australia and new zealand nutrient reference...
TRANSCRIPT

AustralianandNewZealandNutrientReferenceValuesforFluoride
AreportpreparedfortheAustralianGovernment
DepartmentofHealth
By
ExpertWorkingGroupforFluoride
JanisBaines,MichaelFoley,AndrewJohnSpencer,MarcoPeresandUtzMuellerwithResearchAssistancefrom
JudyCunningham,EmmanuelGnanamanickam,NajithAmarasenaJULY2015

ii
TableofContents
1. Introduction..............................................................................................7
1.1Fundingsource.........................................................................................7
1.2UseofNutrientReferenceValues............................................................7
1.3Summaryof2006NRVsforFluoride......................................................10
1.4Triggersandrationaleforreview...........................................................11
1.5Backgroundinformation-fluoride.........................................................11
2. ScopeandPurpose..................................................................................13
3. EvidenceReview.....................................................................................14
3.1Fluorideintakeestimatesininfantsandyoungchildren.......................14
3.1.1 AustraliaandNewZealand.......................................................14
3.1.2 International.............................................................................15
3.2Selectionofbiomarkersforfluoride......................................................17
3.2.1 Dentalcaries.............................................................................17
3.2.2 Fluorosis....................................................................................21
3.3Selectionofevidence.............................................................................25
3.3.1 Reviewofmajorreports...........................................................26
3.3.2 Systematicreviewofnewliterature.........................................31
3.3.3 SystematicLiteratureReviewResults.......................................34
3.4Assumptionsandlimitations..................................................................39
3.5Reviewofevidence-DerivationofULandAI........................................40
3.5.1 DoseresponseassessmenttoestablishaUL...........................40
3.5.2 DietaryFluorideIntakeestimatesfortheDeanstudy..............44
3.5.3 UpperLevelofIntake(UL)........................................................46
3.5.4 AdequateIntake(AI).................................................................48
3.5.5 CurrentfluorideintakeinAustraliaandNewZealand.............49
4 Guidelinerecommendations...................................................................52
4.1DraftNRVs..............................................................................................52
4.1.2 UpperLevelofIntake(UL)........................................................52
4.1.3 AdequateIntake(AI).................................................................52
4.2ValidityofRecommendations................................................................53
4.3Furtherresearch.....................................................................................54
5 Membershipofgroupsandcommitteesinvolvedinthedevelopmentprocess....................................................................................................55
6 Glossary..................................................................................................57
7 Listofabbreviations................................................................................59
8 ReferenceList..........................................................................................63
9 Listoftables............................................................................................74
10 Listoffigures...........................................................................................75
11 Listofboxes............................................................................................76
12 Appendix1.Summaryoffindings–GRADEassessment...........................77
13 Attachments...........................................................................................84


1 AustralianandNewZealandNutrientReferenceValuesforFluoride
ExecutiveSummary
TheNutrientReferenceValues(NRVs)areasetofrecommendednutrientintakesusedtoassessdietaryrequirementsofindividualsandpopulationgroups.ThecurrentNRVsforAustraliaandNewZealandwerepublishedin2006(NHMRC&MOH2006)afteracomprehensivereviewprocesscommissionedbytheDepartmentofHealthandAgeing(DOHA)andtheNewZealandMinistryofHealth(MoH).TheNationalHealthandMedicalResearchCouncil(NHMRC),whichcarriedoutthereview,recommendedthattheserecommendationsbereviewedeveryfiveyears.In2011DOHA,nowtheDepartmentofHealth(DoH),inconsultationwiththeNZMoHcommissionedascopingstudyforundertakingareviewoftheNRVs.ThisresultedinthedevelopmentofaMethodologicalFrameworkforthereviewbyNousandaconsortiumofexperts(NousGroup2013).Thepurposeofthepresentreviewistotestthisframeworkonthreenutrients,onebeingfluoride.
Fluorideisnaturallypresentinthefoodanddrinkweconsumeandisconsideredanormalconstituentofthehumanbody.Thefluorideconcentrationinbonesandteethisabout10,000timesthatinbodyfluidsandsofttissues(Bergmann&Bergmann1991;1995).Nearly99%ofthebody’sfluorideisboundstronglytocalcifiedtissues.Fluorideinboneappearstoexistinbothrapidly-andslowly-exchangeablepools.
Fluorideavailablesystemicallyduringtoothdevelopmentisincorporatedintoteethasfluorapatiteintoothenamel.Fluorapatiteintoothenamelaltersitscrystallinestructure,reducingthesolubilityofenameltoaciddissolution,ordemineralization.Athigherfluorideintakesthecrystallinestructuremaybedisruptedduringtoothdevelopmentperiods,formingporositieswhicharethebasisofdentalfluorosis.However,outcomessuchasskeletalfluorosisandbonefracturesoccuronlyafterprolongedexposuretoveryhighfluorideintakes.Fluorideatthesurfaceofenamelcanalsoformcalciumfluoride,amorerapidly-exchangeablepooloffluoridetoalterthedemineralization-remineralizationbalance,whichisthedynamicprocessunderlyingdentalcaries.DentalcariesisalargelypreventablebuthighlyprevalentchronicdiseaseinAustralianandNewZealandchildrenandadults.
AustraliaandNewZealandhavepursuedpublichealthpolicytoadjustfluorideintakeatthepopulationlevelwiththeaimofpreventingdentalcarieswithoutcausingmoderateorseveredentalfluorosisandotheradverseeffects.Itisconsidereddesirabletohaveafluorideintakethatissufficienttopreventdentalcaries(anAdequateIntake)withoutexceedingintakesthatareassociatedwithmoderateorseveredentalfluorosis(anUpperLevelofIntake).However,thereisevidencethatfluorideintakesmayexceedrecommendedlevelsorestablishedupperlevelsofintakeforchildrenevenwhenwaterfluoridationlevelsfollowthecurrenttargetdrinkingwaterlevelsinAustralia(0.6-1.1mgF/L)(NHMRC2007)andNewZealand(0.7to1.0mgF/L)(MoH2005)and/orwhenindividualsareexposedtofluoride

2 AustralianandNewZealandNutrientReferenceValuesforFluoride
fromothersources1.Yetneithercountryexperiencesmorethantherareoccurrenceofmoderateorseveredentalfluorosis.ThisapparentexceedanceofrecommendedfluorideintakelevelswithouttheoccurrenceofmoderateorseveredentalfluorosiscreatedtheconundrumaroundNRVsforfluoridetowhichthisreportresponds.
ThecurrentNRVsforfluorideforallagegroupswerenotabletobereviewedinthetimeallocatedforthispilotreview.TheExpertWorkingGroup(EWG)narrowedthescopeofitsreviewtoanAdequateIntake(AI)andUpperLevelofIntake(UL)forfluorideforinfantsandyoungchildren,asthecriticalagegroupstoconsiderfordentalcariesandfluorosis.TheEWGnotedtheterm‘TolerableUpperLevelofIntake’wasanappropriatewaytodescribetheULforfluoridethathasbeenusedinternationally,however,tomaintainconsistencywiththeestablishmentofNRVsforothernutrientsinAustraliaandNewZealand,theterm‘UpperLevelofIntake’wasretainedforfluoride.
TheEWGconductedseveralliteraturereviews.First,eightformalreportsincludingthelandmarkUSInstituteofMedicineonfluoride,publishedin1997,andsevenotherspublishedinthe17yearssincetheIOMreport,werereviewed(IOM1997,McDonaghetal..2000,NRC2006,EPA2010a,b,SCHER2011,EFSA2005,2013).ThefocusofthisreviewofreportswasthedataavailableuponwhichtobuildNRVsandthemethodologyadopted.ThereviewofreportsrevealedthecentralrolethatDean’sdataofthelate1930s-40s(Deanetal.1941,1942;Dean1942,1946)hadinalltheseevaluationsinestimationofdose-responserelationshipsbetweencriticalfluorideconcentrationsinthewatersupplyandthepreventionofdentalcariesandadversedentalfluorosis.
Theend-pointfordentalcariesintheDeanstudieswasthecariesexperiencemeasuredbytheDecayed,Missing,andFilledTeethscoreamong12–14yearoldchildrenwhiletheendpointfordentalfluorosiswastheDean’sIndexscoresortheCommunityFluorosisIndex.Themostseveredentalfluorosisobservedhadpittingorlossofdentalenamel,interpretedasaDean’sIndexscoreof4(Dean1942).
ApproachestothederivationoffluorideintakesatcriticalfluorideconcentrationsinthewatersupplywereassessedsoastoguidetheEWG’ssubsequentdeterminations.
Literaturepublishedin2005andonwardswassearchedandrelevantliteratureidentified.NoalternativedatawereidentifiedthatcouldbesubstitutedforDean’sdatafromthe1930s(Deanetal.1941,1942;Dean1942,1946)forcriticalfluorideconcentrationsinrelationtothepreventionofdentalcariesandminimisationofmoderateandseveredentalfluorosis.Thebulkoftherelevantliteratureaddressedfluorideintakesincontemporarycommunitiesandthepreventionofcariesorriskofdentalfluorosis.
1DrinkingwaterGuidelinesinAustraliaandNewZealandarebasedonhealthconsiderationsandstatethe
concentrationoffluorideindrinkingwatershouldbeintherangeof0.7to1.0mgF/Lbutshouldnotexceed1.5mgF/L(NHMRC2013,MoH2005).However,intheNHMRC2007statementonthesafetyandefficacyoffluoridation,itisrecommendedthatwaterinAustraliabefluoridatedintherange0.6-1.1mg/L,dependingonclimate,tobalancethereductionofdentalcariesandoccurrenceofdentalfluorosis(NHMRC2007).

3 AustralianandNewZealandNutrientReferenceValuesforFluoride
TheEWGidentifiedthecriticalfluorideconcentrationsinthewatersupplyfromDean’sdataforthenearmaximalpreventionofdentalcaries(theAI)andforpreventionofmoderateorseveredentalfluorosis(theUL).Nearmaximalcariespreventionwasassociatedwithafluorideconcentrationof1.0mgF/L,whilethecriticalconcentrationforpreventionofseverefluorosis(<0.5%prevalenceofseverefluorosis)was1.9mgF/L.
Dietaryfluorideintakeforchildrenatthecriticalfluorideconcentrationswasestimatedusingthreesetsofdataonfluidandfoodconsumptionamongchildren:McClure’smodeldiet,theUS1977–78NationwideFoodConsumptionSurveyandtheAustralian1995NationalNutritionSurvey(McClure1943,EPA2010a,FSANZ2014).Therewasahighlevelofagreementbetweenthedailyfluorideintakeestimates.Theyrangedfromapproximately0.04mgF/kgbw/dayatthemeanto0.20mgF/kgbw/dayatthe95thpercentileofintake.
Thedistributionoffluorideintakesforarangeofchildagesandtheirassociatedbodyweightsatthecriticalfluorideconcentrationof1.9mg/Lwaterwasdeterminedandthe95thpercentileoffluorideintakesusedtoestablishanUpperLevelofIntakeoffluoride.TheUpperLevelofIntakeoffluoridewasestablishedat0.20mgF/kgbw/dayforchildrentoavoidseveredentalfluorosis.ThisestimateishigherthantheexistingUpperLevelofIntakeoffluorideof0.1mgF/kgbw/daypreviouslyestablishedbytheNHMRCin2006,whichwasbasedontheIOM1997report(NHMRC2006).TheEWGwassatisfiedthattherewasaninconsistencyintheestimationoftheUpperIntakeLevelintheIOMreport.TheEWGnotedthattherevisedULishigherthanthefluorideReferenceDoseof0.08mgF/kgbw/dayestablishedbytheEPAin2010(EPA2010a).TheEWGconsideredtheEPA’suseofthemeandietaryfluorideintake,ratherthanahighpercentilefluorideintake,at1.9mgF/LindrinkingwatertointerpretfluorideintakesatthecriticalfluorideconcentrationdidnotprovidearobustbasistoderiveanUpperLevelofIntakeforfluoride.
Theaveragefluorideintakewascalculatedforarangeofchildren’sagesandtheirassociatedbodyweightsatafluorideconcentrationof1.0mgF/Lindrinkingwater.ThecurrentAdequateIntakeof0.05mgF/kgbw/daywasreaffirmedtobeanintakelikelytobeassociatedwithappreciablyreducedratesofdentalcaries.AnAIwasnotestablishedforinfantslessthan6monthsofage,asfluidsforthemajorityoftheseinfantswereassumedtobebreastmilk.
TheUpperLevelofIntakeoffluoridewascomparedwithestimatedtotaldailyfluorideintakes(fluid,foodandingestedtoothpaste)forAustralianandNewZealandchildrenlivinginareaswith1.0mgF/Linthewatersupply.Theupperrangeofthetotaldailyfluorideintakeestimateswas0.10to0.14mgF/kgbw/dayacrossdifferentagegroupsconsidered,whichisconsiderablylowerthantheestablishedUpperLevelofIntakeoffluorideof0.2mgF/kgbw/day.
ThenewreferencebodyweightdataforAustralianandNewZealandpopulationswasusedtoderivetherecommendationsonaperdaybasisfromtheUpperLevelofIntakeoffluorideof0.2mgF/kgbw/dayforchildrenaged4-8years.ThemostrecentUSreferencebodyweightdatawereusedforinfantsandchildrenaged1-3yearsasnosuitableAustralianandNewZealanddatawereavailablefortheseagegroups(NRC2005,AppendixB).

4 AustralianandNewZealandNutrientReferenceValuesforFluoride
UpperLevelofIntake
Age Meanbw(kg) UL
Infants0–6months 6 1.2mg/day
7–12months 9 1.8mg/day
Children1–3years 12 2.4mg/day
4–8years 22 4.4mg/day
TheAdequateIntakeoffluorideforchildrenupto8yearsoldof0.05mgF/kgbw/dayisequivalenttothefollowingintakesexpressedasmgF/day,usingthesamereferencebodyweightdataasfortheUL.
AdequateIntake Age Meanbw(kg) AI
Infants0–6months 6 Notapplicable
7–12months 9 0.45mg/day
Children1–3years 12 0.6mg/day
4–8years 22 1.1mg/day
TheEWGconsidersthereisaModeratedegreeofcertaintyintheestimatesoftheAIandUL,usingtheGRADEsystem.StrengthsoftheevidenceincludethelargenumberofchildrenincludedintheDeanobservationalstudies,thewiderangeofdrinkingwaterfluorideconcentrationsreported,thecleardoseresponserelationshipsfoundbetweenthewaterfluorideconcentrationsanddentalcariesorfluorosisandtheabsenceofpotentialconfoundingfactorsthatarepresentinlaterstudiesfromtheuseoffluoridatedwatersupplies,andtoothpaste,supplementsanddentaltreatmentscontainingfluoride.TheseissuessupportincreasingtheratingbasedonthestrengthoftheevidencefromtheusualLowforevidencefromobservationalstudiestoModerate.AlthoughdataforfoodandfluidconsumptionandbodyweightswerenotdirectlyavailablefromtheDeanstudiesandhadtobedrawnfromothersources,thethreesourcesofinformationusedforthispurposeprovidedconsistentresultsandhadgoodprecision.
TheseestimateshavenoimplicationsforcurrentdrinkingwaterstandardsinAustraliaandNewZealandorforactiononfluorideintakefromtheingestionoftoothpaste.
FutureworkincludesthereviewofexistingULsandAIsforolderchildrenandadults,includingpregnantandlactatingwomen.

5 AustralianandNewZealandNutrientReferenceValuesforFluoride
SummaryofRecommendations
Fluorideiswidespreadinnatureandanormalpartofthehumanbody.Itisparticularlyconcentratedinteethandboneandhelpsformtoothenamel.Fluorideisingestedfromseveralsourcesincludingfoods,fluoridatedandunfluoridatedwater,fluoridatedtoothpastesandsomedietarysupplements.Bothinadequateandexcessivefluorideintakescanaffectdentalhealth.Inadequateintakesareassociatedwithincreasedtoothdecay(dentalcaries)andexcessiveintakeswithdamagetotoothenamel(dentalfluorosis).
NutrientreferencevalueswereestablishedforfluoridebyNHMRC/MoHin2006followingareview,whichdrewonanearlierreviewbytheUSInstituteofMedicinein1997.Nutrientreferencevaluesareguidestodietaryintakesthathelptoprotectpopulationsandindividualsagainstdeficiencydiseaseand,insomecases,againstexcessivenutrientintakes.Inthe2006review,bothAdequateIntakes(AI)andUpperLevelsofIntake(UL)wereestablishedforfluorideintakefordifferentagegroups.
RecentestimatesofdietaryfluorideintakeinAustraliaandNewZealandhavesuggestedthatthefluorideintakeofasubstantialproportionofinfantsandyoungchildrenmayexceedtheUL.Atthesametime,thereisnoevidenceofwidespreadoccurrenceofmoderateorseveredentalfluorosis.ThissuggeststhattheexistingULneedsreconsideration.
Thisreportexaminesevidencefromthe1997InstituteofMedicinereviewandsevenothermajorreviewsoffluoridereleasedsincethe1997reviewandfromasystematicreviewofpost-2005scientificliteratureonfluorideintakesandoralhealth.Fromthisexaminationofrelevantevidence,aULandanAIforfluorideweredeterminedforchildrenupto8yearsofage.
AsthisreportwasapilotforfutureNRVreviews,itwaslimitedtoconsideringchildrenupto8yearsofage,thecriticalagegrouptoconsiderfordentalcariesandfluorosis.
Dentalfluorosiswaschosenasthekeymeasureofexcessfluorideintakeanddentalcariesasthemeasureoffluorideadequacy.Thesemeasuresareconsistentwiththoseusedinothermajorreviews.ThesereviewsshowedthecentralroleofobservationaldatacollectedintheUSinthelate1930s-40sforestimatingdose-responserelationshipsbetweenthepresenceofdentalcariesordentalfluorosisandtheconcentrationoffluorideinthewatersupply.Thesystematicliteraturereviewdidnotfindanymorerecentdata,observationalorexperimental,thatcouldreplaceit.
BasedontheseUSdata,thereportidentifiesthecriticalfluorideconcentrationsinthewatersupplyforoptimisingpreventionofdentalcariesandforminimisingseveredentalfluorosis:1.0mgfluoride/litreand1.9mgfluoride/Lrespectively.Fromthesevalues,togetherwithnationallyrepresentativedataonwaterandfoodconsumptionandbodyweightdataforAustralianandNewZealandpopulations,theUpperLevelofIntakeoffluorideforinfantsandchildrenupto8yearsoldwasestimatedtobe0.2mgfluoride/kgbodyweight/day.TheAdequateIntakewasreaffirmedtobe0.05mgF/kgbodyweight/day.NewreferencebodyweightdataforAustralianandNewZealandchildrenaged4yearsandabovewereusedtodeterminenewvaluesfortheAIandULexpressedinmgF/day;themostrecentUS

6 AustralianandNewZealandNutrientReferenceValuesforFluoride
referencebodyweightdatawereusedforinfantsandchildrenaged1-3yearsasnoAustralianandNewZealanddatawereavailablefortheseagegroups.
TheEWGconsidersthereisaModeratedegreeofcertaintyintheestimatesoftheAIandUL,usingtheGRADEsystem(seeAppendix1).StrengthsoftheevidenceincludethelargenumberofchildrenincludedintheUSobservationalstudy,thewiderangeofdrinkingwaterfluorideconcentrationsreported,thecleardoseresponserelationshipsfoundandtheabsenceofpotentialconfoundingfactorsthatarepresentinlaterstudiesfromtheuseoffluoridatedwatersupplies,andtoothpaste,supplementsanddentaltreatmentscontainingfluoride.TheseissuessupporttheratingupthestrengthoftheevidencefromtheusualLow,forevidencefromobservationalstudies,toModerate.AlthoughdataforfoodandfluidconsumptionandbodyweightswerenotdirectlyavailablefromtheUSstudyandhadtobedrawnfromothersources,thethreesourcesofinformationusedforthispurposeprovidedconsistentresultsandhadgoodprecision.
TheEWGstronglyrecommendstheadoptionofthesevaluesfortheULandAIforAustralianandNewZealandchildrenagedupto8years.
TheseestimateshavenoimplicationsforcurrentdrinkingwaterstandardsinAustraliaandNewZealandorforactiononfluorideintakefromingestionoftoothpaste.
RecommendedfutureworkincludesthereviewofexistingULsandAIsforolderchildrenandadults,includingpregnantandlactatingwomen.
7 AustralianandNewZealandNutrientReferenceValuesforFluoride
1. Introduction
1.1 Fundingsource
ThisreviewhasbeenfundedbytheAustralianDepartmentofHealthandtheNewZealandMinistryofHealth.
1.2 UseofNutrientReferenceValues
NutrientReferenceValues(NRVs)areasetofrecommendednutrientintakesdesignedtoassistnutritionandhealthprofessionalsassessthedietaryrequirementsofindividualsandgroups.Publichealthnutritionists,foodlegislatorsandthefoodindustryalsousetheNRVsfordietarymodellingand/orfoodlabellingandfoodformulation.
ThecurrentNRVsforAustraliaandNewZealandwerepublishedin2006afteracomprehensivereviewprocessoftheRecommendedDietaryIntakes(theonlytypeofnutrientreferencevaluethathadbeenproducedatthetime),commissionedbytheDepartmentofHealth(Health)inconjunctionwiththeNewZealandMinistryofHealth(NZMoH).
ThereviewresultedinanewsetofrecommendationsknownastheNutrientReferenceValuesforAustraliaandNewZealand(2006).TheNationalHealthandMedicalResearchCouncil(NHMRC)carriedoutthe2006reviewandrecommendedthattheseguidelinesbereviewedeveryfiveyearstoensurevaluesremainrelevant,appropriateanduseful.
In2011Health,inconsultationwiththeNZMoH,commissionedascopingstudytodeterminetheneedandscopeforareviewofNRVs.Thescopingstudyconsidereddevelopmentsincomparablecountries,expertopinions,stakeholderconsultationandpublicsubmissions.Thescopingstudyconcludedtherewassufficientjustificationforconductingareviewandasaresult,HealthandtheNZMoHengagedNousGroupandatechnicalteamledbyBakerIDI,todevelopaMethodologicalFrameworktoguidefutureNRVreviews.
ASteeringGroupisoverseeingthereviewprocessandisresponsibleforallstrategic,fundingandtechnicaldecisionsofthereview.Itconsistsofrepresentativesfrombothfundingagencies,HealthandtheNZMoH,withtheNHMRCasanobserver.TheSteeringGroupisalsoresponsiblefortheongoingmonitoringoftriggersforanewreview,andensuringnutrientreviewsareconductedinatimelymanner.
ReviewsarebeingconductedonarollingbasistoensureNRVsremainrelevantandappropriate.Theprocesscomplieswiththe2011NHMRCProceduresandrequirementsformeetingthe2011NHMRCstandardforclinicalpracticeguidelines.
TheDOHappointedanAdvisoryCommitteeasanexpertreferenceandadvisorygroupwhichalsoactsasanindependentmoderatorofnutrientrecommendations.
8 AustralianandNewZealandNutrientReferenceValuesforFluoride
TheAdvisoryCommitteecomprisesmemberswithabroadrangeofexpertise,includingexpertsintheareasofmicronutrients,toxicology,publichealth,enduserneeds,research,chronicdisease,nutritionandmacronutrientsfromAustraliaandNewZealand.
ThescopingstudyalsoidentifiedtherationaleandtriggersforreviewingspecificnutrientsincludingchangesordevelopmentstoNRVsincomparableOECDcountries,emergenceofnewevidence,impactonpublichealthprioritiesand/orconcernsregardingthestrengthoftheunderlyingmethodologyorevidence.FluoridewasidentifiedasaprioritynutrientforreviewandthishasbeenfundedbyHealthandNZMoH.
TheHealth(withtheadvicefromNZMoHandtheAdvisoryCommittee),establishedagroupofexpertstoconductthisfluoridereview.TheExpertWorkingGroupwasprimarilyresponsibleforexaminingscientificevidenceandestablishingnutrientvalues.
MembershipofthegroupsinvolvedinthedevelopmentoftheNRVguidelinescanbefoundinSection5.
ThesuiteofNRVtermsoutlinedinthe2006document(NHMRC2006),adaptedfromtheUS/CanadianDietaryReferenceIntakes(DRIs),wereconsideredtoremainapplicablefortheNRVreviewswithnochangeofnametothereferenceindicators(NHMRC2006,NousGroup2013).

9 AustralianandNewZealandNutrientReferenceValuesforFluoride
NRVtermsEAR EstimatedAverageRequirementAdailynutrientlevelestimatedtomeettherequirementsofhalfthehealthyindividualsinaparticularlifestageandgendergroup.
RDI RecommendedDietaryIntakeThedailyintakelevelthatissufficienttomeettherequirementsofnearlyall(97–98%)healthyindividualsinaparticularlifestageandgendergroup.
AI AdequateIntakeTheaveragedailynutrientintakelevelbasedonobservedorexperimentallydeterminedapproximationsorestimatesofnutrientintakebyagroup(orgroups)ofapparentlyhealthypeoplethatareassumedtobeadequate.
EER EstimatedEnergyRequirement
Theaveragedietaryenergyintakethatispredictedtomaintainenergybalanceinahealthyadultofdefinedage,gender,weight,heightandlevelofphysicalactivity,consistentwithgoodhealth.Inchildrenandpregnantandlactatingwomen,theEERistakentoincludetheneedsassociatedwiththedepositionoftissuesorthesecretionofmilkatratesconsistentwithgoodhealth.
UL UpperLevelofIntake
Thehighestlevelofnutrientintakelevellikelytoposenoadversehealtheffectstoalmostallindividualsinthegeneralpopulation.AsintakeincreasesabovetheUL,thepotentialriskeffectincreases.
AMDR AcceptableMacronutrientDistributionRange
Anestimateoftherangeofintakeforeachmacronutrientforindividuals(expressedaspercentcontributiontoenergy),whichwouldallowforanadequateintakeofalltheothernutrientswhilstmaximisinggeneralhealthoutcome.
SDT SuggestedDietaryTarget
Adailyaverageintakefromfoodandbeveragesforcertainnutrientsthatwillhelpinpreventionofchronicdisease.
10 AustralianandNewZealandNutrientReferenceValuesforFluoride
1.3 Summaryof2006NRVsforFluoride
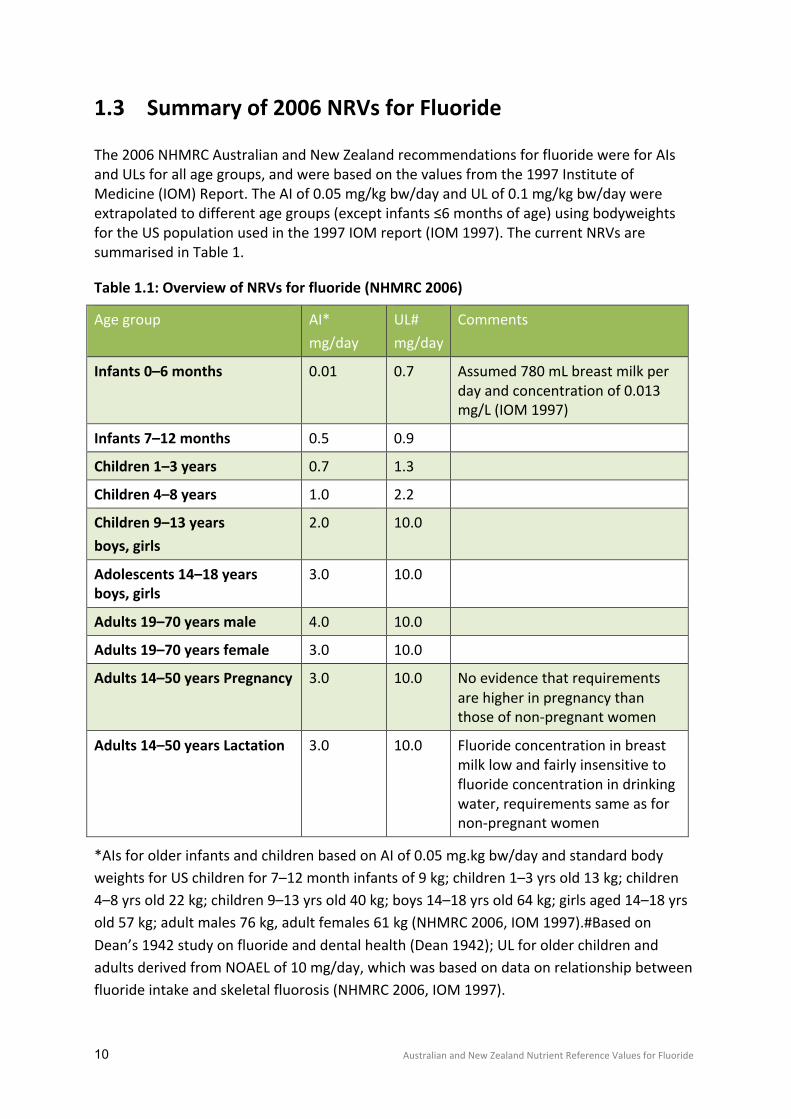
The2006NHMRCAustralianandNewZealandrecommendationsforfluoridewereforAIsandULsforallagegroups,andwerebasedonthevaluesfromthe1997InstituteofMedicine(IOM)Report.TheAIof0.05mg/kgbw/dayandULof0.1mg/kgbw/daywereextrapolatedtodifferentagegroups(exceptinfants≤6monthsofage)usingbodyweightsfortheUSpopulationusedinthe1997IOMreport(IOM1997).ThecurrentNRVsaresummarisedinTable1.
Table1.1:OverviewofNRVsforfluoride(NHMRC2006)
Agegroup AI*mg/day
UL#mg/day
Comments
Infants0–6months 0.01 0.7 Assumed780mLbreastmilkperdayandconcentrationof0.013mg/L(IOM1997)
Infants7–12months 0.5 0.9
Children1–3years 0.7 1.3
Children4–8years 1.0 2.2
Children9–13yearsboys,girls
2.0 10.0
Adolescents14–18yearsboys,girls
3.0 10.0
Adults19–70yearsmale 4.0 10.0
Adults19–70yearsfemale 3.0 10.0
Adults14–50yearsPregnancy 3.0 10.0 Noevidencethatrequirementsarehigherinpregnancythanthoseofnon-pregnantwomen
Adults14–50yearsLactation 3.0 10.0 Fluorideconcentrationinbreastmilklowandfairlyinsensitivetofluorideconcentrationindrinkingwater,requirementssameasfornon-pregnantwomen
*AIsforolderinfantsandchildrenbasedonAIof0.05mg.kgbw/dayandstandardbodyweightsforUSchildrenfor7–12monthinfantsof9kg;children1–3yrsold13kg;children4–8yrsold22kg;children9–13yrsold40kg;boys14–18yrsold64kg;girlsaged14–18yrsold57kg;adultmales76kg,adultfemales61kg(NHMRC2006,IOM1997).#BasedonDean’s1942studyonfluorideanddentalhealth(Dean1942);ULforolderchildrenandadultsderivedfromNOAELof10mg/day,whichwasbasedondataonrelationshipbetweenfluorideintakeandskeletalfluorosis(NHMRC2006,IOM1997).

11 AustralianandNewZealandNutrientReferenceValuesforFluoride
1.4 Triggersandrationaleforreview
TheAustralianDrinkingWaterGuidelinesandNewZealandDrinkingWaterStandardsbothrecommendwaterfluoridationlevelsintherangeof0.7–1.0mgF/Lwithamaximumlevelinbothcountriesof1.5mg/L(NHMRC2013,MOH2005).However,itisnotedthatintheNHMRC2007statementonthesafetyandefficacyoffluoridation,itisrecommendedthatwaterbefluoridatedintherange0.6-1.1mg/L,dependingonclimate,tobalancethereductionofdentalcariesandoccurrenceofdentalfluorosis(NHMRC2007).
ThereisAustralian,NewZealandandinternationalevidencethatestimatedfluorideintakesforasizeableminorityofthepopulationwhoconsumedrinkingwateratoptimallevelsoffluoridation(1.0mgF/L)areabovetheULforfluoride(0.1mg/kgbw/day)(FSANZ2009).Yetneithercountryexperiencesmorethantherareoccurrenceofmoderateorseveredentalfluorosis.ThisapparentexceedanceofrecommendedfluorideintakelevelswithouttheoccurrenceofadversedentalfluorosiscreatedtheconundrumaroundNRVsforfluoridetowhichthisreportresponds.
Thissituationcallsforare-evaluationofthedatawhichunderpinsthecurrentUL.AspartofthisreviewanevaluationoftheAIwasalsoincludedforcompleteness.AsthisreportwasapilotforafutureNRVreviews,itwaslimitedtoconsideringchildrenupto8yearsofage,thecriticalagegrouptoconsiderfordentalcariesandfluorosis.
1.5 Backgroundinformation-fluoride
Fluorideisnaturallypresentinthefoodanddrinkweconsumeandisconsideredtobeanormalconstituentofthehumanbody.Thefluorideconcentrationinbonesandteethisabout10,000timesthatinbodyfluidsandsofttissues(Bergmann&Bergmann1991;1995).Nearly99%ofthebody’sfluorideisboundstronglytocalcifiedtissues.Fluorideinboneappearstoexistinbothrapidly-andslowly-exchangeablepools.
Fluorideavailablesystemicallyduringtoothdevelopmentisincorporatedintoteethasfluorapatiteintoothenamel.Fluorapatiteintoothenamelaltersitscrystallinestructure,reducingthesolubilityofenameltoaciddissolution,ordemineralization.Athigherfluorideintakesthecrystallinestructuremaybedisruptedformingporositieswhicharethebasisofdentalfluorosis.Outcomesoffluorideintakeonbonehavebeenconsidered,especiallyamongadults.However,outcomessuchasskeletalfluorosisandbonefracturesoccuronlyafterprolongedexposuretoveryhighfluorideintakes.
Fluorideatthesurfaceofenamelcanalsoformcalciumfluoride,amorerapidly-exchangeablepooloffluoridetoalterthedemineralization-remineralizationbalancewhichisthedynamicprocessunderlyingdentalcaries.DentalcariesisalargelypreventablebuthighlyprevalentchronicdiseaseinAustralianandNewZealandchildrenandadults.
AustraliaandNewZealandhavepursuedpublichealthpolicytoadjustfluorideintakeatthepopulationlevelwiththeaimofpreventingdentalcarieswithoutcausingmoderateorseveredentalfluorosiswithadverseeffects.Itisconsidereddesirabletohaveafluoride

12 AustralianandNewZealandNutrientReferenceValuesforFluoride
intakethatissufficienttopreventmuchdentalcaries(anAI)withoutexceedingintakesthatareassociatedwithmoderateorseveredentalfluorosis(aUL).
13 AustralianandNewZealandNutrientReferenceValuesforFluoride
2. ScopeandPurpose
ThepurposeofthisreviewwastodiscussandderiveaULandanAIforfluorideintakeforinfantsandyoungchildren,byconductingasystematicreviewofrelevantliteraturereleasedsincethe2006NHMRCreviewandbyconsideringrecentinternationalreviewsinthiscontext.
Basedonthisconsideration,thereviewdeterminedthecriticalfluorideconcentrationindrinkingwatertominimisebothdentalcariesandseveredentalfluorosis.Fromthis,usingnationallyrepresentativedataforfluidandfoodconsumptionandbodyweightdataforAustralianandNewZealandpopulations,aULandanAIforfluoride,expressedinmgF/bw/day,werederived.Finally,recommendationsforrevisedULandAIvalues,expressedinmgF/dayfordifferentagegroups,weredetermined.TheEWGnotedtheterm‘TolerableUpperLevelofIntake’wasanappropriatewaytodescribetheULforfluoridethatwasconsistentwithuseinternationallyinthatfluorideisnotanessentialnutrient,however,tomaintainconsistencywiththeestablishmentofNRVsforothernutrientsinAustraliaandNewZealand,theterm‘UpperLevelofIntake’wasretainedforfluoride.
ThisreportisrestrictedtodiscussionandderivationofrelevantNRVsforfluoride(ULandAI)forinfantsandyoungchildrenupto8yearsofage,whoweredeterminedtobethetwocriticalgroupsforreconsideration.TimeandresourcesavailableforthetaskrestrictedthescopeoftheworktobeundertakenandincludedinthisreportbytheEWG;itwasnotpossibletoassessAIsorULsforolderchildrenoradults.
TheEvidenceReviewinsection3setoutthereviewprocessandfindings,withfurtherdetailprovidedinSupportingDocuments1-4.TherecommendationsfortheULandAIforfluorideininfantsandyoungchildrenaresetoutinsection4.
NoissuesspecifictoAboriginalandTorresStraitIslanderpeopleinAustraliaortoMaoriandPacificIslanderpeopleinNewZealandhavebeenidentifiedinthisreport.
14 AustralianandNewZealandNutrientReferenceValuesforFluoride
3. EvidenceReview
3.1 Fluorideintakeestimatesininfantsandyoungchildren
3.1.1 AustraliaandNewZealand
ThereisAustralian,NewZealandandinternationalevidencethatestimatedfluorideintakesforasizeableminorityofthepopulationwhoconsumedrinkingwateratoptimallevelsoffluoridation(1.0mgF/L)areabovetheULforfluorideof0.1mg/kgbw/day(FSANZ2009,NHMRC2013,MOH2005).Yetneithercountryexperiencesmorethantherareoccurrenceofmoderateorseveredentalfluorosis.ThisapparentexceedanceofrecommendedfluorideintakelevelswithouttheoccurrenceofadversedentalfluorosiscreatedtheconundrumaroundNRVsforfluoridetowhichthisEvidenceReviewresponds.
FoodStandardsAustraliaNewZealand(FSANZ),whenconsideringthevoluntaryadditionoffluoridetopackagedwaterin2009,foundthatinfantsandchildrenundertheageof8yearsconsumingfluoridatedwaterwerethegroupmostlikelytoexceedtheULforfluorideof0.1mg/kgbw/dayassetbyNHMRCin2006(FSANZ2009a,NHMRC2006).Allinfantsfedsolelywithinfantformulamadewithnon-fluoridatedorfluoridatedwaterhadestimatedfluorideintakesthatexceededtheUL.Forinfantsaged6–12monthsconsumptionoffluoridatedwaterontopofdietaryfluoridesources,includinginfantformula,increasedestimatedfluorideintakeovertheUL.Some22%of2–3yearoldAustralianchildrenand5%of4–8yearoldAustralianchildrenhadestimatedfluorideintakesthatexceededtheULwhenassumingthatallwaterconsumedwasfluoridatedatthemaximumlevelof1.0mgF/L(FSANZ2009a).
Cresseyetal.in2010updatedtheestimatesforfluorideintakeinNewZealandusinganalyticaldataforthefluoridecontentoffoodsfromtheNZTotalDietSurveyin1990/91,whichanalysedfluoridecontentoffoodsandusedasimulatedtypicaldiettoestimateintake(Cresseyetal.2010).CresseyfoundthatformanytheestimatedmeanfluorideintakewasbelowtheAIof0.05mg/kgbw/dayforoptimalcariesprotection(Cresseyetal.2010).Allgroupsexcept6–12montholdinfantslivinginfluoridatedareasandassuminguseofhighfluoridetoothpastehadestimatedfluorideintakesbelowtheUL(0.1mg/kgbw/day).Whileinfantsconsumingformulapreparedwithfluoride-freewater(deionisedwater)hadintakeswellbelowtheUL,asizableproportionofinfants,assuminguseofwaterwithfluorideconcentrationsof0.7or1.0mgF/L,hadestimatedfluorideintakesthatexceededtheUL(30%and90%respectively).
Cliffordetal.in2009studiedfluorideintakefrominfantformulaavailableinAustraliaandfoundthatinfantformulapowderscontainedloweraveragelevelsoffluoridein2006-07(0.07mg/kg)thanthatreportedbySilvain1996(0.24mg/kg),adecadeearlier(Cliffordetal.2009,Silvaetal.1996).Usingthesenewdata,revisedfluorideintakesforinfantswereestimatedbyFSANZforthisreviewfollowingrecommendedfluidintakes.Wheninfantformulawasreconstitutedwithwaterwithnofluoride,theULwasnotexceeded.However

15 AustralianandNewZealandNutrientReferenceValuesforFluoride
whensomeformulaewerereconstitutedwithfluoridatedwater,theULwasexceeded,especiallyfor0-3montholdinfants(FSANZ2014).
SupportingDocument1providesmoredetailonfluorideintakeestimatesforAustralianandNewZealandinfantsandyoungchildren.
3.1.2 International
Anumberofstudieshavecomparedestimatedfluorideintakeagainstlong-standingrecommendationsoffluorideintake.TheserecommendationswerebasedonanaveragefluorideintakeestimatedbyMcClure(1943)of0.05mg/kgbw/dayforchildrenwith1.0mgF/Linthewatersupply,alsoexpressedasarangefrom0.05–0.07mg/kgbw/day.Thisisoftenreferredtoastherecommended‘optimal’doserange,terminologythatreportedlyemergedasarecommendationfromFarkasandFarkasandlaterwasacceptedbyOphaugetal.(FarkasandFarkas1974.Ophaugetal.1980).
ErdalandBuchananstudiedtheestimatedaveragedailyintakeoffluorideintheUnitedStatesofAmerica,viaallapplicableexposurepathwayscontributingtodentalfluorosisriskforinfantsandchildrenlivinginhypotheticalfluoridatedandnon-fluoridatedcommunities(ErdalandBuchanan2005).Theyalsoestimatedhazardquotientsandindicesforexposureconditionsrepresentativeofcentraltendencyexposure(CTE)andreasonablemaximumexposure(RME).Forinfants<1yearofageinareasofwaterfluoridation(1.0mgF/L),thecumulativedailyfluorideintakewasestimatedtobe0.11and0.20mg/kgbw/dayfortheCTEandRMEscenariosrespectively.Inolderchildren(3–5yearsofage)underthesameconditions,theCTEandRMEfluorideintakewasestimatedasbeing0.06and0.23mg/kgbw/day,respectively.Ininfantsthemajorsourceoffluoridewasinfantformulaandthefluoridatedwaterusedtoreconstituteit.Inolderchildrenthemainsourcewasinadvertentingestionoftoothpastefluoridatedat1000mgF/kg.
Reportingthattheirestimateswereingoodagreementwithmeasurement-basedestimates,ErdalandBuchananfoundthatCTEestimateswerewithintherecommendedrangefordentalcariesprevention,buttheRMEestimateswereabovetheTolerableUpperIntakeLimitestablishedbytheUSEnvironmentalProtectionAgencyatthattime(recommendedsafethresholdof0.06mg/kgbw/day;lowerboundvalue0.05mg/kgbw/day,upperboundvalue0.07mg/kgbw/day).Thissuggestedsomechildrenwereatriskofadversedentalfluorosis(ErdalandBuchanan2005).
TheIowaFluorideStudy(Hongetal.2006,Warrenetal.2009)examinedfluorideintakeacrossthefirst36monthsoflifeanditsassociationwithanydentalfluorosis(includingverymildchangestoonlyafractionofthesurfaceofkeyteeth).Hongetal.reportedthatfluorosisprevalencewasrelatedtoelevatedfluorideintakewhenaveragedoverthefirst3yearsoflife,butwasevenmorestronglyrelatedtofluorideintakethatwaselevatedforallofthefirst3yearsoflife.However,Warrenetal.reportedontheconsiderableoverlapinthefluorideintakeofchildrenintheIowaFluorideStudywithandwithoutdentalfluorosiswithupto20%ofchildrenwithfluorideintakesabovetherecommendedlevelof0.05mg/kgbw/day,somebyseveraltimesthislevel,whereseveredentalfluorosiswasnotobserved.

16 AustralianandNewZealandNutrientReferenceValuesforFluoride
Colombianresearchreportedin2005examinedthetotalfluorideintakeofchildrenaged22–35monthsinfourColumbiancities.Francoetal.usedtheduplicateplatemethodandrecoveryoftoothpasteusedintoothbrushing.Toothpasteaccountedforapproximately70%offluorideintake,followedbyfood(24%)andbeverages(<6%)(Francoetal.2005a).Meandailyfluorideintakewashigherinchildrenfromhighsocio-economicstatusbackgroundsinseveralcities.Manychildrenhadtotalfluorideintakesabovetherecommendedrange(i.e.,above0.05–0.07mg/kgbw/day).ArelatedpaperbyFrancoetal.includedafocusonfluoridatedtablesalt.ItconcludedthatpreschoolchildrenresidinginColumbianurbanareaswereingestingamountsoffluorideabovetheupperboundoftheEPArecommendedsafethreshold(0.07mg/kgbw/day)(Francoetal.2005b).
Fluorideintakefromtoothpasteanddietin1–3yearoldBrazilianchildrenwasreportedbydeAlmeidaetal.in2007.Amonglownumbersofchildreninfluoridatedandnon-fluoridatedareas,fluorideintakewasmonitoredbydirectmeasurementoffluoridedispensedandrecoveredduringtoothbrushingandtheduplicateplatemethodforfoods.FluorideintakewasabovetheupperboundoftheEPArecommendedsafethresholdfordentalfluorosis(>0.07mg/kgbw/day).Toothpastewasresponsibleforanaverageof81.5%ofdailyfluorideintake(deAlmeidaetal.2007).
ThisresearchinBrazilwasfollowed-upbyMiziaraetal.in2009whostudiedfluorideintakeamong2–6yearoldchildreninafluoridatedcommunityusingafoodfrequencyapproachandestimatedfluorideintakefromfluoridatedtoothpaste.Amongthechildrenevaluated,31.2%wereestimatedtohaveanintakeoffluorideabovethesafethresholdfordentalfluorosis(>0.07mg/kgbw/d)(Miziaraetal.2009).
Nohnoetal.in2011studiedthefluorideintakeofJapaneseinfantsfrominfantformula.Eachinfantformulapowderwasreconstitutedwithdistilledwaterorwaterwith0.13mgF/Landfluorideintakeestimatedfrommodeldiets.Thepotentialfluorideintakeofaninfantdependedonthefluoridelevelofthewaterusedtoreconstitutetheformula.RiskoffluorosiswasdeemedtobelowasmostJapanesewatersuppliesarelowinfluoride.HowevertherewasapossibilityofexceedingtheTolerableUpperIntakeLevelreferredtointheirpaper,especiallyforinfantswithinthefirst5monthsoflife(Nohnoetal.2011).
ThesameapproachwaspursuedbySiewetal.inUSbasedresearch(Siewetal.2009).Theydeterminedtheconcentrationsoffluorideinformulaandestimatedthefluorideintakeofinfantsconsumingpredominantlyformulaagainstvariousconcentrationsoffluoridatedwater.Theybasedconsumptionvolumesonpublishedrecommendations.Theyconcludedthatsomeinfantsbetweenbirthand6monthsofage,whoconsumepowderedandliquidconcentrateformula,reconstitutedwithwatercontaining1.0mgF/L,werelikelytoexceedtheUpperLevelofIntakeforfluoride.
Sohnetal.examinedfluidintakesof1–10yearoldsintheUSAviaa24hourrecalldietsurveyaspartofthethirdNationalHealthandNutritionExaminationSurvey1988–94(Sohnetal.2009).Theamountoffluorideingestedfromfluidswasestimatedfromseveralassumptionsabouttheconcentrationoffluorideindrinkingwaterandbeverages.Theestimatedfluorideintakeatthe75thpercentile(0.05mg/kgbw/dayormore)and90thpercentile(0.07mg/kgbw/dayormore)heldacrossallagegroups.Somechildrenwereingestingsignificantlymorefluoridethanothersdependingonsocio-demographicfactors

17 AustralianandNewZealandNutrientReferenceValuesforFluoride
andfluidconsumptionpatterns.Sohnetal.calledforadditionalresearchonfluorideingestionanditsimpactondentalfluorosis.
Morerecentpublishedinformationonfluorideintakeexplorestheingestionoffluoridatedtoothpasteby4-6yearoldsbyZohoorietal.(Zohoorietal.2012).Thefluorideintakeof4–6yearoldsfromfluoridatedtoothpastewasstudiedintheNewcastleareaoftheUK.Theresearchinvolvedalownumberofsubjects.Whiletheaverageamountoffluoridatedtoothpasteusedperbrushingwasmorethantwicetherecommendedamount(0.25g),onlyonechild(outof61)hadadailyfluorideintakethatexceededtheTolerableUpperLevelofIntakeof0.1mg/kgbw/dfortheiragegroup(fromtoothpastealone).
InasubsequentpublicationbyZohoorietal.(Zohoorietal.2014),fluorideintakewasestimatedforinfants1–12monthsoldlivinginfluoridatedandnon-fluoridatedareasoftheUKviaa3dayfooddiarycoupledwithanalysisofthefluoridecontentoffoodsanddrinksconsumed.Totaldailyfluorideintakewasestimatedfromdiet,plusfluoridesupplementsandfluoridatedtoothpastewhereused.Theconclusionwasthatinfantslivinginfluoridatedareasmayreceiveafluorideintakefromdietonlyofmorethantherecommendedrangeof0.05-0.07mgF/kgbw/day.
3.2 Selectionofbiomarkersforfluoride
TheWorkingGroupconsideredarangeofbiomarkersforfluoride,selectingdentalcariesandfluorosisasthebiomarkerstousefortheNRVreviewforinfantsandyoungchildren.TheevidencetosupportthisdecisionisgivenbelowandinSupportingDocument2.AsummaryofotherbiomarkersconsideredaspartofthescopingprocessbutnotusedinthisNRVreviewisgivenbelow.
3.2.1 Dentalcaries
Dentalcariesistheresultofaninteractionofbiologicalandenvironmentalprocesses(Holstetal.2001).Thebiologicalprocessisdefinedbythedemineralizationanddestructionofdentalhardtissuesbyacidicby-productsfrombacterialfermentationofdietarycarbohydrates,mainlysucrose(Selwitzetal.2007).Theenvironmentalprocessisacombinationofbehaviour,contextualandsocietalfactors(Holstetal.2001).Theaetiologyofdentalcariesiscomplexandinvolvesdifferentlevelsofdeterminantsfromsocialstructure,socalleddistaldeterminants,tointermediatedeterminantssuchasbehavioursanddentalcareutilisation,whichinturnaffectsmoreproximaldeterminants,suchasdentalbiofilm,fluorideexposure,andsalivaflowandcomposition.Cariesisadynamicprocessofdemineralizationandremineralisationofthetoothtissuesbutthemajorityofthelesions,particularlyinpermanentteeth,progressslowlythroughenameltodentine(Mejareetal.1998)andcanbeseeninthecrownoftheteethintheprimaryandpermanentdentitionandrootsurfacesofteethinthepermanentdentition.
Dentalcariesisamajorpublichealthproblemworldwide,itisoneofthemostprevalentpreventablechronicdiseases(Vosetal.2012),andthemostcommonchronicchildhooddiseaseinmostindustrializedcountries,affecting60–90%ofschoolchildren(Petersen2003).Despiteimprovementinthelastdecadesindevelopedcountries,recentstudiesshowedthat
18 AustralianandNewZealandNutrientReferenceValuesforFluoride
cariesintheprimarydentitionisincreasingintheUSA,UK,Canada,Australia,NorwayandtheNetherlands(Gaoetal.2010).
Alongwithitshighprevalenceandfinancialburdenforsociety,dentalcariesisthemaincauseoftoothacheinchildren(Boeiraetal.2012)anditisthemainreasonfortoothextraction,resultingintoothloss,amongadults.Theexperienceofpain,chewingdifficulties,restrictionofsomefoodsandproblemswithsmilingandcommunicationduetodamagedteeth,haveanimportantimpactonpeople’slivesandwell-being(Petersenetal.2005).
Themeasurementofdentalcarieshaslargelyremainedunchangedsincethe1930s.WhilstDeanandcolleaguesusedslightlydifferentnomenclature,theywereessentiallyrecordingtheprevalenceofcariesinthepermanentdentition(i.e.,oneormoreteethwithcariesexperience)amongchildren12–14yearsoldandthenumberofteethwithdecay(D),missingbecauseofcaries(M),orfilled(F).ThenomenclatureoftheDMFTeethIndexhasbeensettledsincethelate1930s(Kleinetal.1938).RulesfortheobservationofdecayinatoothandtherecordingofteethmissingduetocarieshavebeenavailablefromtheWorldHealthOrganization(WHO2013).Sincethe1960sandonwardsrefinementstothesebasicmeasureswereintroduced.Thesehaveincludedvaryingtheunitofobservationincludingindividualtoothsurfacesandmorerecentlyobservingdecayatearlierthresholdsthancavitationordentineinvolvement.Thisreporthasstayedwiththedecayed,missing(duetocaries)andfilledprimary(dmft)andpermanent(DMF)teethindicesasthatprovidescontinuitywiththekeydatatoestablishadose-responserelationshipbetweenfluorideandcaries.
AsummaryoftheknownprevalenceandextentofdentalcariesintheAustralianandNewZealandchildpopulationsisgiveninTable3.1below.ThedatapresentedinTable3.1werederivedfromoralhealthsurveysallconductedinthe2000decade.ApproximatelyhalfofallchildreninAustraliaaged5–6yearsoldandinNewZealandaged5–11yearsoldhaveexperienceofcariesintheprimarydentitionandhaveonetotwoteethonaveragewithcariesexperience.Alowerproportionof12yearolds,approximately30%,haveexperienceofcariesinthepermanentdentitionandtheaveragenumberofteethwithcariesexperienceisbelowonetooth.Boththeprevalenceandexperience(dmftorDMFT)arestronglyage-relatedandshowvariationacrosssitesinAustralia,betweenthetwocountriesandbetweenareasthathavefluoridatedwaterornot.

19 AustralianandNewZealandNutrientReferenceValuesforFluoride
Table3.1:SummaryofdatafordentalcariesinAustralianandNewZealandchildren
Year dmft/DMFT %Cariesfree
Region Age(years)
Fluoridation(mg/Lwater)
Study
2010-12
dmft:2.75(2.16-3.34)dmft:(4.31(3.79-4.84)DMFT:0.82(0.65-0.99)DMFT:1.51(1.31-1.71)
63.1(59.2-66.4)*52.3(48.7-55.9)*70.6(67.2-73.9)*60.7(57.8-63.5)*
Queensland 5-85-89-149-14
FareaNon-FareaFareaNon-Farea
Do&Spencer2015Doetal.2015
2009 dmft:2.13(2.08–2.18)DMFT:1.05(1.01–1.08)
53.754.9
Australia,National(excludingNSW,VIC)
5–612
NSNS
Haetal.2013
2007 dmft:1.88(1.78–1.99)DMFT0.95(0.85–1.05)
50.269.4
Australia,National(excludingVic)
5–612
NSNS
Meijaetat2012
2007 dmft:1.40(1.22–1.58)dmft:2.62(1.89–3.36)DMFT:0.71(0.63–0.79)DMFT:0.98(0.75–1.21)
63.2(60.0–66.3)45.9(35.0–56.7)63.2(63.7–69.4)45.9(48.8–64.0)
NSW 5–65–611–1211-12
FareaNon-FareaFareaNon-Farea
COHSNSW2009
2005 dmft2.27DMFT1.11
na Australia,National(excludingNSW)
612
NSNS
Meijaetat2012

20 AustralianandNewZealandNutrientReferenceValuesforFluoride
Year dmft/DMFT %Cariesfree
Region Age(years)
Fluoridation(mg/Lwater)
Study
2003 dmft0.63(0.37–0.88)dmft0.95(0.57–1.32)DMFT0.33(0.13–0.54)
756179
NSW 6811
Farea Evansetal.2009
2009 dmft:0.8(0.3–1.2)dmft:1.9(1.5–2.3)DMFT:0.5(0.3–0.6)dmft+DMFT2.4(2.0–2.8)dmft+DMFT1.5(1.1–1.9)
79.7(71.7–87.7)51.0(53.2–58.8)75.0(71.4–83.5)nana
NZ,National 2–45-115-115–175-17
NSNSNSNon-FareasFareas
NZMoH2010
Notes:Farea=fluoridatedarea0.8–0.85mgF/L,NFarea=non-fluoridatedarea<0.2–0.3
mgF/L.
NS=notspecified.
Thedose-responserelationshipbetweenfluorideconcentrationinwatersuppliesanddentalcarieswasestablishedbyDeanandcolleaguesinthe21CitiesStudy(Deanetal.1941,1942)2.ThecurrentNRVsforfluorideestablishedinAustraliaandNewZealandandelsewhereforinfantsandchildrenwerebasedontheIOMrecommendations,whichwerederivedfromthispivotalstudy(IOM1997,NHMRC2006,EPA2010a,b,EFSA2013).ThevalueofDean’sstudyisthatitwasundertakenbeforewaterfluoridationprograms,fluoridatedtoothpasteanddentaltreatmentwithfluorideproductswereavailablesoitispossibletoexploretherelationshipbetweendentalcariesandthenaturalleveloffluorideintapwaterwithouttheseconfoundingfactors.FurtherresearchfollowedonfromDean’soriginalstudyondentalcariesandwaterfluoridation.ImportantreportsincludeGalagan
2Deanetal.studied26citiesinUSintotal;21citieswereselectedassuitableforthefluorideanddentalcariesresearch,aslightlydifferent
listof22citieswasselectedforthefluorideandfluorosisresearch.

21 AustralianandNewZealandNutrientReferenceValuesforFluoride
andVermillian(1957),EklundandStriffler(1980),Helleretal.(1997)andtwosystematicreviews-theYorkReview(McDonaghetal.in2000andRugg-GunnandDo(2012)3.AnumberofreportsonwardfromthelandmarkIOMreportin1997alsoprovideoverviewsofthedose-responserelationship,theEPAreviewin2006and2010(EPA2006,2010a,b)andtheECScientificCommitteeonHealthandEnvironmentalRiskReviewin2011(SCHER2011),aswellasresearchspecifictoAustraliaandNewZealand.FurtherdetailsontheresearchonthelinkbetweendentalcariesandfluoridelevelsinwatersuppliesissummarisedinSupportingDocument2andfromthesereportsisalsosummarisedinSupportingDocument3.
3.2.2 Fluorosis
Thedose-responseoffluorideinwatersuppliesandoralhealthisalsoinseparablefromdentalfluorosis.Theoriginofadose-responserelationbetweenfluorideinwatersuppliesandoralhealthwasinitiallyfocussedondentalfluorosis,notdentalcaries.Dentalfluorosisisadevelopmentalconditionordefectoftheenamellayerofteeth.Itischaracterizedbywhiteflecksorwhite,wavylines(opacities)ontheenamelofteeth.Astheseverityofdentalfluorosisincreases,thewhitelinesmaycoalescetoformcloudypatchesinvolvingsteadilymoreofthetoothsurface.Atseverelevels,thewholesurfacemaybeinvolvedinopacitiesandpitting;chippingorlossofenamelstructuremayoccur.
Therearesetrulesfortheobservationofdentalfluorosisthatattempttoseparateoutenamelopacitiesthatarefluoroticinoriginfromthosethatarenon-fluorotic.ThebestknownsetofcriteriaforadifferentialdiagnosisoffluoroticopacitiesisthatofRussell(Russell1961)whichweremorewidelypromulgatedbyHorowitzin1986(Horowitz1986).Theseinvolvetheareaofatoothsurfaceaffected,theshapeofthelesions,theirdemarcationfromthesurroundingunaffectedpartsofthetoothsurface,thecolouroftheaffectedareas,andthepatternofteethaffectedinthewholemouth.Anessentialaspecttodocumentingdentalfluorosisistheapplicationofthesecriteriawhilstexaminingaperson,and/ortheapplicationofthesesortsofcriteriaviaalgorithmsusedinanalysis.Onceadifferentialdiagnosisoffluorosisismade,variousscoringsystemsareavailabletoratetheseverityofthefluoroticchanges.ThebestknownoftheseisDean’sIndex(ClassificationSystem)forDentalFluorosis(Dean1942),andthesubsequentsummarymeasurefromthis,theCommunityFluorosisIndex(Dean1946).
InmorerecenttimesnewindiceshavebecomewidelyusedincludingtheThylstrupandFejerskovIndex(ThylstrupandFejerskov1978),theToothSurfaceIndexofFluorosis(Horowitzetal.1984)andtheFluorosisRiskIndex(Pendrys1990).EachoftheseindiceshasdifferentemphaseswhichmakecomparisonbetweenthemandwiththeDean’sIndexsubtlycomplex.Forinstance,Dean’sIndexclassifiesanindividualbythesecondmostsevere
3TheEWGnoteamorerecentsystematicreviewwaspublishedin2015butcouldnotbeincludedinthereportduetotimingofits
publication(Iheozor-EjioforZ,WorthingtonHV,WalshT,O'MalleyL,ClarksonJE,MaceyR,AlamR,TugwellP,WelchV,GlennyAM2015.Waterfluoridationforthepreventionofdentalcaries.,CochraneDatabaseSystRev.2015Jun18;6:CD010856.doi:10.1002/14651858.CD010856.pub2).
22 AustralianandNewZealandNutrientReferenceValuesforFluoride
observationoffluorosisatthetooth-levelinthemouth,theThylstrupandFejerskovIndexisadrytoothindexthatscoresthemostseverepresentationoffluorosis,theToothSurfaceFluorosisIndexisawettoothindexmeanttoreflectwhatonewouldseeineverydayactivity,whiletheFluorosisRiskIndexdividesthetoothsurfaceintothirdsandcancaptureveryearlystagesoffluorosisandindicationsofthetimingoftheriskexposure.AnyexaminationofdentalfluorosisrunsintothestronghistoricalbackgroundusingDean’sIndexandthemorerecentdominationoftheThylstrupandFejerskovIndex,especiallyinAustralianoralepidemiology.
AdifferentpathtoobservationsondentalfluorosisisthatoftheDevelopmentalDefectsofEnamelrecordingsystemwhichfirstlyrecordsalldefectsofenamelatanexaminationandthenseparatesoutpresumedfluoroticopacitiesfromotherenameldefectslikedemarcated,hyperplasticdefectsandcombinationsofthese,onthebasisoffluoroticdefectsbeingdiffuseonaffectedsurfacesandthedistributionofaffectedteethbeingsymmetrical,butnotalwaysofthesameseverity.TheDevelopmentalDefectsofEnamel(DDE)haditsorigininNewZealandandhasbeenwidelyusedinoralepidemiologicalsurveys(FDI,1982;Clarkson,O'Mullane1989).
Apopulation-basedstudyinthestateofNSWin2007examineddentalfluorosisinchildrenusingtheTFIndex(NSWCDHS2007).Atotalof5017childrenaged8–12yearswereexaminedforfluorosis.Theprevalenceofmoderate/severedentalfluorosis(TFscore4or5)was0.3%(14cases).Amongthose,twocaseswereconsideredashavingaTFscoreof5(severedentalfluorosis–thehealthadverseendpoint).TheprevalenceofthisadverseendpointintheNSWchildpopulationwas,therefore,0.04%.
StudiesinWesternAustraliaandSouthAustraliausingtheTFindexdidnotobserveanycasesofmoderatetoseveredentalfluorosis(Riordan2002;Do&Spencer2007)(seeTable3.2).
TheNZNationalOralHealthSurvey2009(NZMoH2010a)reportednocasesofseverefluorosisusingtheDeanIndex,whiletheprevalenceofmoderatefluorosiswas2.0%.
AstudyinNSWin2003(Baletal.2014)reporteddentalfluorosisusingDeanIndex.Some1%wasobservedtohavemoderatedentalfluorosiswhilesome0.135%(4cases)reportedlyhadseveredentalfluorosis.
Furtherinformationondentalfluorosis,itsmeasurementandreportsoftheprevalenceoffluorosisinAustralianandNewZealandpopulationsandothercountriesisgiveninSupportingDocument2.
23 AustralianandNewZealandNutrientReferenceValuesforFluoride
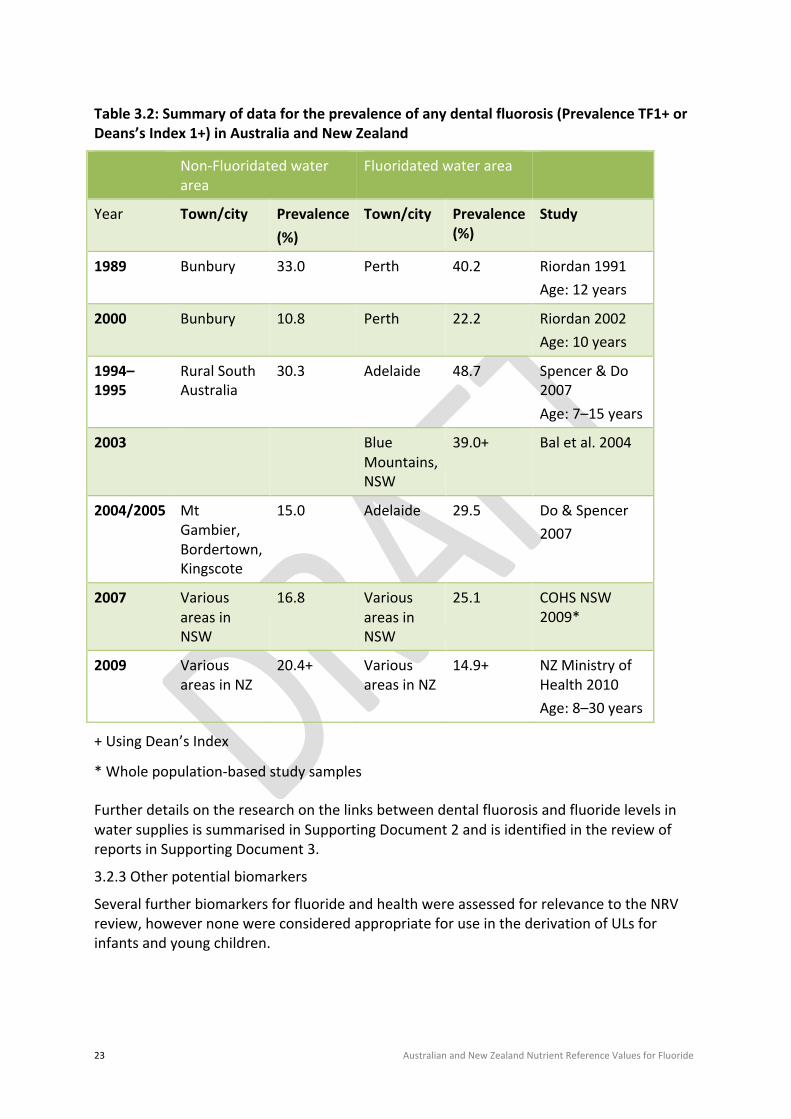
Table3.2:Summaryofdatafortheprevalenceofanydentalfluorosis(PrevalenceTF1+orDeans’sIndex1+)inAustraliaandNewZealand
Non-Fluoridatedwaterarea
Fluoridatedwaterarea
Year Town/city Prevalence(%)
Town/city Prevalence(%)
Study
1989 Bunbury 33.0 Perth 40.2 Riordan1991Age:12years
2000 Bunbury 10.8 Perth 22.2 Riordan2002Age:10years
1994–1995
RuralSouthAustralia
30.3 Adelaide 48.7 Spencer&Do2007Age:7–15years
2003 BlueMountains,NSW
39.0+ Baletal.2004
2004/2005 MtGambier,Bordertown,Kingscote
15.0 Adelaide 29.5 Do&Spencer2007
2007 VariousareasinNSW
16.8 VariousareasinNSW
25.1 COHSNSW2009*
2009 VariousareasinNZ
20.4+ VariousareasinNZ
14.9+ NZMinistryofHealth2010Age:8–30years
+UsingDean’sIndex
*Wholepopulation-basedstudysamples
FurtherdetailsontheresearchonthelinksbetweendentalfluorosisandfluoridelevelsinwatersuppliesissummarisedinSupportingDocument2andisidentifiedinthereviewofreportsinSupportingDocument3.
3.2.3Otherpotentialbiomarkers
SeveralfurtherbiomarkersforfluorideandhealthwereassessedforrelevancetotheNRVreview,howevernonewereconsideredappropriateforuseinthederivationofULsforinfantsandyoungchildren.

24 AustralianandNewZealandNutrientReferenceValuesforFluoride
Osteoporosis,osteosarcoma,pinealglandphysiology,IQanddelayedpermanenttootheruptionwereconsideredbytheEWGaspotentialbiomarkerswithoutcomessummarisedbrieflybelow.
TheEWGwasnotinapositiontoevaluateanypublisheddataonthegenotoxicpotentialoffluorideinthetimeframeforthispilotreviewastheliteratureavailabledidnotmeetthecriteriasetforconsideringhumandataonly.Itwasnotedthatthereareinternationalguidelinesfortestingchemicalsinthefoodsupply,includingtheirpotentialtodamageDNA,utilisingavarietyofwell–validatedbiomarkers,suchaschromosomalaberrationsandmicronuclei(OECD2014).TheEWGacknowledgedthereisabodyofliteraturethatmainlyrelatestoinvitrostudiesorstudiesinratsoftheimpactoffluorideoncellfunctionthatcanbededucedbyexploringstudiesthathaveinvestigatedeffectsongeneexpression.ThereisalackofinvivodataonDNAdamageindicesinhumanswithvaryingfluorideexposures,whichisaknowledgegap.
Osteoporosisandbonefractures:Thisisconsideredpotentiallyrelevantasabiomarkerforadultsbutnotforinfantsoryoungchildren.Alargenumberofstudieshaveinvestigatedpossibleassociationsbetweenthelevelsoffluorideindrinkingwaterandtheriskoffracturesofthehipandotherbones.Anassociationisbiologicallyplausible,sinceveryhighlevelsoffluorideareknowntoaffectbonedensityandstrength,butmayalsoreduceboneflexibility.However,researchindicatesthatwaterfluoridationatlevelsaimedatdentalcariespreventionhasbeenequivocalwithsmallvariationaroundthe‘noeffect’finding.Ithasbeenconcludedthatfluorideatlevelsassociatedwithwaterfluoridationhasnocleareffectonhipfractureriskinadults(McDonaghetal.2000,Nasmanetal.2013).ArecentreportfromthelongitudinalIowaFluorideStudyfoundnosignificantrelationshipbetweendailyfluorideintakeandadolescents’bonedensity(Levyetal.2014).
Osteosarcoma:Thisisnotconsideredsuitableasabiomarker.Anumberofstudieshaveinvestigatedlinksbetweentheleveloffluoridationandosteosarcoma,anoften-fatalbonecancermostcommonlydiagnosedinadolescents.Anassociationbetweenfluorideandosteosarcomaisbiologicallyplausible,sincebonesreadilytakeupmuchofthefluorideingested;children/adolescentsareoftendiagnosedaroundthetimeofthepubertalgrowthspurt,whenosteoblasticactivityisparticularlyhigh.Whiletherehasbeenonerecentreportofanassociationofosteosarcomainmaleswithearlierexposuretofluoridatedwater(Bassinetal.2006),mostavailablescientificevidencestronglysuggeststhatcommunitywaterfluoridationisnotassociatedwithosteosarcoma(Cohn1992,DouglassandJoshipura2006,Kimetal.2011,LevyetLeclerc2012,Blakeyetal.2014).
Pinealgland:Thisisnotconsideredsuitableasabiomarker.Concernshavebeenexpressedaboutpossibleharmfuleffectsoffluorideonthepinealgland(Luke1997,2001).Thepinealglandliesnearthecentreofthebrain,butoutsidethebloodbrainbarrierthatrestrictsthepassageoffluorideintothecentralnervoussystem.Lukestudiedtheaccumulationoffluorideinthepinealglandofolderadultcadavers.Fluoridedepositionwaslinkedtocalciumlevels,butwasconsideredanormalprocessofageing.Whiletherehasbeenspeculationthatsuchfluoridedepositionmayberelatedtobrainfunction,theEWGconsideredthatinsufficientevidenceexistedtodetermineanypossiblelinksbetweenthisdepositioninthepinealglandfunctionandhumanhealth.
25 AustralianandNewZealandNutrientReferenceValuesforFluoride
IntelligenceQuotient(IQ):Thisisnotconsideredsuitableasabiomarker.Arecentmeta-analysisofanumberofstudiesdatingbacktothe1980s,almostallfromChina,concludedthatnaturallyoccurringfluoridelevelsindrinkingwatermainlyintherangeof2-11mg/Lmayreducechildren’sIQsbyalmost7points(Choietal.2012).However,theinterpretationofthissystematicreviewwascautionedbytheauthorsgiventhelackofindividual-levelmeasuresonexposure,neurobehaviouralperformanceandcovariatesthatwouldadjustforeducationalresourcesoffamiliesandcommunities,aswellasotherpossiblecontaminantsfromlowqualitycoal.EvenstrongercriticismhasbeenmadebyBormanandFyfe(2013).TheoutcomesoftheChinesestudieshavenotbeenconfirmedincountriespractisingcommunitywaterfluoridation.RecentlyBroadbent,usingdatafromtheDunedinBirthCohortstudy,foundnosupportfortheassertionthatfluorideexposurewasrelatedtoIQ(Broadbentetal.2015).
Delayedpermanenttootheruption:Thisisnotconsideredsuitableasabiomarker.Delayederuptionofthepermanentteethhasbeenraisedasagrowthanddevelopmentconsequenceoffluorideintake.Howeveracounterargumentisthatfluorideintakereducescariesintheprimarydentitionandtheearlylossofaffectedteeth,eithernaturallyorasaresultofdentaltreatment.Itisthereforenotsurprisingthattheliteratureisequivocalondelayederuption.Thelatestreportsdonotsupportanysignificantdelayintheeruptionofthepermanentteeth(Jolaosoetal.2014).Thereforedelayederuptionwasnotconsideredsuitableasabiomarker.
3.3 Selectionofevidence
TheNHMRCprepareditslatestreportondietaryreferencevaluesforfluorideandothernutrientsforAustraliansandNewZealandersin2005.Accordingly,thetaskoftheEWGwastoreviewanynewevidenceonfluorideanditsrelatednutritionalreferencedatasince2005.However,consideringtherangeofinformationthatcanbegatheredthroughreviewingthepertinentliteratureacrossthelasttwodecades,theEWGagreedthatthefollowingmajorpublicationsonfluoridealongsidetheirrelatedbibliographies,wouldberelevantandusefulinthecontextofthecurrentreportandshouldbereviewedindetail:
1. InstituteofMedicine-DietaryReferenceIntakes(DRI)forCa,P,Mg,VitaminDandFluoride(IOM1997)
2. TheNHSCentreforReviewsandDisseminationattheUniversityofYork-TheYorkReview:Asystematicreviewofwaterfluoridation(McDonaghetal.2000)
3. EuropeanFoodSafetyAuthority(EFSA2005):OpinionoftheScientificPanelonDieteticProducts,NutritionandAllergiesonarequestfromtheCommissionrelatedtotheTolerableUpperIntakeLevelofFluoride
4. NationalResearchCouncil(NRC2006)-Fluorideindrinkingwater:AscientificreviewofEPA’sstandards
5. USEnvironmentProtectionAgency(EPA2010aandb)-Fluoride:ExposureandRelativeSourceContribution(RSC),AnalysisandDose–responseanalysisfornon-cancereffects

26 AustralianandNewZealandNutrientReferenceValuesforFluoride
6. ScientificCommitteeonHealthandEnvironmentRisk(SCHER2011)-Opiniononcriticalreviewofanynewevidenceonthehazardprofile,healtheffects,andhumanexposuretofluorideandthefluoridatingagentsofdrinkingwater
7. EuropeanFoodSafetyAuthority(EFSA2013):Scientificopinionondietaryreferencevalues(DRV)forfluoride.
3.3.1 Reviewofmajorreports
DetailedcommentsonthereportsreviewedaregiveninSupportingDocument3,includingtheoverview,methods,findings/estimatesandacommentonstrengths,weaknessesandinconsistenciesofthesereports.AsummaryoftheoutcomesofthereviewisgiveninTable3.3below.
Inbrief,theULof0.1mgF/kgbw/dayestablishedbytheIOMin1997hasbeenadoptedbymanyagencieswithoutfurtherconsideringitsderivation,inparticular,theconversionofafluorideconcentrationinreticulatedwaterintoafluorideintakeforchildren.ThisstepisessentialbecauseDean’s22citydentalfluorosisprevalencedatadidnotprovideanydetailsaboutwaterconsumptionorbodyweightsofthechildren.TheEWGnotedthatthebestavailabledose-responsedataforderivationofaULwasstilltheDean’sstudywhichwasconductedover70yearsago.
ThereareanumberofothermethodologicalissuestobeconsideredwhenestablishingaULorReferenceDose(RfD)(asestablishedbyEPA)thatareapparentfromthereviewoftheabovereports.Theseinclude:
• theselectionofanappropriateend-pointoroutcomei.e.severityofdentalfluorosisconsideredtobeadverse
• theacceptabilityofathresholdprevalenceoftheend-point
• theidentificationofsuitabledatawhichestablishesacleardose-responserelationshipbetweenfluorideintakeandtheprevalenceoftheend-point
• theapplicationofeitheradeterministicNOAELandLOAELanalysisorastatisticalBenchmarkDoseanalysistoasuitabledose-responserelationship.
TheseissuesarediscussedfurtherinSection3.5.