asymptomatic hypogammaglobulininemic patients do we need immunoglobulins?
DESCRIPTION
Asymptomatic hypogammaglobulininemic patients Do we need immunoglobulins?. Jiří Litzman, Marcela Vlková, Maria Šárfyová Dept Clin Immunol Allergol, Masaryk University, Brno. Biological functions of immunoglobulins. Act i vation of complement system (IgG, IgM) Opsonization (namely IgG) - PowerPoint PPT PresentationTRANSCRIPT

Asymptomatic Asymptomatic hypogammaglobulininemic hypogammaglobulininemic
patientspatientsDo we need Do we need
immunoglobulins?immunoglobulins?
Jiří Litzman, Marcela Vlková, Maria Jiří Litzman, Marcela Vlková, Maria ŠárfyováŠárfyová
Dept Clin Immunol Allergol, Dept Clin Immunol Allergol, Masaryk University, BrnoMasaryk University, Brno
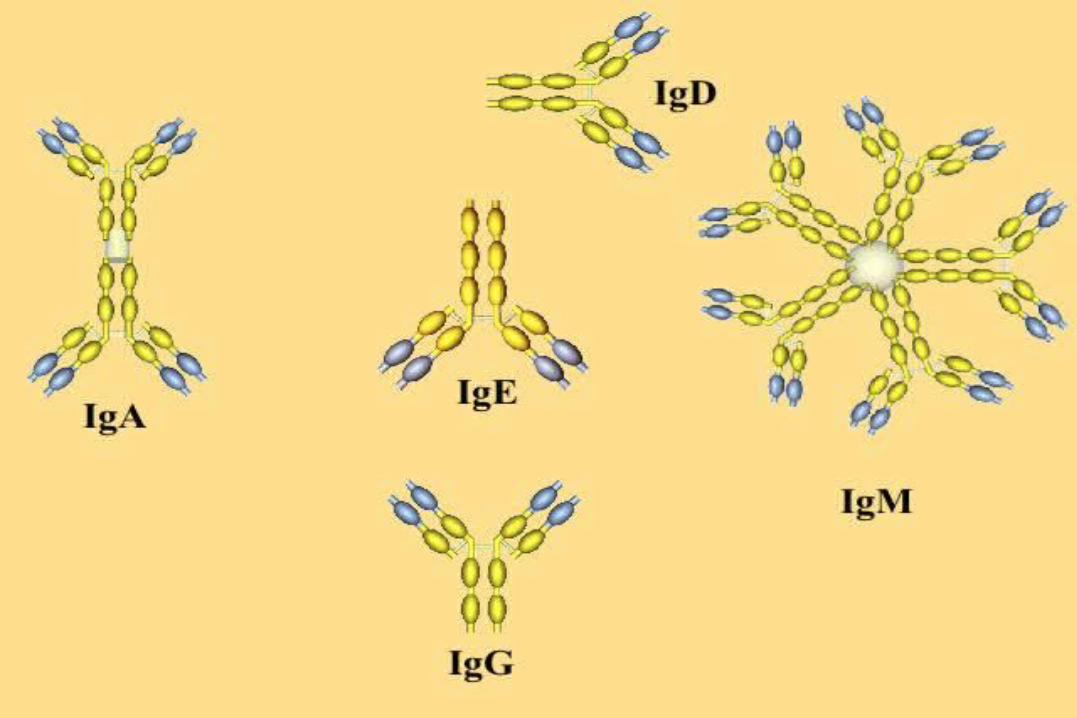

Biological functions of Biological functions of immunoglobulinsimmunoglobulins
ActActiivation of complement system (IgG, IgM)vation of complement system (IgG, IgM) Opsonization (namely IgG)Opsonization (namely IgG) Neuralization of antigens (IgG, IgA, IgM)Neuralization of antigens (IgG, IgA, IgM) Adesion interferenceAdesion interference (IgA, IgG) (IgA, IgG) Aglutination, precipittion (IgG, IgM)Aglutination, precipittion (IgG, IgM) Degranution of mast cells (IgEDegranution of mast cells (IgE Imunoregulation (namely IgG)Imunoregulation (namely IgG)
Clinical manifClinical manifesestation of tation of immunoglobulin immunoglobulin
defdefiiciencyciency FrequentFrequent and complicated infections of the and complicated infections of the
respiratory tract.respiratory tract. Patients suffer from recurrent attacks of Patients suffer from recurrent attacks of
bronchitis, sinusitis, pneumonia, otitis.bronchitis, sinusitis, pneumonia, otitis. Infections are caused namely by encapsulated Infections are caused namely by encapsulated
bacteria: bacteria: Heamohilus spHeamohilus sp., ., Str. pmeumoniaeStr. pmeumoniae, , St. St. aureus. aureus.
Typical complications are bronchiectasis Typical complications are bronchiectasis and/or lung fibrosisand/or lung fibrosis..
Patient No. 1 (born 1974)Patient No. 1 (born 1974)
Family History: negativeFamily History: negative 12 years12 years: skin rash, gradually disappeared : skin rash, gradually disappeared The patient never suffered from The patient never suffered from
frequent/severe infections.frequent/severe infections. 24 years24 years: delivered twins. Liver fu: delivered twins. Liver funnction ction
test were abnormal. Electrophoresis test were abnormal. Electrophoresis showed low gamma-fraction.showed low gamma-fraction.

Patient No. 1 (24 Patient No. 1 (24 years) -laboratory years) -laboratory
investigationsinvestigations IgG: 3.31 g/l (7-16)IgG: 3.31 g/l (7-16) IgA: <0.08 g/l IgA: <0.08 g/l IgM<0.08 g/lIgM<0.08 g/l anti-tetanic toxoid: 0.080 IU/ml (>0.120) after anti-tetanic toxoid: 0.080 IU/ml (>0.120) after
vaccination 0.158 IU/mlvaccination 0.158 IU/ml anti-HIB: 0.04 mg/l (0,09-17.7) anti-HIB: 0.04 mg/l (0,09-17.7) anti-PCP: 1.4 mg/l (>15.0)anti-PCP: 1.4 mg/l (>15.0) Isohemagglutinis anti-A, anti-B: titre 1:2Isohemagglutinis anti-A, anti-B: titre 1:2

Patient no I. (born 1974)Patient no I. (born 1974)
Aged 25: hypotAged 25: hypothhyreosis yreosis Decrease of IgG was documented (2.8 Decrease of IgG was documented (2.8
g/l), treatment by intramuscular g/l), treatment by intramuscular immunoglobulin 1.2 g/week was immunoglobulin 1.2 g/week was initiated.initiated.
Currently: 30 years, IgG: 3.0-3.5 g/l. Currently: 30 years, IgG: 3.0-3.5 g/l. She does not suffer from frequent She does not suffer from frequent infections.infections.

Patient No. 2 (born 1981)Patient No. 2 (born 1981)
Family history: negativeFamily history: negative Frequent respiratory tract infections from Frequent respiratory tract infections from
childhood, repeated schildhood, repeated sinuinusitis, 2x pneumonia, sitis, 2x pneumonia, 1313 years: tonsilyears: tonsilllectomy for chronic tonsillitis. ectomy for chronic tonsillitis. 13 year13 yearss: first immunological investigation:: first immunological investigation:
IgG: 3.7 g/l, IgA: 0.15 g/l, IgM: 1.04 g/l, Treatment IgG: 3.7 g/l, IgA: 0.15 g/l, IgM: 1.04 g/l, Treatment by IMIG was introduced, frequent infections by IMIG was introduced, frequent infections didissappeared (with the exappeared (with the excception of rhinitis) eption of rhinitis)
Patient No 2 – (aged 20) Patient No 2 – (aged 20)
IgG: 2.80 g/lIgG: 2.80 g/l IgA: 0.04g/lIgA: 0.04g/l IgM: 0.49 g/lIgM: 0.49 g/l anti-tet-tox: 0,111 IU/ml (>0.120), anti-tet-tox: 0,111 IU/ml (>0.120), anti-HIB: 0.16 mg/l (0.09-17.7)anti-HIB: 0.16 mg/l (0.09-17.7) anti-PCP: 12,1 mg/l (> 15.4)anti-PCP: 12,1 mg/l (> 15.4) Isohaemaglutinins: anti-A: 1:32, anti-B 1:16Isohaemaglutinins: anti-A: 1:32, anti-B 1:16 No frequent infections.No frequent infections. Treatment: IMIG 1.2 g IMIG/2 weeks.Treatment: IMIG 1.2 g IMIG/2 weeks.

Patient no. 2 (1981)Patient no. 2 (1981)
Aged 22 – spent 18 months in USA and Aged 22 – spent 18 months in USA and Japan, without any treatment. Japan, without any treatment.
She had no clinical problems, even her She had no clinical problems, even her chronic rhinchronic rhintitiis disappeared. is disappeared.
No abnormalitiesNo abnormalitiesees in HRCT an lung s in HRCT an lung function tests were observed.function tests were observed.
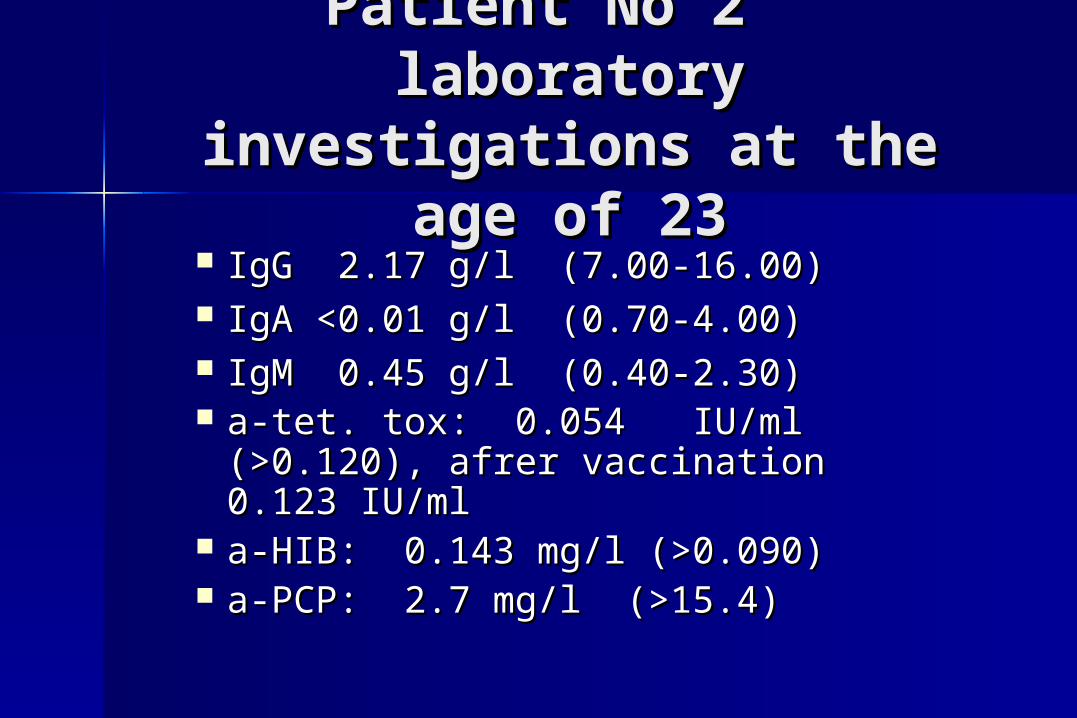
Patient No 2 Patient No 2 laboratory investigations laboratory investigations
at the age of 23at the age of 23 IgG 2.17 g/l (7.00-16.00) IgG 2.17 g/l (7.00-16.00) IgA <0.01 g/l (0.70-4.00) IgA <0.01 g/l (0.70-4.00) IgM 0.45 g/l (0.40-2.30) IgM 0.45 g/l (0.40-2.30) a-tet. tox: 0.054 IU/ml (>0.120), a-tet. tox: 0.054 IU/ml (>0.120),
afrer vaccination 0.123 IU/mlafrer vaccination 0.123 IU/ml a-HIB: 0.143 mg/l (>0.090) a-HIB: 0.143 mg/l (>0.090) a-PCP: 2.7 mg/l (>15.4)a-PCP: 2.7 mg/l (>15.4)
Patient No 3 (born Patient No 3 (born 1967)1967)
Family history: negativeFamily history: negative No frequent infections during childhood No frequent infections during childhood 21 years21 years: delivere: deliveredd a boy, pneumonia after a boy, pneumonia after
delivery.delivery. The next two pregnacies without complications.The next two pregnacies without complications. The patiThe patientent “did not visit a doctor because of “did not visit a doctor because of
infection during the last 10 years“.infection during the last 10 years“. 3636 year yearss: miscarriage at 11th week of : miscarriage at 11th week of
pregnancy.pregnancy.
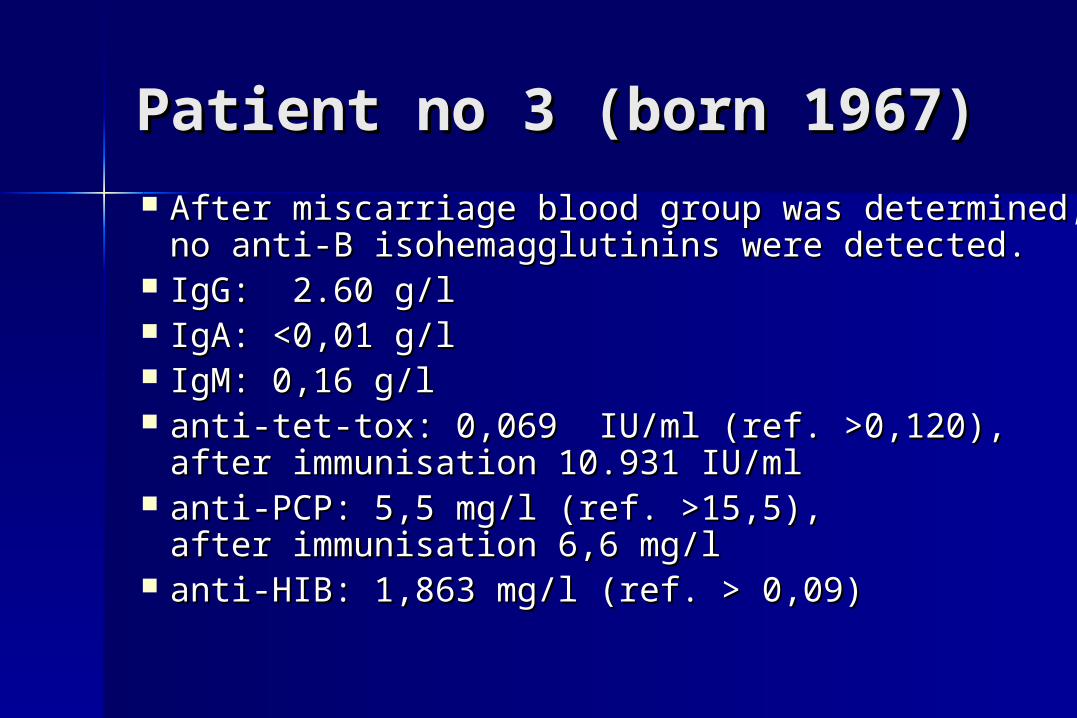
Patient no 3 (born 1967)Patient no 3 (born 1967) After miscarriage blood group was determined, After miscarriage blood group was determined,
no anti-B isohemagglutinins were detected. no anti-B isohemagglutinins were detected. IgG: 2.60 g/lIgG: 2.60 g/l IgA: <0,01 g/lIgA: <0,01 g/l IgM: 0,16 g/lIgM: 0,16 g/l anti-tet-tox: 0,069 IU/ml (ref. >0,120), anti-tet-tox: 0,069 IU/ml (ref. >0,120),
after immunisation 10.931 IU/mlafter immunisation 10.931 IU/ml anti-PCP: 5,5 mg/l (ref. >15,5), anti-PCP: 5,5 mg/l (ref. >15,5),
after immunisation 6,6 mg/lafter immunisation 6,6 mg/l anti-HIB: 1,863 mg/l (ref. > 0,09)anti-HIB: 1,863 mg/l (ref. > 0,09)

To treat or not to treat ?

Possible complications Possible complications inin untreated untreated hypogammaglobulinemic hypogammaglobulinemic patientspatients Life-threateniLife-threateninng pneumoniag pneumonia MeningitisMeningitis Irrevesible lung damage: fibrosis Irrevesible lung damage: fibrosis
and/or bronchiectasisand/or bronchiectasis Other severe infectionsOther severe infections

Patient with X-LAPatient with X-LA
Negative family historyNegative family history By 12 months no frequent or severe By 12 months no frequent or severe
infections.infections. At 12 months phlegAt 12 months phlegmmona of the left cheek.ona of the left cheek. At 18/12 otogenic At 18/12 otogenic meningitismeningitis with septicemia, with septicemia,
irirrreversible deafneversible deafneess.ss. First pneumonia at 2 years.First pneumonia at 2 years. Antromastoidectomy at 3 years Antromastoidectomy at 3 years Diagnosis of X-LA was made at 4 years. Diagnosis of X-LA was made at 4 years.
Patient with CVID Patient with CVID (born 1964)(born 1964)
No frequent infections during childhoodNo frequent infections during childhood Meningitis at 15 yearsMeningitis at 15 years 19 years: pneumonia, first immunological 19 years: pneumonia, first immunological
invesinvesttigation was performed: IgG: 1igation was performed: IgG: 1..72 72 g/lg/l, , IgA: 0IgA: 0..34 g/l34 g/l, , IgM: 0IgM: 0..11 g/l11 g/l
After initiation of immunoglobulin After initiation of immunoglobulin treament he dotreament he doees ns noot suffer from frequent t suffer from frequent infections but one pneumonia occurredinfections but one pneumonia occurred..
Patient with lung fibrosis Patient with lung fibrosis (born 1970) (born 1970)
Negative family historyNegative family history At 17 years „mild pneumonia“, but thAt 17 years „mild pneumonia“, but theen without n without
frequent infectionsfrequent infections Deliverd a baby at 29 years, afterwards Deliverd a baby at 29 years, afterwards
increased frequency of respiratory tract increased frequency of respiratory tract infections for approximately 9 months. infections for approximately 9 months.
At 30 years - dyspnoea, lung fibrosis was At 30 years - dyspnoea, lung fibrosis was diagnosed.diagnosed.
At 31 years: IgG: 2.13 g/l, IgA: 0.14 g/l, At 31 years: IgG: 2.13 g/l, IgA: 0.14 g/l, IgM:IgM: 0.28 g/l 0.28 g/l

Causes of immunological Causes of immunological investigation of new CVID investigation of new CVID
patients in 1983-2004patients in 1983-2004
Total: 55Total: 55 Pneumonia: 37Pneumonia: 37 Frequent mild respiratory tract Frequent mild respiratory tract
infections: 10infections: 10 Lung fibrosis: 3Lung fibrosis: 3 Other causes: 5Other causes: 5

Number of episodes of Number of episodes of pneumoniea before diagnosis pneumoniea before diagnosis
of CVID was made of CVID was made (Dept. Clin. Immunol. Brno)(Dept. Clin. Immunol. Brno)
0
5
10
15
20
25
30
1980 1985 1990 1995 2000
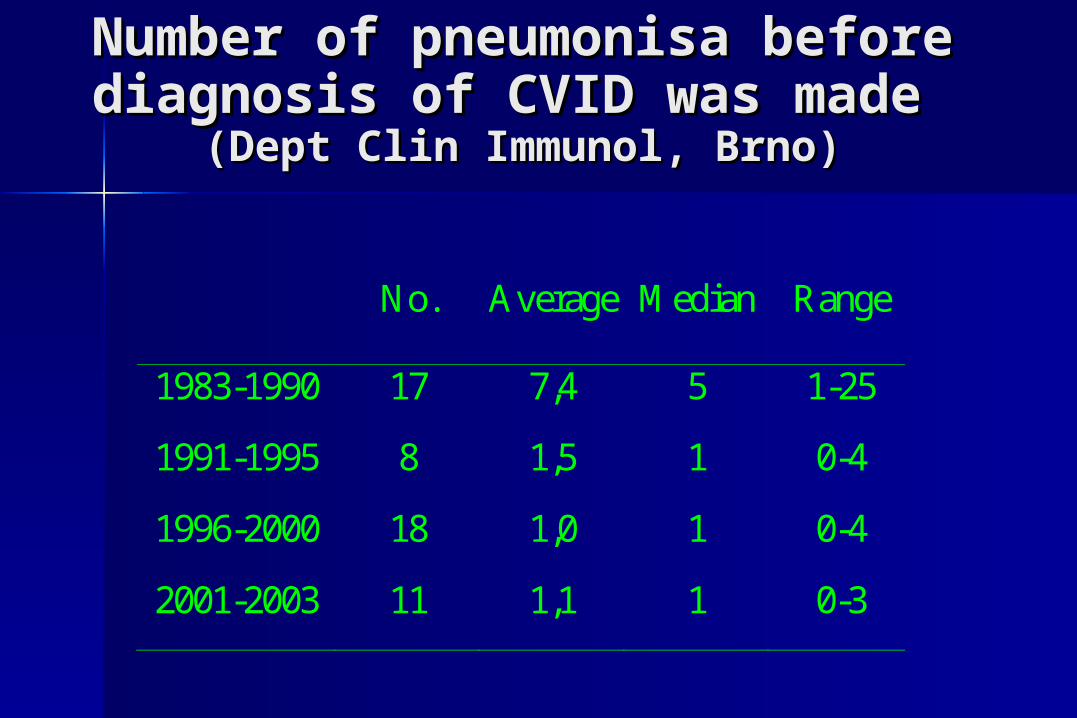
Number of pneumonisa before Number of pneumonisa before diagnosis of CVID was made diagnosis of CVID was made
(Dept Clin Immunol, Brno)(Dept Clin Immunol, Brno)
No. Average Median Range
1983-1990 17 7,4 5 1-25
1991-1995 8 1,5 1 0-4
1996-2000 18 1,0 1 0-4
2001-2003 11 1,1 1 0-3

Criteria for introduction IVIG Criteria for introduction IVIG treatmenttreatment
IgG <2,5 g/l: all patients IgG <2,5 g/l: all patients IgG 2,5-4 g/l: In patients with increased IgG 2,5-4 g/l: In patients with increased
susceptibility to infections.susceptibility to infections. IgG: 4-7 g/l: In patients with increased IgG: 4-7 g/l: In patients with increased
susceptibility to infections and antibody susceptibility to infections and antibody response defresponse defiiciency.ciency.
(Zielen S, In: Wahn V (ed): Klinischer Einsatz von Intravenösen Immunoglobulinen, Uni-Med Verlag AG, 2000.)