astro camp - registration application · astro camp - registration application. astro camp ® will...
TRANSCRIPT
Astro Camp - Registration Application
Astro Camp® will be held at Infinity Science Center, located at 1 Discovery Cir, Pearlington, MS 39572. (Payments and registration forms should not be mailed to this address see address below.)
Total tuition cost for Astro Camp is $140 per camper. Astro Camp/Stars tuition, in part, covers the cost of the materials used in the course of the camp, including daily meals and snacks, t-shirts, camp journals and consumables for hands-on activities.
Please make check or money order payable to NVision Solutions, Inc.
The registration application, check and all related forms should be mailed to:
NASA Stennis Space Center
Office of Education Attn: Nvision Solutions, Inc./ASTRO CAMP Roy S. Estess Bldg. Room 108 Stennis Space Center, MS 39529-6000
Registration forms may only be mailed; they may not be hand delivered.
If you have questions, please call the NASA Education Office Astro Camp Line at 228-688-3485, or 1-800-237-1821 (Option 4).
First Day of Camp Processing - MONDAY - 8:00 a.m. All parents and campers must report to the Astro Camp Infinity Science Center for day-one drop off, followed by parent orientation held at 8:35 a.m. Camp hours are 8:00 – 3:30 daily.
Please circle only one session of camp (offered by grade/date). Grade level refers to grade the child will be entering in the fall:
Astro Camp 2nd – 4th Graders Astro Camp 5th – 7th Graders STARS 8th – 10th Graders June 5-9, 2017 June 5-9, 2017
June 12-16, 2017 June 12-16, 2017 June 19-23, 2017 June 19-23, 2017
June 26-30, 2017 June 26-30, 2017 July 10-14, 2017 July 10-14, 2017 July 17-21, 2017 July 17-21, 2017
Camper’s Name: _________________________________________________________ Age: ________
Mailing Address: _______________ ____________
City/State/Zip:
Parent’s/Guardian’s Name
Daytime Phone: ( ______) ____Evening Phone: (_______) __________________
Email: ____________________________________________
Please circle T-shirt size: Youth M Youth L Adult SM Adult M Adult L Adult XL NOSL- Astro Camp Summer 2017 1

Parent Authorization
Camper’s Name: ___________________________________________________________________________
Age: ___________ Camp Dates: _____________________________________________________________
Parent / Guardian Name(s): __________________________________________________________________
Parent / Guardian Daytime Phone: ________________________ Alternate:__________________________
Email (optional) please print - _______________________________________________________________ Email will be used to send notification of upcoming camps and communication during camps. ASTRO CAMP BEHAVIOR POLICY The Astro Camp staff strives to ensure that every camper has a safe, fun and meaningful experience. Instances of unsafe behavior or misconduct, or failure to follow the directions of the staff, detract from this experience. Flagrant or repeated misbehavior will result in removal of a camper from the camp session. Upon removal from camp, readmission will be evaluated on a case by case basis, and only after a parent/staff conference. PARENTAL AUTHORIZATION
News Release As a camp participant, your child may have their photo and/or name included in our news releases or NASA website. By registering your child and completing this form, you acknowledge and authorize this action.
Camper Release To assure the protection of Astro Camp participants, please provide the name and relationship of the individuals who have your permission to pick up your child. Your child will not be released without this permission. The camp supervisor/coordinator must be notified as soon as possible for early release. Forms will be provided during camp for parents’ to place additional persons on the approved permission list for child pickup. By signing this, you acknowledge that your child will not be considered as delivered into the safekeeping of Astro Camp personnel, unless the child is delivered directly to personnel at the check in table on the second floor of Infinity.
Transportation to Events Children will be transported to events at Stennis Space Center or Michoud on NASA/Infinity tour busses. If a child becomes ill, it may be necessary for personnel to transport the child to the clinic on Stennis Space Center along with any medical information provided about the child. If a child is transported to the clinic, the parent/guardian will be notified as soon as possible. By signing this form you acknowledge and authorize that under these circumstances, your child will be transported away from Infinity Science Center. ________________________________ __________________________________ Name Relationship to Child ________________________________ __________________________________ Name Relationship to Child I hereby acknowledge and authorize all of the statements above. SIGNATURE OF: ____________________________________________________ Date: ____________ PARENT / GUARDIAN
NOSL- Astro Camp Summer 2017 2

RELEASE/CONSENT FORM Stennis Space Center
Please print name:___________________________
[Please read the following consent statement and sign below.]
I hereby consent, release and provide permission to NASA’s Stennis Space Center to use (in full or in part) all photographic and videotape images taken of me and/or audio recordings made of my voice without consideration or compensation. The images/recordings captured may be used in brochures, news releases and other types of venues and materials to promote NASA’s programs.
I hereby consent:___________________________ ________________ PLEASE SIGN YOUR NAME HERE
Date: ___________________________
Witness sign here: ___________________________ __________
Note: If person being photographed or videotaped is a minor, please complete the following information.
Parent or Legal Guardian: _______ . PLEASE PRINT AND SIGN YOUR NAME
Address:
State:_____________________________ City:_______________________ Zip Code:______________
Date of Legal Guardian Signature:____________________________________________________________
If you are with a school or other group, please provide the name of the group and contact person’s name and number:
__________________________________________________________________________________________
On behalf of Stennis Space Center, thank you for your continued support and participation in our museum,
programs and services. For more information, visit our Web site at http://.ssc.nasa.gov/public/visitors.
NOSL- Astro Camp Summer 2017 3

Astro Camp - Health and Medication Policy
Health Policy
Children who are unable to participate in the day’s activities should not be in attendance. This may be a
hardship on families, but is necessary for the health and safety of staff and all campers. If a camper is sent
home from Astro Camp due to illness, instructions will be given to the parents regarding return.
Health and Care Guidelines
1. Children who appear ill on arrival to any camp session including rash, vomiting, diarrhea, fever, red eyes
with mucous discharge, or who may be experiencing signs of a communicable ailment, cannot be admitted to
the program without written clearance from a physician stating that the child is cleared to participate and is
not contagious.
2. Children who become ill during the course of the day with any of the above symptoms, or other serious
indicators of illness, must be checked out of camp by a parent at the earliest feasible time, but no later than
two (2) hours after a parent has been notified. Failure to do so will result in disenrollment from the program.
3. The Astro Camp staff may transport the camper to the nearest medical clinic if immediate treatment is
required.
An Astro Camp Medical Release and Consent Form must be completed, signed by a parent or guardian
and submitted at registration to authorize Astro Camp staff to transport a child to a medical clinic.
4. All parents will be notified if the Astro Camp staff becomes aware that a camper has exposed others to a
communicable disease.
5. Children with special needs will be accommodated whenever possible. Before registering a child, parents
should consult with the Astro Camp staff if a special need exists. A statement from a physician must be
submitted specifying the special needs of the child.
If at all possible, parents should adjust medication schedules so that the Astro Camp staff are not responsible
for administering medications during camp. If no other alternative exists, the decision to administer
medication will be on a case-by-case basis. This decision will depend on the following conditions:
Only topical, oral, or inhaler medications will be routinely administered.
Emergency or “rescue” medications (such as epipens or asthma inhalers) will be kept in the same
location as a camper, but will only be utilized in the event of a medical crisis. Parents will be notified as
soon as possible after such medication is administered.
NOSL- Astro Camp Summer 2017 4

Medication Administration Process
Prescription medicines and over-the-counter topical medications may be administered by the Astro Camp
Staff if the following conditions are met:
1. Medication must be in original bottle/container. Containers for medications must have child-resistant
packaging.
2. Packages for medication must include original pharmacy label. The pharmacy label will include the child’s
first and last name; date prescription filled and expiration date; name of health care provider; instructions for
administration (dosage, frequency) and storage; name and strength of medication must appear on the
bottle/container of all prescription medications.
An Astro Camp Medication Authorization Form must be completed and signed by a parent or guardian
and submitted at registration before any medications can be administered. Staff will log all
medications given on the medication form.
NOSL- Astro Camp Summer 2017 5

Astro Camp Medical Release and Consent Form
Child’s Name:______________________________________________________________________________
Parent’s Name (same listed on registration):_____________________________________________________
Medical Release In the event of a medical emergency, I hereby authorize Astro Camp medical personnel designee to treat my child, who may be transported to the nearest medical facility, including a Medical Clinic. I also hereby confirm that I have read and will comply with the “Camper Health and Medication Policy.”
Please complete the Medication Authorization Form if medication is required.
Parent / Guardian Name: _____________________________________________________________________
Parent / Guardian Signature:__________________________________________________________________
Phone: (_____) _____________________________ Alternate Phone: (______) ________________________
Date: _____________________
Alternate Emergency Contact:
Name: _____________________________________________ Phone: (______) _________________________
Relationship to child: ______________________________________________________________________
Name: _____________________________________________ Phone: (______) ________________________
Relationship to child: _______________________________________________________________
Health Information In order to ensure your child's educational needs are met, please provide us with any information that would help us accommodate your child. (For instance, Astro Camp involves group and individual activities that may result in loud unexpected noise that could over stimulate some children.)
Use the space below to provide any information regarding chronic illness, allergies, or any other health or behavior information that may be helpful in assessing or treating your child in case of illness or emergency. Please be as thorough as possible; attach a separate sheet if necessary.
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________ NOSL- Astro Camp Summer 2017 6
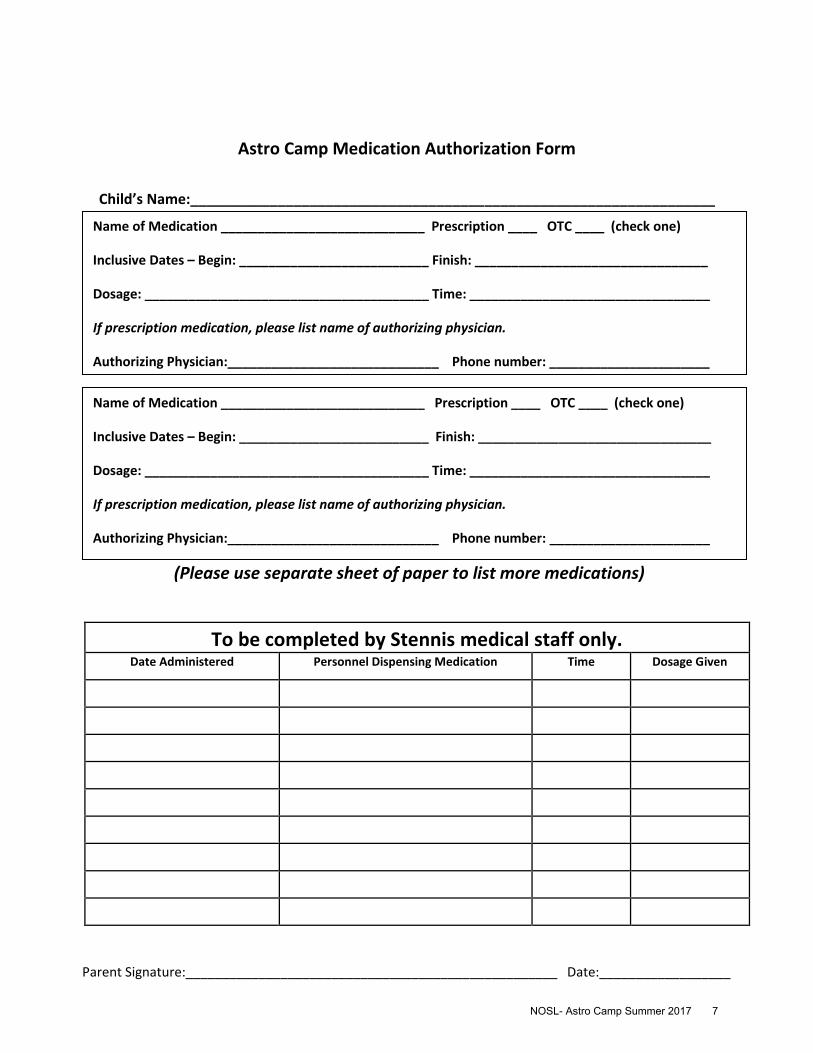
Astro Camp Medication Authorization Form
Child’s Name:__________________________________________________________________
(Please use separate sheet of paper to list more medications)
To be completed by Stennis medical staff only. Date Administered Personnel Dispensing Medication Time Dosage Given
Name of Medication ____________________________ Prescription ____ OTC ____ (check one)
Inclusive Dates – Begin: __________________________ Finish: ________________________________
Dosage: _______________________________________ Time: _________________________________
If prescription medication, please list name of authorizing physician.
Authorizing Physician:_____________________________ Phone number: ______________________
Name of Medication ____________________________ Prescription ____ OTC ____ (check one)
Inclusive Dates – Begin: __________________________ Finish: ________________________________
Dosage: _______________________________________ Time: _________________________________
If prescription medication, please list name of authorizing physician.
Authorizing Physician:_____________________________ Phone number: ______________________
Parent Signature:___________________________________________________ Date:__________________
NOSL- Astro Camp Summer 2017 7

This page is intentionally left blank

Astro Camp Parental Authorization
for
Additional Transportation Release
Child’s Name:______________________________________________________
Parent’s/ Guardian’s Name____________________________________________________________________
Parent’s/Guardian’s Contact Phone_____________________________________________________________
Dates _____________________________________________________________________________________
The individuals listed below have permission to drop off or pick up my child from Astro Camp at Infinity
Science Center. By signing this, you acknowledge that your child will not be considered as delivered into the
safekeeping of Astro Camp personnel, unless the child is delivered directly to personnel at the check in table
located inside Infinity Science Center. All Astro Camper’s must be signed out each afternoon to the Parent,
Guardian or specified individual listed below on the second floor Astro Camp reception desk. Identification is
required. Additions to the list must be made in person by the Parent/Guardian in writing. Telephone calls
cannot be accepted.
Individual Name Contact Number
1.___________________________________________________ _____________________________
2.___________________________________________________ _____________________________
3.___________________________________________________ _____________________________
4.___________________________________________________ _____________________________
5.___________________________________________________ _____________________________
6.___________________________________________________ _____________________________
Parent Signature:____________________________________________________________________________
NOSL- Astro Camp Summer 2017 8

This page is intentionally left blank