association of wolbachia with heartworm disease in
TRANSCRIPT

1
ASSOCIATION OF WOLBACHIA WITH HEARTWORM DISEASE IN CATS AND DOGS
By
PATRICIA ANN DINGMAN
A THESIS PRESENTED TO THE GRADUATE SCHOOL OF THE UNIVERSITY OF FLORIDA IN PARTIAL FULFILLMENT
OF THE REQUIREMENTS FOR THE DEGREE OF MASTER OF SCIENCE
UNIVERSITY OF FLORIDA
2009

2
© 2009 Patricia Ann Dingman

3
To my cats, Sara and CC and my dog, Ellington Foxworthy
4
ACKNOWLEDGMENTS
I thank Nicholas Ronnquist for being patient and understanding. I thank my mentor
and inspiration, Dr. Julie Levy. She has given me so many opportunities to succeed and
has greatly contributed to my personal and professional growth. I would like to thank Dr.
Calvin Johnson, Dr. Ellis Greiner, and Dr. Charles Courtney for their patience and
support.
5
TABLE OF CONTENTS page
ACKNOWLEDGMENTS ...............................................................................................................4
LIST OF TABLES...........................................................................................................................7
LIST OF FIGURES .........................................................................................................................8
ABSTRACT ....................................................................................................................................9
CHAPTER
1 DIROFILARIA IMMITIS ........................................................................................................11
Identification...........................................................................................................................11 Life Cycle/Pathogenesis .........................................................................................................11 Epidemiology..........................................................................................................................13 Heartworm Disease.................................................................................................................13 Heartworm-Associated Lung Pathology.................................................................................14 Diagnosis of Heartworm Infection .........................................................................................15 Heartworm Treatment.............................................................................................................15
2 WOLBACHIA..........................................................................................................................17
Biology ...................................................................................................................................17 Endosymbiotic Relationship with D. immitis .........................................................................17
3 EXPERIMENTAL DESIGN..................................................................................................20
Materials and Methods ...........................................................................................................20 Animals............................................................................................................................20 Sample Collection ...........................................................................................................21 Serology...........................................................................................................................21 Parasitology .....................................................................................................................22 Pulmonary Histologic Morphometry...............................................................................22 Wolbachia DNA Detection..............................................................................................23 Wolbachia Immunohistochemistry..................................................................................24 Statistical Analyses..........................................................................................................24
4 RESULTS...............................................................................................................................32
Statistical Analyses.................................................................................................................32 Serology...........................................................................................................................32 Parasitology .....................................................................................................................32 Detection of Wolbachia ...................................................................................................33 Pulmonary Histologic Morphometry...............................................................................33
6
5 DISCUSSION.........................................................................................................................44
6 CONCLUSIONS ....................................................................................................................46
LIST OF REFERENCES...............................................................................................................47
BIOGRAPHICAL SKETCH .........................................................................................................51

7
LIST OF TABLES
Table page 3-1 Pulmonary arteriolar lesion scoring system.......................................................................25
3-2 Bronchiolar lesion scoring system. ....................................................................................26
3-3 Pulmonary interstitial and alveolar smooth muscle scoring system. .................................27
4-2 The prevalence of Ancylostoma spp. and ascarids in cats and dogs with pulmonary lesions ..............................................................................................................36
4-3 Frequency of pulmonary lesions in cats and dogs with and without Wolbachia...............37

8
LIST OF FIGURES
Figure page 3-1 Representative feline pulmonary tissues demonstrating lesion scores in
arterioles.............................................................................................................................28
3-2 Representative feline pulmonary tissues demonstrating lesion scores in bronchioles.........................................................................................................................29
3-3 Representative feline pulmonary tissues demonstrating lesion scores in alveolar smooth muscle......................................................................................................30
3-4 Representative feline pulmonary tissues demonstrating lesion scores in interstitium .........................................................................................................................31
4-1 Feline D. immitis antibody titer versus Wolbachia surface protein (WSP) antibody titer in all cats......................................................................................................38
4-2 Canine D. immitis antibody titer versus Wolbachia surface protein (WSP) antibody titer in all dogs ....................................................................................................39
4-3 Severity of pulmonary lesions in cats with or without detectable Wolbachia DNA and/or Wolbachia surface protein in lung tissues.....................................................40
4-4 Severity of pulmonary lesions in dogs with or without detectable Wolbachia DNA and/or Wolbachia surface protein in lung tissues.....................................................41
4-5 Severity of pulmonary lesions in cats with or without detectable circulating Wolbachia surface protein antibodies (WSP Ab) ..............................................................42
4-6 Severity of pulmonary lesions in dogs with or without detectable circulating Wolbachia surface protein antibodies (WSP Ab) ..............................................................43

9
Abstract of Thesis Presented to the Graduate School of the University of Florida in Partial Fulfillment of the
Requirements for the Degree of Master of Science
ASSOCIATION OF WOLBACHIA WITH HEARTWORM DISEASE IN CATS AND DOGS
By
Patricia Ann Dingman
May 2009 Chair: Julie Levy Major: Veterinary Medical Sciences
Although the presence of adult Dirofilaria immitis in the pulmonary arteries and its
associated arteritis and thromboembolic disease can explain some of the manifestations
of canine and feline heartworm disease, the cause of other findings remains unclear. For
example, cats with D. immitis antibodies but lacking adult parasites in the pulmonary
arteries frequent develop histological lesions of Heartworm-Associated Respiratory
Disease. All D. immitis parasites harbor Wolbachia and D. immitis-infected animals can
have circulating Wolbachia antibodies and pro-inflammatory Wolbachia antigens
deposited in tissues. Little is known about the role Wolbachia plays in the pulmonary
pathology of animals naturally infected with D. immitis. The purpose of this study was to
determine the contribution of Wolbachia to the pathogenesis of natural heartworm
disease in cats and dogs. We hypothesized that animals having sufficient Wolbachia
burden to be detected in pulmonary tissue by immunohistochemistry and/or by PCR
would have more severe pulmonary disease than those with bacteria below the limits of
detection. We further hypothesized that animals that were immunoreactive to pro-
inflammatory WSP would have more severe pulmonary lesions than those that were
seronegative for WSP antibodies. Blood and pulmonary tissue samples were collected
10
from cats and dogs representing three different D. immitis infection statuses: heartworm-
free, heartworm-exposed, heartworm-infected. There was a positive but weak correlation
between the magnitude of D. immitis antibody titers and WSP antibody titers in cats
(r=0.57, p<0.001) and in dogs (r=0.39, p<0.001). Pulmonary lesions were more common
in HW-infected animals than in HW-free animals. Pulmonary arteriolar occlusion was
more common in HW-infected cats (57%) (p=0.003) than in HW-infected dogs (17%).
Although pulmonary lesions were most common in HW-infected animals, there was no
clear additive effect when either Wolbachia DNA/WSP was detected in pulmonary tissue
or when circulating WSP antibodies were detected. Similarly, there were no significant
differences in the magnitude of pulmonary lesion scores within each HW-infection status
group regardless of whether Wolbachia DNA/WSP or WSP antibodies were detected.
The relationship between Wolbachia and pulmonary pathology in heartworm-infected
animals remains to be determined. The lack of clear evidence for a role of Wolbachia in
heartworm disease creates a dilemma for veterinarians treating cats and dogs in D.
immitis-endemic areas. Although the indiscriminant use of antibiotics should be avoided,
many clinicians prescribe doxycycline based on the favorable responses observed in
human filarial diseases and on promising results from the first published studies of
doxycycline use in D. immitis-infected dogs.
11
CHAPTER 1 DIROFILARIA IMMITIS
Identification
Dirofilaria immitis (heartworms) are filarial helminths that belong to the phylum,
Nematoda (roundworms) and superfamily Filaroidea. Other filarial nematodes, including
Wuchereria bancrofti and Brugia malayi, are known to cause human lymphatic filariasis
(elephantiasis), and Onchocerca volvulus is a causative agent for human river blindness disease.
Microfilariae (mff) are mobile vermiform embryos and are the microscopic immature stage
of D. immitis circulating in the blood of the vertebrate host. They are not sheathed and have a
straight tapered tail. Their size ranges from 286-340 µm in length and 6-7 µm in diameter. The
physical characteristics of D. immitis microfilariae distinguish them from other filarial species
such as Dipetalonema reconditum (Yabsley et al., 2004).
Dirofilaria immitis show sexual dimorphism; adult males range between 12 and 20 cm and
are much shorter in length than the female worms, which can grow as long as 30 cm in length.
Both sexes are thin, measuring less than 5 mm wide and white in color. They are cylindrical in
shape and a psuedocoelon is present. Males have coiled (corkscrew) tails, whereas the females’
tails are straight.
Life Cycle/Pathogenesis
There are three factors involving D. immitis transmission. First there needs to be an
infected vertebrate with circulating microfilariae, most commonly a domestic dog, which is a
definitive host for D. immitis. Heartworm-infected canids have circulating microfilariae and are
considered the natural reservoir for these parasites. Although cats are naturally more resistant to
D. immitis, feline infection is likely to occur anywhere the parasite is found in canids.
Microfilaremia is uncommon in cats and therefore for a cat to become infected with D. immitis
12
there needs to be an infected canid nearby (Genchi et al., 2008). Environmental conditions must
be appropriate for D. immitis larval development because environmental temperature affects
growth within the mosquito and microfilariae. Finally, vector competent mosquitoes such as the
Culex spp. must feed on both infected canids and susceptible hosts to effect transmission (Nelson
et al., 2005a; Ralston et al., 1998). Almost 70 species belonging to the family Culicidae are
considered potential vectors (Aedes spp., Anopheles spp., Culex spp., and Mansonia spp.).
To begin the cycle, a female mosquito feeds on a microfilaremic dog and the microfilariae
are ingested during the blood meal. The microfilariae pass through the hemocoel and into the
malpighian tubules of the mosquito. There they mature into first stage larvae (L1s) and molt to
second stage larvae (L2s) within 10 days. Ten to fourteen days later, they become third stage
larvae (L3s), which is the infective stage. The L3s migrate to the salivary glands and proboscis
and when the mosquito feeds, the L3s are deposited onto the skin and then enter the wound made
by the mosquito. The larvae begin to develop and molt into the 4th stage larva in 3-4 days.
Fourth-stage larvae migrate to the muscle fascia of the thorax and abdomen, molt, and then L5s
enter the circulatory system over a period of 3 to 4 months. They are carried to the pulmonary
arteries, heart, and lungs via blood circulation 4 to 7 months post infection. Once in the heart and
lungs they mature into adult worms approximately 6 months after infection if both male and
female worms are present. Adult female worms begin to produce microfilariae 6 to 9 months
(180 to 190 days) after the initial infection, which is the infectious period when D. immitis can be
acquired by mosquitoes and then transmitted to other cats or dogs. In cats, arrested development
of the worm is common because cats are not the natural host. Fewer worms reach maturity in
cats compared to dogs. Only about 20% of D. immitis larvae become adult worms in cats,
whereas up to 75% of D. immitis larvae in dogs become adults. Microfilariae were shown to

13
remain in blood circulation for up to two years in a dog that was experimentally inoculated with
microfilaremic blood (Underwood and Harwood, 1939). Adult worms in dogs can live up to 5 to
7 years in dogs (Newton, 1968) and 2 to 3 years in cats. Aberrant migration of the parasite has
been documented, resulting in disease associated with dysfunction of the target tissue (Nogami
and Sato, 1997).
Epidemiology
In areas endemic for D. immitis, prevalence in dogs that are not on heartworm preventive
can exceed 50%. Feline heartworm prevalence is often 5-20% of the positive dog population
(Atkins et al., 1998; Bowman et al., 2007; Carleton and Tolbert, 2004; Hermesmeyer et al., 2000;
Miller, 1998; Nogami and Sato, 1997; Patton and McCracken, 1991; Ryan and Newcomb, 1995).
Recently a nationwide survey estimated the feline heartworm prevalence rate, determined by
antigen testing, to be 0.6 times the canine prevalence (Lorentzen and Caola, 2008). Northern
Florida is a high endemic area and many dogs are not on preventive. The prevalence in
unprotected dogs is 25-50%. In Northern Florida, feline heartworms are found in 5% of the cat
population in an animal shelter (Levy et al., 2003; Snyder et al., 2000). Studies have
demonstrated conflicting results when examining the cats’ gender as a predisposing risk factor
for D. immitis. Some researchers have found male cats to be at a higher risk for heartworm
infection (Kramer and Genchi, 2002; Levy et al., 2003) whereas others reported gender not being
a determining factor for infection (Atkins et al., 2000; Genchi et al., 2008; Liu et al., 2005).
Heartworm Disease
Heartworm infection can have different effects on cats and dogs. Dogs have higher parasite
intensities, often reaching greater than 30 adult worms compared to cats that have only 1-3 adult
worms (Nogami and Sato, 1997; Ryan and Newcomb, 1995). Dogs are often microfilaremic
versus cats are not usually microfilaremic and it is much easier to diagnose infection in dogs than
14
in cats. Clinical signs in dogs include coughing, exercise intolerance, dyspnea, hepatomegaly,
syncope, and ascites. Clinical signs in cats include lethargy, coughing, anorexia, chylothorax,
and vomiting. Commonly cats have dyspnea or respiratory distress similar to feline bronchial
disease (asthma) and dogs experience right-heart failure (Nelson et al., 2005a, b). Often times,
there are no signs. When signs do occur, they are often the result of the arrival of L5s in the
pulmonary arteries which leads to acute pneumonitis. Signs may also occur when the deaths of
adult worms cause thromboembolism and anaphylaxis and may result in sudden death (Dillon,
1998).
Heartworm-Associated Pulmonary Pathology
Although the presence of adult D. immitis in the pulmonary arteries and its associated
arteritis and thromboembolic disease can explain some of the manifestations of canine and feline
heartworm disease (HWD), the cause of other findings remains unclear. This is particularly true
for cats, which frequently develop generalized severe bronchointerstitial disease and
extrapulmonary signs in response to very low worm intensitites (Atkins et al., 2000). In cats,
even a single worm can produce fatal disease.
Browne et al., (2005) examined 630 cats from an animal control shelter and assigned them
to three groups (HW-infected, HW-exposed, and HW-free) based on serological tests and
necropsy findings. Pulmonary lesions characterized by pulmonary arterial occlusive hypertrophy
were common in cats with adult worms and in cats that were free of adult worms but with D.
immitis antibodies, suggesting that even transient infection leave cats with long-lasting
pulmonary pathology. Occlusive hypertrophy is a characteristic of feline heartworm disease and
is defined as >95% occlusion of the arteriolar lumen by an increase in the thickness of the tunica
media. Almost 80% of the HW-infected cats had hypertrophy, followed with the HW-exposed

15
(50%) and HW-free (13%) and there was a significant association between the number of
occluded vessels and HW status.
Diagnosis of Heartworm Infection
There are many blood tests for diagnosis of heartworm infection. A blood concentration
test such as the Knotts method or membrane filtration can detect circulating microfilariae in the
blood stream. Dirofilaria immitis antigen tests detect proteins shed from female adult worms.
False-negatives occur if the dog or cat has an all male, a low worm burden, or juvenile worms.
Dirofilaria immitis antibody tests indicate exposure to heartworms, but not necessarily current
infection. Enzyme-linked immunosorbent assays (ELISA) or non-ELISA lateral flow tests can be
used to detect D. immitis antigen or antibodies. Additional support for a diagnosis of D. immitis
infection includes thoracic radiography and echocardiography, as well as combining or repeating
antigen and antibody tests (Berdoulay et al., 2004; Nelson, 2008; Snyder et al., 2000). A
necropsy may provide a definitive answer; however D. immitis have been known to migrate to
aberrant locations (Nogami and Sato, 1997; Oh et al., 2008) and necropsy may not detect
immature infections.
Heartworm Treatment
Although canine heartworm infection is very common, it is also 100% preventable.
Preventives must be administered monthly starting approximately one month after the beginning
of the transmission season and ending approximately one month after the end of the season
according to the American Heartworm Society (AHS) (Nelson et al., 2005a, b). Prevention is
most important during the transmission period but to insure client compliance, and to account for
transmission variability in microclimates, treatment year-round is recommended.
Currently there are no FDA-approved drugs available for adulticide treatment in cats and
because infected cats usually lack circulating microfilaria, they do not need microfilaricide

16
treatment. Adulticide therapy in cats has been associated with a mortality rate of 20-30%. AHS
recommends prednisone and supportive therapy to ameliorate clinical signs of disease in cats.
Surgical removal of the worms can be attempted in cats with uncontrolled signs. Aspirin is no
longer recommended as a treatment for heartworm disease in cats. FDA-approved heartworm
preventives for cats include ivermectin, milbemycin oxime, and selamectin. The preventives
should be administered 30 days after transmission season begins and 30 days after it ends on a
monthly basis (Nelson et al., 2005a).
There are more treatment options for dogs than for cats. Dogs should begin preventives at
8 weeks of age. Adult dogs starting preventives for the first time should be tested for D. immitis.
Ivermectin, milbemycin oxime, moxidectin, and selamectin are macrocyclic lactones most
effective against mff, L3s, and L4s. Daily diethylcarbamazine (DEC) can also be used as a
preventive but is rarely used due to the availability of monthly preventives. Testing for
microfilariae is required before treating with DEC to avoid adverse reaction in infected dogs. Re-
testing is recommended for all the preventives 7 months after the end of the transmission season
to assure prevention of infection. The only FDA-licensed adulticide treatment for dogs is
melarsomine dihydrochloride. Using low-dose ivermectin as an adulticide can take several years
to cure infection and is not generally recommended. Microfilaricide treatment should be
performed after adulticide therapy. Re-testing for microfilariae and D. immitis antigens are
recommended after adulticide therapy (Nelson et al., 2005b).

17
CHAPTER 2 WOLBACHIA
Biology
The genus Wolbachia belongs to the order, Rickettsiales. Wolbachia is phylogenetically
related to Ehrlichia spp. and Anaplasma spp. The only species identified in the genus is
Wolbachia pipientis. These gram-negative bacteria are found in 100% of the D. immitis
population; all individuals are infected. The bacteria are present in all developmental stages and
are located in the hypodermal cells of the lateral chords (Kozek, 2005; Kramer et al., 2003).
Wolbachia are transmitted maternally (female to offspring). After the first week when L3s
entered the host, bacteria growth increases until L4 development. The amount of bacterial cells
remains constant in male worms, but as the females begin to mature, the bacteria increase in
number and infect the ovaries, oocytes, and embryonic stages inside the uteri. They have not
been reported from the male reproductive system.
Researchers have discovered Wolbachia surface proteins (WSP) circulating in heartworm-
infected dogs, localized in the lungs and kidneys where microfilariae are common (Kozek, 2005;
Kramer et al., 2003). Macrophages containing Wolbachia have been identified in the lung, liver,
and kidneys of dogs with natural D. immitis infection (Kramer et al., 2005b). Dirofilaria immitis-
infected animals also have circulating WSP antibodies (Bazzocchi et al., 2000a; Kozek, 2005;
Kramer et al., 2008; Kramer et al., 2005b; Morchon et al., 2004).
Endosymbiotic Relationship with D. immitis
In recent years, it has been recognized that a large array of helminths and arthropods are
colonized by Wolbachia (Bandi et al., 1998; McCall, 2005). Human and animal filarial
nematodes, including the agents of human river blindness (Onchocerca volvulus), lymphatic
filariasis (Brugia malayi), and feline and canine heartworm disease (Dirofilaria immitis), harbor

18
Wolbachia in a mutually dependent manner (Bazzocchi et al., 2000b Kozek, 2005; Kramer et al.,
2003; McCall, 2005; Taylor, 2003). Wolbachia aid in the parasite’s survival and reproduction
and can also influence the sex of the filarial parasites (Bandi et al., 1998; Bandi et al.,
1999).Filariae rendered free of Wolbachia by treatment with tetracycline antibiotics show
inhibition of maturation, survival, and reproduction (Bandi et al., 1999; Casiraghi et al., 2002;
Genchi et al., 1998; Makepeace et al., 2006; Pfarr and Hoerauf, 2006).
Wolbachia are released in large numbers during parasite molts, during production of
microfilariae, and at death of the parasite (Bandi et al., 1999; Taylor, 2003; Taylor et al., 2005).
Wolbachia-associated-molecules (WAMs) have recently been shown to be associated with
inflammation in the parasitized mammalian hosts (Bazzocchi et al., 2000a; Bazzocchi et al.,
2003; Kozek, 2005; Kramer et al., 2005a; Kramer et al., 2005b; McCall, 2005; Morchon et al.,
2004; Taylor, 2003). These inflammatory responses appear to be most profound when the
parasite dies naturally or as a result of anti-filarial drug treatment. In contrast, the death of
parasites rendered free of Wolbachia stimulates less intense inflammation in the host. This
observation has led to treatment strategies for river blindness and lymphatic filariasis that include
pretreatment with tetracycline antibiotics to reduce the burden of Wolbachia, followed by
ivermectin to eliminate the parasites (Makepeace et al., 2006; Taylor, 2003).
Wolbachia surface protein (WSP) stimulates canine neutrophil chemotaxis and IL-8
production (Bazzocchi et al., 2003). Stimulation of canine vascular endothelial cells with WSP
resulted in production of cyclooxygenase-2, 5-lipooxygenase, leukotriene B4, intracellular
adhesion molecules, E-cadherin, and vascular endothelial growth factor (Simon et al., 2008). In
cats, experimental D. immitis infection resulted in production of antibodies against both D.
immitis and Wolbachia within two months of exposure to infective larvae (Morchon et al., 2004).
19
Treatment with ivermectin 30 days later to abort D. immitis infection was associated with
disappearance of D. immitis antibodies, but persistence of Wolbachia antibodies. Dogs
experimentally infected with D. immitis and treated with doxycycline in combination with
ivermectin and melarsomine had less pulmonary pathology than dogs treated with melarsomine
alone (Kramer et al., 2008). Taken together, these studies suggest a role for Wolbachia in the
pathogenesis of heartworm disease.
If recently reported experiences with antibiotic treatment of filarial diseases prove to be
predictive of responses in naturally infected animals, then treatment with doxycycline prior to
adulticide therapy in dogs may sterilize D. immitis of Wolbachia, leading to fewer inflammatory
side-effects when the adult worms die. Doxycycline therapy may be especially helpful for cats,
which suffer substantial and life-threatening effects of heartworm disease, but for which
adulticide therapy is associated with high mortality rates and is generally contraindicated.
Elimination of inflammatory Wolbachia organisms may allow cats to coexist more comfortably
with their parasites, even if an actual cure is not feasible. However, it is not currently known
what role Wolbachia plays in the pathogenesis of natural heartworm disease.
The purpose of this study was to determine the contribution of Wolbachia to the
pathogenesis of natural heartworm disease in cats and dogs. Since all D. immitis parasites harbor
Wolbachia, it is difficult to differentiate the effects of the parasite from those of its endosymbiont
bacteria. We hypothesized that animals having sufficient Wolbachia burden to be detected in
pulmonary tissue by immunohistochemistry and/or by PCR would have more severe pulmonary
disease than those with bacteria below the limits of detection. We further hypothesized that
animals that were immunoreactive to pro-inflammatory WSP would have more severe
pulmonary lesions than those that were seronegative for WSP antibodies.

20
CHAPTER 3 EXPERIMENTAL DESIGN
Materials and Methods
Animals
Over a two year period (2005-2007), dog (n=90) and cat (n=90) cadavers were collected
from Alachua County Animal Services (ACAS) in Gainesville, Florida following euthanasia for
reasons unrelated to the study. Cadavers were transported to the University of Florida for
necropsy.
For this study, samples were collected from cats and dogs representing three different D.
immitis infection statuses. The heartworm-free (HW-free) groups were composed of 30 cats and
30 dogs that were free of any evidence of current or previous D. immitis infection (seronegative
for D. immitis antigen and antibodies and negative for parasites at necropsy). The heartworm-
exposed (HW-exposed) groups were composed of 30 cats and 30 dogs with evidence of either
larval-stage infection or past infection (seropositive for D. immitis antibodies), but no evidence
of current adult parasite infection (seronegative for D. immitis antigen and negative for parasites
at necropsy). The heartworm-infected (HW-infected) groups were composed of 30 cats and 30
dogs with adult parasites in the heart or pulmonary arteries at necropsy (regardless of serological
status). The severity of pulmonary lesions in each group was correlated with the detection of
Wolbachia proteins or nucleic acid sequences and with the presence of Wolbachia antibodies.
This study was approved by the University of Florida Institutional Animal Care and Use
Committee (IACUC approval number E12).
21
Sample Collection
Blood (4 mL) was collected by transthoracic cardiocentesis into EDTA and serum
separator tubes from each animal within 2 hours after death. Aliquots of EDTA whole blood and
serum were stored at -20°C pending analysis.
The heart and lungs were removed and dissected for the detection of D. immitis. Sections
of the right caudal lung lobe were preserved in 10% formalin for histomorphometry and
immunohistochemistry. Additional sections of fresh lung tissue were stored at -70°C for PCR
analysis. Any recovered D. immitis were preserved in 70% ethanol at room temperature for
immunohistochemistry and PCR.
Feces were collected from the large intestine of each animal and stored at 4°C pending
flotation analysis.
Serology
Cat and dog EDTA whole blood samples were tested by ELISA for D. immitis antigen
(Feline SNAP® Heartworm Antigen Test Kit, Canine SNAP® Heartworm Antigen Test Kit;
IDEXX Laboratories Inc., Westbrook, ME, USA; IDEXX). Feline serum samples were also
screened for D. immitis antibodies with a lateral flow immunoassay (HESKA Solo StepTM FH,
Heska Corporation, CO, USA). These serological results were used to aid in the selection of
cadavers for dissection. Dirofilaria immitis antibody titers and Wolbachia surface protein (WSP)
antibody titers were determined for both cats and dogs as described by Morchon et al., (2004).
Cat serum samples were also tested for FIV antibodies and FeLV antigen by ELISA (PetChek
ELISA, IDEXX Laboratories Inc.)
22
Parasitology
Dirofilaria immitis collected at necropsy were counted and examined with a dissecting
microscope to determine sex and age (adult, juvenile, or unknown) of recovered worms. Male
adult worms were identified by their cork-like tails.
Several common parasites of cats and dogs migrate through the lungs as part of their life
cycle and can induce damage that is indistinguishable from that induced by HW infection. To
control for this, feces were examined for ova and larvae. Feces (approximately 1 g) were mixed
with sodium nitrate solution (1.200 specific gravity; Fecasol Solution, Evsco Pharmaceuticals,
Buena, NJ, USA) in a standardized flotation device (Fecalyzer, Evsco Pharmaceuticals),
incubated with a cover slip for 15 minutes, and then evaluated qualitatively by light microscopy
at 100X for the presence of any ova or larvae.
Pulmonary Histologic Morphometry
Formalin-fixed and paraffin-embedded 5 µm sections of tissue collected from the right
caudal lung lobe were stained with hematoxylin and eosin. Digital images were acquired at 100-
400X magnification (Q-Capture software, Q-Imaging Corp, Burnaby, BC, Canada). For each
animal, 10 arterioles, 10 bronchioles, five areas of interstitium, and five areas of alveoli were
assessed. Arteriolar and bronchiolar wall areas were quantified in two-dimensional cross-
sections of the structures as a measure of wall thickness using computer software (Image J,
National Institutes of Health, Bethesda, Maryland, USA). Wall area was calculated by digitally
tracing the entire external and luminal surfaces of the structures and then subtracting the luminal
area from the total area as described in Browne et al. (2005). Pulmonary arteriolar occlusive
hypertrophy was defined as an arteriolar wall that exceeded 95% of the total area, resulting in a
reduced luminal area < 5% of the vessel area.
23
In addition to morphometric evaluation of arteriolar and bronchiolar thickness, pulmonary
tissues were scored for severity of histologic lesions on a 0 (normal) to 3 (severely abnormal)
scale. Lesions of the arterioles and bronchioles were scored according to the systems described
in Tables 3-1 and 3-2 and are shown in Figures 3-1 and 3-2. Lesions of the interstitium were
scored based on the frequency of inflammatory cells and the presence of edema within alveolar
septa, whereas lesions of the alveoli were scored according to the relative quantity of smooth
muscle nodules within the tips of alveolar septa as described in Table 3-3 and shown in Figures
3-3 and 3-4. When various components of a structure had different severity grades, the score was
based on the predominant lesion. Mean pulmonary lesion scores for each animal were calculated.
For determination of lesion prevalences, mean scores ≤ 1 were considered to be free of lesions
and mean scores > 1 were considered to have lesions.
Wolbachia DNA Detection
DNA was extracted from lung tissue (40 mg) and parasite tissue (up to 52 µg) using a
commercial kit (DNeasy Tissue Kit, Qiagen Inc., Qiagen Inc.). DNA quality was confirmed by
spectrophotometry and amplification of the ubiquitous housekeeping gene GAPDH. A
conventional PCR assay amplifying a region of the 16S-23S intergenic spacer gene (5’CTG
GGG ACT ACG GTC GCA AGA C 3’ forward; 5’CTC CAG TTT ATC ACT GGA AGT T 3’
reverse) common to Ehrlichia spp., Anaplasma spp., Neorickettsia risticii, and Wolbachia was
performed as described by Lappin et al. (2004). For amplicons of the appropriate size, genetic
sequencing was performed (Macromolecular Resources, Colorado State University, Fort Collins,
CO), and the resultant sequences analyzed by comparison to sequences in GenBank. BLAST
software (National Institutes of Health, NCBI website) was used to confirm the species source of
amplification products. Samples were considered positive for Wolbachia only if PCR assay
results were confirmed by genetic sequencing.
24
Wolbachia Immunohistochemistry
Lung tissues and D. immitis parasites were assessed for Wolbachia antigen (WSP) by
immunohistochemistry as described by Kramer et al. (2003). Formalin-fixed paraffin-embedded
5 µm lung sections and heartworm sections were affixed to polylysinated slides. The sections
were incubated in 3% H2O2 for 10 minutes at room temperature. The slides were then treated
with bovine serum albumin and fetal calf serum with phosphate buffered saline (PBS) for 15
minutes. Wolbachia antigens were detected by incubation with rabbit anti-WSP polyclonal
antibody diluted at 1:200 in PBS for 20 minutes followed by anti-rabbit IgG-streptavidin
complex (LSAB2 kit, DAKO, Italy). Color was developed with biotin-horseradish peroxidase,
and sections were counterstained with hematoxylin (LSAB2 kit, DAKO, Italy). Slides were
reviewed microscopically at 100X and were scored as positive or negative for specific staining.
Statistical Analyses
Animals were grouped by heartworm-infection status (HW-free, HW-exposed, HW-infected)
and by Wolbachia status (DNA-, protein-, or antibody-positive or negative) for statistical
analyses. Correlation between the magnitude of D. immitis antibody titers and WSP antibody
titers was measured with the Pearson’s r test (SigmaStat 3.5 statistical analysis software, SPSS
Inc., Chicago, IL, USA). Chi-square analysis was used to compare prevalences of parasitism and
pulmonary lesions when n ≥ 5 and the Fisher exact test was used to compare prevalences when
any group n < 5 (Epi InfoTM 3.5.1, Centers for Disease Control, Atlanta, Georgia). The mean
values of the pulmonary lesion scores were compared using the Wilcoxon rank rum test.
Differences were considered significant when p<0.05.
25
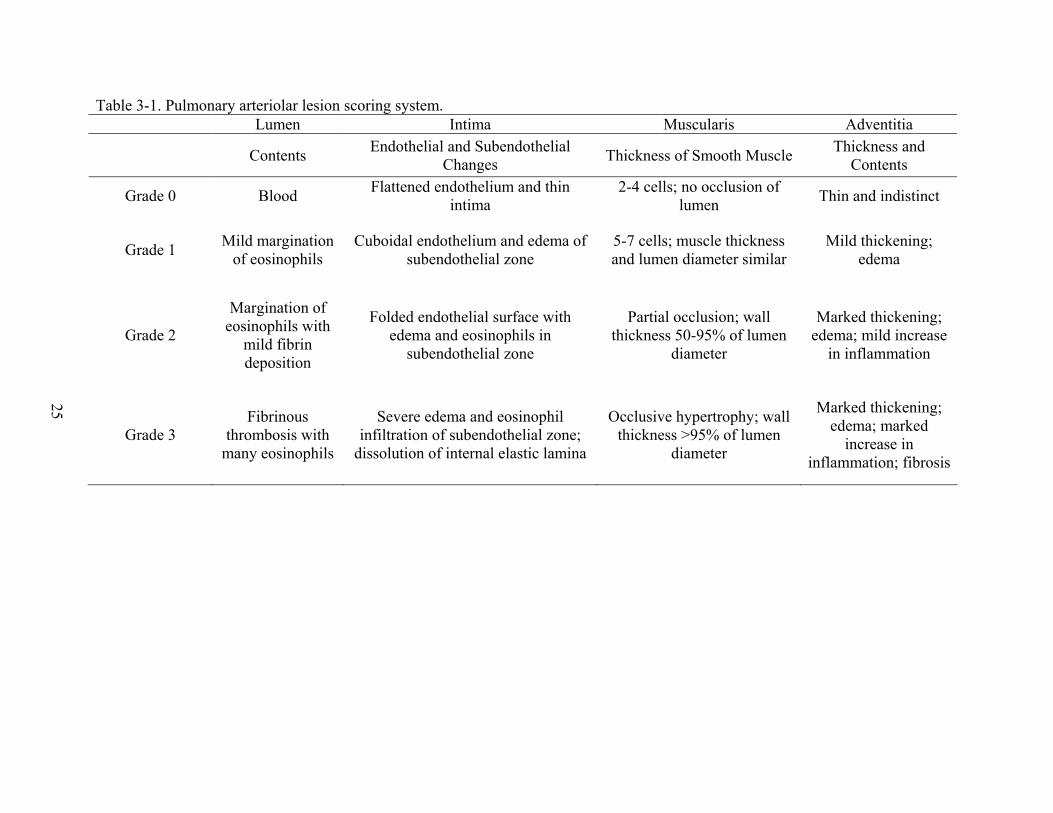
Table 3-1. Pulmonary arteriolar lesion scoring system. Lumen Intima Muscularis Adventitia
Contents Endothelial and Subendothelial
Changes Thickness of Smooth Muscle
Thickness and Contents
Grade 0 Blood Flattened endothelium and thin
intima 2-4 cells; no occlusion of
lumen Thin and indistinct
Grade 1 Mild margination
of eosinophils Cuboidal endothelium and edema of
subendothelial zone 5-7 cells; muscle thickness and lumen diameter similar
Mild thickening; edema
Grade 2
Margination of eosinophils with
mild fibrin deposition
Folded endothelial surface with edema and eosinophils in
subendothelial zone
Partial occlusion; wall thickness 50-95% of lumen
diameter
Marked thickening; edema; mild increase
in inflammation
Grade 3 Fibrinous
thrombosis with many eosinophils
Severe edema and eosinophil infiltration of subendothelial zone;
dissolution of internal elastic lamina
Occlusive hypertrophy; wall thickness >95% of lumen
diameter
Marked thickening; edema; marked
increase in inflammation; fibrosis

26
Table 3-2. Bronchiolar lesion scoring system.
Lumen Mucosa Submucosa Muscularis
Contents Epithelial Changes
Edema Inflammation Serous Glands Fibrosis Thickness of
Smooth Muscle
Grade 0 None Cuboidal Minimal Minimal Rare None 1-2 cells
Grade 1 Mild
seromucoid secretion
Low columnar with mild
crowding and folding
Mild Mild Mild increase Mild 3-4 cells
Grade 2
Moderate seromucoid
secretion with
inflammation
Tall columnar
with moderate
crowding and folding
Moderate Moderate Moderate increase (nesting)
Moderate 5-6 cells
Grade 3
Severe seromucoid
secretion with
inflammation
Tall columnar
with severe crowding and
folding
Severe Severe Severe increase
(circumferential) Severe >6 cells
27
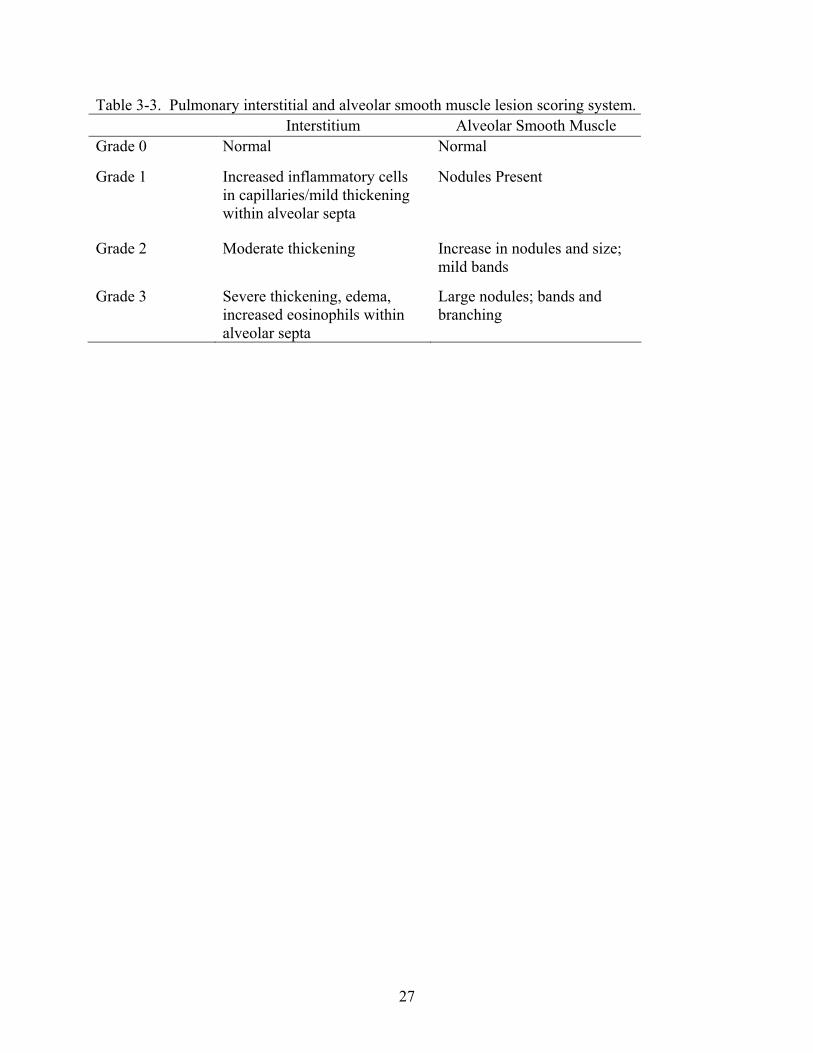
Table 3-3. Pulmonary interstitial and alveolar smooth muscle lesion scoring system. Interstitium Alveolar Smooth Muscle Grade 0 Normal Normal
Grade 1 Increased inflammatory cells in capillaries/mild thickening within alveolar septa
Nodules Present
Grade 2 Moderate thickening Increase in nodules and size; mild bands
Grade 3 Severe thickening, edema, increased eosinophils within alveolar septa
Large nodules; bands and branching

28
Figure 3-1. Representative feline pulmonary tissues demonstrating lesion scores in arterioles. Scores were assigned based on descriptions in Table 3-1. Grade 0 represented normal tissue (arrow pointing to red blood cells in open lumen area) and Grade 3 was considered the most severe lesion. There is a slight increase in smooth muscle in the Grade 1 arteriole (arrow). Edema (arrow) and the hypertrophied smooth muscle are present in the Grade 2 arteriole. The Grade 3 arteriole is displaying occlusive hypertrophy with no visible lumen (wall area >95% of total area) (arrow) (H&E stain, bar=100 µm).
Grade 0 Grade 1
Grade 2 Grade 3
29
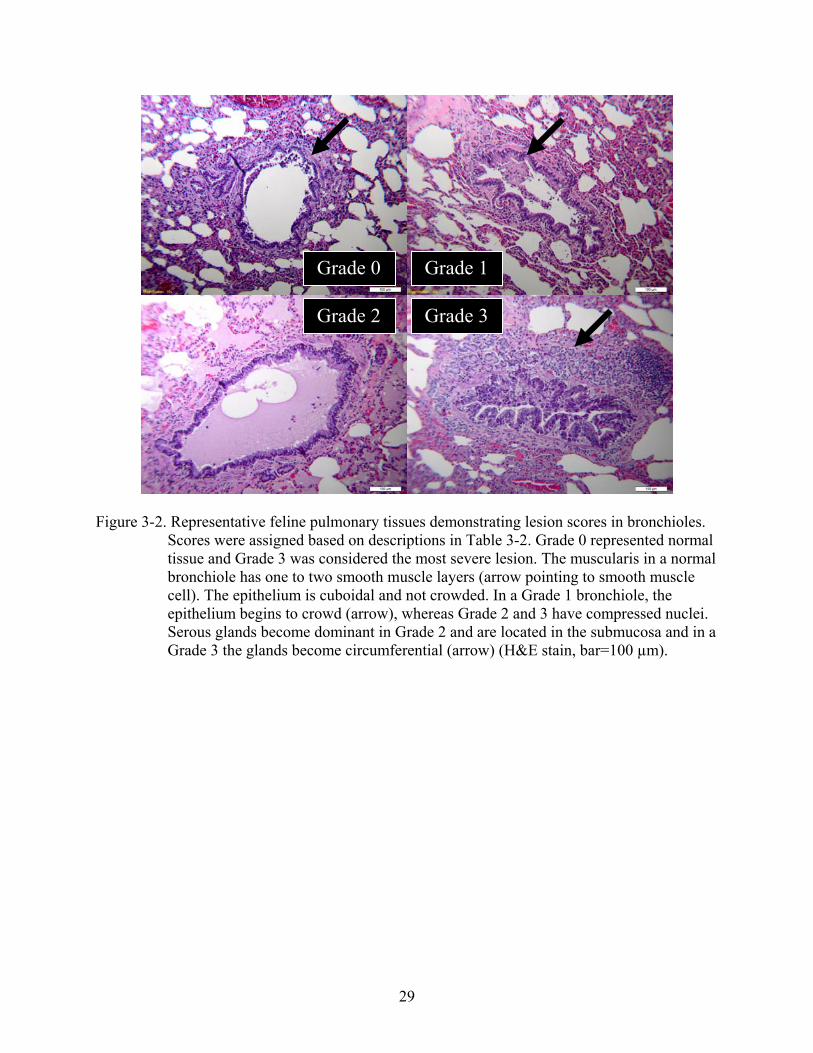
Figure 3-2. Representative feline pulmonary tissues demonstrating lesion scores in bronchioles.
Scores were assigned based on descriptions in Table 3-2. Grade 0 represented normal tissue and Grade 3 was considered the most severe lesion. The muscularis in a normal bronchiole has one to two smooth muscle layers (arrow pointing to smooth muscle cell). The epithelium is cuboidal and not crowded. In a Grade 1 bronchiole, the epithelium begins to crowd (arrow), whereas Grade 2 and 3 have compressed nuclei. Serous glands become dominant in Grade 2 and are located in the submucosa and in a Grade 3 the glands become circumferential (arrow) (H&E stain, bar=100 µm).
Grade 0 Grade 1
Grade 2 Grade 3

30
Figure 3-3. Representative feline pulmonary tissues demonstrating lesion scores in alveolar
smooth muscle. Scores were assigned based on descriptions in Table 3-3. Grade 0 represented normal tissue and Grade 3 was considered the most severe lesion. Smooth muscle nodule (arrow A) size varies with grades. Banding develops in Grade 2, and nodules and bands become undistinguishable in Grade 3 (arrow B) (H&E stain, bar=100 µm).
Grade 0 Grade 1
Grade 2 Grade 3
A
B

31
Figure 3-4. Representative feline pulmonary tissues demonstrating lesion scores in interstitium.
Scores were assigned based on descriptions in Table 3-3. Grade 0 represented normal tissue and Grade 3 was considered the most severe lesion. The arrow is pointing to the thickening within alveolar septa and inflammatory cells within the capillaries. (H&E stain, bar=100 µm).
Grade 0 Grade 1
Grade 2 Grade 3
32
CHAPTER 4 RESULTS
Statistical Analyses
Serology
This study was not designed to report the sensitivity or specificity of the antibody or
antigen tests because serology results were used to select specimens for necropsy.
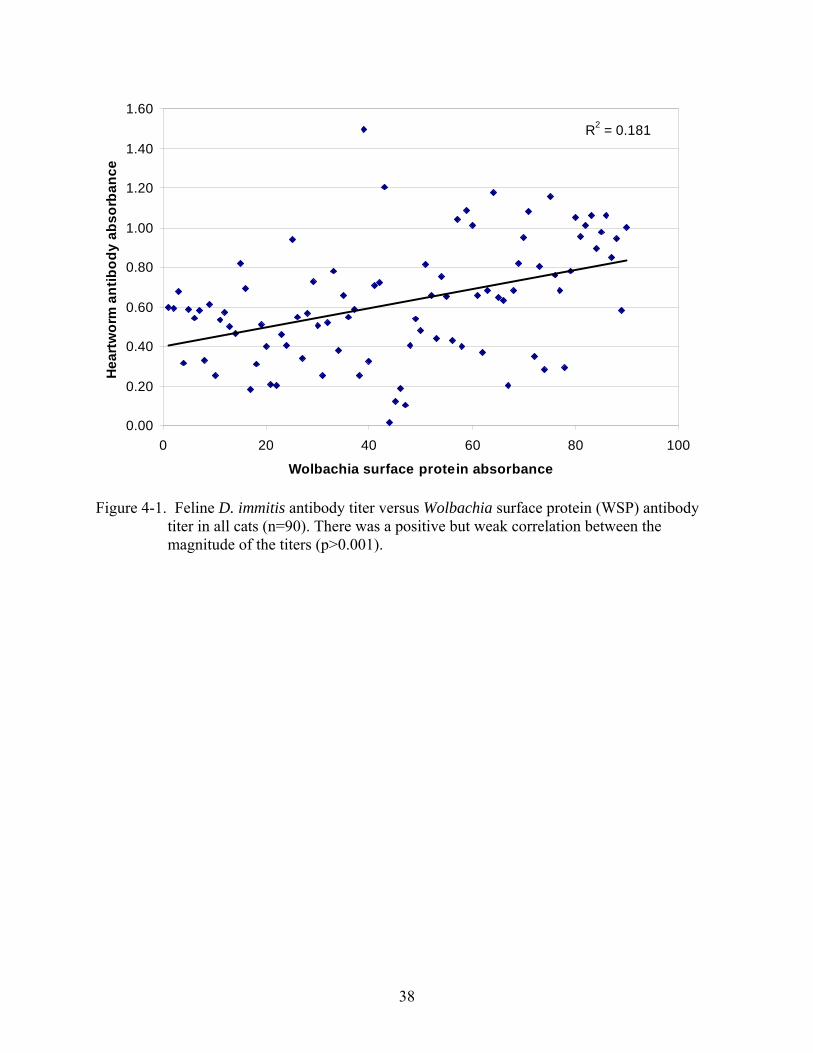
There was a positive but weak correlation between the magnitude of D. immitis antibody
titers and WSP titers in cats (r=0.57, p<0.001) and in dogs (r=0.39, p<0.001) (Figures 4-1, 4-2).
Antibodies against WSP were detected in a majority of HW-infected cats and dogs and in
variable proportions of animals in other HW-status groups (Table 4-1). Of the 90 cats in the
study, 10 had FIV antibodies (five from the HW-infected group and five from the HW-exposed
group) and one was infected with FeLV (from the HW-exposed group).
Parasitology
Low D. immitis intensities were common in cats in the HW-infected group
(mean=1.7±0.2 worms, range=1-6). Of the 51 D. immitis collected from the 30 HW-infected
cats, most were female (35/51, 69%). Only five cats had both male and female worms. Higher
worm intensities were common in dogs in the HW-infected group (mean=36.3±5.9 worms,
range=3-133). Of the 1,090 D. immitis collected from the 30 HW-infected dogs, most were
female (606/1090, 56%). All dogs had both female and male worms.
Ancylostoma spp. were common in both cats (52%) and dogs (61%). Other
gastrointestinal parasites identified included whipworms (0% of cats, 27% of dogs) and ascarids
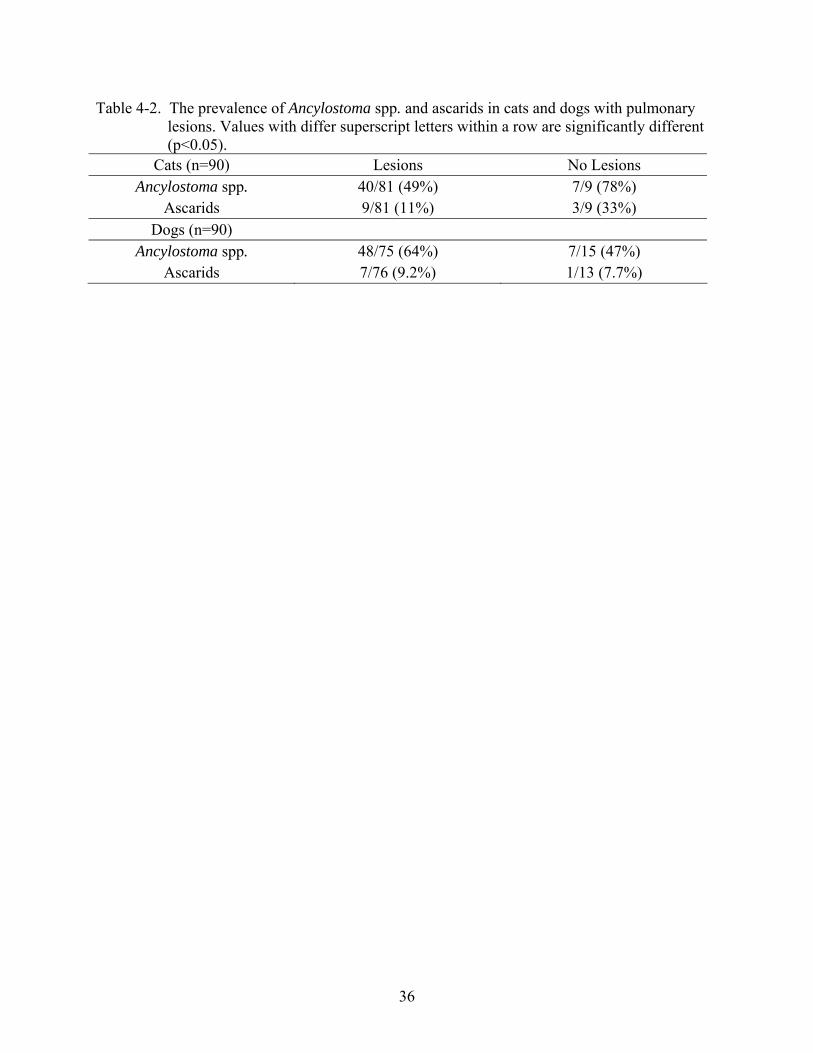
(13% of cats, 9% of dogs). There were no significant associations between the overall presence
of pulmonary lesions in cats or dogs and the presence of Ancylostoma spp. or ascarids, two
parasites with a pulmonary migratory phase in their life-cycle (p>0.09) (Table 4-2). When

33
animals were grouped according to subtype of lesion (arteriolar, bronchiolar, alveolar smooth
muscle, or interstitial), cats with alveolar lesions were less likely to have ascarids than those
without lesions (p=0.02) and dogs with interstitial lesions were more likely to have Ancylostoma
spp. than dogs without lesions (p=0.02).
Detection of Wolbachia
Wolbachia DNA was amplified from adult D. immitis collected from 26 of 30 HW-
infected cats, and from D. immitis collected from all of the HW-infected dogs. Three out of the
four Wolbachia-negative D. immitis samples from the HW-infected cats were GAPDH negative,
indicating inadequate DNA quality. WSP was detected by immunohistochemistry in D. immitis
specimens from all cats and dogs. In general, Wolbachia DNA or WSP was identified most
commonly in the lungs of HW-infected animals, but was also present in variable proportions of
lung samples in the other HW-infection status groups (Table 4-1).
Pulmonary Histologic Morphometry
As expected, pulmonary lesions were more common in HW-infected animals than in HW-free
animals (Table 4-1). Pulmonary arteriolar occlusion was more common in HW-infected cats
(57%) (p=0.003) than in HW-infected dogs (17%). In addition, HW-infected cats with occlusion
had more affected arterioles (43±6%) than did HW-infected dogs with occlusion (12± 2%)
(p=0.007). In cats, occlusive hypertrophy was identified most commonly in the HW-infected
group, but was also present in the HW-free and HW-exposed groups. In contrast, arteriolar
occlusion in dogs was present only in the HW-infected group. Although there were differences in
the proportions of cats affected by arteriolar occlusion, there were no significant differences in
the severity of occlusion among the groups. The percentage of occluded vessels in the HW-
exposed group (44±11%) was similar to that of the HW-infected group, and the HW-free group
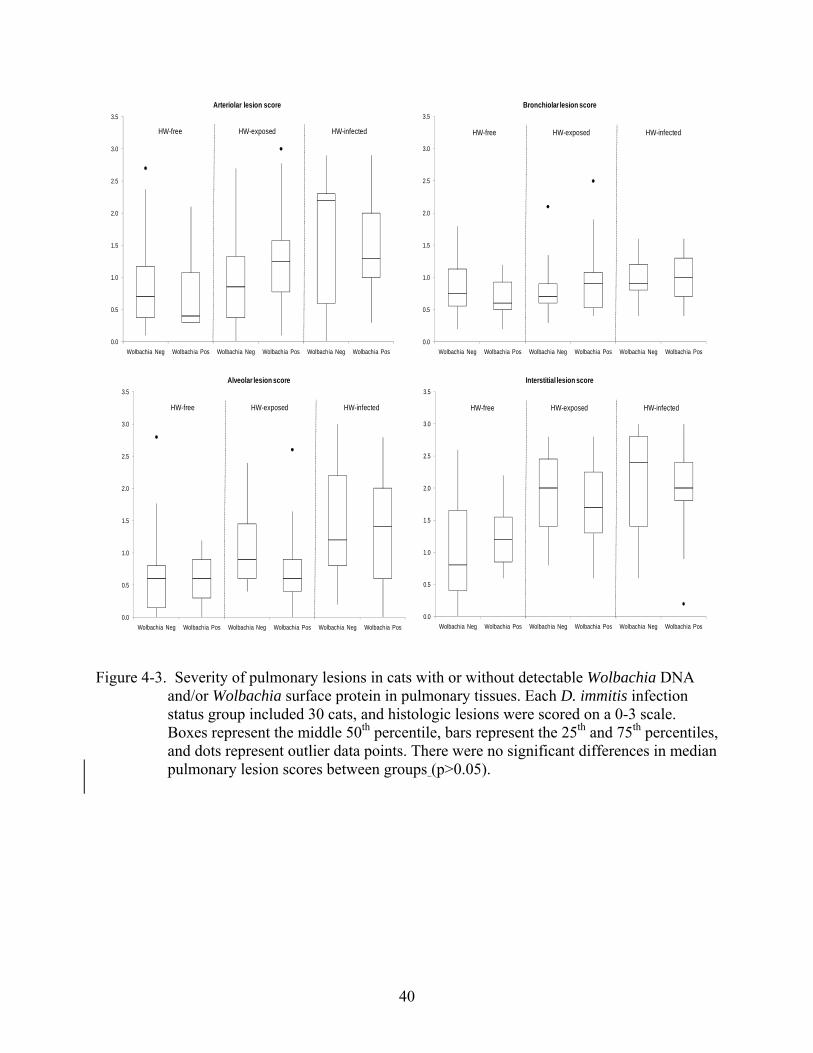
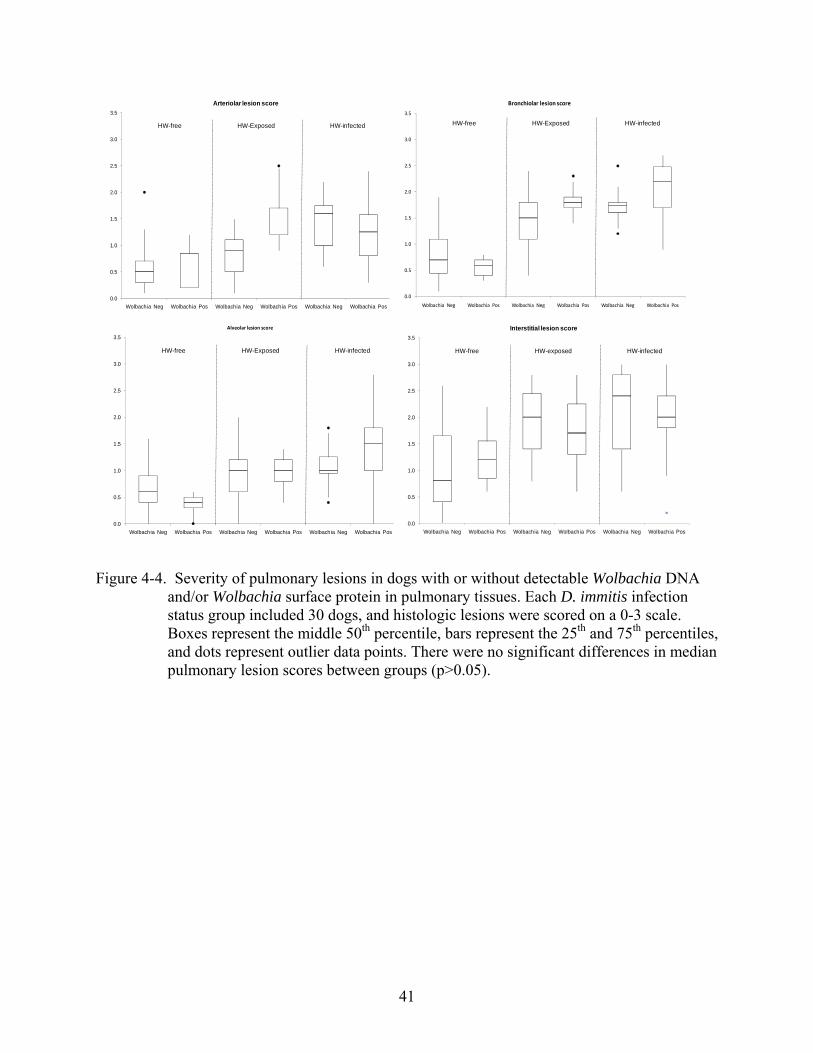
(28±7%) (p=0.31). Although pulmonary lesions were most common in HW-infected animals,
34
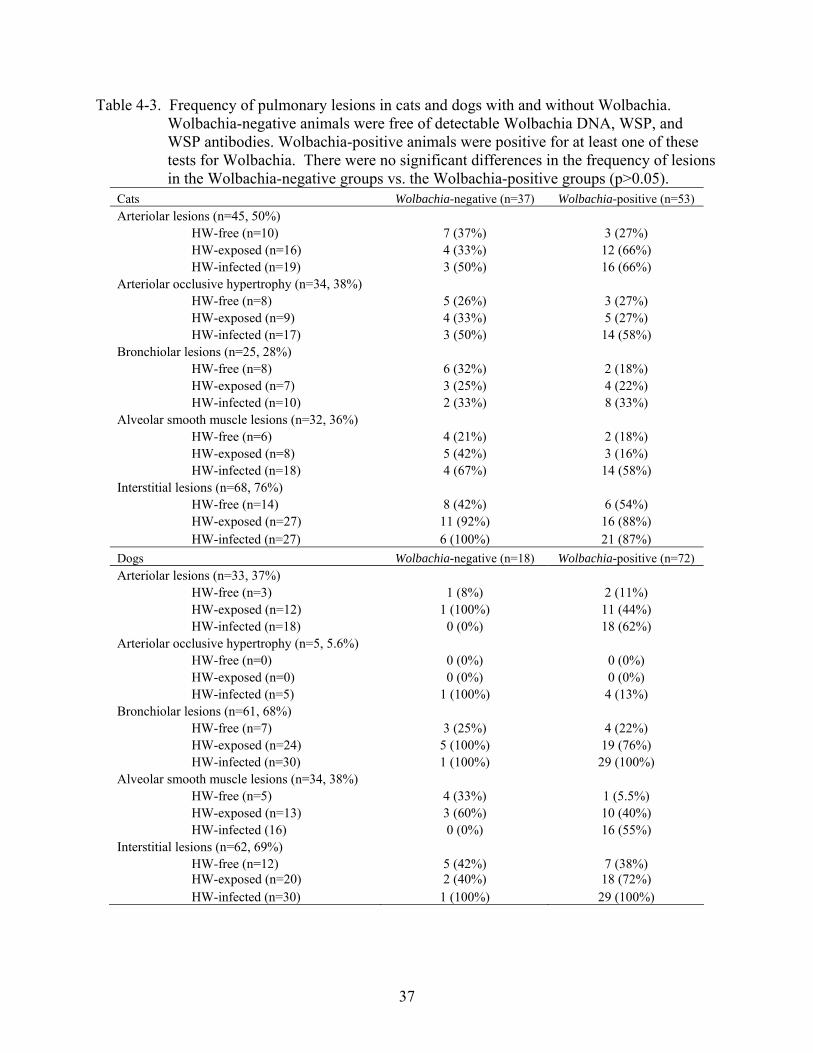
there was no clear additive effect on the prevalence of lesions when either Wolbachia DNA/WSP
was detected in pulmonary tissue or when circulating Wolbachia antibodies were detected (Table
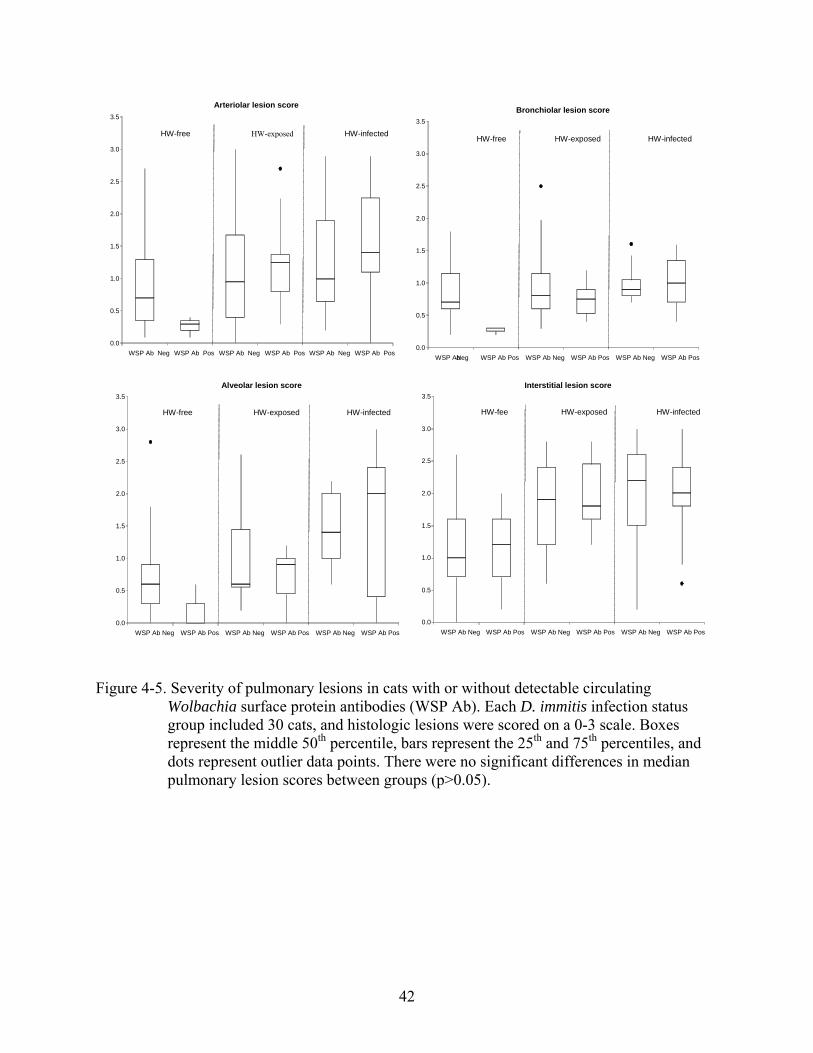
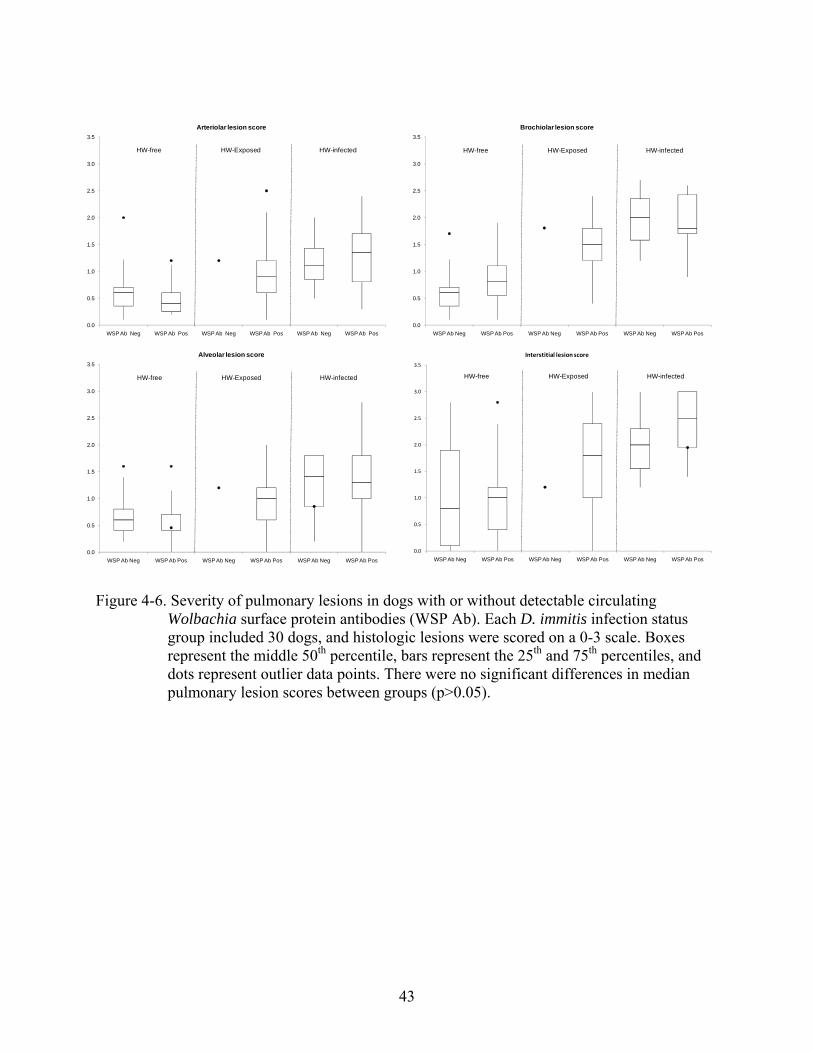
4-3). Similarly, there were no significant differences in the magnitude of pulmonary lesion
scores within each HW-infection status group regardless of whether Wolbachia DNA/WSP or
antibodies were detected (Figures 4-3 to 4-6).

35
Table 4-1. Prevalence of Wolbachia surface protein (WSP) antibodies, Wolbachia DNA, WSP, and pulmonary lesions in cats and dogs with no evidence of D. immitis infection (HW-free), evidence of either larval-stage infection or past infection (HW-exposed), or with adult D. immitis in the heart or pulmonary arteries (HW-infected). Values with different superscript letters within a row are significantly different (p<0.05).
Cats HW-free HW-exposed HW-infected
WSP antibodies 3 (10%)a 10 (33%)b 18 (60%)c Wolbachia DNA in lung 7 (23%) 12 (40%) 12 (40%) WSP in lung 4 (13%) 5 (16%) 10 (33%)
Arteriolar lesions 10 (33%)a 16 (53%) 19 (63%)b Arteriolar occlusive hypertrophy 8 (27%)a 9 (30%) a 17 (57%)b Bronchiolar lesions 8 (27%) 7 (23%) 10 (33%)
Interstitial lesions 14 (47%)a 27 (90%)b 27 (90%)b
Alveolar smooth muscle lesions 6 (20%)a 8 (27%)a 18 (60%)b Dogs
WSP antibodies 14 (46%)a 23 (76%)b 20 (66%)
Wolbachia DNA in lung 0 (0%)a 1 (3.4%)a 14(46%)b
WSP in lung 7 (23%) 4 (13%)a 12 (40%)b
Arteriolar lesions 3 (10%)a 12 (40%)b 18 (60%)b Arteriolar occlusive hypertrophy 0 (0%)a 0 (0%)a 5 (17%)b
Bronchiolar lesions 7 (23%)a 24 (80%)b 30 (100%)c
Interstitial lesions 12 (40%)a 20 (67%)b 30 (100%)c
Alveolar smooth muscle lesions 5 (17%)a 13 (43%)b 16 (53%)b
36
Table 4-2. The prevalence of Ancylostoma spp. and ascarids in cats and dogs with pulmonary lesions. Values with differ superscript letters within a row are significantly different (p<0.05).
Cats (n=90) Lesions No Lesions Ancylostoma spp. 40/81 (49%) 7/9 (78%)
Ascarids 9/81 (11%) 3/9 (33%) Dogs (n=90)
Ancylostoma spp. 48/75 (64%) 7/15 (47%) Ascarids 7/76 (9.2%) 1/13 (7.7%)
37
Table 4-3. Frequency of pulmonary lesions in cats and dogs with and without Wolbachia. Wolbachia-negative animals were free of detectable Wolbachia DNA, WSP, and WSP antibodies. Wolbachia-positive animals were positive for at least one of these tests for Wolbachia. There were no significant differences in the frequency of lesions in the Wolbachia-negative groups vs. the Wolbachia-positive groups (p>0.05).
Cats Wolbachia-negative (n=37) Wolbachia-positive (n=53) Arteriolar lesions (n=45, 50%)
HW-free (n=10) 7 (37%) 3 (27%) HW-exposed (n=16) 4 (33%) 12 (66%) HW-infected (n=19) 3 (50%) 16 (66%)
Arteriolar occlusive hypertrophy (n=34, 38%) HW-free (n=8) 5 (26%) 3 (27%) HW-exposed (n=9) 4 (33%) 5 (27%) HW-infected (n=17) 3 (50%) 14 (58%)
Bronchiolar lesions (n=25, 28%) HW-free (n=8) 6 (32%) 2 (18%) HW-exposed (n=7) 3 (25%) 4 (22%) HW-infected (n=10) 2 (33%) 8 (33%)
Alveolar smooth muscle lesions (n=32, 36%) HW-free (n=6) 4 (21%) 2 (18%) HW-exposed (n=8) 5 (42%) 3 (16%) HW-infected (n=18) 4 (67%) 14 (58%)
Interstitial lesions (n=68, 76%) HW-free (n=14) 8 (42%) 6 (54%) HW-exposed (n=27) 11 (92%) 16 (88%) HW-infected (n=27) 6 (100%) 21 (87%)
Dogs Wolbachia-negative (n=18) Wolbachia-positive (n=72) Arteriolar lesions (n=33, 37%)
HW-free (n=3) 1 (8%) 2 (11%) HW-exposed (n=12) 1 (100%) 11 (44%) HW-infected (n=18) 0 (0%) 18 (62%)
Arteriolar occlusive hypertrophy (n=5, 5.6%) HW-free (n=0) 0 (0%) 0 (0%) HW-exposed (n=0) 0 (0%) 0 (0%) HW-infected (n=5) 1 (100%) 4 (13%)
Bronchiolar lesions (n=61, 68%) HW-free (n=7) 3 (25%) 4 (22%) HW-exposed (n=24) 5 (100%) 19 (76%) HW-infected (n=30) 1 (100%) 29 (100%)
Alveolar smooth muscle lesions (n=34, 38%) HW-free (n=5) 4 (33%) 1 (5.5%) HW-exposed (n=13) 3 (60%) 10 (40%) HW-infected (16) 0 (0%) 16 (55%)
Interstitial lesions (n=62, 69%) HW-free (n=12) 5 (42%) 7 (38%) HW-exposed (n=20) 2 (40%) 18 (72%) HW-infected (n=30) 1 (100%) 29 (100%)
38
R2 = 0.181
0.00
0.20
0.40
0.60
0.80
1.00
1.20
1.40
1.60
0 20 40 60 80 100
Wolbachia surface protein absorbance
He
art
wo
rm a
nti
bo
dy
ab
so
rba
nc
e
Figure 4-1. Feline D. immitis antibody titer versus Wolbachia surface protein (WSP) antibody titer in all cats (n=90). There was a positive but weak correlation between the magnitude of the titers (p>0.001).

39
R2 = 0.1591
0.00
0.50
1.00
1.50
2.00
2.50
0.00 0.20 0.40 0.60 0.80 1.00 1.20 1.40 1.60
Wolbachia surface protein absorbance
He
art
wo
rm a
nti
bo
dy
ab
so
rba
nc
e
Figure 4-2. Canine D. immitis antibody titer versus Wolbachia surface protein (WSP) antibody titer in all dogs (n=90). There was a positive but weak correlation between the magnitude of the titers (p>0.001).
40
Figure 4-3. Severity of pulmonary lesions in cats with or without detectable Wolbachia DNA and/or Wolbachia surface protein in pulmonary tissues. Each D. immitis infection status group included 30 cats, and histologic lesions were scored on a 0-3 scale. Boxes represent the middle 50th percentile, bars represent the 25th and 75th percentiles, and dots represent outlier data points. There were no significant differences in median pulmonary lesion scores between groups (p>0.05).
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
Wolbachia Neg Wolbachia Pos Wolbachia Neg Wolbachia Pos Wolbachia Neg Wolbachia Pos
Arteriolar lesion score
HW-free HW-exposed HW-infected
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
Wolbachia Neg Wolbachia Pos Wolbachia Neg Wolbachia Pos Wolbachia Neg Wolbachia Pos
Bronchiolar lesion score
HW-free HW-exposed HW-infected
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
Wolbachia Neg Wolbachia Pos Wolbachia Neg Wolbachia Pos Wolbachia Neg Wolbachia Pos
Alveolar lesion score
HW-free HW-exposed HW-infected
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
Wolbachia Neg Wolbachia Pos Wolbachia Neg Wolbachia Pos Wolbachia Neg Wolbachia Pos
Interstitial lesion score
HW-free HW-exposed HW-infected
41
Figure 4-4. Severity of pulmonary lesions in dogs with or without detectable Wolbachia DNA and/or Wolbachia surface protein in pulmonary tissues. Each D. immitis infection status group included 30 dogs, and histologic lesions were scored on a 0-3 scale. Boxes represent the middle 50th percentile, bars represent the 25th and 75th percentiles, and dots represent outlier data points. There were no significant differences in median pulmonary lesion scores between groups (p>0.05).
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
Wolbachia Neg Wolbachia Pos Wolbachia Neg Wolbachia Pos Wolbachia Neg Wolbachia Pos
Arteriolar lesion score
HW-free HW-Exposed HW-infected
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
Wolbachia Neg Wolbachia Pos Wolbachia Neg Wolbachia Pos Wolbachia Neg Wolbachia Pos
Bronchiolar lesion score
HW-free HW-Exposed HW-infected
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
Wolbachia Neg Wolbachia Pos Wolbachia Neg Wolbachia Pos Wolbachia Neg Wolbachia Pos
Alveolar lesion score
HW-free HW-Exposed HW-infected
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
Wolbachia Neg Wolbachia Pos Wolbachia Neg Wolbachia Pos Wolbachia Neg Wolbachia Pos
Interstitial lesion score
HW-free HW-exposed HW-infected
42
Figure 4-5. Severity of pulmonary lesions in cats with or without detectable circulating Wolbachia surface protein antibodies (WSP Ab). Each D. immitis infection status group included 30 cats, and histologic lesions were scored on a 0-3 scale. Boxes represent the middle 50th percentile, bars represent the 25th and 75th percentiles, and dots represent outlier data points. There were no significant differences in median pulmonary lesion scores between groups (p>0.05).
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
WSP Ab Neg WSP Ab Pos WSP Ab Neg WSP Ab Pos WSP Ab Neg WSP Ab Pos
Arteriolar lesion score
HW-free HW-exposed HW-infected
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
WSP Ab Neg WSP Ab Pos WSP Ab Neg WSP Ab Pos WSP Ab Neg WSP Ab Pos
Alveolar lesion score
HW-free HW-exposed
HW-infected
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
WSP Ab-Neg WSP Ab Pos WSP Ab Neg WSP Ab Pos WSP Ab Neg WSP Ab Pos
Bronchiolar lesion score
HW-free HW-exposed HW-infected
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
WSP Ab Neg WSP Ab Pos WSP Ab Neg WSP Ab Pos WSP Ab Neg WSP Ab Pos
Interstitial lesion score
HW-fee
HW-exposed HW-infected
43
Figure 4-6. Severity of pulmonary lesions in dogs with or without detectable circulating
Wolbachia surface protein antibodies (WSP Ab). Each D. immitis infection status group included 30 dogs, and histologic lesions were scored on a 0-3 scale. Boxes represent the middle 50th percentile, bars represent the 25th and 75th percentiles, and dots represent outlier data points. There were no significant differences in median pulmonary lesion scores between groups (p>0.05).
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
WSP Ab Neg WSP Ab Pos WSP Ab Neg WSP Ab Pos WSP Ab Neg WSP Ab Pos
Arteriolar lesion score
HW-free HW-Exposed HW-infected
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
WSP Ab Neg WSP Ab Pos WSP Ab Neg WSP Ab Pos WSP Ab Neg WSP Ab Pos
Brochiolar lesion score
HW-free HW-Exposed HW-infected
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
WSP Ab Neg WSP Ab Pos WSP Ab Neg WSP Ab Pos WSP Ab Neg WSP Ab Pos
Alveolar lesion score
HW-free HW-Exposed HW-infected
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
WSP Ab Neg WSP Ab Pos WSP Ab Neg WSP Ab Pos WSP Ab Neg WSP Ab Pos
Interstitial lesion score
HW-free HW-Exposed HW-infected
44
CHAPTER 5 DISCUSSION
In this study, we identified the presence of Wolbachia in HW-defined groups of cats and
dogs to determine if there was an association between the bacterium and the severity of
pulmonary lesions characteristic of heartworm disease. Although pulmonary lesions were most
severe in animals with adult D. immitis there was no clear additive effect when Wolbachia was
present in sufficient amounts for detection in the lungs or when immunoreactivity against
Wolbachia was detected.
Since all D. immitis carry Wolbachia, it is difficult to separate the effect of the parasite
from the effect of its endosymbiont. In both cats and dogs, the frequency of detection of
Wolbachia in the lung of HW-exposed animals was intermediate between that of HW-free
animals and HW-infected animals. Similarly, the frequency and severity of pulmonary lesions in
HW-exposed animals also tended to be intermediate between that of HW-free animals and HW-
infected animals. Although these findings could suggest that the presence of Wolbachia in
amounts sufficient for detection in the lungs or the immune responses to Wolbachia antibodies
are associated with increased pulmonary disease, it is not possible to completely rule out an
effect of the parasite as well.
Wolbachia was detected in animals with no evidence of adult D. immitis. Studies have
demonstrated bacteria are released in large amounts when the parasite dies (Kramer et al., 2008;
Saint Andre et al., 2002). Therefore it is possible the HW-exposed group of animals had previous
D immitis infection that deposited WSP or that had initiated an anti-WSP response (Morchon et.
al., 2004).
When interpreting the pathological findings of the pulmonary tissues, it was important to
account for the potential contribution by migration of immature intestinal parasites such
45
Ancylostoma spp. and ascarids. A Baermann’s test was not conducted and it is possible other
parasites, such as lungworms, could also contribute to the pulmonary disease but escaped
detection (Patton and McCracken, 1991).
The lack of clear evidence for a role of Wolbachia in heartworm disease creates a dilemma
for veterinarians treating cats and dogs in D. immitis-endemic areas. Although the indiscriminant
use of antibiotics should be avoided, many clinicians prescribe doxycycline based on the
favorable responses observed in human filarial diseases and on promising results from the first
published studies of doxycycline use in D. immitis-infected dogs.
46
CHAPTER 6 CONCLUSIONS
Our study design was did not demonstrate that the presence of Wolbachia or WSP
antibodies was associated with increased pulmonary disease associated with D. immitis infection.
Future studies could further address this potential association by treating HW-exposed and HW-
infected animals with the anti-Wolbachia antibiotic doxycycline and observing the evolution of
pulmonary disease. Alternatively, studies could be performed to compare disease development in
animals experimentally infected with natural D. immitis versus D. immitis rendered free of
Wolbachia by doxycycline treatment.
47
LIST OF REFERENCES
Atkins, C.E., DeFrancesco, T.C., Coats, J.R., Sidley, J.A., Keene, B.W., 2000, Heartworm infection in cats: 50 cases (1985-1997). J Am Vet Med Assoc 217, 355-358.
Atkins, C.E., DeFrancesco, T.C., Miller, M.W., Meurs, K.M., Keene, B., 1998, Prevalence of heartworm infection in cats with signs of cardiorespiratory abnormalities. J Am Vet Med Assoc 212, 517-520.
Bandi, C., Anderson, T.J., Genchi, C., Blaxter, M.L., 1998, Phylogeny of Wolbachia in filarial nematodes. Proc Biol Sci 265, 2407-2413.
Bandi, C., McCall, J.W., Genchi, C., Corona, S., Venco, L., Sacchi, L., 1999, Effects of tetracycline on the filarial worms Brugia pahangi and Dirofilaria immitis and their bacterial endosymbionts Wolbachia. Int J Parasitol 29, 357-364.
Bazzocchi, C., Ceciliani, F., McCall, J.W., Ricci, I., Genchi, C., Bandi, C., 2000a, Antigenic role of the endosymbionts of filarial nematodes: IgG response against the Wolbachia surface protein in cats infected with Dirofilaria immitis. Proc Biol Sci 267, 2511-2516.
Bazzocchi, C., Genchi, C., Paltrinieri, S., Lecchi, C., Mortarino, M., Bandi, C., 2003, Immunological role of the endosymbionts of Dirofilaria immitis: the Wolbachia surface protein activates canine neutrophils with production of IL-8. Vet Parasitol 117, 73-83.
Bazzocchi, C., Jamnongluk, W., O'Neill, S.L., Anderson, T.J., Genchi, C., Bandi, C., 2000b, wsp gene sequences from the Wolbachia of filarial nematodes. Curr Microbiol 41, 96-100.
Berdoulay, P., Levy, J.K., Snyder, P.S., Pegelow, M.J., Hooks, J.L., Tavares, L.M., Gibson, N.M., Salute, M.E., 2004, Comparison of serological tests for the detection of natural heartworm infection in cats. J Am Anim Hosp Assoc 40, 376-384.
Bowman, D.D., Torre, C.J., Mannella, C., 2007, Survey of 11 western states for heartworm (Dirofilaria immitis) infection, heartworm diagnostic and prevention protocols, and fecal examination protocols for gastrointestinal parasites. Vet Ther 8, 293-304.
Browne, L.E., Carter, T.D., Levy, J.K., Snyder, P.S., Johnson, C.M., 2005, Pulmonary arterial disease in cats seropositive for Dirofilaria immitis but lacking adult heartworms in the heart and lungs. Am J Vet Res 66, 1544-1549.
Carleton, R.E., Tolbert, M.K., 2004, Prevalence of Dirofilaria immitis and gastrointestinal helminths in cats euthanized at animal control agencies in northwest Georgia. Vet Parasitol 119, 319-326.
Casiraghi, M., McCall, J.W., Simoncini, L., Kramer, L.H., Sacchi, L., Genchi, C., Werren, J.H., Bandi, C., 2002, Tetracycline treatment and sex-ratio distortion: a role for Wolbachia in the moulting of filarial nematodes? Int J Parasitol 32, 1457-1468.
48
Dillon, R., 1998, Clinical significance of feline heartworm disease. Vet Clin North Am Small Anim Pract 28, 1547-1565, x.
Genchi, C., Sacchi, L., Bandi, C., Venco, L., 1998, Preliminary results on the effect of tetracycline on the embryogenesis and symbiotic bacteria (Wolbachia) of Dirofilaria immitis. An update and discussion. Parassitologia 40, 247-249.
Genchi, C., Venco, L., Ferrari, N., Mortarino, M., Genchi, M., 2008, Feline heartworm (Dirofilaria immitis) infection: a statistical elaboration of the duration of the infection and life expectancy in asymptomatic cats. Vet Parasitol 158, 177-182.
Hermesmeyer, M., Limberg-Child, R.K., Murphy, A.J., Mansfield, L.S., 2000, Prevalence of Dirofilaria immitis infection among shelter cats. J Am Vet Med Assoc 217, 211-212.
Kozek, W.J., 2005, What is new in the Wolbachia/Dirofilaria interaction? Vet Parasitol 133, 127-132.
Kramer, L., Genchi, C., 2002, Feline heartworm infection: serological survey of asymptomatic cats living in northern Italy. Vet Parasitol 104, 43-50.
Kramer, L., Grandi, G., Leoni, M., Passeri, B., McCall, J., Genchi, C., Mortarino, M., Bazzocchi, C., 2008, Wolbachia and its influence on the pathology and immunology of Dirofilaria immitis infection. Vet Parasitol 158, 191-195.
Kramer, L., Simon, F., Tamarozzi, F., Genchi, M., Bazzocchi, C., 2005a, Is Wolbachia complicating the pathological effects of Dirofilaria immitis infections? Vet Parasitol 133, 133-136.
Kramer, L.H., Passeri, B., Corona, S., Simoncini, L., Casiraghi, M., 2003, Immunohistochemical/immunogold detection and distribution of the endosymbiont Wolbachia of Dirofilaria immitis and Brugia pahangi using a polyclonal antiserum raised against WSP (Wolbachia surface protein). Parasitol Res 89, 381-386.
Kramer, L.H., Tamarozzi, F., Morchon, R., Lopez-Belmonte, J., Marcos-Atxutegi, C., Martin-Pacho, R., Simon, F., 2005b, Immune response to and tissue localization of the Wolbachia surface protein (WSP) in dogs with natural heartworm (Dirofilaria immitis) infection. Vet Immunol Immunopathol 106, 303-308.
Lappin, M.R., Breitschwerdt, E.B., Jensen, W.A., Dunnigan, B., Rha, J.Y., Williams, C.R., Brewer, M., Fall, M., 2004, Molecular and serologic evidence of Anaplasma phagocytophilum infection in cats in North America. J Am Vet Med Assoc 225, 893-896, 879.
Levy, J.K., Snyder, P.S., Taveres, L.M., Hooks, J.L., Pegelow, M.J., Slater, M.R., Hughes, K.L., Salute, M.E., 2003, Prevalence and risk factors for heartworm infection in cats from northern Florida. J Am Anim Hosp Assoc 39, 533-537.
49
Liu, J., Song, K.H., Lee, S.E., Lee, J.Y., Lee, J.I., Hayasaki, M., You, M.J., Kim, D.H., 2005, Serological and molecular survey of Dirofilaria immitis infection in stray cats in Gyunggi province, South Korea. Vet Parasitol 130, 125-129.
Lorentzen, L., Caola, A.E., 2008, Incidence of positive heartworm antibody and antigen tests at IDEXX Laboratories: trends and potential impact on feline heartworm awareness and prevention. Vet Parasitol 158, 183-190.
Makepeace, B.L., Rodgers, L., Trees, A.J., 2006, Rate of elimination of Wolbachia pipientis by doxycycline in vitro increases following drug withdrawal. Antimicrob Agents Chemother 50, 922-927.
McCall, J.W., 2005, The safety-net story about macrocyclic lactone heartworm preventives: a review, an update, and recommendations. Vet Parasitol 133, 197-206.
Miller, M.W., 1998, Feline dirofilariasis. Clin Tech Small Anim Pract 13, 99-108.
Morchon, R., Ferreira, A.C., Martin-Pacho, J.R., Montoya, A., Mortarino, M., Genchi, C., Simon, F., 2004, Specific IgG antibody response against antigens of Dirofilaria immitis and its Wolbachia endosymbiont bacterium in cats with natural and experimental infections. Vet Parasitol 125, 313-321.
National Institutes of Health, NCBI. BLAST software. Accessed on-line at http://blast.ncbi.nlm.nih.gov/Blast.cgi.
Nelson, C.T., 2008, Dirofilaria immitis in cats: diagnosis and management. Compend Contin Educ Vet 30, 393-400; quiz 400.
Nelson, C.T., McCall, J.W., Rubin, S.B., Buzhardt, L.F., Dorion, D.W., Graham, W., Longhofer, S.L., Guerrero, J., Robertson-Plouch, C., Paul, A., 2005a, 2005 Guidelines for the diagnosis, prevention and management of heartworm (Dirofilaria immitis) infection in cats. Vet Parasitol 133, 267-275.
Nelson, C.T., McCall, J.W., Rubin, S.B., Buzhardt, L.F., Dorion, D.W., Graham, W., Longhofer, S.L., Guerrero, J., Robertson-Plouch, C., Paul, A., 2005b, 2005 Guidelines for the diagnosis, prevention and management of heartworm (Dirofilaria immitis) infection in dogs. Vet Parasitol 133, 255-266.
Newton, W.L., 1968, Longevity of an experimental infection with Dirofilaria immitis in a dog. J. Parasitol 54, 187-188.
Nogami, S., Sato, T., 1997, Prevalence of Dirofilaria immitis infection in cats in Saitama, Japan. J Vet Med Sci 59, 869-871.
Oh, H., Jun, H., You, M., Hayasaki, M., Song, K., 2008, Ectopic Migration of an Adult Heartworm in a Dog with Dirofilariasis. Korean J Parasitol 46, 171-173.
50
Patton, S., McCracken, M.D., 1991, Prevalence of Dirofilaria immitis in cats and dogs in eastern Tennessee. J Vet Diagn Invest 3, 79-80.
Pfarr, K.M., Hoerauf, A.M., 2006, Antibiotics which target the Wolbachia endosymbionts of filarial parasites: a new strategy for control of filariasis and amelioration of pathology. Mini Rev Med Chem 6, 203-210.
Ralston, S., Stemme, K., Guerrero, J., 1998, Preventing heartworm disease. Feline Pract. 26, 18-22.
Ryan, W.G., Newcomb, C.T., 1995, Prevalence of feline heartworm disease-a global perspective. In: Proceedings of the Heartworm Symposium, American Heartworm Society, Batavia, Illinois.
Saint Andre, A., Blackwell, N.M., Hall, L.R., Hoerauf, A., Brattig, N.W., Volkmann, L., Taylor, M.J., Ford, L., Hise, A.G., Lass, J.H., Diaconu, E., Pearlman, E., 2002, The role of endosymbiotic Wolbachia bacteria in the pathogenesis of river blindness. Science 295, 1892-1895.
Simon, F., Morchon, R., Rodriguez-Barbero, A., Lopez-Belmonte, J., Grandi, G., Genchi, C., 2008, Dirofilaria immitis and Wolbachia-derived antigens: its effect on endothelial mammal cells. Vet Parasitol 158, 223-231.
Snyder, P.S., Levy, J.K., Salute, M.E., Gorman, S.P., Kubilis, P.S., Smail, P.W., George, L.L., 2000, Performance of serologic tests used to detect heartworm infection in cats. J Am Vet Med Assoc 216, 693-700.
Taylor, M.J., 2003, Wolbachia in the inflammatory pathogenesis of human filariasis. Ann N Y Acad Sci 990, 444-449.
Taylor, M.J., Bandi, C., Hoerauf, A., 2005, Wolbachia bacterial endosymbionts of filarial nematodes. Adv Parasitol 60, 245-284.
Taylor, M.J., Cross, H.F., Ford, L., Makunde, W.H., Prasad, G.B., Bilo, K., 2001, Wolbachia bacteria in filarial immunity and disease. Parasite Immunol 23, 401-409.
Yabsley, M.J., Dresden-Osbourne, C., Pirkle, E.A., Kirven, J.M., Noblet, G.P., 2004, Filarial worm infections in shelter dogs and cats from northwestern south Carolina, U.S.A. Comp. Parasitol 71, 154-157.
Willard, M.D., Roberts, R.E., Allison, N., Grieve, R.B., Escher, K., 1988, Diagnosis of Aelurostrongylus abstrusus and Dirofilaria immitis infections in cats from a humane shelter. J Am Vet Med Assoc 192, 913-916.

51
BIOGRAPHICAL SKETCH
Patricia Ann Dingman was born in 1982, in Angeles City, Philippines. She attended
elementary school in Okinawa, Japan, and Plattsburgh, New York, and finished high school in
Coudersport, Pennsylvania. Patricia graduated from the State University of New York Oswego
with a B.S. in zoology in 2006. She received her M.S. in veterinary medical sciences in 2009
from the University of Florida and plans to continue her education in veterinary medicine.
When Patricia volunteered for Dr. Levy, she had the opportunity to investigate disease
transmission in cats and dogs following Hurricane Katrina and attend monthly trap-neuter-return
clinics for feral cats (Operation Catnip). These experiences have inspired her to continue
pursuing veterinary-related research in cats.