asymptomatic bacteriuria in pregnancy - nvmm.nl · what is asb? asb = asymptomatic bacteriuria...
TRANSCRIPT
Asymptomatic
bacteriuria in pregnancy Brenda Kazemier
AIOS gynaecologie Amsterdam UMC

Physiologic changes in pregnancy
UTI in pregnancy more often complicated
Pregnancy
Change immune system woman
Urinary stasis
Vesicoureteral reflux
Diabetes
Puerperium
Decreased bladder sensitivity
Bladder overdistension
Catheterization
What is ASB?
ASB = ASymptomatic Bacteriuria
Presence of bacteria in urine without complaints of UTI
Cutoff ≥ 10e5 colony forming units per ml
Incidence in pregnancy around 2-10%
Some even report up to 40%
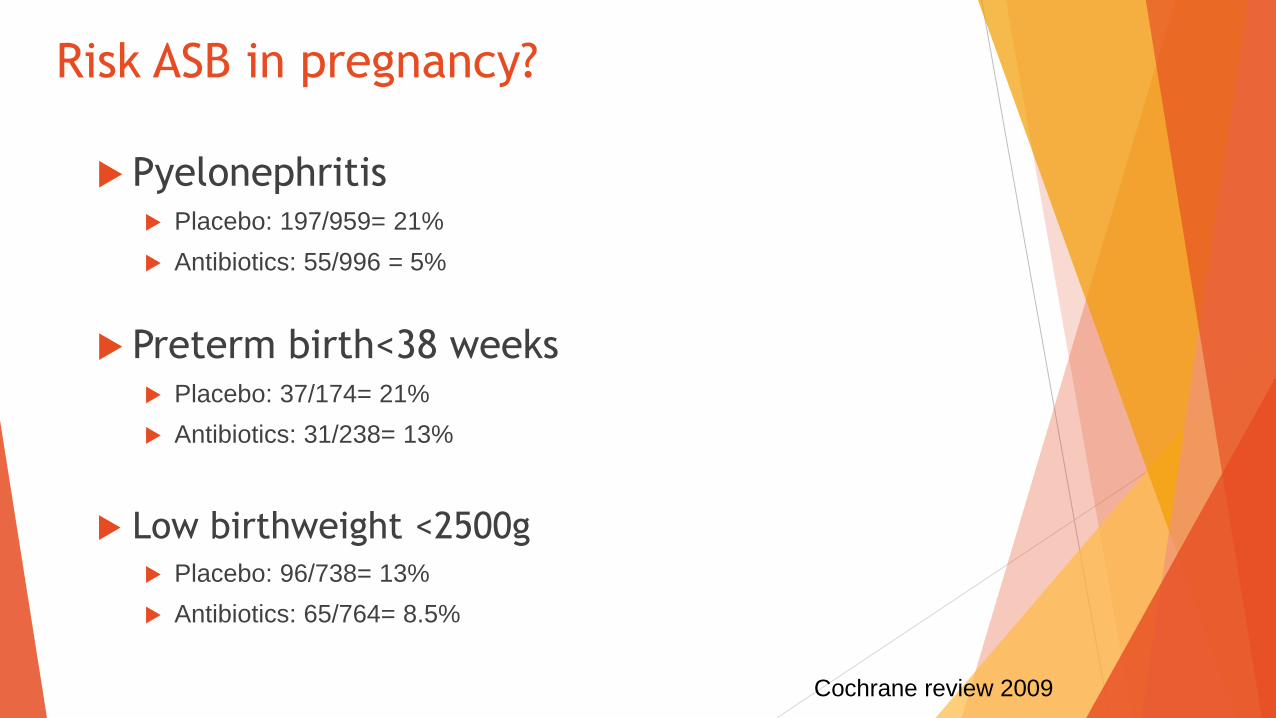
Risk ASB in pregnancy?
Pyelonephritis Placebo: 197/959= 21%
Antibiotics: 55/996 = 5%
Preterm birth<38 weeks Placebo: 37/174= 21%
Antibiotics: 31/238= 13%
Low birthweight <2500g Placebo: 96/738= 13%
Antibiotics: 65/764= 8.5%
Cochrane review 2009
Why repeat trials?
Existing data outdated, trials published between 1960 and1987
No ultrasound for dating pregnancy, diagnosis preterm birth?
Incidence ASB and pyelonephritis unknown in the Netherlands
Other countries allready screen and treat routinely
Netherlands relatively conservative with antibiotics
Study design
Screen study with embedded randomised controlled trial
Population: low risk women between 16-21 weeks of pregnancy
Exclusion criteria:
Symptomatic or use of antibiotics
Previous preterm delivery <34wks
Diabetes Mellitus
Known structural anomalies urinary tract
Allergy to nitrofurantoin
Multiple pregnancy
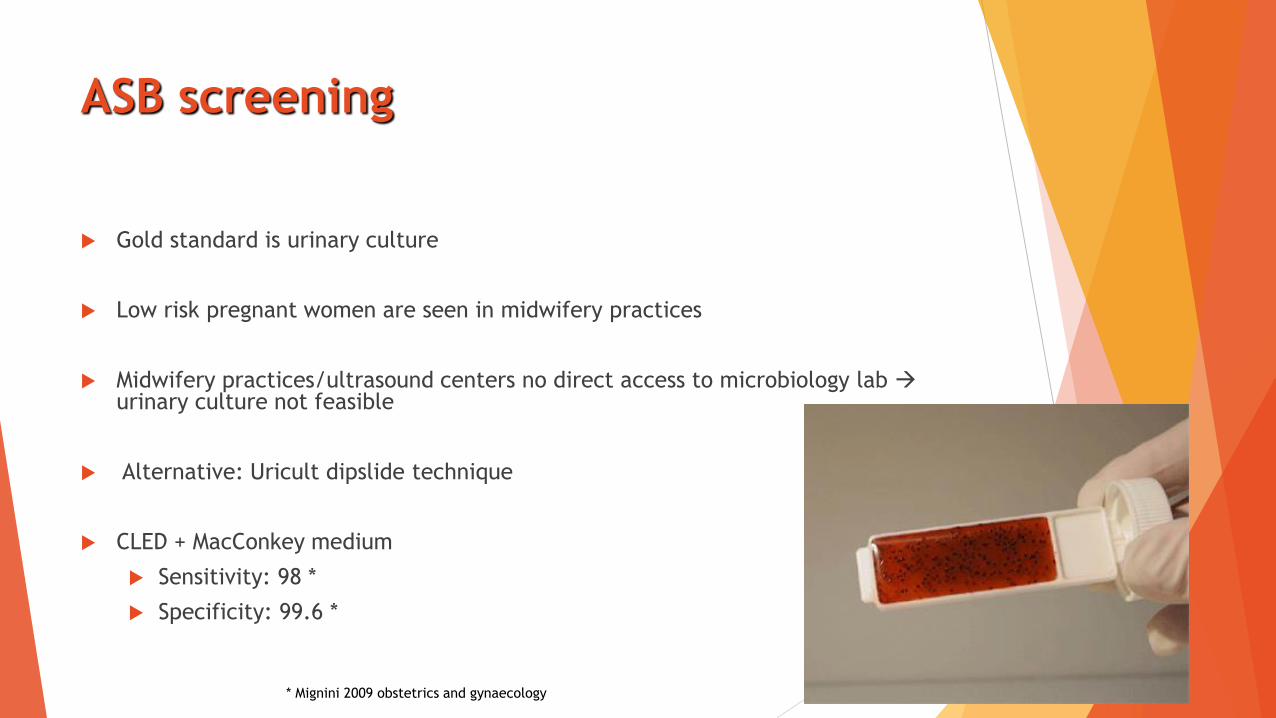
ASB screening
Gold standard is urinary culture
Low risk pregnant women are seen in midwifery practices
Midwifery practices/ultrasound centers no direct access to microbiology lab urinary culture not feasible
Alternative: Uricult dipslide technique
CLED + MacConkey medium
Sensitivity: 98 *
Specificity: 99.6 *
* Mignini 2009 obstetrics and gynaecology
Interpretation of dipslides
Dipslides were sent to one central laboratory (Laboratory for infectious
diseases, Groningen)
The isolates of positive dipslides were determined by standard methods and
VITEC automated systems (BioMerieux) and if the culture is positive, only the
dominant phenotype (two types at most) will be analyzed.
Resistance of all uropathogens for the most commonly used antimicrobial
agents will be determined following EUCAST guidelines and breakpoints.
ASB treat
Randomized controlled trial
Intervention: 2x100mg nitrofurantoin for 5 days or placebo
1 week after end of treatment follow up culture

Outcomes ASB trial
Composite primary outcome:
• Pyelonephritis &/or preterm birth <34 wk
Secondary outcomes
- Neonatal outcomes (preterm birth, growth restriction)
- Maternal morbidity (UTI)
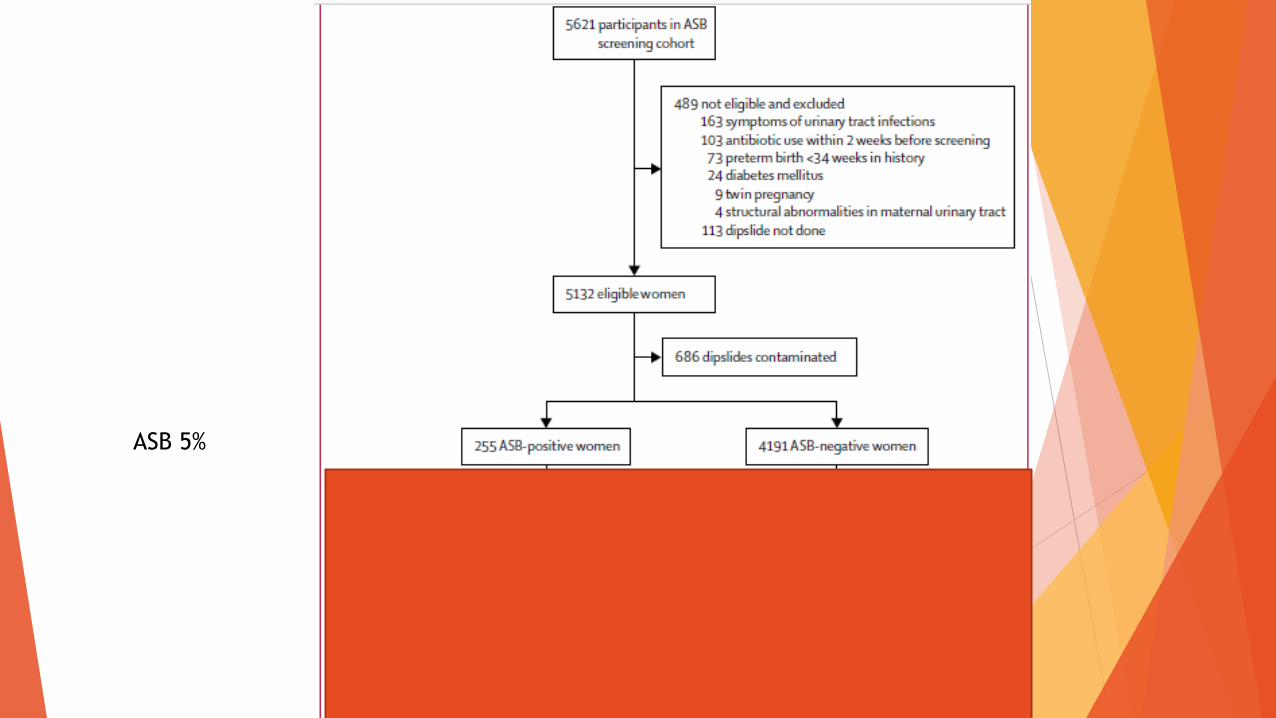
ASB 5%
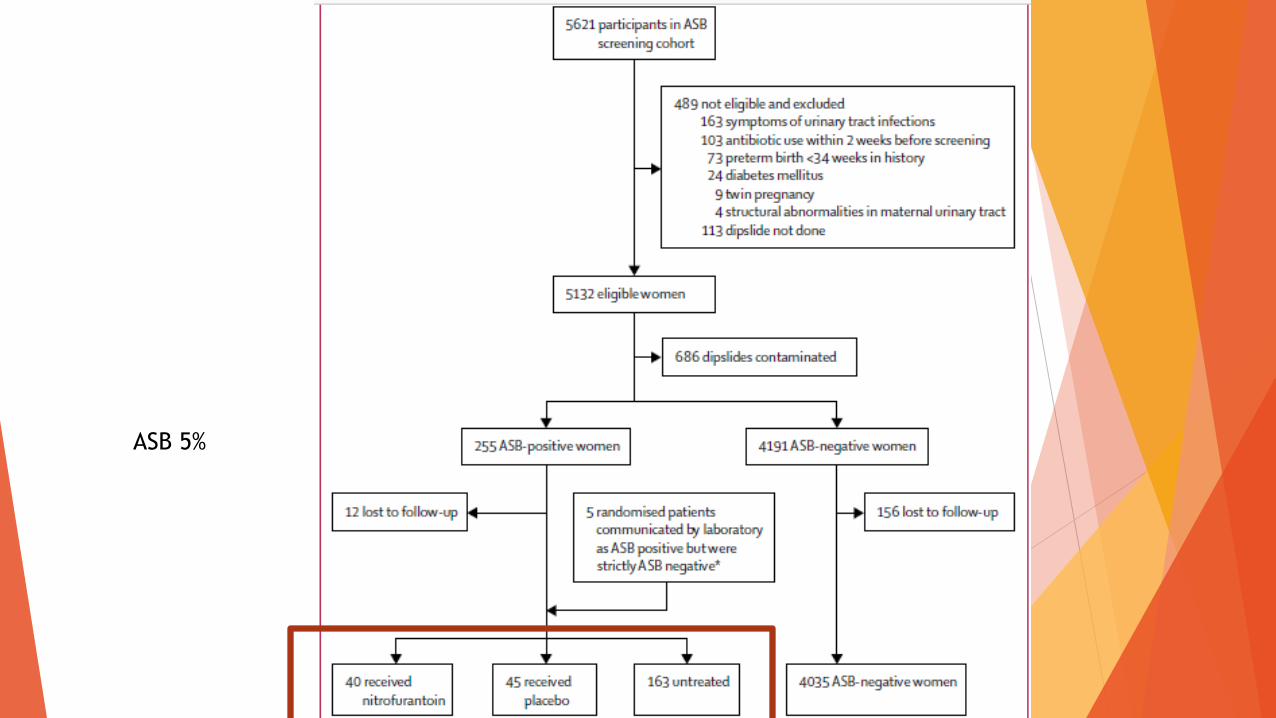
ASB 5%
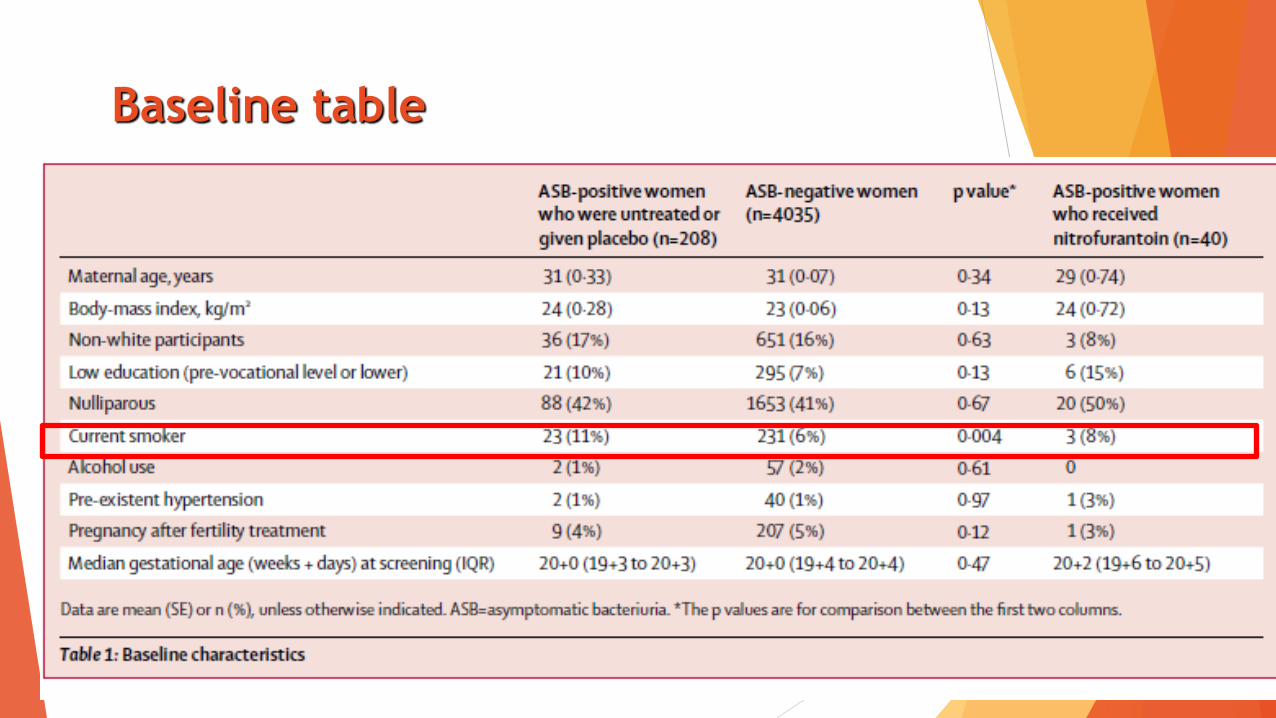
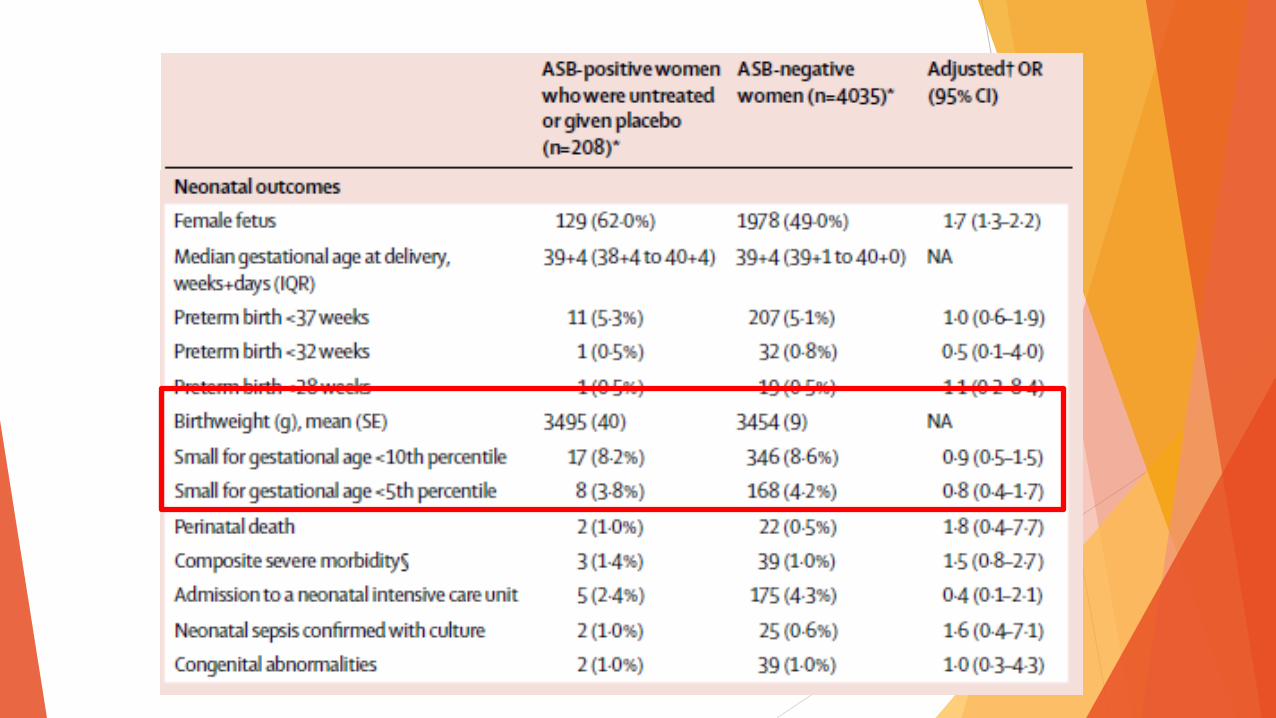
Baseline table

5,3
0,5 0,5
5,1
0,8 0,5
0
1
2
3
4
5
6
Preterm birth <37weeks
Preterm birth <32weeks
Preterm birth <28weeks
Preterm birth in women with and without ASB
ASB No ASB
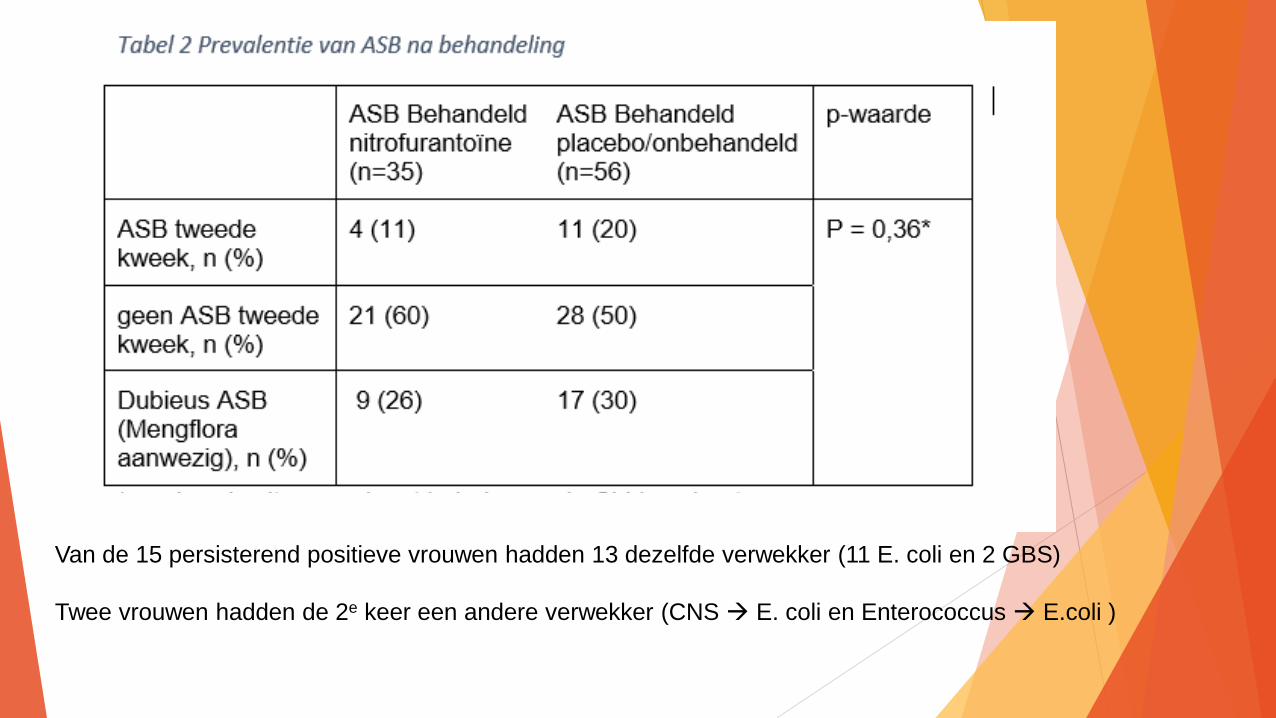
Van de 15 persisterend positieve vrouwen hadden 13 dezelfde verwekker (11 E. coli en 2 GBS)
Twee vrouwen hadden de 2e keer een andere verwekker (CNS E. coli en Enterococcus E.coli )
Subanalyses cohort
Symptomatische UWI vs geen symptomatische UWI
Klachten passen bij UWI + behandeling met antibiotica
Klinische diagnose, geen kweken bekend
Maternale en neonatale uitkomsten
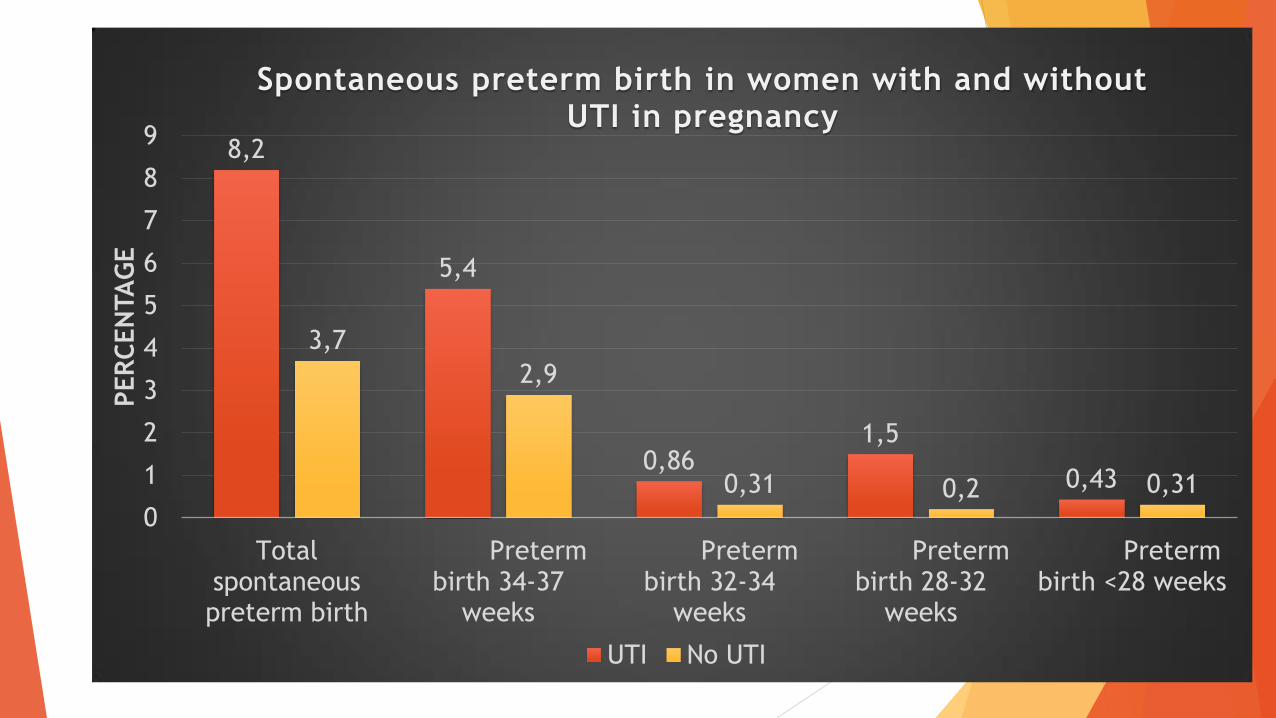
8,2
5,4
0,86 1,5
0,43
3,7
2,9
0,31 0,2 0,31
0
1
2
3
4
5
6
7
8
9
Totalspontaneouspreterm birth
Pretermbirth 34-37
weeks
Pretermbirth 32-34
weeks
Pretermbirth 28-32
weeks
Pretermbirth <28 weeks
PER
CEN
TA
GE
Spontaneous preterm birth in women with and without UTI in pregnancy
UTI No UTI

Conclusion
• Prevalence ASB in the Netherlands is 5%
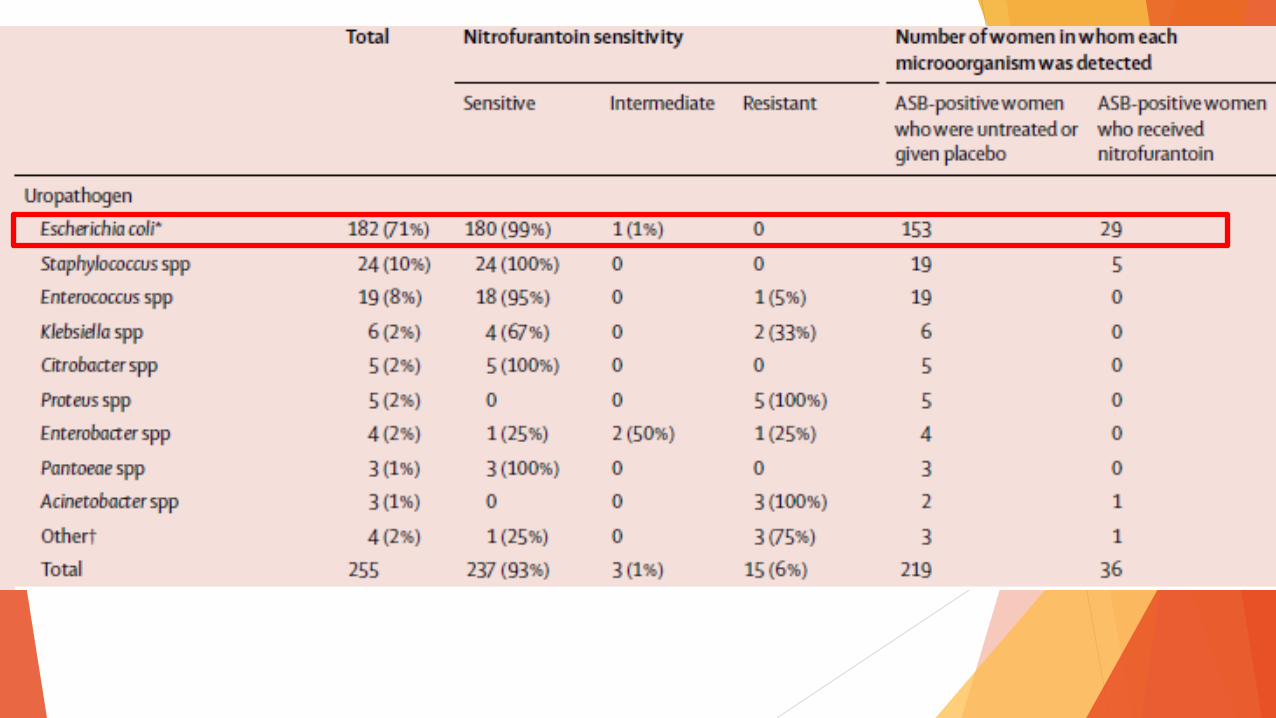
• Uropathogens conform literature
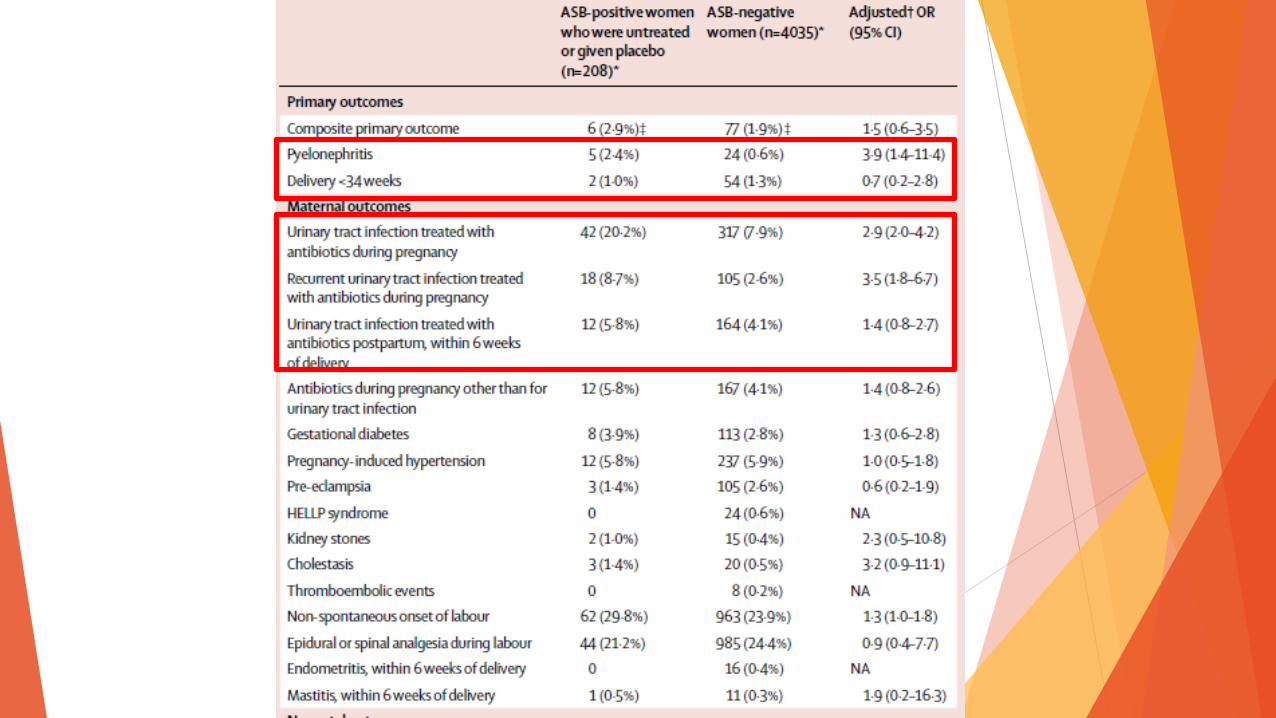
• Women with untreated ASB are at increased risk of pyelonephritis and symptomatic UTI during
pregnancy.
• The absolute risk of pyelonephritis with untreated ASB is small (2%) and much lower than
currently reported in literature (21%)
• Most women with pyelonephritis did not have ASB around 20 weeks of gestation (83%)
Conclusion • 50% of women receiving placebo were ASB negative 1 week after end of treatment
• 11% of women receiving nitrofurantoin were persistent ASB positive 1 week after end of treatment
• Compliance? Length of treatment?
• Women with ASB are not at increased risk for preterm birth or low birth weight
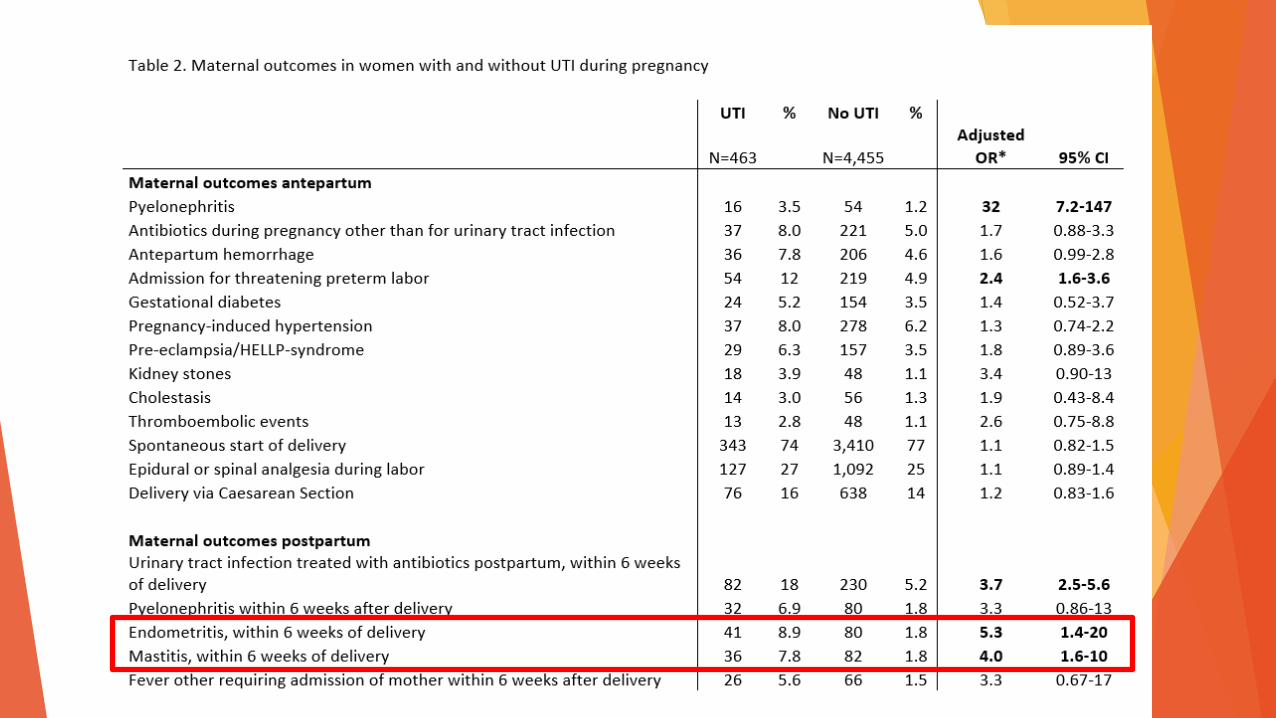
• Women with symptomatic UTI are at increased risk for preterm birth
• And at increased risk for endometritis and mastitis after birth
Discussion The biggest challenge remains differentiating between significant (disease) and
insignificant colonisation (not related to symptoms or adverse events)
Symptoms in pregnancy very difficult
Not clear which microorganisms are considered uropathogens and which are contaminants resulting in a wide range of reported incidences of ASB
Can differences in virulence explain difference in preterm birth risk between ASB and symptomatic UTI?
Do women with UTI represent a subtype of pregnant women at high risk for complications in general?
Not only increased preterm birth but also mastitis and endometritis
Perhaps not UTI leading to preterm birth but other common risk factors?
Consequences ASB in high risk women?

Questions?
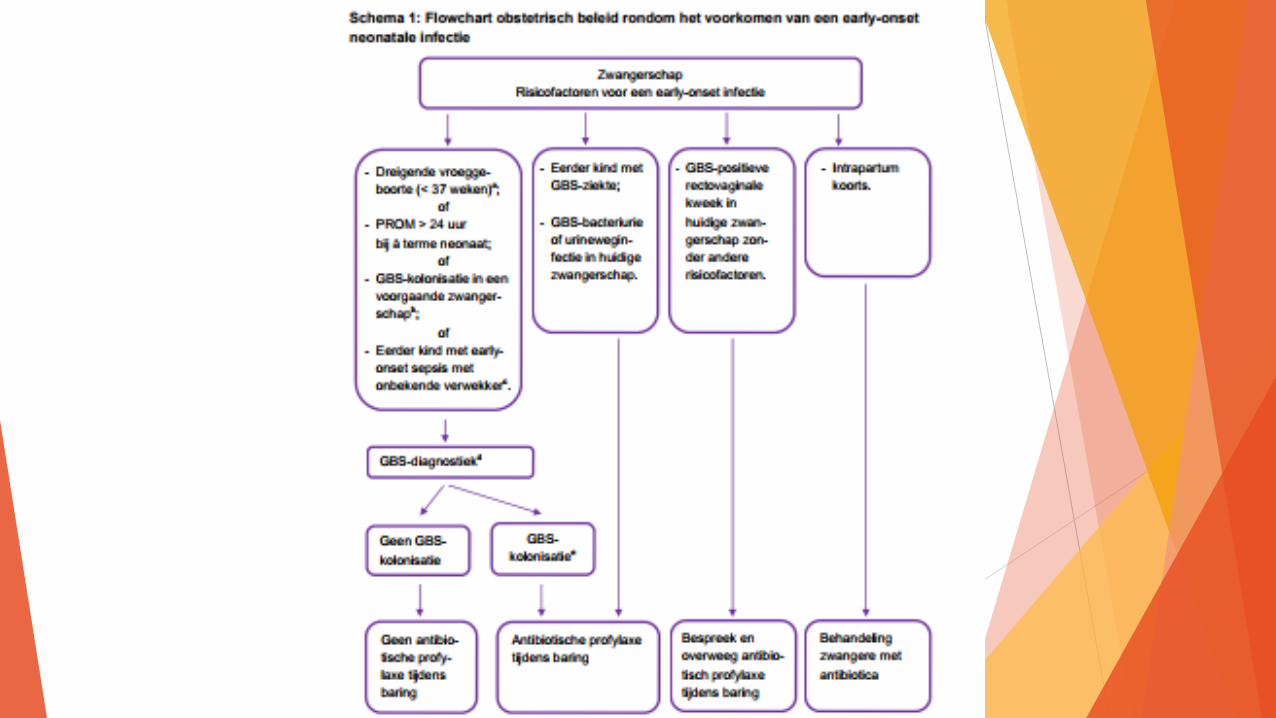
GBS bacteriuria
Any amount of GBS was present in 77 women (1.5%)
None had GBS present in at least 10e5 CFU/ml or more.
GBS was found as an isolated micro-organism (less than 10e5 CFU/ml) in 58 women and on
contaminated dipslides in 19 women.
Analysis on outcomes of these pregnancies will be performed in future