate when more information is known about the relationships between variablesrelationships between variables..

3. Signs- The suicide attempt may be viewed 3. Signs- The suicide attempt may be viewed as a sign of other lesser known client traits.as a sign of other lesser known client traits. Inferences made from sign perspective (Neitzel et al., 2003)Inferences made from sign perspective (Neitzel et al., 2003)
*The client’s aggressive impulses have been turned against the self.*The client’s aggressive impulses have been turned against the self.*The client’s behavior reflects intrapsychic conflicts.*The client’s behavior reflects intrapsychic conflicts.*The pill taking may be an unconscious cry for help. *The pill taking may be an unconscious cry for help.
Here a Clinician with a psychodynamic approach makes inferences well Here a Clinician with a psychodynamic approach makes inferences well beyond the scope of the assessment data in determining why the individual beyond the scope of the assessment data in determining why the individual made the suicide attempt.made the suicide attempt.
Caution– the sign approach may lead to inaccurate inferences regarding a Caution– the sign approach may lead to inaccurate inferences regarding a client’s motives, actions, traits, etc. This is one of the fundamental client’s motives, actions, traits, etc. This is one of the fundamental problems using such a method. Nevertheless, sometimes Clinicians go with problems using such a method. Nevertheless, sometimes Clinicians go with a “a “hunchhunch” in explaining why a person behaved a given way. ” in explaining why a person behaved a given way.
4. Communicating Assessment Data4. Communicating Assessment Data Once the Clinician as assessed the data they Once the Clinician as assessed the data they
write up a detailed report for other Clinicians write up a detailed report for other Clinicians and professionals to view.and professionals to view.
This report needs to be clear, relevant to the This report needs to be clear, relevant to the treatment outcomes proposed, and efficient treatment outcomes proposed, and efficient for the treatment to be implemented. for the treatment to be implemented.
II. Clinical Interviews:II. Clinical Interviews:
Clinicians have a Clinicians have a conversation with the client conversation with the client with the purpose of learning more about the with the purpose of learning more about the client.client.
This allows the Clinician to both observe This allows the Clinician to both observe verbal & non-verbal behavior in a social verbal & non-verbal behavior in a social interaction (providing two sources of interaction (providing two sources of information).information).

A. Types of Clinical Interviews:A. Types of Clinical Interviews: 1. 1. Intake interviews-Intake interviews- are the most common form of interviews are the most common form of interviews
in which clients come to clinicians because of a problem they are in which clients come to clinicians because of a problem they are having.having.
Clinicians try to determine several things from intake Clinicians try to determine several things from intake interviews:interviews:
*Can I help this person?*Can I help this person? *Is this client’s problem within my area of expertise?*Is this client’s problem within my area of expertise? *Will this person benefit from treatment?*Will this person benefit from treatment? *Can I make a diagnosis of the problem?*Can I make a diagnosis of the problem? *Can I establish a rapport with this person to treat them?*Can I establish a rapport with this person to treat them?
2. 2. Problem-Referral InterviewsProblem-Referral Interviews:: In these interviews, the client has been referred to the Clinician In these interviews, the client has been referred to the Clinician
from another sources or agency (psychiatrist, court, school, from another sources or agency (psychiatrist, court, school, employer, social service agency, etc.). employer, social service agency, etc.).
These individuals are sent to the Clinician to address a These individuals are sent to the Clinician to address a specific referral issue. specific referral issue.
Examples include:Examples include: Is the person stand to fit trial?Is the person stand to fit trial? Is the person psychotic?Is the person psychotic? Is the person mentally retarded or developmentally delayed?Is the person mentally retarded or developmentally delayed? Is the parent fit for custody? Is the parent in the best interest of Is the parent fit for custody? Is the parent in the best interest of
the child?the child?
3. 3. Orientation InterviewsOrientation Interviews::
These interviews are conducted to provide the client These interviews are conducted to provide the client with information regarding the assessment, treatment, with information regarding the assessment, treatment, or research procedures to be implemented.or research procedures to be implemented.
AdvantagesAdvantages:: 1. Client learns more about assessment & treatment 1. Client learns more about assessment & treatment
outcomes in his/her situation.outcomes in his/her situation. 2. Are important for research participants so that we 2. Are important for research participants so that we
can learn more about assessment & treatment outcomes can learn more about assessment & treatment outcomes (e.g., efficacy of therapeutic methods.)(e.g., efficacy of therapeutic methods.)
4. 4. Termination or Debriefing InterviewsTermination or Debriefing Interviews These interviews are conducted once These interviews are conducted once
assessment has been completed. Essentially, assessment has been completed. Essentially, they allow the Clinician to convey what they they allow the Clinician to convey what they “found” during the assessment.“found” during the assessment.
E.g., following a problem-referral interview E.g., following a problem-referral interview the clinician may have enough information to the clinician may have enough information to convey the answer the client regarding the convey the answer the client regarding the referral question. referral question.
*Yes, you are fit to stand trial!!)*Yes, you are fit to stand trial!!)
5. 5. Crisis InterviewsCrisis Interviews::If a client is having a crisis (e.g., rape hotline, domestic If a client is having a crisis (e.g., rape hotline, domestic
abuse, etc.) where they need the Clinician immediately, abuse, etc.) where they need the Clinician immediately, a crisis interview may be conducted.a crisis interview may be conducted.
Crisis interviews are designed to provide immediate Crisis interviews are designed to provide immediate social & administrative support, collect assessment social & administrative support, collect assessment data, and provide help as quickly as possible. data, and provide help as quickly as possible.
Because this is a crisis, the Clinician needs to be as calm Because this is a crisis, the Clinician needs to be as calm as possible & determine if the client is a danger to as possible & determine if the client is a danger to themselves or others. The Clinician may also have to themselves or others. The Clinician may also have to determine if the individual needs to be hospitalized for determine if the individual needs to be hospitalized for their safety. their safety.

B. Interview Structure: the most fundamental part B. Interview Structure: the most fundamental part of an interview is its structure.of an interview is its structure. Structure refers to the degree to which the interviewer Structure refers to the degree to which the interviewer
determines the content and course of the determines the content and course of the conversation. conversation.
There are two There are two basic kinds of structurebasic kinds of structure for interviews: for interviews: 1. Nondirective interviews1. Nondirective interviews - -in which the clinician in which the clinician
does a little as possible to stop the natural flow of the does a little as possible to stop the natural flow of the conversation with the client.conversation with the client.
2. Structured interview2. Structured interview -the interview is carefully -the interview is carefully planned with a systematic format. planned with a systematic format.

Structured interviewsStructured interviews To make reliable and valid diagnoses, clinicians To make reliable and valid diagnoses, clinicians
need to gather need to gather standardizedstandardized information on information on patients.patients.
SCID (Structured Clinical Interview)- a SCID (Structured Clinical Interview)- a structured interview for Axis I of the DSM.structured interview for Axis I of the DSM.
Questions are in prescribed order for interviewer Questions are in prescribed order for interviewer to ask. The SCID is a branching interview, which to ask. The SCID is a branching interview, which means the patient’s response to one question, will means the patient’s response to one question, will determine the next question asked.determine the next question asked.
C. Stages in the Interview: Basic formatC. Stages in the Interview: Basic format Stage 1: Beginning the Interview – The clinician Stage 1: Beginning the Interview – The clinician
begins the interview in a comfortable setting, and begins the interview in a comfortable setting, and by trying to establish rapport with the client.by trying to establish rapport with the client.
This can be done by:This can be done by: *Sitting fairly close to the client (when possible)*Sitting fairly close to the client (when possible) *Keeping physical barriers between the client & *Keeping physical barriers between the client &
Clinician to a minimumClinician to a minimum *Start interview with non-threatening small talk to *Start interview with non-threatening small talk to
allow the client time to relaxallow the client time to relax *Review client’s referral or background info so the *Review client’s referral or background info so the
Clinician may have some information on the client Clinician may have some information on the client before starting the interview.before starting the interview.
*Provide reassurance and support.*Provide reassurance and support.

Stage 2: The middle of the interviewStage 2: The middle of the interview The clinician should try to make the transition The clinician should try to make the transition
from the beginning to the middle of the from the beginning to the middle of the interview as smooth as possible.interview as smooth as possible.
Non-directive tacticsNon-directive tactics: Most Clinicians begin the : Most Clinicians begin the second stage of the interview with non-directive second stage of the interview with non-directive open-ended open-ended questions. questions.
E.g., “What brings you here today?”E.g., “What brings you here today?” This puts onus on client & allows them to direct This puts onus on client & allows them to direct
the flow of the conversation.the flow of the conversation.
Active ListeningActive Listening Is a non-directive tactic where the clinician responds to the Is a non-directive tactic where the clinician responds to the
client’s speech in ways that client’s speech in ways that indicate understandingindicate understanding & facilitate & facilitate further communication.further communication.
E.g., Clinician may say something like, “E.g., Clinician may say something like, “I seeI see” or “” or “I’m with I’m with youyou,” in response to a major point a client has just made. ,” in response to a major point a client has just made.
Related to this concept is “Related to this concept is “paraphrasingparaphrasing” ” in which Clinicians in which Clinicians restate what their clients say to demonstrate they are listening to restate what their clients say to demonstrate they are listening to them and are willing to give the client a chance to correct the them and are willing to give the client a chance to correct the comment if misinterpretedcomment if misinterpreted..
Rogers called “paraphrasing” Rogers called “paraphrasing” reflectionreflection. .
Reflection examples:Reflection examples: Example A:Example A: Client: Sometimes I get so mad at my boss, I could just kill himClient: Sometimes I get so mad at my boss, I could just kill him Clinician: You would just like to get rid of your boss altogether.Clinician: You would just like to get rid of your boss altogether.
Example B:Example B:
Client: Sometimes I get so mad at my boss, I could just kill him.Client: Sometimes I get so mad at my boss, I could just kill him.
Clinician: Your boss really upsets you sometimes.Clinician: Your boss really upsets you sometimes.
In Example A, the Clinician restates the client’s remark. This does show active In Example A, the Clinician restates the client’s remark. This does show active listening. In Example B, the Clinician reflects the emotion or feeling made listening. In Example B, the Clinician reflects the emotion or feeling made in the client’s remark. in the client’s remark.
Both versions usually will facilitate the client to continue discussing the Both versions usually will facilitate the client to continue discussing the program. program.
Directive techniques:Directive techniques:
Clinicians may also use more directive Clinicians may also use more directive tactics to determine what’s bothering their tactics to determine what’s bothering their clients. This is usually done after a good clients. This is usually done after a good rapport has been established so as to avoid rapport has been established so as to avoid threatening the client.threatening the client.
Stage 3: Closing the InterviewStage 3: Closing the Interview
The Clinician closes the interview by making sure The Clinician closes the interview by making sure they have enough information for assessment as well they have enough information for assessment as well as continuing to establish a good rapport with the as continuing to establish a good rapport with the client.client.
The clinician may reiterate what was covered in the The clinician may reiterate what was covered in the interview for clarification and for the chance to ask interview for clarification and for the chance to ask more questions before closing the interview. more questions before closing the interview.
This allows the clinician to summarize the interview This allows the clinician to summarize the interview content and to make sure nothing was misunderstood content and to make sure nothing was misunderstood or omitted. or omitted.