at the heart of it - fmf · at the heart of it: ... cv, cardiovascular; mi, myocardial infarction;...
TRANSCRIPT

An ancillary session at the 2017 Family Medicine Forum
At the Heart of It: A New Look at Clinical Cardiovascular Disease in Diabetes Thursday, November 9, 2017 | 06:45-07:45
Session ID no. 185941-109 After attending this session, participants will be able to:
Review and interpret the CDA recommendations, including the November 2016 updates, for vascular protection and diabetes management in patients with type 2 diabetes, with and without cardiovascular disease.
Summarize available cardiovascular outcome data and discuss their applicability in the primary care setting.
Compare and contrast among individual agents within the DPP-4 inhibitor, GLP-1 receptor agonist, and SGLT2 inhibitor classes.
This program has been certified by the College of Family Physicians of Canada and the Quebec office for up to 1.00 Group Learning credits.
This program was supported in part by an educational grant from Novo Nordisk Canada Inc.
Ting-Yu Wang, MDCM, FRCPC, MSc Community endocrinologist at Hôpital du Haut-Richelieu, Lakeshore General Hospital, and Montreal Chinese Hospital
Dr. Ting-Yu Wang received her Medicine and Endocrinology training, in addition to a Master’s in Epidemiology, at McGill University in Montreal, Quebec. Dr. Wang is a practising community endocrinologist at Hôpital du Haut-Richelieu (Saint-Jean-sur-Richelieu), Lakeshore General Hospital (Pointe-Claire), and Montreal Chinese Hospital (Montreal). Through these various practice locations, Dr. Wang provides care to multi-ethnic populations. Her primary clinical focus is in diabetes, with a special interest in the Chinese population.

1
At the Heart of It:
A New Look at Clinical Cardiovascular Disease (CVD) in Diabetes
Faculty/presenter disclosure
• Faculty: Ting-Yu Wang, MDCM, FRCPC, Msc
• Relationships with commercial interests:◦ Grants/Research Support: None◦ Speakers Bureau/Honoraria: Amgen, AstraZeneca, Eli Lilly/Boehringer-Ingelheim,
Janssen, Merck, Novo Nordisk, Sanofi-Aventis ◦ Consulting Fees: Amgen, AstraZeneca, Eli Lilly, Janssen, LifeScan, Merck, Novo
Nordisk, Sanofi-Aventis ◦ Other: None
Disclosure of commercial support
• This program has received financial support from Novo Nordisk Canada Inc. in the form of an educational grant
• This program has received in-kind support from Novo Nordisk Canada Inc. in the form of logistical support
• Potential for conflict(s) of interest:◦ Dr. Ting-Yu Wang has received funding or honoraria from Novo Nordisk Canada Inc.
AND/OR organization whose product(s) are being discussed in this program AstraZeneca Canada Inc.: saxagliptin, exenatide, dapagliflozin Boehringer Ingelheim (Canada) Ltd.: linagliptin, empagliflozin Eli Lilly Canada Inc.: dulaglutide Janssen Inc.: canagliflozin Merck Canada Inc.: sitagliptin sanofi-aventis Canada: lixisenatide†
◦ Novo Nordisk Canada Inc. developed products that will be discussed in this program: Liraglutide Semaglutide†
◦ Dr. Wang will receive an honorarium from the CFPC/FMF committee for this session
*Not available in Canada. †Not approved for use in Canada.

2
Mitigating potential bias
• Bias in this program has been mitigated using independent content validation as follows:◦ All content has been reviewed by a physician steering committee, pharmacist
expert reviewers, and the College of Family Physicians of Canada◦ All data has been sourced from evidence that is clinically accepted ◦ All support used in justification of patient care recommendations conform to
generally accepted standards and Canadian Diabetes Association 2013 clinical practice guidelines, and 2016 interim update, as well as the most recently available clinical data
Steering committee
• Sara Stafford, MDCM, FRCPC◦ Endocrinologist with the Fraser Health Division of Endocrinology◦ Clinical Instructor, UBC, Vancouver, BC
• Connie Ellis, MD, CCFP, FCFP◦ Specialist in family medicine from Alberta
• Jeffrey Habert, MD, CCFP, FCFP◦ Family physician◦ Assistant Professor, University of Toronto, Dept. of Family and Community Medicine
• Marie-Chantal Ménard, MD ◦ Family Physician at Centre Hygie, St-Jean-sur-Richelieu in Quebec
• Robert S. Roscoe, B.Sc.Pharm, ACPR, CDE, CPT◦ Pharmacist in New Brunswick
• Sally Zaky Sadek, Doctor of Pharmacy, CDE◦ Pharmacist in Ontario
Program objectives
After attending this program, participants will be able to:• Review and interpret the CDA recommendations, including the November
2016 updates, for vascular protection and diabetes management in patients with type 2 diabetes, with and without cardiovascular disease
• Summarize available cardiovascular outcome data and discuss their relevance in the primary care setting
• Compare and contrast among individual agents within the DPP-4 inhibitor, GLP-1 receptor agonist, and SGLT2 inhibitor classes
CDA, Canadian Diabetes Association; DPP-4, dipeptidyl peptidase 4; GLP-1, glucagon-like peptide 1; SGLT2, sodium glucose transporter 2.

3
ACR, albumin:creatinine ratio; FRS, Framingham Risk Score=Estimation of 10-year cardiovascular disease risk; G1P1, gravidity (number of times female is or has been pregnant), parity (number of times female has carried the pregnancies to a viable gestational age).
Meet LouisePersonal history
• 63 years old• City planner with private coverage• Indicates she is working on being more
active and will further improve her diet and activity levels
Assessments
• A1C 8.3%• BMI 32.2 kg/m2
• LDL 1.9 mmol/L• HDL 1.2 mmol/L• BP 136/78 mmHg• eGFR 72 mL/min/1.73 m2
• Urine ACR 1.4 mg/mmol
Medical history
• Diagnosed with diabetes 6 years ago• G1P1: Experienced mild preeclampsia at
the end of her pregnancy with her son• Post menopausal• Family history of coronary heart disease• Diagnosed with hypertension 8 years ago• FRS high
Medications
• Rosuvastatin 20 mg • Perindopril 8 mg • Metformin 1 g bid
Public Health Agency of Canada. Diabetes in Canada: Facts and figures from a public health perspective. Ottawa. 2011; American Heart Association. Cardiovascular Disease & Diabetes. 2016. Available at: http://www.heart.org/HEARTORG/Conditions/Diabetes/WhyDiabetesMatters/Cardiovascular-Disease-Diabetes_UCM_313865_Article.jsp.
Diabetes and cardiovascular disease are intertwined
Diabetes Cardiovascular disease
• Most common condition reported in Canadians with diabetes • Most common cause of death in individuals with type 2 diabetes
Type 2 diabetes is associated with an increased incidence of CVDIn a cohort of nearly 2 million people, there was a:
in people with type 2 diabetes compared to the general population
Unheralded coronary death=coronary death that was not previously expected/recognized.Shah AD. Lancet Diabetes Endocrinol. 2015;3:105–113.
62%increase in
Stable angina Unstable angina Nonfatal MI
Unheralded coronary death
Heart failure Ischemic stroke
53%increase in
54%increase in
43%increase in
56%increase in
72%increase in

4
MI at a younger age among those with diabetes
20-30 31-40 41-45 46-50 51-55 56-60 61-65 66-70 71-75 76-80 81-85
MI, myocardial infarctionBooth GL et al. Lancet. 2006;368:29–36.
Age group
0.5
1.0
1.5
2.0
2.5
3.0
0
No
. ev
ents
per
10
0 p
erso
n-y
ears
All lines fitted according to a polynomial equation; R2= 0.99–1.00 for each.
Diabetes n = 379,003 No diabetes n = 9,018,082 Database 1994-2000
No diabetesMen
Women
DiabetesMenWomen
No diabetesDiabetesMenWomen
Conventional arm Intensive arm
MD follows clinical practice guidelines
Therapies to achieve targets in glycemia, lipids, BP and microalbuminuriaMultidisciplinary care q3moASA and ACE inhibitors(independent of BP)
BP, blood pressure; CABG, coronary artery bypass grafting; CV, cardiovascular; MI, myocardial infarction; PCI, percutaneous coronary intervention; PVD, peripheral vascular disease. Gaede P et al. N Engl J Med. 2003;348:383–393.
What are the benefits of multifactorial interventions to achieve targets with respect to CV protection?
Type 2 diabetes + Microalbuminuria
n = 160
8-year follow-up composite outcome:CV death, MI, CABG, PCI, stroke,
amputation, or PVD surgery
Intensive group achieved targets
STENO 2
<4.5 mmol/L <1.7 mmol/L
• After 7.8 years, intensive therapy reduced:◦ CVD by 53%◦ Nephropathy by 61%◦ Retinopathy by 48% ◦ Autonomic neuropathy by 63%
Legacy effect observed: • 21.2 years after intervention start,
intensive therapy had reduced: ◦ CVD by 51%◦ Mortality by 45%◦ Retinopathy by 33%◦ Nephropathy by 48%
• Median time before first CV event was 8.1 years longer in the intensive group
Gaede P et al. N Engl J Med. 2003;348:383–393; Gaede P et al. Diabetologia. 2016;59:2298–2307.
What are the benefits of multifactorial interventions to achieve targets with respect to CV protection?
STENO 2 after 7.8 years

5
CDA recommendations: Multifaceted Strategy: Vascular Protection Checklist
A • A1C – optimal glycemic control (usually ≤7%) B • BP – optimal blood pressure control (<130/80 mmHg) C • Cholesterol – LDL ≤2.0 mmol/L if decided to treat D • Drugs to protect the heart (regardless of baseline BP or LDL)
A – ACEi or ARB │ S – Statin │ A – ASA if indicated
E • Exercise / Eating healthily – regular physical activity, achieve andmaintain healthy body weight
S • Smoking cessation
ACEi, angiotensin-converting-enzyme inhibitor; ARB, angiotensin II receptor blockers; ASA, acetylsalicylic acid; BP, blood pressure; LDL, low density lipoprotein.Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. Canadian Diabetes Association. 2013 Clinical practice guidelines for the prevention and management of diabetes in Canada. Can J Diabetes. 2013;37(suppl 1):S1–S212.
Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. Canadian Diabetes Association. Can J Diabetes. 2016;40:484–486.
What’s new? CDA recommendations: Type 2 diabetes management algorithm
NEW!
What’s new? CDA recommendations: Type 2 diabetes management algorithm
Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. Canadian Diabetes Association. Can J Diabetes. 2016;40:484–486.
NEW!(Mar 2016)
NEW!(Nov 2016)

6
ACR, albumin:creatinine ratio; FRS, Framingham Risk Score=Estimation of 10-year cardiovascular disease risk; G1P1, gravidity (number of times female is or has been pregnant), parity (number of times female has carried the pregnancies to a viable gestational age).
Let’s take another look at LouisePersonal history
• 63 years old• City planner with private coverage• Indicates she is working on being more
active and will further improve her diet and activity levels
Assessments
• A1C 8.3%• BMI 32.2 kg/m2
• LDL 1.9 mmol/L• HDL 1.2 mmol/L• BP 136/78 mmHg• eGFR 72 mL/min/1.73 m2
• Urine ACR 1.4 mg/mmol
Medical history
• Diagnosed with diabetes 6 years ago• G1P1: Experienced mild preeclampsia at
the end of her pregnancy with her son• Post menopausal• Family history of coronary heart disease• Diagnosed with hypertension 8 years ago• FRS high
Medications
• Rosuvastatin 20 mg • Perindopril 8 mg • Metformin 1 g bid
What would you prescribe for Louise?
An agent with proven CVD benefit should be considered for Louise based on her characteristics
a. Trueb. False
Based on patient population of EMPA-REG (empagliflozin)• Adults with type 2 diabetes• A1C 7–10% for treated subjects• A1C 7–9% for drug-naïve subjects• BMI ≤45 kg/m2
• Established cardiovascular disease (CVD):◦ Prior myocardial infarction◦ Coronary artery disease ◦ Unstable angina◦ Prior stroke◦ Occlusive peripheral
arterial disease
Zinman B et al. Cardiovascular Diabetology. 2014;13:102
Defining “Clinical Cardiovascular Disease”

7
Patient population of LEADER (liraglutide)• Adults with type 2 diabetes• A1C ≥7.0% (no upper limit)• Drug-naïve or treated with
≥1 OAD or insulin ± OADs • Any BMI • Age ≥50 years and established
CVD or chronic renal failureor
• Age ≥60 years and risk factors for CV disease
LEADER, Liraglutide Effect and Action in Diabetes: Evaluation of cardiovascular outcome Results Marso S et al. Am Heart J. 2013;166:823-830.e5.
Defining “Clinical Cardiovascular Disease”
ACR, albumin:creatinine ratio; FRS, Framingham Risk Score=Estimation of 10-year cardiovascular disease risk; G1P1, gravidity (number of times female is or has been pregnant), parity (number of times female has carried the pregnancies to a viable gestational age).
Meet LouisePersonal history
• 63 years old• City planner with private coverage• Indicates she is working on being more
active and will further improve her diet and activity levels
Assessments
• A1C 8.3%• BMI 32.2 kg/m2
• LDL 1.9 mmol/L• HDL 1.2 mmol/L• BP 136/78 mmHg• eGFR 72 mL/min/1.73 m2
• Urine ACR 1.4 mg/mmol
Medical history
• Diagnosed with diabetes 6 years ago• G1P1: Experienced mild preeclampsia at
the end of her pregnancy with her son• Post menopausal• Family history of coronary heart disease• Diagnosed with hypertension 8 years ago• FRS high
Louise does not have CVD, but is at increased risk. Choose a second-line agent individualized to her characteristics (e.g., A1C reduction >1%, weight loss/neutrality, LDL decrease/neutral, CV risk factors, etc.).
Medications• Rosuvastatin 20 mg • Perindopril 8 mg • Metformin 1 g bid
ACR, albumin:creatinine ratio; FRS, Framingham Risk Score=Estimation of 10-year cardiovascular disease risk; G1P1, gravidity (number of times female is or has been pregnant), parity (number of times female has carried the pregnancies to a viable gestational age).
What if Louise had CVD?Personal history
• 63 years old• City planner with private coverage• Indicates she is working on being more
active and will further improve her diet and activity levels
Assessments
• A1C 8.3%• BMI 32.2 kg/m2
• LDL 1.9 mmol/L• HDL 1.2 mmol/L• BP 136/78 mmHg• eGFR 72 mL/min/1.73 m2
• Urine ACR 1.4 mg/mmolMedical history
• Diagnosed with diabetes 6 years ago• G1P1: Experienced mild preeclampsia at
the end of her pregnancy with her son• Post menopausal• Family history of coronary heart disease• Diagnosed with hypertension 8 years ago• FRS high• Prior MI with stent x2 (2 years ago)
Medications
• Rosuvastatin 20 mg • Perindopril 8 mg • Aspirin 81 mg• Metformin 1 g bid
What should I know before prescribing a product for Louise if she has cardiovascular disease?
1. What is a cardiovascular outcome trial? 2. What if I prescribe a DPP-4 inhibitor?3. What if I prescribe a GLP-1 receptor agonist?4. What if I prescribe an SGLT2 inhibitor?

8
• In 2008, the US Food and Drug Administration (FDA) issued guidance requiring robust assessment of cardiovascular safety forall antihyperglycemictherapies to be licensed in the future
What is a cardiovascular outcome trial?
FDA Guidance for Industry: Diabetes Mellitus; Evaluating CV risk in new antidiabetic therapies to treat type 2 diabetes. www.fda.gov; Hirshberg & Raz. Diabetes Care 2011;34(Suppl.2):S101–6.
Aim: To demonstrate no increased CV risk vs. placebo (as part of standard of
care, SOC)
Initiation of blinded treatment or placebo (+ SOC)
Minimal/no difference in A1C between groups
No increased CV risk (safety) of treatment demonstrated by non-inferiority
(typically of MACE)
• In 2008, the US Food and Drug Administration (FDA) issued guidance requiring robust assessment of cardiovascular safety forall antihyperglycemictherapies to be licensed in the future
What is a cardiovascular outcome trial?
FDA Guidance for Industry: Diabetes Mellitus; Evaluating CV risk in new antidiabetic therapies to treat type 2 diabetes. www.fda.gov; Hirshberg & Raz. Diabetes Care. 2011;34(Suppl.2):S101–6.
Aim: To demonstrate no increased CV risk vs. placebo (as part of standard of
care, SOC)
Initiation of blinded treatment or placebo (+ SOC)
Minimal/no difference in A1C between groups
No increased CV risk (safety) of treatment demonstrated by non-inferiority
(typically of MACE)
What is “standard of care”?Blood glucose• HbA1c ≤7.0% (individualized depending on patient [pt]).• If >7.0%, additional HbA1c measurement after 3 m. If HbA1c
still >7.0%, treatment should be intensified to achieve target if appropriate
Blood pressure• Target: 130/80 mmHg
Antihypertensive therapy • First line: ACEi or ARBs• Based on individual pt needs: Ca2+-blockers, diuretics, others
Lipid targets and therapy • LDL <2.0 mmol/L• Statins recommended for all pts• Second line therapy at investigators discretion
Antiplatelet therapy • Aspirin or clopidogrel (if aspirin intolerant) for pts with prior CV
events (MI, cerebrovascular accident, or revascularization)
• In 2008, the US Food and Drug Administration (FDA) issued guidance requiring robust assessment of cardiovascular safety forall antihyperglycemictherapies to be licensed in the future
What is a cardiovascular outcome trial?
FDA Guidance for Industry: Diabetes Mellitus; Evaluating CV risk in new antidiabetic therapies to treat type 2 diabetes. www.fda.gov; Hirshberg & Raz. Diabetes Care. 2011;34(Suppl.2):S101–6.
Aim: To demonstrate no increased CV risk vs. placebo (as part of standard of
care, SOC)
Initiation of blinded treatment or placebo (+ SOC)
Minimal/no difference in A1C between groups
No increased CV risk (safety) of treatment demonstrated by non-inferiority
(typically of MACE)
Why minimize the difference in A1C?
• CV studies aim to achieve similar glucose control (glycemic equipoise) between treatment groups
• This helps minimize any potential effect that differences in glucose control might have on CV outcomes

9
• In 2008, the US Food and Drug Administration (FDA) issued guidance requiring robust assessment of cardiovascular safety forall antihyperglycemictherapies to be licensed in the future
What is a cardiovascular outcome trial?
FDA Guidance for Industry: Diabetes Mellitus; Evaluating CV risk in new antidiabetic therapies to treat type 2 diabetes. www.fda.gov; Hirshberg & Raz. Diabetes Care.2011;34(Suppl.2):S101–6.
Aim: To demonstrate no increased CV risk vs. placebo (as part of standard of
care, SOC)
Initiation of blinded treatment or placebo (+ SOC)
Minimal/no difference in A1C between groups
No increased CV risk (safety) of treatment demonstrated by non-inferiority
(typically of MACE)
Major AdverseCardiovascular Events
(MACE)
Composite of all major CV events:• CV death• Non-fatal myocardial
infarction • Non-fatal stroke
MACE is the primary endpoint for the majority of studies
ACR, albumin:creatinine ratio; FRS, Framingham Risk Score=Estimation of 10-year cardiovascular disease risk; G1P1, gravidity (number of times female is or has been pregnant), parity (number of times female has carried the pregnancies to a viable gestational age).
What if Louise had CVD?Personal history
• 63 years old• City planner with private coverage• Indicates she is working on being more
active and will further improve her diet and activity levels
Assessments
• A1C 8.3%• BMI 32.2 kg/m2
• LDL 1.9 mmol/L• HDL 1.2 mmol/L• BP 136/78 mmHg• eGFR 72 mL/min/1.73 m2
• Urine ACR 1.4 mg/mmolMedical history
• Diagnosed with diabetes 6 years ago• G1P1: Experienced mild preeclampsia at
the end of her pregnancy with her son• Post menopausal• Family history of coronary heart disease• Diagnosed with hypertension 8 years ago• FRS high• Prior MI with stent x2 (2 years ago)
Medications
• Rosuvastatin 20 mg • Perindopril 8 mg • Aspirin 81 mg• Metformin 1 g bid
What should I know before prescribing a product for Louise if she has cardiovascular disease?
1. What is a cardiovascular outcome trial? 2. What if I prescribe a DPP-4 inhibitor?3. What if I prescribe a GLP-1 receptor agonist?4. What if I prescribe an SGLT2 inhibitor?
DPP-4 inhibitors: How do they compare?
Sitagliptin Saxagliptin Linagliptin Alogliptin
A1C Reduction of ~0.5–0.8%
Weight Weight neutral
Hypoglycemia Low risk of hypoglycemia
CV effects Neutral MACENeutral hHF
Neutral MACEIncreased hHF
n/a Neutral MACENeutral hHF
hHF, hospitalization for heart failure.Januvia® (sitagliptin) Product Monograph. Merck Canada, 2016; Onglyza® (saxagliptin) Product Monograph. AstraZeneca Canada Inc., 2016; Trajenta® (linagliptin) Product Monograph. Boehringer Ingelheim (Canada) Ltd., 2015; Charbonnel B et al. Diabetes Care. 2006;29:2638–43; DeFronzo RA et al. Diabetes Care. 2009;32:1649–55; Taskinen MR et al. Diabetes Obes Metab. 2011;13:65–74; Scirica BM et al. N Engl J Med. 2013;369:1317–26; Zannad F et al. Lancet. 2015;385:2067–76; Green JB et al. N Engl J Med. 2015;373:232–242.
Note: Data are from separate studies; head-to-head data not available in product monographs

10
DPP-4 inhibitors: How do they compare?CVOT – MACE
Study drugn/N (%)
Placebon/N (%)
Hazard ratio 95% CI P value
SAVOR-TIMI(saxagliptin vs.
placebo)
613/8,280(7.4%)
609/8,212(7.4%) 1.00 0.89, 1.12 0.99
EXAMINE(alogliptin vs.
placebo)
305/2,701(11.3%)
316/2,679(11.8%) 0.96 N/A*, 1.16 0.315
TECOS(sitagliptin vs.
placebo)
745/7,332(10.2%)
746/7,339(10.2%) 0.99 0.89, 1.10 0.844
SAVOR + EXAMINE +
TECOS
1,663/18,313(9.1%)
1,671/18,230(9.2%) 0.99 0.92, 1.06
CI, confidence interval; I2, a statistic that indicates the percentage of variance in a meta-analysis that is attributable to study heterogeneity.Peterson ED. American Diabetes Association, 75th Scientific Sessions, June 5–9, 2015, Boston, MA; Scirica BM et al. N Engl J Med. 2013;369:1317–26; Zannad F et al. Lancet. 2015;385:2067–76; Green JB et al. N Engl J Med. 2015;373:232–242.
Favours treatment Favours placebo
0 1 2
DPP-4 inhibitors have demonstrated CV safety, as defined by MACE
Separate studies, not direct comparisonsHeterogeneity test for three trials: p=0.877, I2=0%
DPP-4 inhibitors: How do they compare?CVOT – hospitalization for heart failure (hHF)
Study drugn/N (%)
Placebon/N (%)
Hazard ratio 95% CI P value
SAVOR-TIMI(saxagliptin vs.
placebo)
289/8,280(3.5%)
228/8,212(2.8%) 1.27 1.07, 1.51 0.007
EXAMINE(alogliptin vs.
placebo)
106/2,701(3.9%)
89/2,679(3.3%) 1.19 0.90, 1.58 0.220
TECOS(sitagliptin vs.
placebo)
228/7,332(3.1%)
229/7,339(3.1%) 1.00 0.83, 1.20 0.983
SAVOR + EXAMINE +
TECOS
623/18,313(3.4%)
546/18,230(3.0%) 1.14 0.97, 1.34
CI, confidence interval; I2, a statistic that indicates the percentage of variance in a meta-analysis that is attributable to study heterogeneity.Peterson ED. American Diabetes Association, 75th Scientific Sessions, June 5–9, 2015, Boston, MA; Scirica BM et al. N Engl J Med. 2013;369:1317–26; Zannad F et al. Lancet. 2015;385:2067–76; Green JB et al. N Engl J Med. 2015;373:232–242.
0 1 2Separate studies, not direct comparisonsHeterogeneity test for three trials: p=0.178, I2=42% Favours
treatmentFavoursplacebo
DPP-4 inhibitors: How do they compare?CVOT – hospitalization for heart failure (hHF)
Study drugn/N (%)
Placebon/N (%)
Hazard ratio 95% CI P value
SAVOR-TIMI(saxagliptin vs.
placebo)
289/8,280(3.5%)
228/8,212(2.8%) 1.27 1.07, 1.51 0.007
EXAMINE(alogliptin vs.
placebo)
106/2,701(3.9%)
89/2,679(3.3%) 1.19 0.90, 1.58 0.220
TECOS(sitagliptin vs.
placebo)
228/7,332(3.1%)
229/7,339(3.1%) 1.00 0.83, 1.20 0.983
SAVOR + EXAMINE +
TECOS
623/18,313(3.4%)
546/18,230(3.0%) 1.14 0.97, 1.34
CI, confidence interval; I2, a statistic that indicates the percentage of variance in a meta-analysis that is attributable to study heterogeneity.Peterson ED. American Diabetes Association, 75th Scientific Sessions, June 5–9, 2015, Boston, MA; Scirica BM et al. N Engl J Med. 2013;369:1317–26; Zannad F et al. Lancet. 2015;385:2067–76; Green JB et al. N Engl J Med. 2015;373:232–242.
Favours treatment
Favoursplacebo
0 1 2Separate studies, not direct comparisonsHeterogeneity test for three trials: p=0.178, I2=42%
Class effect unknown, but unlikely
2016 label updates:SAVOR-TIMI (saxagliptin): increased hHF risk observed• Included in both FDA and Health Canada labels
EXAMINE (alogliptin): trend for increased hHF risk• Included in FDA, but not Health Canada label

11
ACR, albumin:creatinine ratio; FRS, Framingham Risk Score=Estimation of 10-year cardiovascular disease risk; G1P1, gravidity (number of times female is or has been pregnant), parity (number of times female has carried the pregnancies to a viable gestational age).
What if Louise had CVD?Personal history
• 63 years old• City planner with private coverage• Indicates she is working on being more
active and will further improve her diet and activity levels
Assessments
• A1C 8.3%• BMI 32.2 kg/m2
• LDL 1.9 mmol/L• HDL 1.2 mmol/L• BP 136/78 mmHg• eGFR 72 mL/min/1.73 m2
• Urine ACR 1.4 mg/mmolMedical history
• Diagnosed with diabetes 6 years ago• G1P1: Experienced mild preeclampsia at
the end of her pregnancy with her son• Post menopausal• Family history of coronary heart disease• Diagnosed with hypertension 8 years ago• FRS high• Prior MI with stent x2 (2 years ago)
Medications
• Rosuvastatin 20 mg • Perindopril 8 mg • Aspirin 81 mg• Metformin 1 g bid
What should I know before prescribing a product for Louise if she has cardiovascular disease?
1. What is a cardiovascular outcome trial? 2. What if I prescribe a DPP-4 inhibitor?3. What if I prescribe a GLP-1 receptor agonist?4. What if I prescribe an SGLT2 inhibitor?
Available* GLP-1 receptor agonists: How do they compare?
Liraglutide Dulaglutide Exenatide BID Exenatide QW
A1C Reduction of ~1.0–1.5%
Non-inferior to liraglutide
Not non-inferior to liraglutide
Not non-inferior to liraglutide
Weight Weight loss of ~2–4 kg
Not non-inferiorto liraglutide
Not non-inferiorto liraglutide
Not non-inferiorto liraglutide
Hypoglycemia Low risk of hypoglycemia
CV effects • MACE benefit• Neutral hHF
n/a n/a • Neutral MACE• Neutral hHF
Dosing 1.2–1.8 mg QD 0.75–1.5 mg QW 5–10 μg BID 2 mg QW
*Albiglutide and lixisenatide are approved but not available and therefore excluded from this slide. As they are not approved in Canada, the following are excluded: ICTA 650 and semaglutide. AWARD-6: Dungan et al. Lancet. 2014;384(9951):1349–57; HARMONY-7: Pratley et al. Lancet Diabetes Endocrinol. 2014;2(4):289–97; DURATION-6: Buse et al. Lancet.2013;381(9861):117–24; LEAD-6: Buse et al. Lancet. 2009;374(9683):39–47; Marso SP et al. NEJM. 2016;375:311–322; Holman RR et al. NEJM. 2017 [Epub ahead of print].
Note: Data are from separate, but head-to-head studies
GLP-1 receptor agonists: LiraglutideCVOT – MACE
The cumulative incidences were estimated with the use of the Kaplan–Meier method, and the hazard ratios with the use of the Cox proportional-hazard regression model. The data analyses are truncated at 54 months, because less than 10% of the patients had an observation time beyond 54 months.CI, confidence interval; CV, cardiovascular; HR, hazard ratio; MI, myocardial infarction.Marso SP et al. NEJM. 2016;375:311–322.
HR 0.87(95% CI 0.78;0.97)
p=0.01
3-point MACETime-to-event analysis of first occurrence of CV death, non-fatal MI, or non-fatal stroke
HR(95% CI) P value
3-Point MACE(1° endpoint)
0.87(0.78;0.97) 0.01
CV death 0.78(0.66;0.93) 0.007
Non-fatal MI 0.88(0.75;1.03) 0.11
Non-fatal stroke 0.89(0.72;1.11) 0.30
Favours treatment
Favoursplacebo
Number of patients at risk
Liraglutide 4668 4593 4496 4400 4280 4172 4072 3982 1562 424
Placebo 4672 4588 4473 4352 4237 4123 4010 3914 1543 407

12
GLP-1 receptor agonists: LiraglutideCVOT – MACE
The cumulative incidences were estimated with the use of the Kaplan–Meier method, and the hazard ratios with the use of the Cox proportional-hazard regression model. The data analyses are truncated at 54 months, because less than 10% of the patients had an observation time beyond 54 months.CI, confidence interval; CV, cardiovascular; HR, hazard ratio; MI, myocardial infarction.Marso SP et al. NEJM. 2016;375:311–322.
HR 0.87(95% CI 0.78;0.97)
p=0.01
3-point MACETime-to-event analysis of first occurrence of CV death, non-fatal MI, or non-fatal stroke
HR(95% CI) P value
3-Point MACE(1° endpoint)
0.87(0.78;0.97) 0.01
CV death 0.78(0.66;0.93) 0.007
Non-fatal MI 0.88(0.75;1.03) 0.11
Non-fatal stroke 0.89(0.72;1.11) 0.30
Favours treatment
Favoursplacebo
Number of patients at risk
Liraglutide 4668 4593 4496 4400 4280 4172 4072 3982 1562 424
Placebo 4672 4588 4473 4352 4237 4123 4010 3914 1543 407
Reminder: 81.3% had prior CVD and 18.7%
were high risk, but without CVD
Benefit is on top of standard of care:• 92.3% on antihypertensives (some
patients on multiple agents) • 55.4% BB• 51% ACEi• 31.8% ARBs• 32% CCB
• 72% on statins• 62.9% on ASA• 15.7% on other antiplatelet agent
The cumulative incidences were estimated with the use of the Kaplan–Meier method, and the hazard ratios with the use of the Cox proportional-hazard regression model. The data analyses are truncated at 54 months, because less than 10% of the patients had an observation time beyond 54 months. CI, confidence interval; CV, cardiovascular; HR, hazard ratio.Marso SP et al. N Engl J Med. 2016;375:311–22.
GLP-1 receptor agonists: LiraglutideCVOT – CV death
HR 0.78(95% CI 0.66;0.93)
p=0.007
Number of patients at risk
Liraglutide 4668 4641 4599 4558 4505 4445 4382 4322 1723 484
Placebo 4672 4648 4601 4546 4479 4407 4338 4267 1709 465
Myocardial infarction Stroke
Hazard ratios and P values were estimated with the use of a Cox proportional-hazards model with treatment as a covariate. *This analysis was not prespecified.CI, confidence interval; HR, hazard ratio; MI, myocardial infarction.Marso SP et al. N Engl J Med. 2016;375:311–22.
GLP-1 receptor agonists: LiraglutideCVOT – MI and stroke
HR(95% CI) P value
Stroke* 0.86(0.71;1.06) 0.16
Fatal stroke* 0.64(0.34;1.19) 0.16
Non-fatal stroke 0.89(0.72;1.11) 0.30
Favours treatment
Favoursplacebo
HR(95% CI) P value
Total MI* 0.86(0.73;1.00) 0.046
Fatal MI* 0.60(0.33;1.10) 0.10
Non-fatal MI 0.88(0.75;1.03) 0.11
Silent MI* 0.86(0.61;1.20) 0.37
Favours treatment
Favoursplacebo

13
The cumulative incidences were estimated with the use of the Kaplan–Meier method, and the hazard ratios with the use of the Cox proportional-hazard regression model. The data analyses are truncated at 54 months, because less than 10% of the patients had an observation time beyond 54 months. CI, confidence interval; CV, cardiovascular; HR, hazard ratio.Marso SP et al. N Engl J Med. 2016;375:311–22.
GLP-1 receptor agonists: LiraglutideCVOT – hHF
HR 0.87(95% CI 0.73;1.05)
p=0.14
Number of patients at risk
Liraglutide 4668 4612 4550 4483 4414 4337 4258 4185 1662 467
Placebo 4672 4612 4540 4464 4372 4288 4187 4107 1647 442
Are the positive CVOT results observed for liraglutide a class effect for GLP-1 receptor agonists?
GLP-1 receptor agonists: Semaglutide*CVOT – MACE
*Semaglutide is an investigational drug and not approved for use in Canada.Kaplan–Meier plot for first event adjudication committee-confirmed CV death, non-fatal MI and non-fatal stroke using ‘in-trial’ data from subjects in the full analysis set. CI, confidence interval; CV, cardiovascular; HR, hazard ratio; MI, myocardial infarction. Marso SP et al. NEJM. 2016;375:1834–1844.
3-point MACETime-to-event analysis of first occurrence of CV death, non-fatal MI, or non-fatal stroke
HR(95% CI) P value
3-Point MACE(1° endpoint)
0.74(0.58;0.95) 0.02
CV death 0.98(0.65;1.48) 0.92
Non-fatal MI 0.74(0.51;1.08) 0.12
Non-fatal stroke 0.61(0.38;0.99) 0.04
Favours treatment
Favoursplacebo
HR 0.74(95% CI 0.58;0.95)
p=0.02 for superiority
Semaglutide, 6.6%
Placebo, 8.9%
Sema 1649 1616 1586 1567 1534 1508 1479
Placebo 1648 1619 1601 1584 1568 1543 1524

14
GLP-1 receptor agonists: LixisenatideCVOT – 4-point MACE
Lixisenatide is not available for use in Canada.CI, confidence interval; CV, cardiovascular; HR, hazard ratio; MACE, major cardiovascular adverse event; MI, myocardial infarction.Pfeffer MA et al. N Engl J Med 2015;373:2247–2257.
4-point MACETime-to-event analysis of first occurrence of
CV death, non-fatal MI, non-fatal stroke, or unstable angina
HR(95% CI) P value
4-Point MACE(1° endpoint)
1.02 (0.89;1.17) 0.81
CV death 0.98 (0.78;1.22) 0.85
Non-fatal MI 1.03 (0.87;1.22) 0.71
Non-fatal stroke 1.12 (0.79;1.58) 0.54
Unstable angina 1.11 (0.47;2.62) 0.81
Favours treatment
Favoursplacebo
0.00 0.50 1.00 1.50 2.00 2.50 3.00
Lixisenatide 3034 2759 1566 476
Placebo 3034 2785 1558 484
HR 1.02(95% CI 0.89;1.17)
p=0.81
GLP-1 receptor agonists: ExenatideCVOT – MACE
CI, confidence interval; CV, cardiovascular; HR, hazard ratio; MI, myocardial infarction. Holman RR et al. NEJM. 2017 [Epub ahead of print].
3-point MACETime-to-event analysis of first occurrence of CV death, non-fatal MI, or non-fatal stroke
HR(95% CI) P value
3-Point MACE(1° endpoint)
0.91(0.83;1.00) 0.061
CV death 0.88(0.73;1.05)
0.628 (homogeneity
among components)
Non-fatal MI 0.95(0.84;1.09)
Non-fatal stroke 0.86(0.70;1.07)
Favours treatment
Favoursplacebo
0
5
10
15
20
0 1 2 3 4 5
Subjects with an event (%)
Time since randomization (years)
HR 0.91(95% CI 0.83;1.00)
p=0.061 for superiority
Exen 7356 6893 5912 3595 2281 727
Placebo 7396 6897 5908 3565 2209 687
Exenatide, 11.4%
Placebo, 12.2%
0 0.5 1 1.5 2
Positive for MACE• Liraglutide (LEADER)1
◦ Results previously shown• Semaglutide* (SUSTAIN 6)2
◦ Results previously shown
Neutral for MACE• ITCA 650 exenatide* (FREEDOM-CVO)3
◦ Completed, no results available• Lixisenatide† (ELIXA)4
◦ Results previously shown• Exenatide QW (EXSCEL)5
◦ Results previously shown
*Not approved for use in Canada.†Approved, but not yet available (as of September 2017).1. Marso SP et al. NEJM. 2016;375:311–322; 2. Marso SP et al. NEJM. 2016; 375:1834–1844; 3. Intarcia Press Release. http://www.intarcia.com/media/press-releases/2016-may-6-cardiovascular-safety.html; 4. Pfeffer MA et al. N Engl J Med. 2015;373:2247–2257; 5. Holman RR et al. NEJM. 2017 [Epub ahead of print]
CVOT results for GLP-1 RAs have been neutral and positive, thus far
Unknown for MACE? Albiglutide (HARMONY) (2018) ?? Dulaglutide (REWIND) (2018) ?

15
GLP-1 receptor agonists:Key tips for initiation• Alleviate concerns around “injection”
◦ Familiarize patients (and yourself) with pen devices / needles Most are so small they are hard to see and so thin they are virtually painless
◦ Perform a “dry” injection to demystify the feeling of using a pen needle and pen◦ Have patients give the first dose in the office
• Provide practical tips to minimize nausea ◦ GI side effects are mostly mild to moderate and transient◦ Counsel patients to: Eat smaller meals, Stop eating when full, Avoid foods that
make them feel sick, Delay dose escalation, Dose at bedtime vs. morning
• Encourage behavioural changes to improve weight management
Adapted from Reid TS. Clinical Diabetes. 2013;31:148–157 and clinical opinion.
ACR, albumin:creatinine ratio; FRS, Framingham Risk Score=Estimation of 10-year cardiovascular disease risk; G1P1, gravidity (number of times female is or has been pregnant), parity (number of times female has carried the pregnancies to a viable gestational age).
What if Louise had CVD?Personal history
• 63 years old• City planner with private coverage• Indicates she is working on being more
active and will further improve her diet and activity levels
Assessments
• A1C 8.3%• BMI 32.2 kg/m2
• LDL 1.9 mmol/L• HDL 1.2 mmol/L• BP 136/78 mmHg• eGFR 72 mL/min/1.73 m2
• Urine ACR 1.4 mg/mmolMedical history
• Diagnosed with diabetes 6 years ago• G1P1: Experienced mild preeclampsia at
the end of her pregnancy with her son• Post menopausal• Family history of coronary heart disease• Diagnosed with hypertension 8 years ago• FRS high• Prior MI with stent x2 (2 years ago)
Medications
• Rosuvastatin 20 mg • Perindopril 8 mg • Aspirin 81 mg• Metformin 1 g bid
What should I know before prescribing a product for Louise if she has cardiovascular disease?
1. What is a cardiovascular outcome trial? 2. What if I prescribe a DPP-4 inhibitor?3. What if I prescribe a GLP-1 receptor agonist?4. What if I prescribe an SGLT2 inhibitor?
SGLT2 inhibitors: How do they compare?
Canagliflozin Dapagliflozin Empagliflozin
A1C Reduction of ~0.7–1.0%
Weight Weight loss of ~2–4 kg
Hypoglycemia Low risk of hypoglycemia
CV effects • MACE benefit• hHF benefit
n/a • MACE benefit• hHF benefit
Invokana® (canagliflozin) Product Monograph. Janssen Inc., 2016; Forxiga® (dapagliflozin) Product Monograph. AstraZeneca Canada Inc., 2016; Jardiance® (empagliflozin) Product Monograph. Boehringer Ingelheim (Canada) Ltd., 2016. Zinman B et al. NEJM. 2015;373:2117–2128; Neal B et al. NEJM. 2017;377(7):644–657.
Note: Data are from separate studies; no head-to-head data available
16
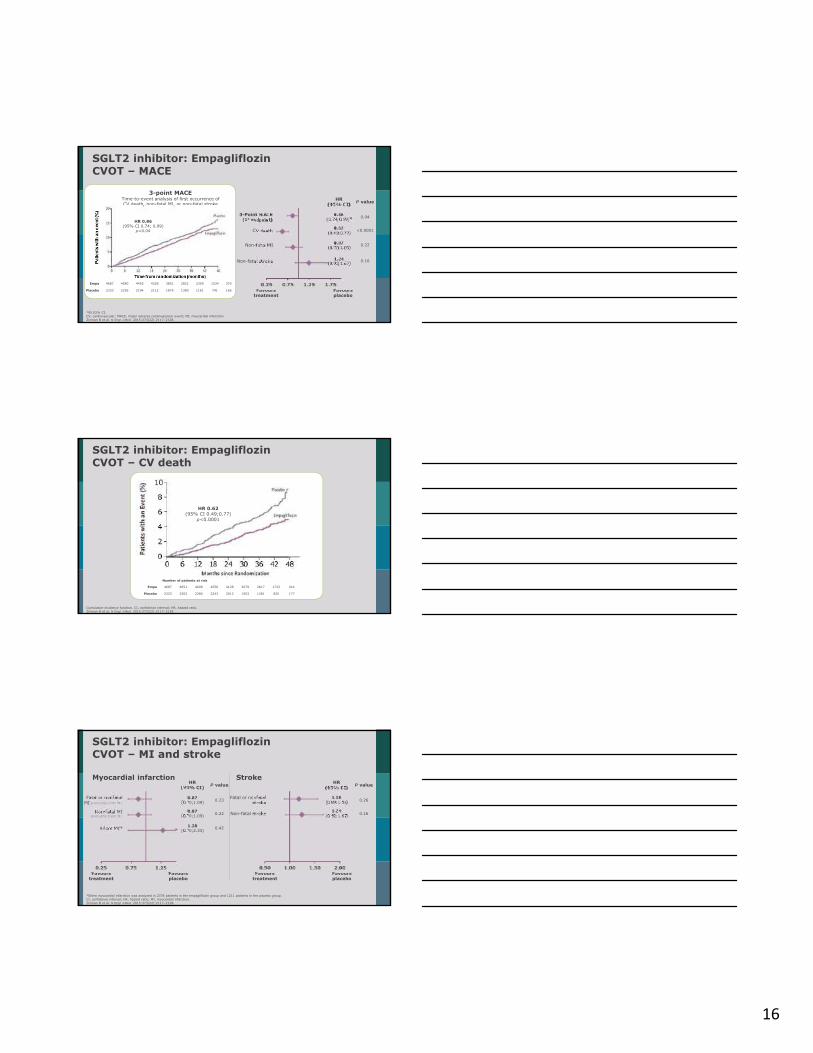
SGLT2 inhibitor: EmpagliflozinCVOT – MACE
*95.02% CI.CV, cardiovascular; MACE, major adverse cardiovascular event; MI, myocardial infarction.Zinman B et al. N Engl J Med. 2015;373(22):2117–2128.
HR(95% CI) P value
3-Point MACE(1° endpoint)
0.86(0.74;0.99)* 0.04
CV death 0.62(0.49;0.77) <0.0001
Non-fatal MI 0.87(0.70;1.09) 0.22
Non-fatal stroke 1.24(0.92;1.67) 0.16
Favours treatment
Favoursplacebo
3-point MACETime-to-event analysis of first occurrence of CV death, non-fatal MI, or non-fatal stroke
Empa 4687 4580 4455 4328 3851 2821 2359 1534 370
Placebo 2333 2256 2194 2112 1875 1380 1161 741 166
HR 0.86(95% CI 0.74; 0.99)
p=0.04
Cumulative incidence function. CI, confidence interval; HR, hazard ratio.Zinman B et al. N Engl J Med. 2015;373(22):2117–2128.
SGLT2 inhibitor: Empagliflozin CVOT – CV death
Number of patients at risk
Empa 4687 4651 4608 4556 4128 3079 2617 1722 414
Placebo 2333 2303 2280 2243 2012 1503 1281 825 177
HR 0.62(95% CI 0.49;0.77)
p<0.0001
Myocardial infarction Stroke
*Silent myocardial infarction was analyzed in 2378 patients in the empagliflozin group and 1211 patients in the placebo group. CI, confidence interval; HR, hazard ratio; MI, myocardial infarction.Zinman B et al. N Engl J Med. 2015;373(22):2117–2128.
SGLT2 inhibitor: EmpagliflozinCVOT – MI and stroke
HR(95% CI) P value
Fatal or nonfatalstroke
1.18(0.89;1.56) 0.26
Non-fatal stroke 1.24(0.92;1.67) 0.16
Favours treatment
Favoursplacebo
HR(95% CI) P value
Fatal or nonfatalMI (excluding silent MI)
0.87(0.70;1.09) 0.23
Non-fatal MI (excluding silent MI)
0.87(0.70;1.09) 0.22
Silent MI* 1.28(0.70;2.33) 0.42
Favours treatment
Favoursplacebo

17
Cumulative incidence function. CI, confidence interval; HR, hazard ratio.Zinman B et al. N Engl J Med. 2015;373(22):2117–2128.
SGLT2 inhibitor: EmpagliflozinCVOT – hHF
Number of patients at risk
Empa 4687 4614 4523 4427 3988 2950 2487 1634 395
Placebo 2333 2271 2226 2173 1932 1424 1202 775 168
HR 0.65(95% CI 0.50;0.85)
p=0.002
SGLT2 inhibitor: CanagliflozinCVOT – MACE
CV, cardiovascular; MACE, major adverse cardiovascular event; MI, myocardial infarction.Neal B et al. NEJM. 2017;377(7):644–657.
HR(95% CI) P value
3-Point MACE(1° endpoint)
0.86(0.75;0.97) 0.0158
CV death 0.87(0.72;1.06) n/a
Non-fatal MI 0.85(0.69;1.05) n/a
Non-fatal stroke 0.90(0.71;1.15) n/a
Favourstreatment
Favoursplacebo
3-point MACETime-to-event analysis of first occurrence of CV death, non-fatal MI, or non-fatal stroke
Cana 5795 5566 4343 2555 2460 2363 1661
Placebo 4347 4153 2942 1240 1187 1120 789
HR 0.86(95% CI 0.75; 0.97)
p=0.0158
Placebo
Canagliflozin
• Safety profile consistent with previously reported risks • New finding of increased risk of amputation
(toe or metatarsal) • 6.3 vs. 3.4 participants per 1000 patient-years;
HR 1.97 (95% CI 1.41; 2.75)
SGLT2 inhibitors:Key tips for initiation• Assess renal function1
◦ Do not initiate if eGFR is <60◦ Caution with renal dysfunction and loop diuretics
• Counsel patients on potential side effects1
◦ Genital infections, UTI, hypotension, dose-related changes in LDL-C◦ Dapagliflozin not to be used if bladder cancer◦ Rare diabetes ketoacidosis (may occur with no hyperglycemia)
• Caution in the elderly1
◦ Link between the risks of bone fracture and loss of bone mineral density with the use of canagliflozin2
With use of dapagliflozin, these risks were only identified in patients who had CKD No evidence of bone-related side effects was found to date with the use of empagliflozin
◦ Risk of reduced intravascular volume3
CKD, chronic kidney disease; LDL-C, low-density lipoprotein cholesterol; UTI, urinary tract infection.1. Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. Canadian Diabetes Association. Can J Diabetes. 2016;40;193–195; 2. Health Canada Safety Review. November 14, 2016. Available at: http://www.hc-sc.gc.ca/dhp-mps/medeff/reviews-examens/sglt2-3-eng.php; 3. Respective Product Monographs as of November 2016.

18
ACR, albumin:creatinine ratio; FRS, Framingham Risk Score=Estimation of 10-year cardiovascular disease risk; G1P1, gravidity (number of times female is or has been pregnant), parity (number of times female has carried the pregnancies to a viable gestational age)
What if Louise had CVD?Personal history
• 63 years old• City planner with private coverage• Indicates she is working on being more
active and will further improve her diet and activity levels
Assessments
• A1C 8.3%• BMI 32.2 kg/m2
• LDL 1.9 mmol/L• HDL 1.2 mmol/L• BP 136/78 mmHg• eGFR 72 mL/min/1.73 m2
• Urine ACR 1.4 mg/mmolMedical history
• Diagnosed with diabetes 6 years ago• G1P1: Experienced mild preeclampsia at
the end of her pregnancy with her son• Post menopausal• Family history of coronary heart disease• Diagnosed with hypertension 8 years ago• FRS high• Prior MI with stent x2 (2 years ago)
Medications
• Rosuvastatin 20 mg • Perindopril 8 mg • Aspirin 81 mg• Metformin 1 g bid
What would you prescribe for Louise?Let’s summarize our learnings.
1. HOPE investigators. N Engl J Med. 2000;342:145–53; 2. Zinman B et al. N Engl J Med. 2015;373(22):2117–2128; 3. Cordiner R et al. Practical Diabetes. 2016;33(8):266–268; 4. Marso SP et al. NEJM. 2016;375:311–322.
Summary: Number needed to treat (NNT) to prevent a Major Adverse Cardiovascular Event (MACE) across landmark trials in differing patient populations
2000 2015
High CV risk38% diabetes, 46% hypertension
Ramipril1for 4.5 years
Pre-ACEi/ARB era
<29% statin
Empagliflozin2,3
for 3.1 years
T2DM with established CVD
92% hypertension
>80% ACEi/ARB
>75% statin
T2DM with high CV risk (18%)or established CVD (82%)
92% hypertension
Liraglutide3,4
for 3.8 years
>80% ACEi/ARB
>70% statin
2016
Note: Data are from separate studies, in different patient populations
Available* options: How do they compare?
Agent A1C Weight Hypos CV effects
Sitagliptin
Reduction of ~0.5–0.8%
Weight neutral Low
risk
of
hypoglycemia
Neutral for MACE
Saxagliptin Neutral for MACE; hHF
Linagliptin n/a
Alogliptin Neutral for MACE
Liraglutide Reduction of ~1.0–1.5%
Liraglutide ≈Dulaglutide
Liraglutide >Exenatide
Weight loss of ~2–4 kg
Liraglutide >Dulaglutide
Liraglutide >Exenatide
MACE benefit
Dulaglutide n/a
Exenatide BID n/a
Exenatide QW Neutral for MACE
CanagliflozinReduction of ~0.7–1.0%
Weight loss of ~2–4 kg
MACE benefit; amputations
Dapagliflozin n/a
Empagliflozin MACE benefit
*Unapproved/unavailable products not included. References shown on previous slides.

19
ACR, albumin:creatinine ratio; FRS, Framingham Risk Score=Estimation of 10-year cardiovascular disease risk; G1P1, gravidity (number of times female is or has been pregnant), parity (number of times female has carried the pregnancies to a viable gestational age)
What if Louise had CVD?Personal history
• 63 years old• City planner with private coverage• Indicates she is working on being more
active and will further improve her diet and activity levels
Assessments
• A1C 8.3%• BMI 32.2 kg/m2
• LDL 1.9 mmol/L• HDL 1.2 mmol/L• BP 136/78 mmHg• eGFR 72 mL/min/1.73 m2
• Urine ACR 1.4 mg/mmolMedical history
• Diagnosed with diabetes 6 years ago• G1P1: Experienced mild preeclampsia at
the end of her pregnancy with her son• Post menopausal• Family history of coronary heart disease• Diagnosed with hypertension 8 years ago• FRS high• Prior MI with stent x2 (2 years ago)
Medications
• Rosuvastatin 20 mg • Perindopril 8 mg • Aspirin 81 mg• Metformin 1 g bid
What would you prescribe for Louise?
What would you prescribe for Louise?
a. Basal insulin b. DPP-4 inhibitorc. GLP-1 receptor agonistd. SGLT2 inhibitor e. Sulfonylureaf. TZD
What if…?
1. What if Louise was already on a DPP-4i?2. What if Louise’s eGFR was 55 mL/min?3. Can I use both an SGLT2 inhibitor and a GLP-1 receptor
agonist? 4. What are the mechanisms behind the cardiovascular
effects? Does one class work better with earlier CVD vs. later CVD (e.g., heart failure)?
5. What are the mechanisms behind weight loss?

At the Heart of It: A New Look at Clinical Cardiovascular Disease in Diabetes Ancillary Session at the Family Medicine Forum | CERT+ Session ID# 185941-109
Evaluation Form Date: Location: Thursday, November 9, 2017 at 6:45 a.m. Palais des congrès, Montreal Please rate the question in this evaluation according to the following scale:
1–Strongly disagree 2–Disagree 3–Neutral 4–Agree 5–Strongly agree
The Program The program content enhanced my knowledge. 1 2 3 4 5 The program was relevant to my practice. 1 2 3 4 5 The program met the stated learning objectives. 1 2 3 4 5 The program addressed a gap in my knowledge. 1 2 3 4 5 The program was well organized. 1 2 3 4 5 Adequate time was allotted for interaction and discussion. 1 2 3 4 5 The Presenter The presenter delivered the content clearly. 1 2 3 4 5 Questions and discussions were well moderated. 1 2 3 4 5 Time was efficiently managed. 1 2 3 4 5 Please indicate which CanMEDS-FM roles you felt were addressed during this educational activity. (select all that apply) Family Medicine Expert Collaborator Scholar Manager Communicator Health Advocate Professional Did the activity respect the « Ethical code of CME Providers1 »? � Yes � No If not, please explain (Ref.: 1. http://www.cemcq.qc.ca) Did you perceive any degree of bias in any part of the program? Yes No If yes, please explain:
Please describe what you felt was the most effective part of the program.
Please identify an important concept/idea that you learned.
How will you change your practice based on what you learned today? 1. 2.
Do you have any other learning needs related to this topic?
Other comments or suggestions about any aspect of the program: