astro spring refresher 2014 management of … spring refresher 2014 management of central nervous...
TRANSCRIPT

ASTRO Spring Refresher 2014 Management of Central Nervous
System Malignancies
Christina Tsien, MD University of Michigan Medical Center

Learning Objectives • Discuss the current clinical practice in the treatment
of brain metastases
• Discuss the current clinical practice in the treatment of the major adult primary CNS tumors
• Understand the prognostic and predictive variables that allow for the appropriate selection of therapeutic choices, tailored for a specific patient

Overview
• Brain Metastases
• GBM
• Anaplastic Gliomas • Low Grade Gliomas
Presented by:

Brain Metastases
• Presentation
• Role of Surgery
• Treatment
Presented by:

What is the Appropriate Clinical Trial Endpoint in Brain Metastases Trials?
• Overall Survival Issue of “competing” systemic disease
• Response Rate
Image interpretation may be complicated by RT effect. Brain response but also systemic progression, how to score?
• Progression-free survival
Challenge with multiple metastases (individual vs composite)
• Preservation of Function -Neurocognitive Function -QOL/Symptom Burden

Brain Metastases Presentation
Signs – Hemiparesis (59%) – Cognitive problems (58%) – Hemisensory loss (21%) – Papilledema (20%) – Ataxia (19%) – Apraxia (18%)
Symptoms – Headache (49%) – Altered Mental status (32%) – Focal weakness (30%) – Ataxia (21%) – Seizures (18%) – Speech problems (12%)
Posner, 1995

RPA Class: Not all Mets are Created Equal
• Class I – <65, KPS ≥ 70, – Controlled primary – No extracranial mets
• Class II-Rest • Class III-KPS <70
•Gaspar, IJROBP, 47: 1001-6, 2000. •Gaspar, IJROBP, 37: 745-51, 1997.
(7.1)
(2.3)
N = 445 Original 1200
(4.2)

Updated Graded Prognostic Assessment (GPA) by Diagnosis
Sperduto P et al, JCO;30(4):419-25, 2012

Indications for Surgery
• Establish a tissue diagnosis
• Relieve mass effect
• Therapeutic – Randomized trials support surgery for a patient
with a solitary metastasis
Patchell RA, et al. N Engl J Med. 1990;322;494-500. Noordijk EM, et al. Int J Radiat Oncol Biol Phys. 1994;29;711-717. Mintz AH, et al. Cancer. 1996;78:1470-1476.

Randomized Surgical Trials WBRT with/without Surgical Resection
Trial Year Rx N MS Fl P-value
Patchell 90 S/RT 25 40 38 wks <0.01
RT 23 15 8 wks
Noordijk 94 S/RT 32 43 34 0.04
RT 31 26 21
Mintz 96 S/RT 41 24 ~ ns
RT 43 27 ~
Intergroup 90 S/RT 25 55
Fewer local recurrences and remained functionally independent for longer

WBRT lowers all recurrences and CNS deaths, but has no impact on survival
Phase III Surgery +/-WBRT Failure Patterns and Survival
Recurrence Surgery S + WBRT p
Anywhere in CNS 32/46 (70%) 9/49 (18%) <0.001 Local 21/46 (46%) 5/49 (10%)
CNS Death 17/39 (44%) 6/43 (14%) 0.003
Median Survival 43 weeks 48 weeks 0.39
Patchell et al. JAMA 1998;280:1485-9

Surgery for 2 - 4 Metastases
• Retrospective review of 26 patients with resection of multiple mets consistent with 26 similar patients with resected single mets
• Median survival at 1, 2, and 5 years was similar – Median: 14 months vs 14 months – 1 year: 55 vs 50% – 2 years: 32 vs 30% – 5 years: 11 vs 166%
Bindal, et al. J Neurosurg. 1993;79:210.

Enrollment: 1/96-6/01: 331 pts Arm 1: WBRT + SRS ( 164 pts) Arm 2: WBRT (37.5 Gy) alone ( 167 pts) Stratification: 1. Number of brain metastases (1 vs 2 - 3) 2. Extracranial mets (none vs present)
• < 2 cm 24 Gy • 2.1 – 3.0 cm 18 Gy • 3.1 – 4.0 cm 15 Gy
15 & 24% of 1 & 2-3 brain met pts randomized to RS did not receive it
RTOG 9508: Phase III Trial
RTOG Phase I 9005 Shaw E. Int J Radiat Oncol Biol Phys. 2000;47: 291-298.

Summary RTOG 95-08 WBRT +/- SRS
Andrews DW. Lancet. 2004;363:1665-72
Improved OS with WBRT+ SRS only in solitary brain metastasis

Survival Analyses WBRT & SRS WBR P-value
Overall 6.5 mos 5.7 mos 0.13
Solitary brain met 6.5 mos 4.9 mos 0.04
1-3 mets & Age < 50 9.9 mos 8.3 mos 0.04
1-3 mets & NSCLC 5.9 mos 3.9 mos 0.05
1-3 mets & RPA Class 1 11.6 mos 9.6 mos 0.05
Sperduto, ASTRO 2002
RTOG 9508: Subset Analysis

JRSROG 99-1 Phase III SRS +/- WBRT • 132 patients with 1-4 brain metastases < 3 cm
• WB (3 Gy x 10) + SRS vs. SRS alone
– SRS dose for lesions <2 cm: • 22-25 Gy vs. 15.4-17.5 Gy*
– SRS dose for lesions 2-3 cm:
• 18-20 Gy vs. 12.6-14 Gy*
• MRI every 3 months after treatment
Aoyama et al. JAMA 2006,295:2483-91
*30% dose reduction in RS dose if WBRT used

RESULTS: JROSG 99-1 SRS +/- WBRT
Local Tumor Control
Aoyama et al. JAMA 2006,295:2483-91

JROSG 99-1 MMSE
• Progressive disease is worse than WBRT
Aoyama, Int J Radiat Oncol Biol Phys, 68:1388-395, 2007
SRS + WBRT p
Median time to 3 point drop
7.6 mo 16.5 mo .05
1Y freedom from 3 point drop
59 % 76 %
2Y freedom from 3 point drop
52 % 69 %

MD Anderson Randomized Trial Schema
RANDOMIZE
SRS alone
(30 pts)
• RPA class I vs. II
• 1 or 2 vs. 3 Brain Mets
• Melanoma / Renal cell carcinoma vs. Other
STRATIFY
SRS + WBRT
(28 pts)

Mean Probability of NCF Decline
SRS 23%
SRS+WBRT 49%
Neuro-cognitive Decline 4 months post RT HVLT Immediate Recall
96% conf

Results: Freedom From Local Progression
Chang et al, Lancet 10(11):1037-44, 2009

Results: Overall Survival
Chang et al, Lancet 10(11):1037-44, 2009

Summary
• Small study with a single time point assessed
• Impact of disease progression on HVLT was not assessed
• Unexplained survival differences due to imbalanced arms


Results: Overall Survival
Kocher M et al, JCO 29(2):134-41, 2011
10.7 mths
10.9 mths

Rate of Intracranial Progression is Higher in Observation arm
Kocher M et al, JCO 29(2):134-41, 2011

Summary: HRQOL Results No difference in Global HRQOL between WBRT or Observation except at 9 mths
Soffietti R et al, JCO 31(1):65-72, 2013

Summary
• No difference in OS or maintenance of performance status between WBRT or Observation (OBS)
• Improved CNS control at both initial and distant sites with the addition of WBRT
• Adjuvant WBRT substantially reduced the risk of local recurrence following resection of a solitary met


SRS Dosing Post-Resection Cavity
PI: Paul Brown, MD Anderson Cancer Center

Stereotactic Radiosurgery +/- WBRT
• No clear winner or standard of care
• If only focal treatment provided (surgery or SRS) careful imaging follow up is required
• Outcomes may be best with focal treatment in a single lesion
• Clinical trial enrollment is needed to obtain high quality neuro-cognitive data to select therapy

Potential strategies to minimize risk of neuro-cognitive decline with WB RT
Coronal
Axial
Learning & Memory Short Term memory
• Memantine (RTOG 0614) • Hippocampal Sparing
(RTOG 0933)

RTOG 0614: PI Paul Brown, MD

Results • Memantine was well tolerated (similar SE to placebo)
• Less decline in HVLT-delayed recall (DR) at 24 wks in
the memantine arm (p=0.059, primary endpoint )
• Not statistically significant with only 149/508 pts analyzable at 24 wks resulting in 35% statistical power
• Memantine appears to delay time to cognitive decline compared to placebo

Results
Brown P et al, Neuro-Oncology 16(3), 2013

Conclusions • No statistically significant difference noted in HVLT-DR
at 24 wks between Memantine vs. placebo
• Overall, memantine is well-tolerated and delayed time to cognitive decline and reduced rates of decline in memory, executive function and processing speed
• Next NRG Trial will compare the role of WBRT and Memantine +/- hippocampal sparing RT in reducing long-term neuro-cognitive effects

Hippocampal Sparing Whole Brain IMRT
Gondi V, Int J Radiat Biol Phys 2010

RTOG 0933 (PI: Minesh/Gondi)
• Phase II study of Hippocampal Sparing WB RT
• Primary endpoint: HLVT-delayed recall at 4 mths -Target sample size: 102 patients -51 analyzable patients to detect mean relative HLVT-delayed recall decline ≤15%

Results/Conclusion • Median overall survival of 6.8 mths
• Conformal avoidance of the hippocampus during
WBRT – Is associated with memory and quality of life preservation
up to 6 months of f/u – Can be safely administered with 4.5% risk of relapse in the
hippocampal avoidance region (3 pts)
• Phase II results are promising but warrant further validation in a phase III trial Gondi V, ASTRO Plenary Session 2013

Advances in Treatment for Malignant Gliomas
• GBM
• Anaplastic oligodendroglioma/oligoastrocytomas
• Low Grade Gliomas

What is the Appropriate Clinical Trial Endpoint in Glioblastoma?
• Overall Survival – the gold standard
• Treatment response (Physician measured) – Radiographic response based on contrast enhanced MRI
• Clinical Improvement (Patient measured)
– Quality of Life – Neurocognitive function – Symptom Burden
Presented by:


Phase III trial of concomitant temozolomide and RT
Stupp et al; NEJM 2005

MGMT Status Correlates with OS Hegi et al, NEJM 2005
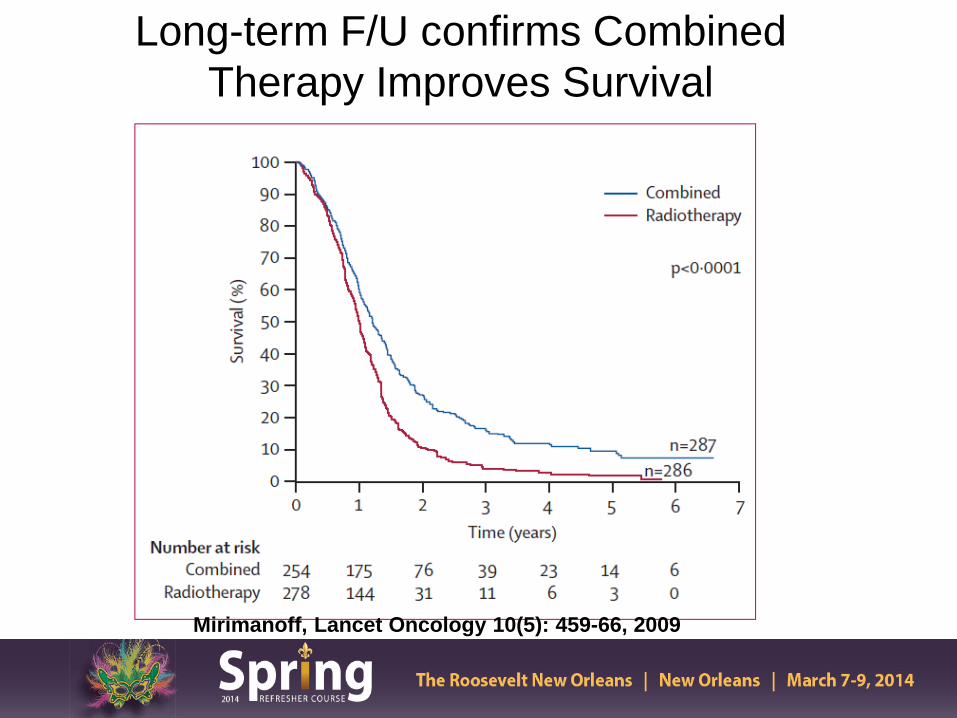
Long-term F/U confirms Combined Therapy Improves Survival
Mirimanoff, Lancet Oncology 10(5): 459-66, 2009

Who Benefits Most From Combined Therapy?
• MGMT Methylated Tumors
• RPA Class III/IV
• Age < 60
• Regardless of Type of Resection

Current Standard of Care-GBM
• Maximal safe surgical resection • Partial brain RT 60 Gy with concomitant and
adjuvant temozolomide
• No standard of care therapy at recurrence

Clinical Target Volume
• GTV plus area of microscopic disease
• MR FLAIR imaging (include edema if present) with margin (2.0 cm)
MR FLAIR

Standard Radiation 60 Gy
• PTV1= GTV + edema + 2 cm margin
PTV1= 46 Gy in 23 fx
• PTV2= GTV+ 2.5 cm margin
PTV2= 14 Gy in 7 fx
46 Gy
14 Gy

Target Volume Definition Based on MR/PET Imaging
T1-Weighted MR FLAIR MR Perfusion 11C MET PET

NRG Br-1 Trial Schema
Tsien C et al, Clin Cancer Res 18(1):273-9, 2012

Molecular Biomarkers in Glioma
• MGMT Promoter Methylation
• 1p19q
• IDH Mutations
• Genomic subtypes (Proneural etc)

IDH Mutations Associated Pathogenesis of Malignant Gliomas
Smeitink J, NEJM 2010

Low Frequency of IDH Mutations in Primary GBM
Yan et al, NEJM 360:765-73,2009

IDH1 Mutations Associated with Gliomas of Better Prognosis
Yan et al, NEJM 360:765-73,2009


Summary
• Novel molecular biomarkers in glioma require further validation
• Identify subgroup of patients with different outcome and approach to treatment

Promise of Anti-Angiogenic Therapy in GBM
VEGF expression on tumor cells

Imaging Changes with Bevacizumab: Pseudo-response
2235027
Baseline Cycle 1 Cycle 2
T1+C
T2
Taal et al, ASCO 2013
Cycle 3

Clinical Problem: Pseudoprogression

RTOG 0825:Phase III Trial Testing First-line Treatment with Bevacizumab
RT (30 Gy) TMZ (75 mg/m2 /d)
ARM A 30 Gy + Daily TMZ
(75 mg/m2 qd) + placebo q 2 wks
TMZ (150 - 200 mg/m2)
d 1-5 q28d X 12 C + placebo q 2 wks
ARM B 30 Gy + Daily TMZ
(75 mg/m2 qd) + Bev (10 mg/m2 q 2 wks)
TMZ (150 - 200 mg/m2) d 1-5 q28d X 12 C +
Bev (10 mg/m2 q 2 wks)
Eligible GBM KPS ≥ 70 Age ≥ 18 Tissue + MGMT & Molecular
Profile Analysis
R A N D O M I Z E
Stratify RPA Class MGMT
Status Molecular
Profile
R E G I S T E R
Molecular stratification factors
Clinical stratification factor
9 gene assay -Prognostic -?Predictive
Wefel, ASCO 2013

RTOG 0825
• Primary Endpoints: – Overall Survival – Progression Free Survival
• Secondary Endpoints
– Outcomes by Tumor Molecular Profile – Toxicity
• Tertiary Endpoints
– Patient Reported Outcomes: Symptoms and QOL – Neurocognitive Function

RTOG 0825- Did not meet pre-defined criteria for PFS
Gilbert M et al, NEJM 370(8): 699-708, 2014

RTOG 0825: No difference in OS
Gilbert M et al, NEJM 370(8): 699-708, 2014

No OS Benefit for BEV in any Subset
BEV PLACEBO
Gilbert M et al, NEJM 370(8): 699-708, 2014

Results • Over time, an increased symptom burden, a worse quality of life and a decline in neurocognitive function was more frequent in the bevacizumab arm
Wefel, ASCO 2013

Conclusions • Determination of progression in patients
receiving anti-angiogenic therapy is more difficult and may be delayed compared to the placebo arm
• There is a potential bias comparing the two arms at the later time points (comparing progressing vs non-progressing patients)
• In BEV treated patients, symptom burden and NCF may be identifying progressing patients prior to conventional imaging
Presented by:

AVAglio Study Design
n=463
n=458
Randomization N=921
Stratification • RPA class • Region
Treatment start 4–7 weeks post-surgery
RT 2Gy; 5 days/week
TMZ 75mg/m² qd
Placebo q2w
TMZ 150–200mg/m² qd days 1–5 q28d
Placebo q2w
RT 2Gy; 5 days/week
TMZ 75mg/m² qd
BEV 10mg/kg q2w
TMZ 150–200mg/m² qd days 1–5 q28d
BEV 10mg/kg q2w
BEV 15mg/kg q3w
Placebo q3w
Debulking surgery or biopsy
Concurrent phase 6 weeks
Tx break 4 weeks
Maintenance phase 6 cycles
Monotherapy phase until PD
Wick W, ASCO 2013

AVAGlio Trial: Investigator-Assessed PFS (Co-Primary Endpoint)
Stratified HR: 0.64 (95% CI: 0.55–0.74) p<0.0001 (log-rank test)
10.6 mo
RT/TMZ/Plb (n=463) RT/TMZ/BEV (n=458)
Prob
abili
ty o
f PFS
Months N at risk RT/TMZ/Plb RT/TMZ/BEV
463 458
349 424
247 366
170 278
110 189
77 104
47 71
23 25
8 13
4 2
0 1
0 0
0 0
0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0
0 3 6 9 12 15 18 21 24 27 30 33 36
6.2 mo
Wick W, ASCO 2013

No Difference in OS with Addition of BEV
Chinot O et al, NEJM 370(8):709-22, 2014

“Deterioration Free Survival”: Motor Dysfunction
RT/TMZ/Plb (n=463) RT/TMZ/BEV (n=458)
Stratified HR: 0.67 (95% CI: 0.58–0.78) p<0.0001 (log-rank test)
Prop
ortio
n w
ithou
t de
finiti
ve d
eter
iora
tion
1.0
0.8
0.6
0.4
0.2
0 0 3 6 9 12 15 18 21 24 27 30 33
Months
5.0 mo
8.6 mo
N at risk RT/TMZ/Plb 463 281 184 121 77 54 34 14 5 2 0 0 RT/TMZ/BEV 458 349 279 204 125 63 45 18 8 2 1 0
N at risk RT/TMZ/Plb 463 284 176 111 76 55 34 14 5 2 0 0 0 RT/TMZ/BEV 458 328 271 189 124 61 43 17 8 2 1 0 0
Stratified HR: 0.87 (95% CI: 0.68–1.11) p=0.2747 (log-rank test)
Prop
ortio
n w
ithou
t de
finiti
ve d
eter
iora
tion
0.8
0.6
0.4
0.2
0 0 3 6 9 12 15 18 21 24 27 30 33 36
Months
31.6 mo
1.0
A. Including PD B. Excluding PD
RT/TMZ/Plb Median not reached
Wick W, ASCO 2013

Deterioration-free Survival in KPS Score
Chinot O et al, NEJM 370(8):709-22, 2014

Conclusions
• In the Avaglio trial, the addition of Bevacizumab showed an improvement in PFS but did not show an improvement in OS
• Gr 3 or higher adverse events was more frequent in
the Bevacizumab than placebo arm respectively (67% vs 51%)
• Decreased need for steroid use, baseline HRQOL and KPS were maintained longer in the bevacizumab arm
Presented by:

Summary • There is no overall survival benefit in the upfront
use of Bevacizumab in newly diagnosed GBM
• Further analysis is required to confirm a role for specific patient populations that may benefit from Bevacizumab (molecular profile, unresectable patients, etc)
Presented by:

Howard Fine, ASCO Plenary 2013

Pseudo Progression
• Reported rates in 15-30% of pts treated with combined chemo-RT
• Higher rate in patients with methylated MGMT promoter (Brandes, JCO 2008)
• Critical to recognize due to its influences on treatment choices and therefore possibly prognosis

Pseudo-Progression
• Currently, there are no reliable methods for distinguishing pseudo-progression from disease progression exist.
• Advanced MR imaging can reveal early differences in vascular properties and tumor cellularity. MR perfusion showed significant changes in rCBV were predictive of progressive disease (p<0.01) Tsien, JCO 2010

RANO Response Criteria
Criterion CR PR SD PD
T1-Gd + None ≥ 50% ↓ < 50% ↓ - < 25% ↑ ≥ 25% ↑*
T2/FLAIR Stable or ↓ Stable or ↓ Stable or ↓ ↑*
New Lesion None None None Present*
Steroids None Stable or ↓ Stable or ↓ NA**
Clinical Status Stable or ↑ Stable or ↑ Stable or ↑ ↓*
Requirement for response
All all All Any*
Wen P et al, JCO 2010

Why is the outcome poor for older patients with GBM ?
• Is biology worse than younger patients?
• Is there a higher rate of morbidity and mortality associated with conventional therapy delivered in older patients?
• Are the majority of patients simply not considered for therapy?

Scott J et al, Cancer 118:5595-600, 2012
RPA Classification of Prognostic Factors in GBM Pts ≥ 70 years of age

RT vs Best Supportive Care
Keime-Guibert et al, NEJM 356:1527-35, 2007 (France) *Trial discontinued early due to planned interim analysis

Hypofractionated vs Standard RT Course
Roa et al, JCO 22:1583-88, 2004, *KPS=70

Nordic Brain Tumor Study Grp
342 GBM pts ≥ 60 yrs of age phase III study A) 60 Gy in 30 fx RT (MS 6 mths) B) 34 Gy in 10 fx RT (7.5 mths) C) TMZ alone (8.3 mths)
Malmstrom A et al, Lancet Oncol 13(9):916-26, 2012
OS > 70 yrs OS for all pts

Health Related QOL analysis for 3 treatment groups
TMZ 60 Gy 34 Gy
Malmstrom A et al, Lancet Oncol 13(9):916-26, 2012

NOA-8 German Study 412 pts ≥ 65 yrs age GBM/AA prospective, randomized phase III multi-institutional study • A) dose dense TMZ alone (MS 8 mths) • B) 54- 60 Gy RT alone (MS 9.6 mths)
Wick W et al, Lancet Oncol 2012; 13: 707–15

OS in relation to MGMT promoter methylation status/treatment received
Wick W et al, Lancet Oncol 2012; 13: 707–15

Combined Chemo-RT
• Phase III EORTC/NCIC trial concurrent and adjuvant TMZ vs RT alone, 30% of patients were between 60-70 yrs of age – 2 yr OS benefit for chemo-RT 22% vs 6% RT arm
(Stupp R et al, Lancet Oncol 10(5):459-66,2009)
• Retrospective data chemo-RT improves median survival in favorable GBM grp in pts 65-70 and ≥ 71 yrs (Barker et al, J Neuro-onc 109:391-397,2012)
• EORTC-NCIC CTG Elderly GBM: Phase III randomized
study 40 Gy in 15 fractions alone or with concurrent and adjuvant TMZ

Summary
• In older GBM patients, combined Chemo-RT (Stupp regimen) has not been compared to a hypo-fractionated RT course with/without chemotherapy in regards to OS, HRQOL, and neuro-cognitive function
• Treatment should be recommended based on molecular predictive biomarkers and clinical factors

Anaplastic Oligodendroglioma

Molecular classification of anaplastic oligodendroglioma
• 1p/19q co-deletion is a biomarker of oligodendroglioma – Predictive and prognostic – Somatic mutations in CIC gene on 19q and FUBP1 gene
[encoding far-upstream element (FUSE) binding protein] on 1p contribute to AO pathophysiology
• CIC mutations seen in 69% of 1p19q co-deleted tumors in one study
• 1p19q often associated with IDH1 mutation and MGMT promoter methylation – Favorable overall molecular phenotype – 1p19q is the only one validated for
treatment decisions
Presented by:
Bettegowda et al, Science, 2011 Capper et al, Acta Neuropathol, 2011 Van den Bent, Clin Cancer Res, 2011 Mulholland, Int J Cancer, 2012 Yip et al, J Pathol, 2012

Anaplastic Oligodendroglioma

• 1p/19q co-deletion detected in 44% (PCV+RT) and 52% (RT)
Cairncross G. JCO 2013, 31:337
PCV+RT did not significantly increase survival compared to RT in all patients

• Median OS
– 14.7y (PCV+RT) – 7.3y (RT)
• PFS
– 8.4y (PCV+RT) – 2.9y (RT)
Cairncross G. JCO 2013, 31:337
PCV+RT improved survival in 1p/19q deleted patients only

IDH Mutational Status Identifies AO Patients that benefit from PCV Chemotherapy with RT
IDH Mutated and 1P/19Q Co-Deleted IDH Mutated and 1P/19Q Non Co-Deleted
Cairncross J G et al. JCO 2014;32:783-790


van den Bent M. JCO 2013, 31:344
• Improved OS in RT/PCV arm: 42 vs 30 mo (p=0.018)
•Improved PFS in RT/PCV arm: 24 vs 13 mo (p=0.003)
•Only 30% pts in the RT/PCV arm received 6 cycles (median 3 cycles delivered)
RT/PCV improved survival in all pts
van den Bent M. JCO 2013, 31:344

van den Bent M. JCO 2013, 31:344
• 1p/19q co-deletion seen in 25% of pts (n=80) with tissue available for analysis
Median Overall Survival RT/PCV RT
Co-deleted Not reached 112 mo
Non co-deleted 25 mo 21 mo
Median PFS RT/PCV RT
Co-deleted 157 mo 50 mo
Non co-deleted 15 mo 9 mo
Improved OS benefit of RT/PCV appears greater for pts with 1p/19q deletion
van den Bent M. JCO 2013, 31:344

van den Bent M. JCO 2013, 31:344
IDH and MGMT methylation prognostic for improved overall survival

Other approaches for newly diagnosed AO • Retrospective data: 1013 patients diagnosed from
1981-2007 – Before 1990 – RT alone – After 1990 50% chemo – 2005-2007 38% chemo alone in 1p19q co-deleted patients
• TMZ 87% and PCV 2% trend starting in 2000 – Overall TTP outcome:
• RT + chemo: 7.2 years • Chemo alone: 3.9 years
– PCV appeared better than TMZ • RT alone: 2.5 years
• Question 1: Is Stupp/EORTC regimen as good for AO with 1p19q co-del as RT/PCV?
• Question 2: what is the best course for non-deleted AO?
Presented by:
Panageus et al, NeuroOncol 2012 Lassman et al , 2011

Ongoing clinical studies for AOA and AO • Concurrent and/or Adjuvant Temozolomide for 1p19q non-
deleted tumors (CATNON) – 4 treatment arms:
• RT alone • RT concurrent TMZ • RT adjuvant TMZ • Stupp regimen
• CODEL
– For patients with 1p19q co-deletion – Randomized to:
• RT + PCV • RT + concomitant and adjuvant TMZ • TMZ alone (exploratory)

Conclusions

Low Grade Gliomas
• 2,000-3000 cases diagnosed yearly in the US
• Heterogeneous group of neoplasms usually occur in younger patients
• WHO Gr 2 astrocytomas, oligodendroglioma and oligoastroctyomas

Unfavorable Prognostic Factors in LGG
• Age ≥ 40
• Largest diameter ≥ 6 cm
• Tumor crossing midline
• Astrocytoma dominant histology
• Neurologic deficit
Pignatti F JCO 2002, 20:2076

Role of Resection for Low Grade Gliomas
• Provides more accurate diagnosis
• Improves neurological status and quality of life
• Gross total resection extends survival
Presented by:

A. Pts with larger pre-op volume have significantly shorter PFS B. Pts with complete resection of FLAIR abnormality have significantly longer OS C. Even small residual volumes adversely affect survival D. Patients with a greater percentage of tumor resection have significantly longer
OS Smith JS JCO 2008, 26(8):1338
p<0.001
p<0.001
p=0.001
p=0.001
Extent of Resection Improves Survival in Low Grade Gliomas

EORTC 22845- “Non-Believer’s Trial”
Karim et al, IJROBP 36: 549, 1996

Wait and see Early RT Median PFS 3.4 years 5.3 years 5yr PFS 35% 55%
van den Bent MJ Lancet 2005, 366:985
Early RT improves PFS
van den Bent MJ Lancet 2005, 366:985

Wait and see Early RT Median OS 7.4 years 7.2 years
5yr OS 66% 68%
van den Bent MJ Lancet 2005, 366:985
Same OS and PFS results when only WHO grade II tumors analyzed
Overall survival not affected by early RT
van den Bent MJ Lancet 2005, 366:985

45 Gy 59.4 Gy 5yr PFS 47% 50% 5 yr OS 58% 59%
No difference in PFS or OS with higher RT doses Karim IJROBP 1996, 36:549
EORTC 22844- “Believer’s Trial” A Randomized Trial on Dose-Response in RT
Of Low Grade Cerebral Glioma

• 203 patients 14% GTR, 35% STR, 51% biopsy
• Randomized:
– 50.4 Gy in 1.8 Gy/fx – 64.8 Gy in 1.8 Gy/fx
• (50.4 Gy + 2cm to preop tumor volume; 14.4 Gy +1cm boost)
• Median f/u 6.4 years
Shaw E JCO 2002, 20:2267
NCCTG/RTOG/ECOG Randomized Study of Low vs High Dose RT in Low Grade Glioma

• 5 yr OS was similar – 72% in the 50.4 Gy arm – 64% in the 64.8 Gy arm (p = 0.48)
Shaw E JCO 2002, 20:2267
No survival benefit with higher RT doses
Shaw E JCO 2002, 20:2267
• 5 yr actuarial incidence of radionecrosis
2% in the 50.4 Gy arm 10% in the 64.8 Gy arm

Low Grade Gliomas: RTOG 98-02

93%
66%
48%
50%
• Significantly lower OS in high risk group
• PFS is ~50% at 5 yrs, regardless of GTR estimate or age Shaw EG. J Neurosurgery 2008, 109(5):835-41
OS and PFS in Low and High Risk Low Grade Glioma Pts

PFS p=0.005 OS p=0.13
• PFS but not OS was improved with RT + PCV • Significantly higher incidence of grade 3 and 4 hematologic toxicity
with RT + PCV (66% vs 11%)
• )
Shaw EG. JCO 2012, 25:3065
Improvement in PFS but not overall Survival

RTOG 98-02 NCI Press Release
• With median f/u of 12 yrs, there was a significant improvement in OS for patients receiving RT+ PCV (13.3 yrs) vs RT alone (7.8 yrs)
• New standard of care for treatment of LGG
• Molecular subset analyses is still on-going

ECOG/Intergroup Phase III trial E3F05 of RT ± TMZ

EORTC 22033-26033: Study Schema
EORTC ROG and BTG, NCI-CTG, TROG, MRC-CTU
Stratification: 1p mutation, contrast on MRI, age and PS, institute, contrast enhancement MRI, age: <40 vs ≥ 40 yrs, WHO PS 0 /1 versus 2
Registration
Radiotherapy (standard arm): 50.4 Gy (28 x 1.8 Gy)
conformal techniques
Random Genetic testing
TMZ (experimental arm): 75 mg/m2 daily x 21 days,
q 28 days until progression or for max. 12 cycles
Initial results do not show a difference in PFS in TMZ arm compared to RT 1p deletion was confirmed to be a positive prognostic factor in both groups

Results • Initial results do not show a difference in PFS in
TMZ arm compared to RT but follow-up is short
• 1p deletion was confirmed to be a positive prognostic factor in both groups
• Further molecular analyses are on-going to determine which subgroup may benefit from TMZ alone

Conclusions • Recent press release suggest a new standard
of care for low grade glioma patients requiring radiation treatment; these patients may now be considered for adjuvant chemotherapy (PCV vs TMZ)

EORTC-NCIC 26021
– Postop MRI at 4-5 months confirming subtotal resection – <4 mitoses/10 HPF and MIB labeling index <4% – RS 12-15 Gy to tumor margin – EBRT 54 Gy in 30 fractions to tumor + 1.5-2.0 cm margin – Targeted sample size 478 patients
• Endpoints: Progression-Free Survival Also: Quality of Life, Survival, Incidence of Salvage Surgery,
Incidence of Acute and Long-term Neurotoxicity
Phase III Study of Adjuvant Radiotherapy or RS vs Observation Only in Patients with
Newly Diagnosed, Incompletely Resected, WHO Grade I Non-Orbital Meningioma