atlas of angina final.qxd:angina l/o final - clinical publishing angina chp1.pdf · an atlas of...
TRANSCRIPT

An
gIn
A
AngInAIan J Sarembock
CliniCal Publishing
An Atlas of Investigation and Management
Sarem
bock
Cl
InIC
Al
Pu
Bl
ISH
Ing
An Atlas of Investigation and Management
AngInAAngina is most commonly associated with myocardial ischemia,
but may also be symptomatic of valvular heart disease,
hypertrophic cardiomyopathy or uncontrolled high blood pressure.
While chronic or stable angina is predictable and relatively easy to
manage, it is the sudden and unexpected onset of symptoms in
patients with unstable angina that represents the most significant
challenge to the clinician, being a risk indicator for acute MI,
severe cardiac arrhythmia or even cardiac arrest. Since chest pain
can also indicate a number of other less critical conditions, it is
important that the clinician can rapidly and accurately determine
the true risk status of the patient in each case.
In this atlas, the authors guide the reader through the assessment
of the patient with chest pain, beginning with the simple physical
examination and evaluation of other risk factors that may be
present, progressing to non-invasive tests such as EKg and various
imaging techniques, with a section on coronary angiography. non-
atherosclerotic causes are dealt with, and the book concludes with
an in-depth discussion on managing the patient with chronic
angina. The diagnostic value of each technique is assessed
throughout and appropriate guidance given on evaluating
clinical findings.
Related titles:
Interventional Cardiology: an Atlas of Investigation and Therapy
B Meier
ISBn 978-1-904392-11-8
Hypertension: an Atlas of Investigation and Management
ED Frolich, HO Ventura
ISBn 978-1-904392-15-6
Therapeutic Strategies in Hypertension
g Bakris
ISBn 978-1-904392-41-5
Website: www.clinicalpublishing.co.uk
ISBn: 978-1-904392-59-0
9 781904 392590
ISBN 1-904392-59-8
Laser Proof
An Atlas of Investigation and Management
ANGINA
Ian J Sarembock MB, ChB, MD, FAHA, FACC, FSCAIProfessor of Medicine
Director, Center for Interventional Cardiology & Coronary Care UnitCardiovascular Division & Cardiovascular Research Center
University of Virginia Health SystemCharlottesville, Virginia, USA
With contributions from:
Fadi M El-Ahdab, MDFellow
Cardiovascular DivisionUniversity of Virginia Health System
Charlottesville, Virginia, USA
David Isbell, MDFellow
Cardiovascular DivisionUniversity of Virginia Health System
Charlottesville, Virginia, USA
Michael Ragosta, MD, FACC, FSCAIAssociate Professor of Medicine
Director, Cardiac Catheterization LaboratoriesCardiovascular Division
University of Virginia Health SystemCharlottesville, Virginia, USA
CLINICAL PUBLISHINGOXFORD
Clinical Publishing
an imprint of Atlas Medical Publishing LtdOxford Centre for InnovationMill Street, Oxford OX2 0JX, UK
Tel: +44 1865 811116Fax: +44 1865 251550Email: [email protected]: www.clinicalpublishing.co.uk
Distributed in USA and Canada by:
Clinical Publishing30 Amberwood ParkwayAshland OH 44805 USA
Tel: 800-247-6553 (toll free within US and Canada)Fax: 419-281-6883Email: [email protected]
Distributed in UK and Rest of World by:
Marston Book Services LtdPO Box 269AbingdonOxon OX14 4YN UK
Tel: +44 1235 465500Fax: +44 1235 465555Email: [email protected]
© Atlas Medical Publishing Ltd 2007
First published 2007
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, ortransmitted, in any form or by any means, without the prior permission in writing of Clinical Publishingor Atlas Medical Publishing Ltd.
Although every effort has been made to ensure that all owners of copyright material have beenacknowledged in this publication, we would be glad to acknowledge in subsequent reprints or editionsany omissions brought to our attention.
A catalogue record of this book is available from the British Library
ISBN-13 978 1 904392 59 0ISBN-10 1 904392 59 8
The publisher makes no representation, express or implied, that the dosages in this book are
correct. Readers must therefore always check the product information and clinical procedures
with the most up-to-date published product information and data sheets provided by the
manufacturers and the most recent codes of conduct and safety regulations. The authors and
the publisher do not accept any liability for any errors in the text or for the misuse or
misapplication of material in this work.
Printed by T G Hostench SA, Barcelona, Spain

Contents
Preface vii
Abbreviations viii
1 Angina pectoris: epidemiology, natural history, and pathophysiology 1FADI EL-AHDAB AND MICHAEL RAGOSTA
Introduction 1Epidemiology 1Natural history 2Pathophysiology 3References 11Further reading 11
2 Angina pectoris: clinical evaluation 13FADI EL-AHDAB AND MICHAEL RAGOSTA
Introduction 13History 14Classification of chest pain 15Differential diagnosis 16Classification of angina 18Risk factor assessment 18Physical exam 19Pre-test probability 20Case scenario 22References 23
3 Noninvasive detection of coronary artery disease 25DAVID ISBELL AND IAN J SAREMBOCK
Introduction 25Risk stratification in the Emergency Department 25Imaging in the Emergency Department 29Patient and test selection 30Exercise EKG stress testing 30Radionuclide imaging to detect ischemia 34Positron emission tomography 37Stress echocardiography 37
vi
Magnetic resonance-based methods of detecting ischemia 41Special populations 47References 47Further reading 49
4 Coronary angio graphy and ancillary techniq ues for the invasive assessmentof angina pectoris 51MICHAEL RAGOSTA
Introduction 51Indications and contraindications 55Risks and potential complications 57Limitations 58Use of adjunctive invasive techniques 60Clinical scenarios 63References 66Further reading 66
5 Nonatherosclerotic causes of angina pectoris and ischemia 67MICHAEL RAGOSTA
Introduction 67Nonatherosclerotic obstruction 68Nonobstructive causes of angina 75Further reading 75
6 An approach to the management of chronic angina 77IAN J SAREMBOCK
Introduction 77Goals of therapy 78Strategies to control the symptoms of angina 80Coronary artery revascularization 87References 97
Index 101

vii
Preface
The purpose of this book, Angina: An Atlas of Investigationand Management, is to share with the readers an outline ofthe most important aspects of the epidemiology, naturalhistory, pathophysiology, clinical evaluation, non-invasivedetection and invasive assessment of angina pectoris, acommon manifestation of ischemic heart disease. Inaddition, we review the important non-atheroscleroticcauses of chest pain and articulate an overall approach to themanagement of chronic angina with respect to goals oftherapy including strategies to control symptoms and therole of coronary artery revascularization.
Over the last century, cardiovascular disease (CVD) hasburgeoned from a relatively minor disease worldwide to aleading cause of morbidity and mortality. By 2020 it isprojected that CVD will surpass infectious disease as theworld's leading cause of death and disability. The majorfactors impacting this include the projected 60% increase inpopulation between 1990 and 2020, the increasing lifeexpectancy as a result of improvements in public health andmedical care that are reducing rates of communicabledisease, malnutrition, and maternal and infant deaths andthe economic, social, and cultural changes that have led toincreases in risk factors for CVD. Chronic angina istraditionally recognized as the cardinal symptom ormanifestation of coronary artery disease (CAD), andworsening angina symptoms signal progression of theunderlying pathology. Angina is a clear warning sign of apotential myocardial infarction; approximately 50% ofmyocardial infarction patients have had preceding angina.Overall, angina presents a tremendous economic burden onthe health care system, society, employers, patients, andtheir families.
According to the American College ofCardiology/American Heart Association (ACC/AHA) 2002
Guideline Update for the Management of Patients withChronic Stable Angina, the goals of chronic anginamanagement are two-fold: to reduce morbidity andmortality; and to reduce symptoms. Medical therapy andrevascularization procedures, either coronary bypassgrafting (CABG) or percutaneous coronary interventions(PCI), play important roles in achieving these goals.However, these treatment options have limitations andsignificant expense and many patients have anatomicalfeatures or co-morbid conditions that prevent their optimalimplementation. Newer drugs and procedures, such astransmyocardial revascularization, enhanced externalcounterpulsation, and gene therapy, are all underinvestigation.
An undertaking of this magnitude needs the combinedefforts of numerous individuals, and as editor of this atlas, Iwant to express my sincere gratitude to my contributingauthors, each of whom made critically importantcontributions. They have worked diligently to meet theformat requirements of this atlas, the concept of whichentails a brief and highly structured text, supported byextensive graphics, flowcharts and tables and numerousphotographs of both the clinical signs of disease and ofcorresponding underlying pathology. Flowcharts, checklistsand algorithms have been used to summarize key facts, andpresent the reader with a rapid reference to the diagnosticprocess. Tables include all key data of diagnostic value. Inaddition, it has been a true pleasure working with thepublishing team of this atlas. Their advice, enthusiasm andcommitment to the project were critical to its success andare sincerely appreciated.
Ian J Sarembock
viii
Abbreviations
ACC American College of CardiologyACE angiotensin-converting enzymeACS acute coronary syndromeADR adverse drug reactionsAHA American Heart AssociationBMI body mass indexBNP brain natriuretic peptideBP blood pressureCABG coronary artery bypass graftingCAD coronary artery diseaseCCB calcium channel blockerCOPD chronic obstructive pulmonary diseaseCRP C-reactive proteinCSA chronic stable anginaCT computed tomographyDENSE displacement encoding with stimulated echoDES drug-eluting stentDSE dobutamine stress ECHOEBCT electron beam computed tomographyECHO echocardiographyED Emergency DepartmentEECP enhanced external counterpulsationETT exercise tolerance testEKG electrocardiogramFFR fractional flow reserveGERD gastroesophageal reflux diseaseGI gastrointestinalHDL high-density lipoproteinIHD ischemic heart diseaseISD ischemic sudden deathLAD left anterior descending (artery)LAO left anterior oblique
LBBB left bundle branch blockLCA left coronary arteryLDL low-density lipoproteinLp(a) lipoprotein-aLV left ventricleLVEF left ventricular ejection fractionMDCT multi-detector computed tomographyMETS metabolic equivalent tasksMI myocardial infarctionMRFP magnetic resonance first pass perfusionMRI magnetic resonance imagingMSCT multi-slice CTPCI percutaneous coronary interventionPET positron emission tomographyPPI proton pump inhibitorPTCA percutaneous transluminal coronary angioplastyQOL quality of lifeRAO right anterior obliqueRCA right coronary arteryRV right ventricleSCS spinal cord stimulationSECP sequential external counterpulsationSPECT single photon emission computed tomographySSFP steady state free precisionSTEMI ST segment elevation myocardial infarctionTENS transcutaneous electrical nerve stimulationTIC time–intensity curvesTIMI Thrombolysis In Myocardial Infarction (risk score)TMR transmyocardial laser revascularizationTTE trans-thoracic echocardiographyUA unstable anginaWHO World Health Organization

Angina pectoris:epidemiology, natural history, and pathophysiologyFadi El-Ahdab, MD, and Michael Ragosta, MD
Chapter 1
Introduction
The term ‘angina’ is from the Latin ‘angere’ meaning tostrangle, and was first described by the English physicianWilliam Heberden in 1768. Angina pectoris refers to thepredictable occurrence of pain or pressure in the chest oradjacent areas (jaw, shoulder, arm, back) caused bymyocardial ischemia. Typically, angina occurs in associationwith physical or emotional stress and is relieved by rest orsublingual nitroglycerin. Chronic stable angina refers to ananginal condition that has been observed over time and hasnot changed in terms of the level of exertion leading toangina, its severity, or frequency. It is important todistinguish stable angina from the acute ischemic syndromeswhich also cause anginal chest pain.
Epidemiology
Angina pectoris is due predominantly to ischemic heartdisease (IHD) from coronary atherosclerosis. IHDrepresents the leading cause of death in the United States(1.1), from several mechanisms including acute myocardialinfarction (MI), fatal arrhythmia, and heart failure.Although IHD is a major cause of death, its most commonmanifestation is chronic stable angina. In several studiesperformed in Western countries, the prevalence of anginapectoris in middle-aged individuals is estimated to bebetween 4 and 12%1–3. The American Heart Associationestimates that there are 16,500,000 patients with stableangina in the United States, and the reported annualincidence of angina among individuals more than 30 years
1
1.1 Causes of death in the United States per year (inthousands). Ischemic heart disease is the leading causeof death followed by cancer, cerebrovascular disease,and trauma.
1,200
1,000
800
600
400
200
0Dea
ths
per
year
(th
ousa
nds)
IHD Cancer AccidentsCause of death

old is 213 per 100,000 population. Angina pectoris is moreoften the presenting symptom of coronary artery disease(CAD) in women than in men, with a female-to-male ratioof 1.7:1. The frequency of atypical presentation is also morecommon among women compared with men. Women havea slightly higher mortality rate from CAD compared withmen, in part because of an older age at presentation and afrequent lack of classic anginal symptoms, thus delaying thediagnosis and treatment of CAD.
Natural history
The majority of patients with chronic stable angina haveunderlying coronary atherosclerosis. The natural history ofthis condition is based on the extent, severity, and nature ofthe underlying atherosclerosis (Table 1.1). The majority ofpatients with angina remain stable, with predictable anginacontrolled with medical therapy or by limitation of activity.In some patients, the condition actually attenuates withreduction of angina over time (likely due to the developmentof collaterals) or even development of an asymptomaticstate. The condition may exacerbate, however, with
worsening of symptoms despite medical therapy and lead tosubstantial impairment in the quality of life from debilitatingchest pain with minimal exertion. This may necessitaterevascularization procedures such as percutaneous coronaryintervention (PCI) or coronary bypass surgery. Moreimportantly, the patient may develop an acute syndromesuch as MI or unstable angina. The transformation of astable to an unstable atherosclerotic lesion is poorlyunderstood but is an important cause of death andmorbidity in patients with coronary disease. It is interestingto note that while 50% of patients with acute MI haveantecedent angina, few patients with angina progress toacute infarction. Two population-based studies fromOlmsted County, Minnesota and Framingham,Massachusetts found 3–3.5% annual rates of MI in patientswith angina4,5. Overall, survival in patients with chronicstable angina is good. The 5-year survival for patients with‘typical stable angina’ was 83% in one study from Italyinvolving 519 patients with angina pectoris. Age, long-standing angina, the presence of previous infarction, heartfailure, and an ischemic resting electrocardiogram (EKG)were among factors associated with a poor prognosis6.
Angina pectoris: epidemiology, natural history, and pathophysiology2
• Chronic stable anginal pattern• Exacerbation:
– need for revascularization procedure:percutaneous coronary interventioncoronary bypass surgery
– development of acute coronary syndrome:acute ST segment myocardial infarctionnon-ST segment myocardial infarctionunstable angina
• Improvement:– reduction in angina– development of asymptomatic state
Table 1.1 Outcome of patients with coronary disease
Pathophysiology
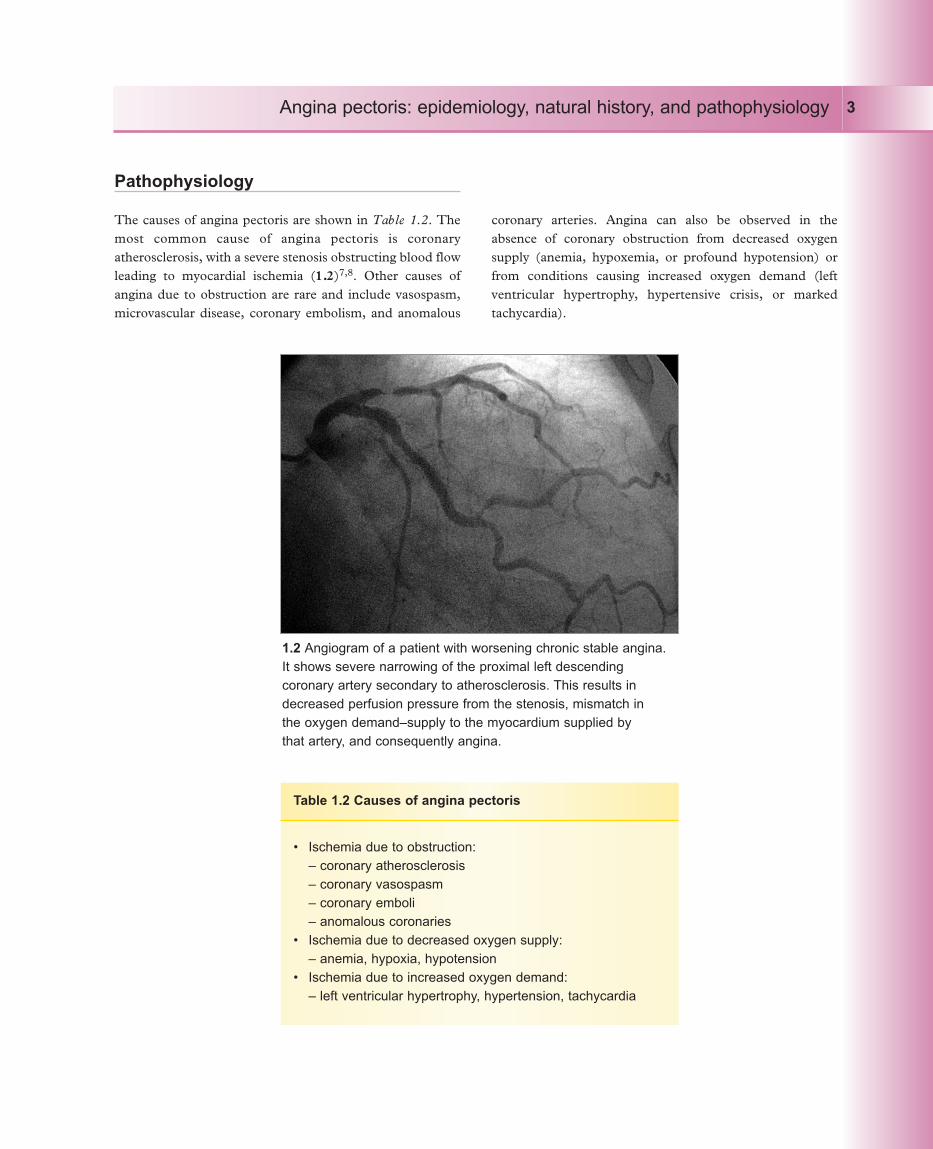
The causes of angina pectoris are shown in Table 1.2. Themost common cause of angina pectoris is coronaryatherosclerosis, with a severe stenosis obstructing blood flowleading to myocardial ischemia (1.2)7,8. Other causes ofangina due to obstruction are rare and include vasospasm,microvascular disease, coronary embolism, and anomalous
coronary arteries. Angina can also be observed in theabsence of coronary obstruction from decreased oxygensupply (anemia, hypoxemia, or profound hypotension) orfrom conditions causing increased oxygen demand (leftventricular hypertrophy, hypertensive crisis, or markedtachycardia).
Angina pectoris: epidemiology, natural history, and pathophysiology 3
• Ischemia due to obstruction:– coronary atherosclerosis– coronary vasospasm– coronary emboli– anomalous coronaries
• Ischemia due to decreased oxygen supply:– anemia, hypoxia, hypotension
• Ischemia due to increased oxygen demand:– left ventricular hypertrophy, hypertension, tachycardia
Table 1.2 Causes of angina pectoris
1.2 Angiogram of a patient with worsening chronic stable angina.It shows severe narrowing of the proximal left descendingcoronary artery secondary to atherosclerosis. This results indecreased perfusion pressure from the stenosis, mismatch in the oxygen demand–supply to the myocardium supplied by that artery, and consequently angina.

The atherosclerotic coronary lesion is a lipid-containingplaque (also known as an atheroma) in the intima of theartery7–11. Atheroma formation is secondary to a complexset of mechanisms only partially understood, involvingendothelial dysfunction, lipoprotein deposition andoxidation in the arterial wall, infiltration by inflammatorycells, cellular proliferation, especially smooth muscle cells,and matrix deposition (1.3). This mechanism may start atan early age. Endothelial dysfunction is thought to be theinitial step in atherosclerosis (1.4). Endothelial dysfunctionmay result from the injurious effects of free radicals causedby tobacco smoking or from the effects of low-densitylipoprotein (LDL) cholesterol, hypertension, diabetes,infectious agents, genetic factors, or a combination of these.Endothelial dysfunction results in increased endothelialpermeability to lipoproteins, increased expression ofadhesion molecules, and release of chemotactic factors thatattract inflammatory cells (monocytes, macrophages,lymphocytes) and smooth muscle cells and facilitate theirmigration into the arterial wall. The fatty streak (1.5) results
Angina pectoris: epidemiology, natural history, and pathophysiology4
Normal artery
Fatty streak
Fibrous plaque
Normal smooth muscle cells and connective tissue with endothelial lining
LDL accumulates between endothelium and connective tissue and is oxidized and incorporated
into macrophages
Further accumulation of cholesterol and division of smooth muscle cells with fibrous tissue
formation and thickening of arterial wall leading to luminal narrowing
Endothelial dysfunction
1.3 Steps in the development of atheroma. Atheroma formation is secondary to a complex set of mechanisms involvingendothelial dysfunction, lipoprotein deposition and oxidation in the arterial wall, infiltration by inflammatory cells, cellularproliferation, especially smooth muscle cells, and matrix deposition.
from the deposition of macrophages, lymphocytes, andsmooth muscle cells into the arterial wall. In the arterialwall, macrophages containing LDL form ‘foamy cells’ andrelease cytokines and free radicals, causing more localdamage and attracting more cells. As more foamy cells,inflammatory cells, and smooth muscle cells accumulate inthe arterial wall, the fatty streak will grow in size and willtend to form a fibrous cap surrounding a lipid core(fibrofatty plaque or atheroma) (1.6). The cap consists ofconnective tissue and the lipid core includes foamy cells,leukocytes, and debris. As the plaque grows in size, it willpush its way towards the lumen of the artery. When it islarge enough to interfere with blood flow, ischemia andangina will result. Stable atheromas have a collagen-rich,thick fibrous cap, abundant smooth muscle cells, and fewermacrophages and usually result in chronic stable angina.Atheromas with thin caps, a large necrotic core andabundant macrophages tend to be less stable (vulnerableplaque) with a tendency to rupture, resulting in acutecoronary syndromes, including MI.
Angina pectoris: epidemiology, natural history, and pathophysiology 5
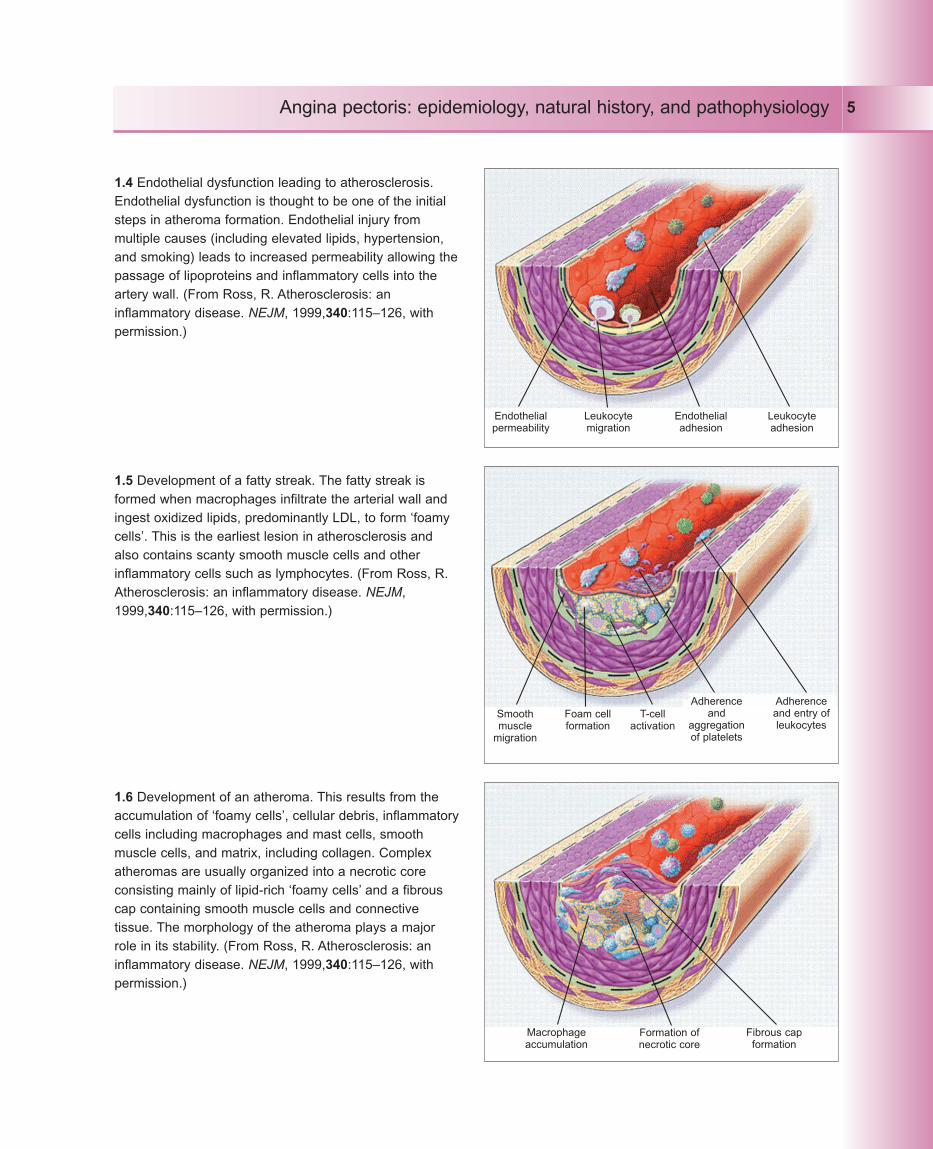
1.4 Endothelial dysfunction leading to atherosclerosis.Endothelial dysfunction is thought to be one of the initialsteps in atheroma formation. Endothelial injury frommultiple causes (including elevated lipids, hypertension,and smoking) leads to increased permeability allowing thepassage of lipoproteins and inflammatory cells into theartery wall. (From Ross, R. Atherosclerosis: aninflammatory disease. NEJM, 1999,340:115–126, withpermission.)
Endothelialpermeability
Leukocytemigration
Endothelialadhesion
Leukocyteadhesion
1.6 Development of an atheroma. This results from theaccumulation of ‘foamy cells’, cellular debris, inflammatorycells including macrophages and mast cells, smoothmuscle cells, and matrix, including collagen. Complexatheromas are usually organized into a necrotic coreconsisting mainly of lipid-rich ‘foamy cells’ and a fibrouscap containing smooth muscle cells and connectivetissue. The morphology of the atheroma plays a majorrole in its stability. (From Ross, R. Atherosclerosis: aninflammatory disease. NEJM, 1999,340:115–126, withpermission.)
1.5 Development of a fatty streak. The fatty streak isformed when macrophages infiltrate the arterial wall andingest oxidized lipids, predominantly LDL, to form ‘foamycells’. This is the earliest lesion in atherosclerosis andalso contains scanty smooth muscle cells and otherinflammatory cells such as lymphocytes. (From Ross, R.Atherosclerosis: an inflammatory disease. NEJM,1999,340:115–126, with permission.)
Smoothmuscle
migration
Foam cellformation
T-cellactivation
Adherenceand
aggregationof platelets
Adherenceand entry ofleukocytes
Macrophageaccumulation
Formation ofnecrotic core
Fibrous capformation

In patients with stable angina, the plaque tends to be slowgrowing and relatively stable. However, the plaque mayundergo rapid and dynamic changes (1.7). Plaque rupturedue to inflammation and other poorly understoodmechanisms may result in platelet aggregation andthrombus formation. There are several consequences of thisevent. The event may be silent and lead to progression ofluminal narrowing. More importantly, the thrombus may beocclusive and lead to sudden death from ventricularfibrillation or a nonfatal ST segment elevation MI.Nonocclusive thrombus may lead to significant flowlimitation at rest and cause the acute ischemic syndromes ofnon-ST segment elevation MI or unstable angina. Unlikechronic stable angina, these conditions are potentially life-threatening and lead to substantial morbidity and mortality.
The mechanisms involved in the development ofischemia are complex and not solely related to the presenceof a coronary stenosis. The amount of oxygen available in
the myocardium is a function of the oxygen demand by theheart and of oxygen supply. Ischemia and subsequentlyangina result from mismatch between the amount of oxygenneeded by the myocardium (oxygen demand) (Table 1.3)and the amount supplied to the myocardium (oxygensupply) (1.8). Myocardial oxygen demand is the majordeterminant of coronary blood flow. It is important to notethat exercise may increase myocardial oxygen demand asmuch as 4–5-fold over baseline. Oxygen supply to themyocardium depends on coronary blood flow, the oxygencontent of the blood (which depends on the bloodoxygenation from the lungs and the amount of hemoglobinthat carries oxygen), and the amount of oxygen extracted bythe myocardium. Since the oxygen content is fixed and themyocardium already extracts most of the oxygen deliveredto it, there is little or no oxygen extraction reserve. Thus,any increase in oxygen consumption requires an increase incoronary blood flow.
Angina pectoris: epidemiology, natural history, and pathophysiology6
1.7 Pathogenesis of acute coronary syndromes. Atherosclerotic plaque mayhave a thick fibrous cap and be stable, causing chronic stable angina whenflow-limiting. In contrast, it might have a thin fibrous cap, large necrotic coreand abundant inflammatory cells, resulting in a vulnerable plaque that is proneto rupture, and thrombosis which might be occlusive (resulting in ST-elevationmyocardial infarction or sudden cardiac death) or nonocclusive (resulting in anacute coronary syndrome). Causes of plaque rupture include inflammation andother unknown mechanisms.
Inflammation?Plaque rupture
Asymptomatic
Stable angina
Thrombus
• Sudden death • Acute coronary syndrome– ST elevation MI– Non-ST elevation MI– Unstable angina pectoris
• Silent progression
Angina pectoris: epidemiology, natural history, and pathophysiology 7
Heart rateContractilityWall stress
Oxygen demand
Normalstate
Matched
Mismatched
IschemiaAngina
Coronary blood flowPerfusion pressureVascular resistance
Oxygen supply
Oxygen contentin blood:
hemoglobinoxygen saturation
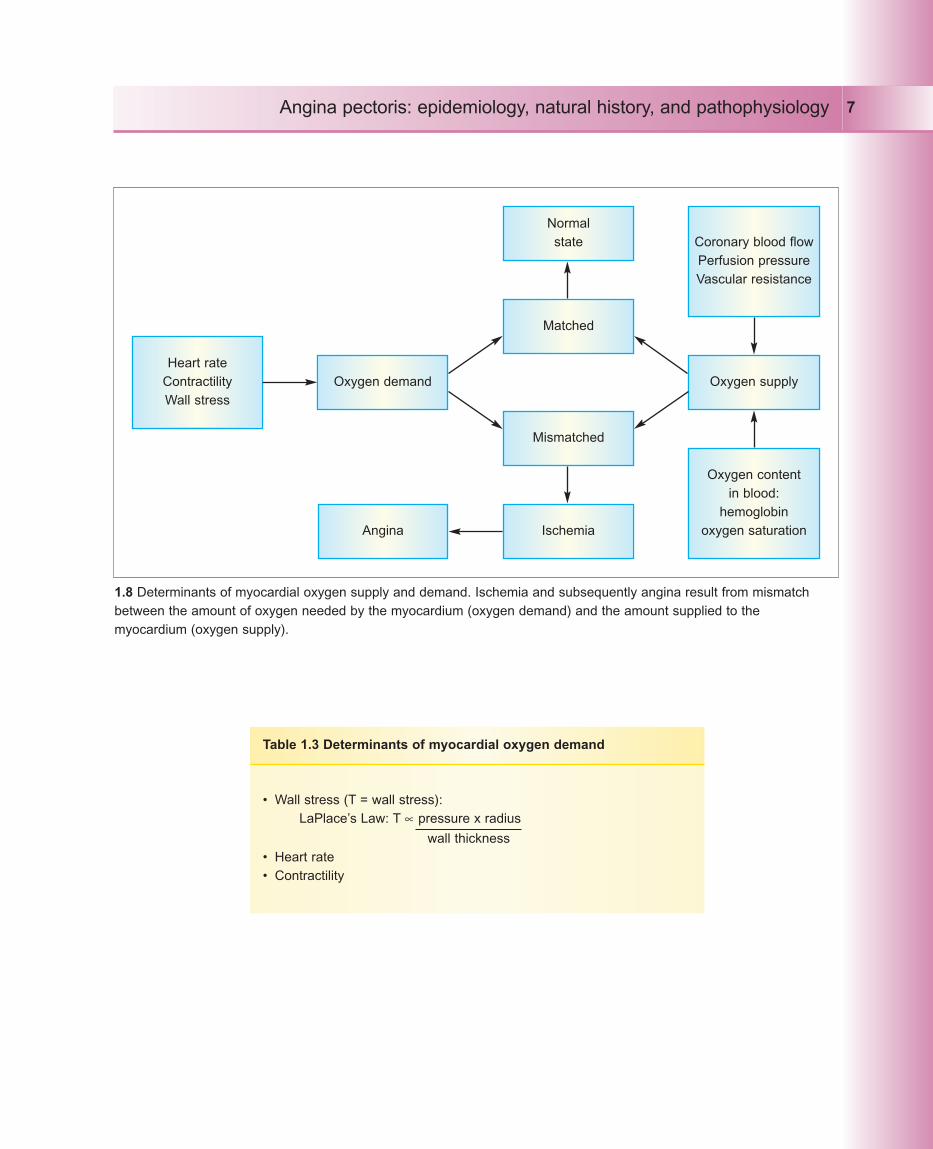
1.8 Determinants of myocardial oxygen supply and demand. Ischemia and subsequently angina result from mismatchbetween the amount of oxygen needed by the myocardium (oxygen demand) and the amount supplied to themyocardium (oxygen supply).
• Wall stress (T = wall stress):LaPlace’s Law: T ∝ pressure x radius
wall thickness• Heart rate• Contractility
Table 1.3 Determinants of myocardial oxygen demand

Coronary blood flow is determined primarily by thecoronary resistance vessels (Table 1.4). These vessels in turnare influenced by endothelial-mediated factors, metabolites,and neurohormonal mechanisms. A complex balance ofthese factors maintains basal flow at fairly constant levelsdespite changing perfusion pressure, by a process known as‘autoregulation’ (1.9). Autoregulation plays a major role instabilizing myocardial blood flow under varying perfusionpressures and is stable over a large range of perfusionpressure. However, autoregulatory mechanisms areoverwhelmed when the perfusion pressure dropssignificantly, resulting in a decrease in blood flow. Thus,myocardial ischemia represents an exhaustion of thecompensatory mechanisms regulating blood flow.
Coronary flow reserve is an important mechanism thatprotects the heart from ischemia with progressive coronaryobstruction (1.10). With progressive luminal narrowing fromatherosclerosis, blood flow remains essentially unchanged atrest because of arteriolar vasodilatation and recruitment fromthe process of autoregulation until the stenosis becomes toosevere (>80%). However, under hyperemic stress, the flow
reserve is exhausted, and flow begins to decline when thediameter of the stenosis exceeds 50%.
Other factors may play a role in causing demand–supplymismatch and ischemia in patients with CAD. Onesuggested mechanism is paradoxical vasoconstriction of thediseased coronary vessels due to dysfunction of the coronaryendothelium, which normally releases vasodilators such asnitric oxide. In atherosclerotic arteries, the dysfunctionalendothelium fails to release vasodilators in response tohyperemia, resulting in vasoconstriction and ischemia.Another mechanism involves de-recruitment of myocardialcapillary beds in diseased coronary vessels during hyperemicstates, causing decreased blood flow to the affectedmyocardium.
Patients with chronic stable angina may have worseningof their symptoms due to progressive disease ortransformation into an acute coronary syndrome. However,based on the complex mechanisms involved in thedevelopment of ischemia, factors other than progressiveobstruction may be involved. These factors are summarizedin Table 1.5.
Angina pectoris: epidemiology, natural history, and pathophysiology8
• Driving pressure through the coronary vessel• Extravascular compression• Coronary resistance vessels:
– endothelial factors – nitric oxide, prostaglandins, endothelin– metabolites – adenosine, hypoxia, hypercapnea– neurohormonal mechanisms
Table 1.4 Determinants of coronary blood flow

Angina pectoris: epidemiology, natural history, and pathophysiology 9
1.9 Autoregulation of coronary blood flow. The role ofcoronary autoregulation in stabilizing myocardial bloodflow under varying perfusion pressures is important, andis stable over a large range of perfusion pressure. Butwhen the perfusion pressure drops significantly,autoregulatory mechanisms become overwhelmed. Thisresults in decrease in blood flow and subsequentlyischemia.
Coronaryblood flow
0 80 160Coronary pressure (mmHg)
Autoregulatory range
1.10 Relation of stenosis severity to coronary bloodflow. Coronary flow reserve is an important mechanismthat protects the heart from ischemia and generallyincreases from 2–5-fold with maximal coronaryvasodilatation. Coronary flow reserve becomesdiminished when lesions are >50% and is essentiallyoverwhelmed for lesions >80%.
Coronaryblood flow
0 50 80 100Stenosis (%)
Vasodilator flow
Flow reserve
Resting flow
Increased oxygen demandNoncardiac:• Hyperthermia• Hyperthyroidism• Sympathomimetic toxicity (cocaine use)• Hypertension• Anxiety• Arteriovenous fistula
Cardiac:• Hypertrophic cardiomyopathy• Aortic stenosis• Dilated cardiomyopathy• Tachycardia:
– ventricular– supraventricular
Decreased oxygen supplyNoncardiac:• Anemia• Hypoxemia:
– pneumonia, asthma, COPD, pulmonary hypertension, interstitial pulmonary fibrosis, obstructive sleep apnea
• Sickle-cell disease• Sympathomimetic toxicity (cocaine use)• Hyperviscosity:
– polycythemia, leukemia, thrombocytosis, hypergammaglobulinemia
Cardiac:• Aortic stenosis• Hypertrophic cardiomyopathy
Table 1.5 Causes of myocardial ischemia other than coronary atherosclerosis
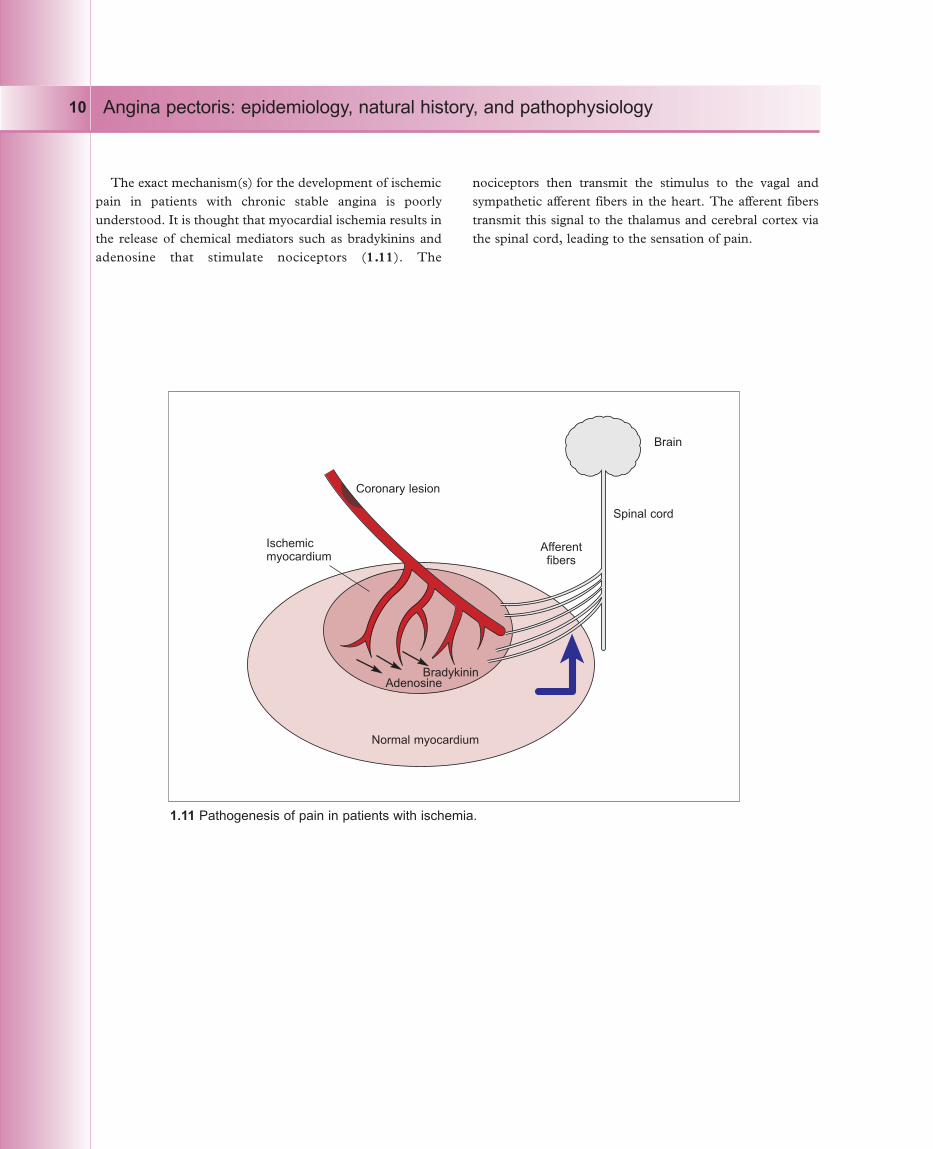
The exact mechanism(s) for the development of ischemicpain in patients with chronic stable angina is poorlyunderstood. It is thought that myocardial ischemia results inthe release of chemical mediators such as bradykinins andadenosine that stimulate nociceptors (1.11). The
nociceptors then transmit the stimulus to the vagal andsympathetic afferent fibers in the heart. The afferent fiberstransmit this signal to the thalamus and cerebral cortex viathe spinal cord, leading to the sensation of pain.
Angina pectoris: epidemiology, natural history, and pathophysiology10
1.11 Pathogenesis of pain in patients with ischemia.
Coronary lesion
Spinal cord
Brain
Normal myocardium
Afferentfibers
BradykininAdenosine
Ischemicmyocardium

References
1 Reid DD, Brett GZ, Hamilton PJS, e t al.Cardiorespiratory disease and diabetes among middle-aged male civil servants. A study of screening andintervention. Lancet 1974;1(7856):469–473.
2 WHO European Collaborative Group. Multifactorial trialin the prevention of coronary heart disease.1.Recruitment and critical findings. Eur Heart J1980;1:73–80.
3 Shaper AG, Cook DG, Walker M, MacFarlane PW.Prevalence of ischemic heart disease in middle-agedBritish men. Br Heart J 1984;51:595–605.
4 Elveback LR, Connolly DC, Melton LJ III. Coronaryheart disease in residents of Rochester, Minnesota 7.Incidence, 1950 through 1982. Mayo Clin Proc1986;61:896–900.
5 Kannel WB, Feinleib M. Natural history of anginapectoris in the Framingham study. Prognosis andsurvival. Am J Cardiol 1972;29:154–163.
6 Brunelli C, Cristofani R, L’Abbate A. Long-term survivalin medically treated patients with ischemic heart diseaseand prognostic importance of clinical andelectrophysiologic data. Eur Heart J 1989;10:292–303.
7 Lambert CR. Pathophysiology of stable angina pectoris.Cardiol Clin 1991;9(1):1–10.
8 Zipes DP. Chronic coronary artery disease. In: ROBonow, B Gersh, E Braunwald (eds), Braunwald’s HeartDisease: A Textbook of Cardiovascular Medicine, 7thedn. Saunders, Philadelphia, 2005.
9 Crawford M, DiMarco J, Paulus W. Cardiology, 2nd edn.Mosby, St Louis, 2003.
10 Abrams J. Chronic stable angina. NEJM2005;352:2524–2533.
11 Ross R. Atherosclerosis: an inflammatory disease.NEJM 1999;340:115–126.
Further reading
Lilly L. Pathophysio logy of Heart Disease. LippincottWilliams & Wilkins, Philadelphia, 2002.
Angina pectoris: epidemiology, natural history, and pathophysiology 11