assistant - american medical association · american medical association bulletin 2014 clinical...
TRANSCRIPT

AssistantOfficial source for CPT coding guidance
Volume 24 Bulletin 1/2014
AMERICAN MEDICAL ASSOCIATION
BULLETIN 2014
Clinical Documentation Assessment: Looking at the Patterns Between the ICD-9-CM and ICD-10-CM Coding Systems
Clinical documentation specificity is one of the most important characteristics of the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) coding system. Additional details in clinical documentation provides more information, suggestions, guidance, and checklists—all of which will be used by coding professionals to select the appropriate codes that most accurately describe the procedure(s)/service(s) provided.
One aspect of performing a clinical document assessment to test an organization’s ICD-10-CM readiness is to assess the quality of its current medical record documentation. In order to do so, it is necessary to be able to identify proper clinical documentation for the ICD-10-CM code set and understand the similarities and differences between the clinical concepts of the ICD-9-CM and ICD-10-CM coding systems. This article provides an overview of conducting a clinical documentation assessment to prepare for the
ICD-10-CM transition, and looks at the similarities and differences between the clinical concepts of ICD-9-CM and ICD-10-CM.
Conducting a Clinical Documentation AssessmentConducting a clinical documentation assessment is a step toward preparing for the transition to the ICD-10-CM code set that does not first require updates to the practice man-agement system (PMS) or electronic health record (EHR). It is important to note that although a clinical documenta-tion assessment can be done without updating either the PMS or EHR right away, updates to these systems may be necessary depending on the results of the assessment. Clinical practices may perform clinical documentation assessments by using current patient charts as samples to code patient scenarios with the ICD-10-CM code set. The
Bulletin_#1_060414_2ndP.indd 1 6/5/14 2:30 PM

2
CPT® Assistant Bulletin / Volume 24 Issue 1 • 2014
charts selected as samples should include a variety of patient conditions, including the most common diagnoses seen in the practice, as well as some conditions that are less com-monly seen. In addition, when conducting a documentation assessment, it is important to identify the information that is considered necessary to complete the coding process but is missing or insufficient in current documentation.
Although current clinical documentation practices may be sufficient for ICD-10-CM coding, it is anticipated that some changes in documentation may be necessary to better describe patients’ clinical scenarios. Due to the increased specificity of the ICD-10-CM diagnosis codes, clinical documentation should be detailed enough to allow coding professionals to identify the most accurate code from the ICD-10-CM code set.
The American Academy of Professional Coders (AAPC) has conducted thousands of documentation assessments. And, based on these assessments, they have concluded that only 63%1 of current documentation is detailed enough to use with the ICD-10-CM code set, which means 4 out of 10 claims could be rejected as insufficient due to a lack of detailed documentation. (Note: This average is mistakenly
listed as 37% on the AAPC’s Web site, which is incorrect.) In addition, if an imprecise ICD-10-CM code is reported—one that does not exactly support a patient’s diagnosis—the claim may not be rejected, but such low accuracy in code selection may result in improper payment or a request by the third-party payer for additional information.
Comparing the Clinical Concepts in ICD-9-CM and ICD-10-CMMany of the clinical concepts found in the ICD-10-CM coding system are already included in the ICD-9-CM code set. However, a clear understanding of the clinical concepts new in ICD-10-CM will allow for documentation specific enough to support accurate coding practices, even if not all of the new ICD-10-CM features apply to all special-ties and not all physicians would need to use them for coding purposes. See Table 1 for a snapshot of the features and examples of the clinical concepts of the ICD-10-CM coding system that are already included in the ICD-9-CM coding system.
Table 1. ICD-10-CM Clinical Concepts From ICD-9-CM: Features and Examples
Features Examples
Coding Concept Description of Coding Concept
Code Number
Code Descriptor
Type Describes a condition that is typically considered a type of a condition, eg, malignant neoplasm, pathological fracture, etc
I26.01
C18.6
N85.01
H35.031
Septic pulmonary embolism with acute cor pulmonale
Malignant neoplasm of descending colon
Benign endometrial hyperplasia
Hypertensive retinopathy, right eye
Temporal factors Relates a condition to a particular time parameter, eg, acute, chronic, recurrent, etc
J01.01
K25.7
J45.21
I48.2
Acute recurrent maxillary sinusitis
Chronic gastric ulcer without hemorrhage or perforation
Mild intermittent asthma with (acute) exacerbation
Chronic atrial fibrillation
Note: Underlined words indicate information in the code descriptor that meets the coding concept.
Bulletin_#1_060414_2ndP.indd 2 6/5/14 2:30 PM
CPT® Assistant Bulletin / Volume 24 Issue 1 • 2014
3
Features Examples
Coding Concept Description of Coding Concept
Code Number
Code Descriptor
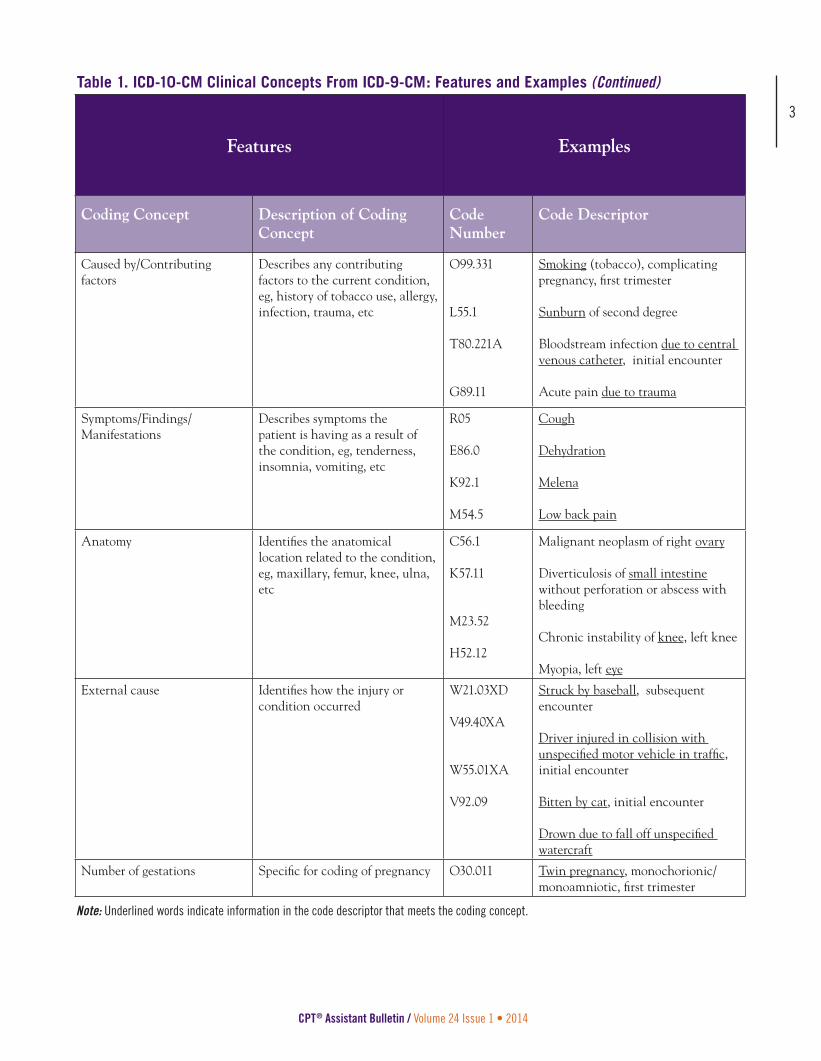
Caused by/Contributing factors
Describes any contributing factors to the current condition, eg, history of tobacco use, allergy, infection, trauma, etc
O99.331
L55.1
T80.221A
G89.11
Smoking (tobacco), complicating pregnancy, first trimester
Sunburn of second degree
Bloodstream infection due to central venous catheter, initial encounter
Acute pain due to trauma
Symptoms/Findings/Manifestations
Describes symptoms the patient is having as a result of the condition, eg, tenderness, insomnia, vomiting, etc
R05
E86.0
K92.1
M54.5
Cough
Dehydration
Melena
Low back pain
Anatomy Identifies the anatomical location related to the condition, eg, maxillary, femur, knee, ulna, etc
C56.1
K57.11
M23.52
H52.12
Malignant neoplasm of right ovary
Diverticulosis of small intestine without perforation or abscess with bleeding
Chronic instability of knee, left knee
Myopia, left eye
External cause Identifies how the injury or condition occurred
W21.03XD
V49.40XA
W55.01XA
V92.09
Struck by baseball, subsequent encounter
Driver injured in collision with unspecified motor vehicle in traffic, initial encounter
Bitten by cat, initial encounter
Drown due to fall off unspecified watercraft
Number of gestations Specific for coding of pregnancy O30.011 Twin pregnancy, monochorionic/monoamniotic, first trimester
Note: Underlined words indicate information in the code descriptor that meets the coding concept.
Table 1. ICD-10-CM Clinical Concepts From ICD-9-CM: Features and Examples (Continued)
Bulletin_#1_060414_2ndP.indd 3 6/5/14 2:30 PM

4
CPT® Assistant Bulletin / Volume 24 Issue 1 • 2014
Features Examples
Coding Concept Description of Coding Concept
Code Number
Code Descriptor
Outcome of delivery Specific for coding of a delivery of a baby
O80 Encounter for full-term uncomplicated delivery
Remission status Identifies that a condition is in remission and no longer active
C92.31
F17.210
F31.71
Myeloid leukemia, in remission
Nicotine dependence, cigarettes, in remission
Bipolar disorder, in partial remission, most recent episode hypomanic
History of Identifies that the patient has a history of the condition
Z85.841
Z87.312
Z87.891
Personal history of malignant neoplasm of brain
Personal history of (healed) stress fracture
Personal history of nicotine dependence
Substance Identifies the substance related to the injury or condition
L23.0
L24.0
Allergic contact dermatitis due to metals
Irritant contact dermatitis due to detergents
Activity Describes the activity that was being done at the time the injury or condition occurred
Y93.02
Y93.82
Activity, running
Activity, spectator at an event
Place of occurrence Identifies the location of the patient at the time of the injury or condition occurred
Y92.010
Y92.321
Y92.61
Kitchen of single-family (private) house as place
Football field as place
Building under construction as place
Note: Underlined words indicate information in the code descriptor that meets the coding concept.
Table 1. ICD-10-CM Clinical Concepts From ICD-9-CM: Features and Examples (Continued)
See Table 2, for some examples and features of the clinical concepts that are new in ICD-10-CM.
Bulletin_#1_060414_2ndP.indd 4 6/5/14 2:30 PM
CPT® Assistant Bulletin / Volume 24 Issue 1 • 2014
5
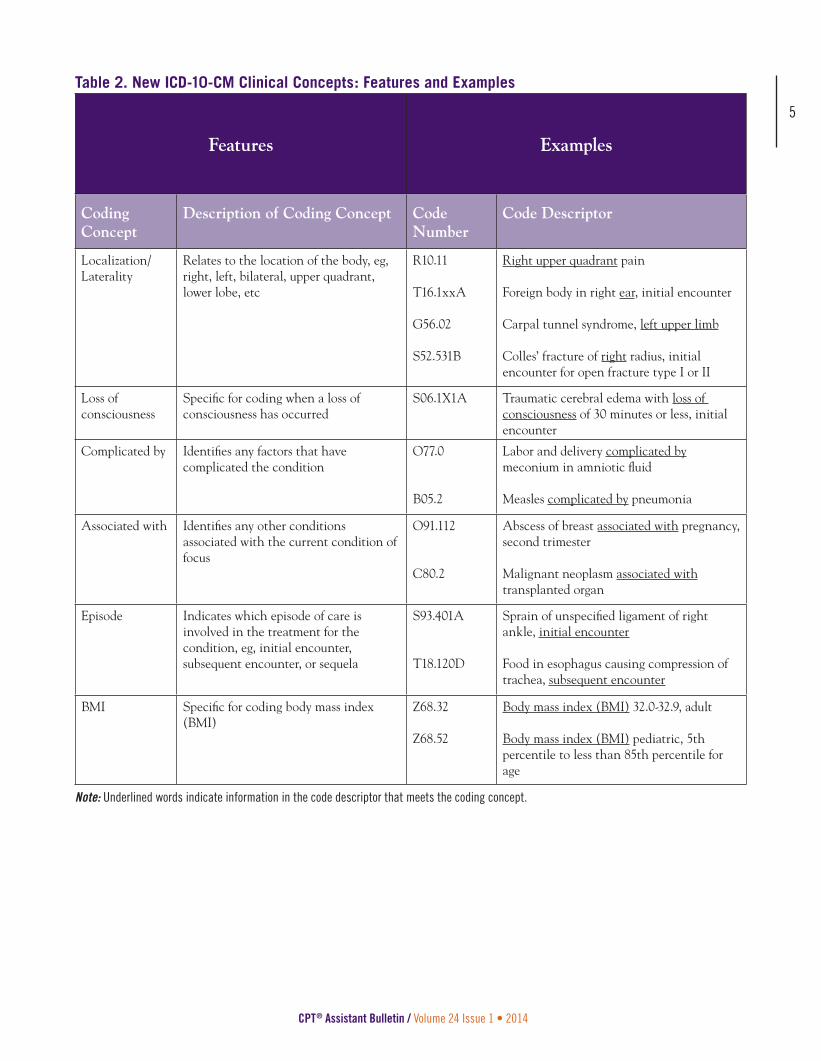
Table 2. New ICD-10-CM Clinical Concepts: Features and Examples
Features Examples
Coding Concept
Description of Coding Concept Code Number
Code Descriptor
Localization/Laterality
Relates to the location of the body, eg, right, left, bilateral, upper quadrant, lower lobe, etc
R10.11
T16.1xxA
G56.02
S52.531B
Right upper quadrant pain
Foreign body in right ear, initial encounter
Carpal tunnel syndrome, left upper limb
Colles’ fracture of right radius, initial encounter for open fracture type I or II
Loss of consciousness
Specific for coding when a loss of consciousness has occurred
S06.1X1A Traumatic cerebral edema with loss of consciousness of 30 minutes or less, initial encounter
Complicated by Identifies any factors that have complicated the condition
O77.0
B05.2
Labor and delivery complicated by meconium in amniotic fluid
Measles complicated by pneumonia
Associated with Identifies any other conditions associated with the current condition of focus
O91.112
C80.2
Abscess of breast associated with pregnancy, second trimester
Malignant neoplasm associated with transplanted organ
Episode Indicates which episode of care is involved in the treatment for the condition, eg, initial encounter, subsequent encounter, or sequela
S93.401A
T18.120D
Sprain of unspecified ligament of right ankle, initial encounter
Food in esophagus causing compression of trachea, subsequent encounter
BMI Specific for coding body mass index (BMI)
Z68.32
Z68.52
Body mass index (BMI) 32.0-32.9, adult
Body mass index (BMI) pediatric, 5th percentile to less than 85th percentile for age
Note: Underlined words indicate information in the code descriptor that meets the coding concept.
Bulletin_#1_060414_2ndP.indd 5 6/5/14 2:30 PM

6
CPT® Assistant Bulletin / Volume 24 Issue 1 • 2014
Benefits of Improved DocumentationSome of the benefits of improved clinical documentation include, but are not limited to, the following:
• More efficient diagnosis coding. Fewer follow-up queries about patient visits means the coding professional and the physician save time.
• Shorter response time to payer requests for additional information. If a payer requests for additional infor-mation about a patient’s condition to support a claim, providing detailed documentation would result in a shorter review period by the payer.
• Better support for audits. More complete documenta-tion makes post-payment reviews and audits easier.
Conducting a clinical documentation assessment is an important step toward preparing for the transition to the ICD-10-CM code set, and the goal of this assess-ment is to minimize the negative effect of ICD-10-CM implementation on the organization’s billing and revenue cycle. Knowing the clinical documentation requirements of the ICD-10-CM coding system and understanding the similarities and differences between the clinical concepts of ICD-9-CM and ICD-10-CM are important steps to highlight and improve the deficiencies of your organiza-tion’s clinical documentation, in order to avoid denied or unbillable claims and reduce lost or interrupted revenues.
Reference1. AAPC. ICD-10 Assessment: Clinical Documentation Evalu-
ation. www.aapc.com/icd-10/assessment-readiness.aspx. Accessed June 5, 2014.
ICD-10-CM 2015 Snapshot details the speci� city required to improve documentation and diagnosis coding.22 specialties available; visit amastore.com to see the complete list
4-page laminated cardPrice: $26.95AMA member price: $21.95
ICD-10 coding is a snap when using AMA Snapshot coding cards.
Price: $26.95AMA member price: $21.95
NEW PRODUCT
FOR THE 2015 CODE YEAR!
ICD-10-PCS 2015 Snapshotprovides greater understanding of
the organizational structure and complexities of procedural codes.
Laminated multi-card packagePrice: $36.95
AMA member price: $31.95
Available September 2014.Order online at amastore.com or call (800) 621-8335.
Bulletin_#1_060414_2ndP.indd 6 6/5/14 2:30 PM

CPT® Assistant Bulletin / Volume 24 Issue 1 • 2014
7
The transition to ICD-10-CM will impact all physician practices. With an increased number of codes, along with enhanced code speci� city, the transition will require a signi� cant amount of planning and training. The third editions of Principles of ICD-10-CM Coding and Principles of ICD-10-CM Coding Workbookwill give you what you need to smoothly and successfully make the move.
Designed for both the self-learner and classroom use, these educational ICD-10-CM coding resources will teach you how to make the correct decision when selecting diagnosis codes using the new coding system. Written for all skill levels from basic to advanced, the Principles of ICD-10-CM Coding book provides examples of “real-life” chart notes to enhance understanding, while the workbook provides hands-on exercises to help you learn and retain the knowledge needed to con� dently move from ICD-9-CM to ICD-10-CM.
MAKE THE TRANSITION EASIER WITH THESE ICD-10-CM CODING RESOURCES
For more information, visit amastore.com or call (800) 621-8335.
MAKE THE TRANSITION EASIER
Bulletin_#1_060414_2ndP.indd 7 6/5/14 2:30 PM

CPT® Assistant Bulletin / Volume 24 Issue 1 • 2014
AssistantOfficial source for CPT coding guidance
AMA Plaza330 North Wabash AvenueChicago, Illinois 60611-5885
AMERICAN MEDICAL ASSOCIATION
Editorial StaffDanielle Pavloski, RHIT, CCS-P, Managing EditorBiljana Dimovski, CDC, Editorial Assistant
Contributing Author(s)Mari R. Savickis, MPANancy Spector, RN, MSC
Production Staff Mary Ann Albanese, Nancy Baker, Lisa Chin-Johnson
Order Information1 year (12 issues) AMA Members* ... $149 Nonmembers ... $199
2 years (24 issues) AMA Members* ... $205 Nonmembers ... $299
Back Issues AMA Members* ... $14.95 Nonmembers ... $19.95
Discount prices online at www.amastore.com
Phone Orders: Call (800) 621-8335 Fax (312) 464-5000.
*To receive the member price, please provide the member’s number.
To change address information, please call AMA’s Customer Services Department at (800) 621-8335.
Notification of change of address must be made at least six weeks in advance.
AMA Web site: www.ama-assn.org
Mailing address: CPT Assistant AMA Plaza 330 North Wabash Avenue Chicago, IL 60611-5885
The CPT Assistant Bulletin information is designed to pro-vide accurate, up-to-date coding information. We continue to make every reasonable effort to ensure the accuracy of the material presented. However, this publication does not replace the CPT codebook; it serves only as a guide.
©2014. American Medical Association. All rights reserved. No part of this publication may be reproduced in any form without prior written permission of the publisher. CPT® is a registered trademark of the American Medical Association.
Bulletin_#1_060414_2ndP.indd 8 6/5/14 2:30 PM