atrial fibrillation after stroke in the...
TRANSCRIPT

209
Atrial Fibrillation After Stroke in the ElderlyPaul J. Friedman, MD, FRACP
To examine the relationship between atrial fibrillation and mortality after stroke, we studied186 men and 167 women from the Waikato Stroke Registry whose mean age was 75.2 ±7.5 years.Twenty-three percent (82 of 353) had atrial fibrillation or flutter on their admission electro-cardiogram. This group differed significantly from that with sinus rhythm in three respects:1) They were older (p<0.01); 2) they had more severe current stroke deficit as evidenced bylower limb power (p<0.05) and Mini-Mental State Score (p<0.001), higher incidence ofhomonomous hemianopia (/><0.05), and lower incidence of lacunar syndrome stroke(p<0.001); and 3) they had a significantly higher incidence of cardiomegaly and congestiveheart failure (p<0.01). Functional outcome was insignificantly better in the group with sinusrhythm. During a mean follow-up period of 18 months, mortality was significantly higher in thegroup with atrial fibrillation (/>=0.001). Proportional hazards modeling, however, showed thatthe apparently poorer survival in those patients with atrial fibrillation could be explained byfactors other than cardiac rhythm, such as age, Mini-Mental State Score, level of conscious-ness, and interstitial edema on admission chest radiograph. Thus, atrial fibrillation was not anindependent predictor of survival after stroke. (Stroke 1991^2:209-214)
Atrial fibrillation is common among elderlypeople with acute stroke.1-2 The medicalliterature regarding atrial fibrillation and
stroke has generally focused on the risk of initial andsubsequent stroke in patients with atrial fibrillation.This risk is highest in people with underlying rheu-matic or valvular heart disease, intermediate in thosewith nonvalvular atrial fibrillation, and lowest inthose with lone atrial fibrillation.3'4 Patients withatria! fibrillation have a higher incidence of conges-tive heart failure than those with sinus rhythm.2-3
Heart failure, in turn, may contribute to the increasedmortality among patients with atrial fibrillation.
Proportional hazards modeling is a powerful toolfor analyzing survival and for determining factorsassociated with mortality. Proportional hazards mod-eling of survival is more informative than analysis atdiscrete time intervals because it uses all survivaldata as opposed to data at one point in time. Inpopulations with coronary artery disease5 and elderlypeople living in the community,6 proportional haz-ards modeling has shown atrial fibrillation to be anindependent predictor of mortality, even after ac-counting for other features of heart disease. Fewstudies have examined atrial fibrillation after strokeas a predictor of survival.7-10 In the only such study to
From the Stroke Unit, Waikato Hospital, Hamilton, NewZealand.
Funded in part by grants from the New Zealand Lottery Boardand the Waikato Medical Research Foundation.
Address for reprints: Paul J. Friedman, Stroke Unit, WaikatoHospital, Hamilton, New Zealand.
Received February 28, 1990; accepted September 7, 1990.
use proportional hazards modeling,7 52 of the 409patients had transient ischemic attack rather thanstroke. Hence, study results may not generalize to apopulation of acute stroke patients. Accordingly, wehave used proportional hazards modeling to examinethe relationship between atrial fibrillation and mor-tality in the Waikato Stroke Registry population.
Subjects and MethodsWe defined stroke as rapidly developing clinical
signs of focal or global (if stupor or coma present)loss of brain function lasting more than 24 hours orleading to death, with no apparent cause other thancerebral infarction or intracerebral hematoma. Pa-tients with subarachnoid hemorrhage were excluded.
We examined all patients aged 60 and aboveadmitted to Waikato Hospital with suspected stroke,usually within 1-3 days after admission. Seventy-sixpercent of patients were admitted within 48 hours ofstroke onset. If there was any doubt about thediagnosis of stroke, the patient did not enter thestroke registry until there was confirmation of thediagnosis by computed tomography (CT), single-photon emission computed tomography (SPECT)using ["Tcjhexamethylpropyleneamine oxime, orautopsy. Probable lacunar syndrome stroke was de-fined by the presence of one of the lacunar syn-dromes11 and the absence of a larger infarction onCT, if performed.
During the 24-month patient entry period (May 1,1987, to May 1, 1989) 388 stroke events were re-corded in the Waikato Stroke Registry. We excluded
by guest on June 15, 2018http://stroke.ahajournals.org/
Dow
nloaded from

210 Stroke Vol 22, No 2, February 1991
35 stroke events for the following reasons: 14 wererecurrences in patients already part of the study, 15had no electrocardiogram, two had a permanentpacemaker or complete heart block, and four werelost to follow-up before 120 days after stroke. Thus,the study included 353 patients—186 men and 167women with a mean age of 75.2 ±7.5 years. Ninety-three percent lived at home as opposed to an insti-tution before the current stroke.
We used minimum power in the affected limbs,graded on the Medical Research Council Scale, asthe index of motor loss from stroke. We calculatedarm power by averaging power scores for elbowflexion and finger abduction. Leg power was calcu-lated by averaging power scores for hip extension,knee extension, and ankle dorsiflexion. Mini-MentalState Score was used to assess cognitive impair-ment.12 The modified Barthel activities of daily living(ADL) score13 ranged from zero (totally dependentand doubly incontinent) to 20 (independent self-careabilities and continent). Prestroke Barthel score wasdetermined from reports of the patient's family.Maximal Barthel score was denned as the highestBarthel score from those measured on days 7, 30, 60,90, 120, and 180 poststroke; it was thus used as atime-independent measure of maximal recovery.
We used the electrocardiogram and chest radio-graph performed at the time of admission to classifycardiac rhythm and radiographic signs of heart failure.Patients with atrial fibrillation or flutter were classifiedas having atrial fibrillation. Those with sinus rhythm,irrespective of the presence of premature beats, wereclassified as having sinus rhythm. We excluded pa-tients with permanent pacemakers or complete heartblock. Cardiomegaly was denned as a cardiothoracicratio above 030, pulmonary venous congestion bydistention of upper lobe veins and peripheral blurring,and interstitial edema by the presence of Kerley Blines and reticular shadowing. Heart failure, myocar-dial infarction, hypertension, and diabetes were de-fined by the past or current clinical diagnoses ofcongestive cardiac failure, myocardial infarction, hy-pertension, and diabetes mellirus, respectively.
For patients who died, the principal cause of deathwas extracted from death certificates. Heart diseaseas a cause of death included myocardial infarction,congestive heart failure, sudden death, and any othercardiac disorder listed as principal cause of death.
We used Student's t test and the x2 test whenappropriate for univariate comparison of the twogroups for continuous and discrete data, respectively.Ninety-five percent confidence intervals were calcu-lated.14 We used a proportional hazards model with aWeibull distribution to analyze survival with the SASStatistical Package procedure LIFEREG. Independentvariables in the model included age, sex, prestrokeBarthel ADL score, prestroke residence (home orinstitution), prior stroke (yes or no), level of con-sciousness on admission (alert or not alert) arm andleg power scores, homonomous hemianopia (present/absent), Mini-Mental State Score, stroke type (lacu-nar or nonlacunar), rhythm (atrial fibrillation or sinusrhythm), cardiomegaly, pulmonary venous conges-tion, interstitial edema (present/absent), heart fail-ure (yes or no), myocardial infarction (yes or no),hypertension (yes or no), and diabetes (yes or no).
The study was approved by the Medical ResearchEthics Committee.
ResultsEighty-two of the 353 patients (23%) had atrial
fibrillation at the time of admission. In 57% thisrhythm had been documented before stroke. Ninety-six percent of patients with atrial fibrillation wereconsidered on clinical grounds to have nonvalvularatrial fibrillation; the remaining three patients hadmitral stenosis, prosthetic heart valve, and hyper-trophic cardiomyopathy, respectively.
The group with atrial fibrillation differed from thatwith sinus rhythm in three respects: they were signif-icantly older; they had more severe current strokedeficit as evidenced by lower incidence of lacunarsyndrome stroke, lower level of consciousness onadmission, lower limb power and Mini-Mental StateScore, and a higher incidence of homonomous hemi-anopia; and they had a higher incidence of cardiome-
TABLE 1. Comparison of Patients With Atrial Fibrillation and Sinus Rhythm After Stroke With Regard toDemographic Characteristics, Prestroke Features, and Clinical Diagnoses
n
Male (% male)
Age
Prestroke Barthel ADL
Prior stroke
Hypertension
Heart failure
Myocardial infarction
Diabetes mellitus
Atrial fibrillation
82
39 (48%)
77.4+8.1*
19.5+1.1
17/82 (21%)
35/82 (43%)
43/82 (52%)t
12/82 (15%)
14/82 (17%)
Sinus rhythm
271
147 (63%)
74.5±7.2
19.2±2.2
65/271 (24%)
142/271 (52%)
38/271 (14%)
51/271 (19%)
46/271 (17%)
95% a-
-19% to +6%
1.0 to 4.8
-0.3 to +0.8
- 1 3 % to +7%
-22% to +2%
27% to 50%
- 1 3 % to +5%
- 9 % to +9%
Values are mean±SD. CI, confidence interval; ADL, activities of daily living score.*p<0.0i.tp<0.001.
by guest on June 15, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Friedman Atrial Fibrillation Poststroke 211
TABLE 2. Comparison of Patients With Atrial Fibrillation and Sinus Rhythm With Regard to Current Stroke Deficitand Admission Chest Radiographic Signs of Heart Failure
Atrial fibrillation Sinus rhythm 95% CI
Lacunar syndrome stroke
Alert on admission
Arm power score
Leg power score
Homonomous hemianopia}
Mini-Mental State Scoret
Cardiomegaly
Pulmonary venous congestion
Interstitial edema
3/82 (4%)'
53/82 (65%)t
1.77±1.86t
2.03±1.88t
32/68 (47%)t10.3±10.4*
("=75)
47f70 (67%)*
22/70 (31%)'
11/70 (16%)§
54/271 (20%)
207/271 (76%)
2.33±1.90
2.62±1.84
75/239 (31%)
15.2±11.2
(n=252)
76/251 (30%)
29/251 (12%)
12/251 (5%)
-22%to0%
-20% to - 2 %
-1.03 to -0.09
-1.05 to -0.13
+4% to +30%
-7.8 to -2 .0
+24% to +49%
+8% to+31%
+2% to +20%
Values are mean±SD. CI, confidence interval.
tp<0.05.^Excludes patients not tested or not able to be tested.§p<0.01.
galy and congestive heart failure as evidenced byadmission chest radiography and clinical diagnosis(Tables 1 and 2).
The two groups were similar with regard to pre-stroke Barthel ADL score, incidence of prior stroke,and frequency of clinical diagnoses of myocardialinfarction and diabetes (Table 1). Hypertension wasinsignificantly more common among those with sinusrhythm (Table 1).
Survival was significantly worse among those withatrial fibrillation as compared to those in sinusrhythm. Figure 1 shows that survival of the twogroups continued to diverge over time; at 6, 12, and18 months poststroke, the difference in survival be-tween the two groups rose from 16% to 18% and29%, respectively.
Computed tomography was performed on agreater proportion of patients with sinus rhythm than
100
2 4 6 8 10 12 14 16 18
Month post-stroke
FIGURE 1. Comparison of survival of patients with atrial
fibrillation (squares) and sinus rhythm (triangles).
with atrial fibrillation (92 of 271 versus 15 of 82,p<0.05). The incidence of intracerebral hematomawas insignificantly higher in the group with sinusrhythm compared to those with atrial fibrillation(20% versus 7% of those undergoing CT scanning,respectively). Patients with sinus rhythm were threetimes more likely to have a nondiagnostic CT scanthan those with atrial fibrillation (18 of 92 versus oneof 15,/>=NS). Patients with atrial fibrillation who hada CT scan were a selective group with much lower90-day mortality than those who did not have a CTscan (20% versus 49%, respectively). In contrast,90-day mortality in patients with sinus rhythm with orwithout CT scanning was similar (25% versus 27%).Overall, 49% of those with sinus rhythm as comparedto 35% of those with atrial fibrillation had either aCT scan, a SPECT scan, or autopsy of the brain.Among patients with first-ever stroke who receivedCT scanning, the frequency of silent infarction on CTwas 13% among those with atrial fibrillation and 10%among those with sinus rhythm.
Mean follow-up was 18 months poststroke (range,4-35 months). Only five of the 82 patients with atrialfibrillation were treated with long-term anticoagula-tion. This decision was generally left to the attendingphysician; some physicians did not use anticoagulantson elderly patients, whereas others would use themonly for those patients with excellent functionalrecovery after stroke.
To analyze predictors of survival, we first enteredsingly the independent variables shown in Tables 1and 2 into a proportional hazards model. The bestunivariate predictors of mortality, ranked in orderaccording to their x2 value from the proportionalhazards model, are shown in Table 3. Cardiac rhythmwas the ninth best predictor of the 12 significantlyassociated with survival. Variables not significantlyrelated to survival included sex, prestroke Barthelscore, prior residence, prior stroke, homonomoushemianopia, myocardial infarction, and diabetes.
by guest on June 15, 2018http://stroke.ahajournals.org/
Dow
nloaded from
212 Stroke Vol 22, No 2, February 1991
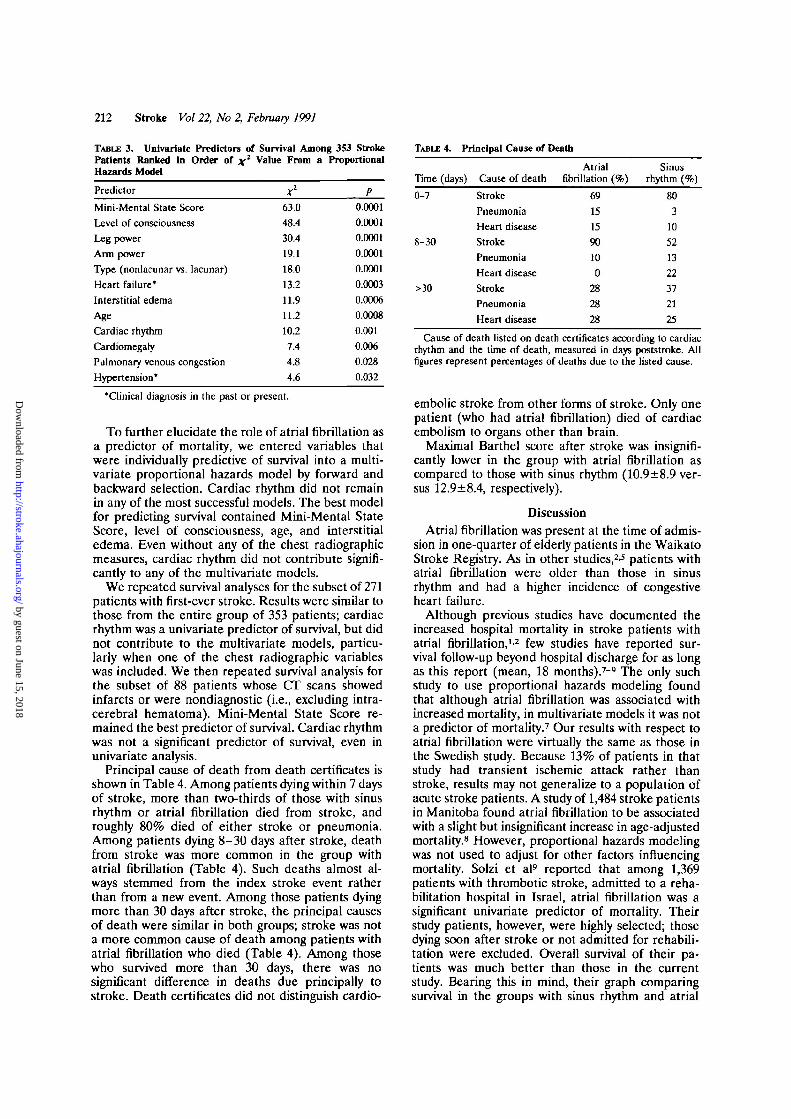
TABLE 3. Univariate Predictors of Survival Among 353 StrokePatients Ranked In Order of x2 Value From a ProportionalHazards Model
Predictor x1 P
Mini-Mental State Score 63.0 0.0001
Level of consciousness 48.4 0.0001
Leg power 30.4 0.0001
Arm power 19.1 0.0001
Type (nonlacunar vs. lacunar) 18.0 0.0001
Heart failure' 13.2 0.0003
Interstitial edema 11.9 0.0006
Age 11.2 0.0008
Cardiac rhythm 10.2 0.001
Cardiomegaly 7.4 0.006
Pulmonary venous congestion 4.8 0.028
Hypertension* 4.6 0.032
'Clinical diagnosis in the past or present.
To further elucidate the role of atrial fibrillation asa predictor of mortality, we entered variables thatwere individually predictive of survival into a multi-variate proportional hazards model by forward andbackward selection. Cardiac rhythm did not remainin any of the most successful models. The best modelfor predicting survival contained Mini-Mental StateScore, level of consciousness, age, and interstitialedema. Even without any of the chest radiographicmeasures, cardiac rhythm did not contribute signifi-cantly to any of the multivariate models.
We repeated survival analyses for the subset of 271patients with first-ever stroke. Results were similar tothose from the entire group of 353 patients; cardiacrhythm was a univariate predictor of survival, but didnot contribute to the multivariate models, particu-larly when one of the chest radiographic variableswas included. We then repeated survival analysis forthe subset of 88 patients whose CT scans showedinfarcts or were nondiagnostic (i.e., excluding intra-cerebral hematoma). Mini-Mental State Score re-mained the best predictor of survival. Cardiac rhythmwas not a significant predictor of survival, even inunivariate analysis.
Principal cause of death from death certificates isshown in Table 4. Among patients dying within 7 daysof stroke, more than two-thirds of those with sinusrhythm or atrial fibrillation died from stroke, androughly 80% died of either stroke or pneumonia.Among patients dying 8-30 days after stroke, deathfrom stroke was more common in the group withatrial fibrillation (Table 4). Such deaths almost al-ways stemmed from the index stroke event ratherthan from a new event. Among those patients dyingmore than 30 days after stroke, the principal causesof death were similar in both groups; stroke was nota more common cause of death among patients withatrial fibrillation who died (Table 4). Among thosewho survived more than 30 days, there was nosignificant difference in deaths due principally tostroke. Death certificates did not distinguish cardio-
TABLE 4. Principal Cause of Death
Time (days)
0-7
8-30
>30
Cause of death
Stroke
Pneumonia
Heart disease
Stroke
Pneumonia
Heart disease
Stroke
Pneumonia
Heart disease
Atnalfibrillation (%)
69
15
15
90
10
0
28
28
28
Sinusrhythm (%)
80
3
10
52
13
22
37
21
25
Cause of death listed on death certificates according to cardiacrhythm and the time of death, measured in days poststroke. Allfigures represent percentages of deaths due to the listed cause.
embolic stroke from other forms of stroke. Only onepatient (who had atrial fibrillation) died of cardiacembolism to organs other than brain.
Maximal Barthel score after stroke was insignifi-cantly lower in the group with atrial fibrillation ascompared to those with sinus rhythm (10.9±8.9 ver-sus 12.9±8.4, respectively).
DiscussionAtrial fibrillation was present at the time of admis-
sion in one-quarter of elderly patients in the WaikatoStroke Registry. As in other studies,2-5 patients withatrial fibrillation were older than those in sinusrhythm and had a higher incidence of congestiveheart failure.
Although previous studies have documented theincreased hospital mortality in stroke patients withatrial fibrillation,1'2 few studies have reported sur-vival follow-up beyond hospital discharge for as longas this report (mean, 18 months).7-9 The only suchstudy to use proportional hazards modeling foundthat although atrial fibrillation was associated withincreased mortality, in multivariate models it was nota predictor of mortality.7 Our results with respect toatrial fibrillation were virtually the same as those inthe Swedish study. Because 13% of patients in thatstudy had transient ischemic attack rather thanstroke, results may not generalize to a population ofacute stroke patients. A study of 1,484 stroke patientsin Manitoba found atrial fibrillation to be associatedwith a slight but insignificant increase in age-adjustedmortality.8 However, proportional hazards modelingwas not used to adjust for other factors influencingmortality. Solzi et al9 reported that among 1,369patients with thrombotic stroke, admitted to a reha-bilitation hospital in Israel, atrial fibrillation was asignificant univariate predictor of mortality. Theirstudy patients, however, were highly selected; thosedying soon after stroke or not admitted for rehabili-tation were excluded. Overall survival of their pa-tients was much better than those in the currentstudy. Bearing this in mind, their graph comparingsurvival in the groups with sinus rhythm and atrial
by guest on June 15, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Friedman Atrial Fibrillation Poststroke 213
fibrillation showed the same continued divergenceover the first 18 months poststroke as ours. Among283 stroke patients from another Swedish study whowere followed a mean of 20 months, atrial fibrillationwas not a significant predictor of mortality even inunivariate analysis.10
Our patients with atrial fibrillation had more severecurrent stroke deficit than those in sinus rhythm. Inparticular, they had a lower incidence of lacunarsyndrome stroke, lower limb power, and Mini-MentalState Score, and a higher incidence of homonomoushemianopia. Overall, this suggests a larger volume ofbrain involved by the current stroke. The Stroke DataBank reported a similar finding15; patients with lacu-nar infarction had a lower incidence of atrial fibrilla-tion than those with nonlacunar infarction (3% versus12%). Atrial fibrillation did not influence functionalrecovery from stroke, as evidenced by maximal Bar-thel ADL score during the first 6 months after stroke.
In univariate analysis using the proportional haz-ards model, atrial fibrillation was one of 12 significantpredictors of mortality. However, in multivariateproportional hazards analysis, atrial fibrillationdropped out of the model. The best predictors ofsurvival were Mini-Mental State Score, level of con-sciousness, age, and interstitial edema. Thus, theapparent increase in mortality among patients withatrial fibrillation can be explained by other differ-ences between that group and those in sinus rhythm.Similar results occurred when analysis was confinedto patients with first-ever stroke.
Other reports have confirmed age79-16"18 and im-paired level of consciousness7-810-17-18 as importantpredictors of mortality after stroke. A study of atrialfibrillation poststroke in Glasgow found an increasedmortality compared to sinus rhythm in patients aged60-79, but not in those aged 80 or older.1 Accord-ingly, we reanalyzed our data using these age brack-ets. The hospital mortality ratio (atrial fibrillationmortality/sinus rhythm mortality) was 1.64 for age60-79 and 1.39 for age 80 or older. Thus, our resultsin part support the findings from Glasgow.
Our study has two major limitations. First, andmost importantly, only 30% of the study patients hadCT scans. To further compound this problem, CTscanning was performed significantly more often inthose patients with sinus rhythm than in those withatrial fibrillation and, when performed, showed ahigher incidence of intracerebral hematoma in thosewith sinus rhythm (20% versus 7%,p=NS). Patientswith intracerebral hematoma have a higher 30-daymortality than those with cerebral infarction.15 Theproportional hazards survival model we used did notinclude disease (infarction versus hematoma) as anindependent variable because of the low frequency ofCT scanning. Had we performed CT scans on allpatients, we could have either excluded those withhematoma or used disease (infarct versus hematoma)as an independent variable in survival modeling.Such analyses would have more accurately assessedthe effects of cardiac rhythm on survival after stroke.
Had we excluded patients with intracerebral he-matoma, the mortality difference between those insinus rhythm and those in atrial fibrillation probablywould have been greater than we observed in ourpatients with either cerebral infarction or intracere-bral hematoma.
The second major limitation of this study was thelow autopsy rate and frequent lack of documentationas to whether disease or death during follow-up wasrelated to cardioembolic events. We had to rely ondeath certificates, which are frequently inaccurate, asa uniform measure to assess cause of death. Deathcertificates rarely distinguished cardioembolic strokefrom other forms of stroke.
Results from this study can be generalized to otherpopulations of elderly patients admitted to hospitalafter stroke as defined by World Health Organizationcriteria (excluding subarachnoid hemorrhage). Only6% of our patients with atrial fibrillation receivedlong-term anticoagulation poststroke. Hence, find-ings from this report cannot be generalized to anti-coagulated patients or to patients not admitted tohospital after stroke. Study results need to be con-firmed in a patient sample undergoing universal earlyCT scanning to detect intracerebral hematoma.
In conclusion, atrial fibrillation poststroke oc-curred in one-quarter of elderly stroke registry pa-tients. Atrial fibrillation was associated with signifi-cantly worse survival than sinus rhythm, but afteradjusting for the greater age, more severe strokedeficit, and higher incidence of heart failure amongpatients with atrial fibrillation, we found that cardiacrhythm was no longer a significant predictor ofsurvival. This is consistent with results from tworandomized trials which found that warfarin reducedthe subsequent rate of systemic emboli without alter-ing mortality in atrial fibrillation.19-20
AcknowledgmentThe author wishes to thank Dr. Harold Henderson
from the Waikato Centre for Applied Statistics forhis statistical advise.
References1. Lowe GD, Jaap AJ, Forbes CD: Relation of atrial fibrillation
and high haematocrit to mortality in acute stroke. Lancet1983;l:784-786
2. Britton M, Gustafsson C: Non-rheumatic atrial fibrillation as arisk factor for stroke. Stroke 1985;16:182-188
3. Wolf PA, Dawber TR, Thomas HE, Kannel WB: Epidemio-logic assessment of chronic atrial fibrillation and risk of stroke:The Framingham Study. Neurology 1978;28:973-977
4. Kopecky SL, Gersh BJ, McGoon MD, Whisnant JP, HolmesDR, Ilstrup DM, Frye RL: The natural history of lone atrialfibrillation: A population-based study over three decades. NEnglJMed 1987;317:669-674
5. Cameron A, Schwartz MJ, Kronmal RA, Kosinski AS: Preva-lence and significance of atrial fibrillation in coronary arterydisease (CASS Registry). Am J CardiM 1988;61:714-717
6. Lake FR, Cullen KJ, de Klerk NH, McCall MG, Rosman DL:Atrial fibrillation and mortality in an elderly population. AustNZJMcd 1989;19:321-326
by guest on June 15, 2018http://stroke.ahajournals.org/
Dow
nloaded from

214 Stroke Vol 22, No 2, February 1991
7. Viitanen M, Eriksson S, Asplund K, Wester PO, Winblad B:Determinants of long-term mortality after stroke. Ada MedScand 1987;221:349-356
8. Abu-Zeid HA, Choi NW, Hsu P, Maini KK: Prognostic factorsin the survival of 1,484 stroke cases observed for 30 to 48months: II. Clinical variables and laboratory measurements.Arch Neurol 1978;35:213-218
9. Solzi P, Ring H, Najenson T, Luz Y: Hemiplegics after a firststroke: Late survival and risk factors. Stroke 1983;14:703-709
10. Miah K, Von Arbin M, Britton M, De Faire U, Helmers C,Maasing R: Prognosis in acute stroke with special reference tosome cardiac factors. J Chron Dis 1983;36:279-288
11. Bamford J, Sandercock P, Jones L, Warlow C: The naturalhistory of lacunar infarction: The Oxfordshire CommunityStroke Project. Stroke 1987;18:545-551
12. Folstein MF, Folstein SE, McHugh PR: Mini-Mental State: Apractical method for grading the cognitive state of patients forthe clinician. J Psychiatr Res 1975;12:189-198
13. Wade DT, Hewer RL: Functional abilities after stroke: Mea-surement, natural history and prognosis. / Neurol NeurosurgPsych 1987;50:177-182
14. Gardner MJ, Altaian DG: Confidence intervals rather than Pvalues: Estimation rather than hypothesis testing. Br Med J1986;292:746-750
15. Foulkes MA, Wolf PA, Price TR, Mohr JP, Hier DB: TheStroke Data Bank: Design, methods and baseline characteris-tics. Stroke 1988;19:547-554
16. Howard G, Walker MD, Becker C, Coull B, Feibel J, McLeroyK, Toole JF, Yatsu F: Community hospital-based strokeprograms: North Carolina, Oregon and New York. III. Factorsinfluencing survival after stroke: Proportional hazards analysisof 4219 patients. Stroke 1986;17:294-299
17. Bonita R, Ford MA, Stewart AW: Predicting survival afterstroke: A three-year follow-up. Stroke 1988;19:669-673
18. Abu-Zeid HA, Choi NW, Hsu P, Maini KK: Prognostic factorsin the survival of 1,484 stroke cases observed for 30 to 48months: I. Diagnostic types and descriptive variables. ArchNeurol 1978;35:121-125
19. Petersen P, Boysen G, Godtredsen J, Andersen AD, AndersenB: Placebo-controlled, randomised trial of warfarin and aspi-rin for prevention of thromboembolic complications in chronicatrial fibrillation. Lancet 1989;1:175-178
20. Stroke Prevention in Atrial Fibrillation Study Group Investi-gators: Preliminary report of the Stroke Prevention in AtrialFibrillation Study Group. N Engl J Med 1990;322:863-868
KEY WORDS • atrial fibrillation • cerebrovascular disorders
by guest on June 15, 2018http://stroke.ahajournals.org/
Dow
nloaded from

P J FriedmanAtrial fibrillation after stroke in the elderly.
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1991 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.22.2.209
1991;22:209-214Stroke.
http://stroke.ahajournals.org/content/22/2/209World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Stroke Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on June 15, 2018http://stroke.ahajournals.org/
Dow
nloaded from