avian influenza, pandemic influenza, ecohealth
DESCRIPTION
Presentation by Colin D Butler and Delia Grace at the Ecohealth 2012 conference held at Kunming, China on 15-18 October 2012.TRANSCRIPT
Avian influenza, pandemic influenza,
ecohealth
International Association for
Ecology and Health, Kunming, October, 2012
A/Prof Colin D Butler National Centre for Epidemiology and
Population Health,
Dr Delia Grace ILRI
Two views of Zoonotic Emerging
Infectious Diseases (ZEIDS)
• ZEIDs have been and continue to be one
of the most important issues in EH
• ZEIDs are less important than neglected
tropical zoonoses and divert resources
from tackling them
• Both views focus on the microbe rather
than the milieu
2
Warning! Contrarian views ahead
• H5N1 very unlikely to become a global
pandemic
• H5N1 very unlikely to establish in SSA
• Current EH side-stepping problems crucial
to our health and future
– Creation of continental-wide pathogenic milieus
– Difficult problems of equity and justice
3
Could H5N1 HPAI become the next
“mother of all pandemics”?
4
Margaret Chan: “three global crises .. on horizon” ..
Climate change
regional food shortages and soaring food prices
pandemic influenza
5
CGIAR report:
SARS: $50 - 100 billion
“major avian influenza pandemic “ > $1 trillion (Burns et al.
2008). $2 trillion (World Bank 2008).
6
milieu and microbe
Claude Bernard (1813-1878)
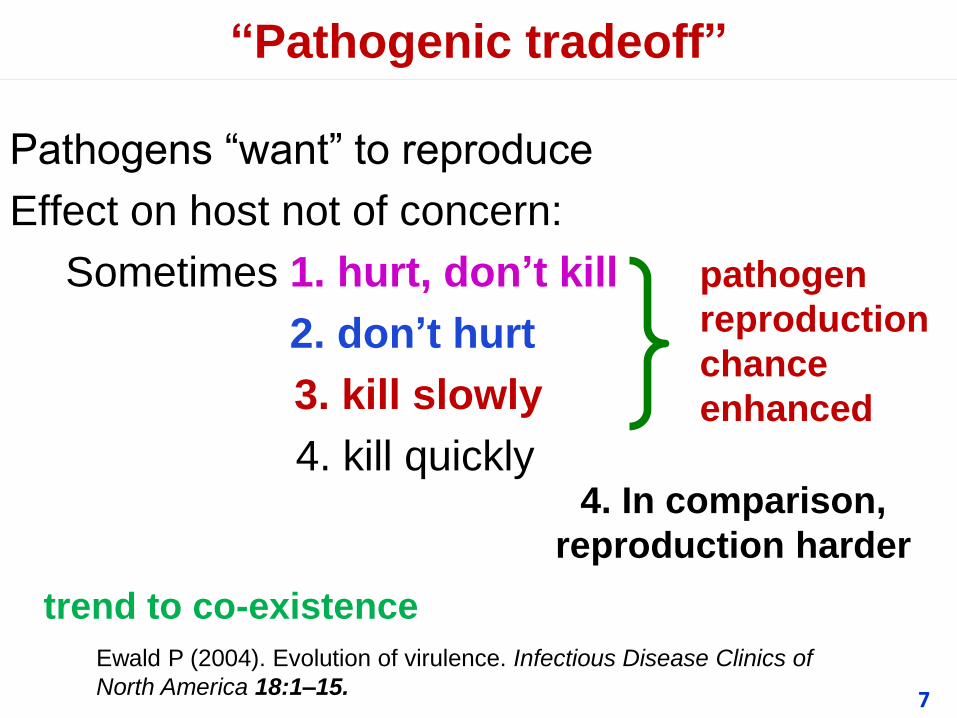
“Pathogenic tradeoff”
Pathogens “want” to reproduce
Effect on host not of concern:
Sometimes 1. hurt, don’t kill
2. don’t hurt
3. kill slowly
4. kill quickly
pathogen
reproduction
chance
enhanced
4. In comparison,
reproduction harder
trend to co-existence
7
Ewald P (2004). Evolution of virulence. Infectious Disease Clinics of
North America 18:1–15.
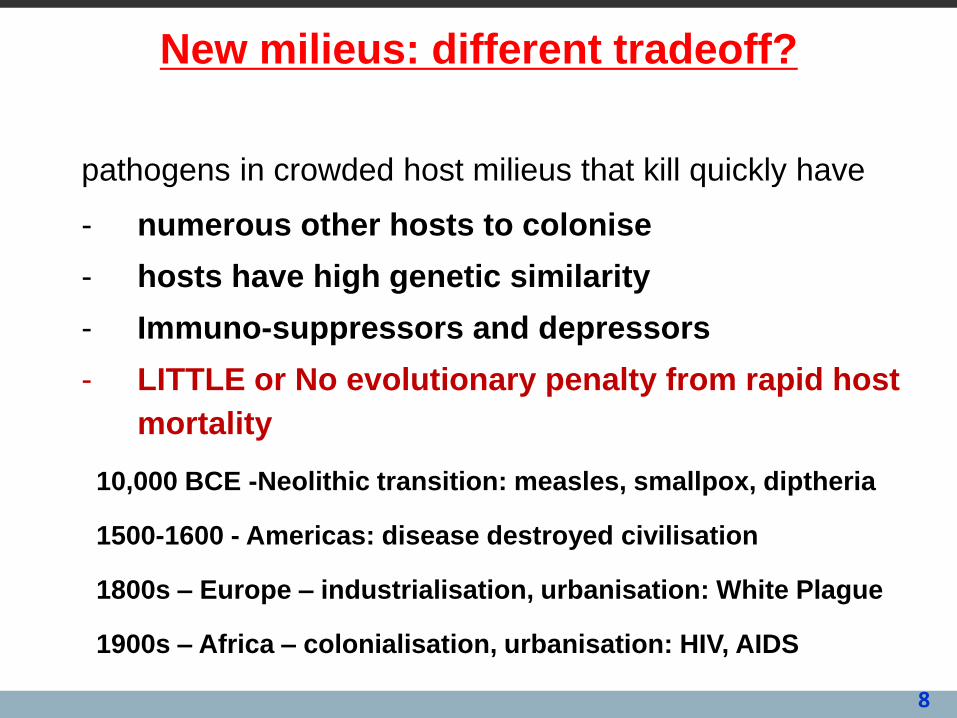
New milieus: different tradeoff?
pathogens in crowded host milieus that kill quickly have
- numerous other hosts to colonise
- hosts have high genetic similarity
- Immuno-suppressors and depressors
- LITTLE or No evolutionary penalty from rapid host
mortality
10,000 BCE -Neolithic transition: measles, smallpox, diptheria
1500-1600 - Americas: disease destroyed civilisation
1800s – Europe – industrialisation, urbanisation: White Plague
1900s – Africa – colonialisation, urbanisation: HIV, AIDS
8
9
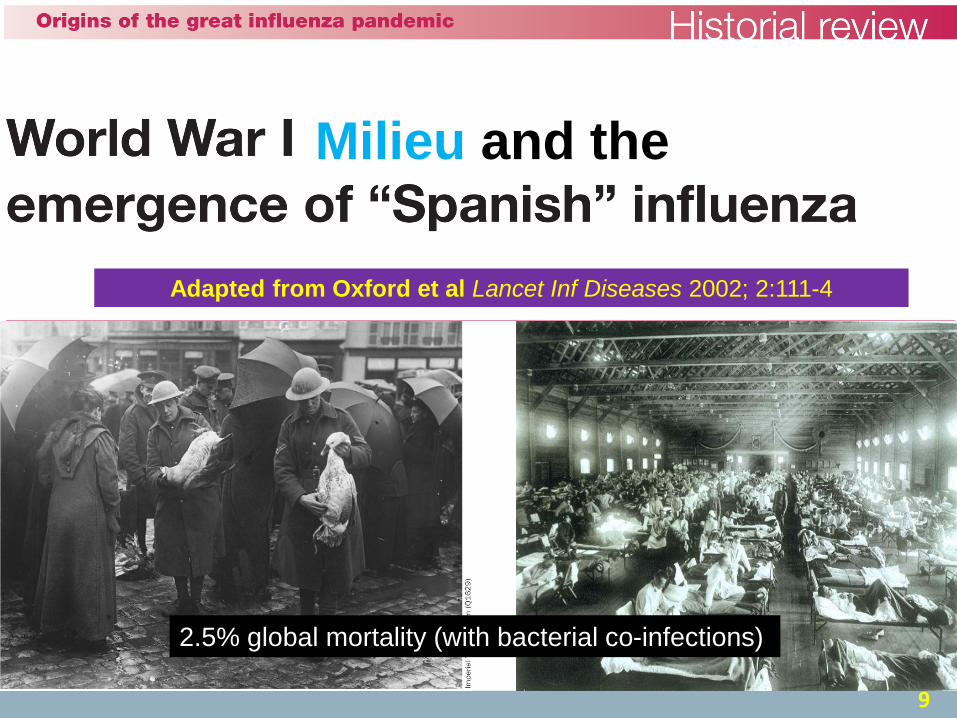
Milieu and the
Adapted from Oxford et al Lancet Inf Diseases 2002; 2:111-4
2.5% global mortality (with bacterial co-infections)
Reasons to be sceptical of H5N1 pandemic
10
1. More capacity to manage:
• Rapid global response (e.g. SARS)
• Numerous antibiotics for secondary bacterial infections
• Flu vaccines + anti-viral antibiotics
2. H5N1 case fatality rate questioned (Palese & Wang)
• If H5N1 develops human Ro >1 human lethality may fall (Ewald)
3. 1918 epidemic very atypical (c500 years human flu
epidemics)
• 1918 milieu extraordinary, unlikely to be coincidental
• Current milieu favours evolution of HPAI, but not HPHI
4. Vested interests exaggerate risk of H5N1 as human
pandemic
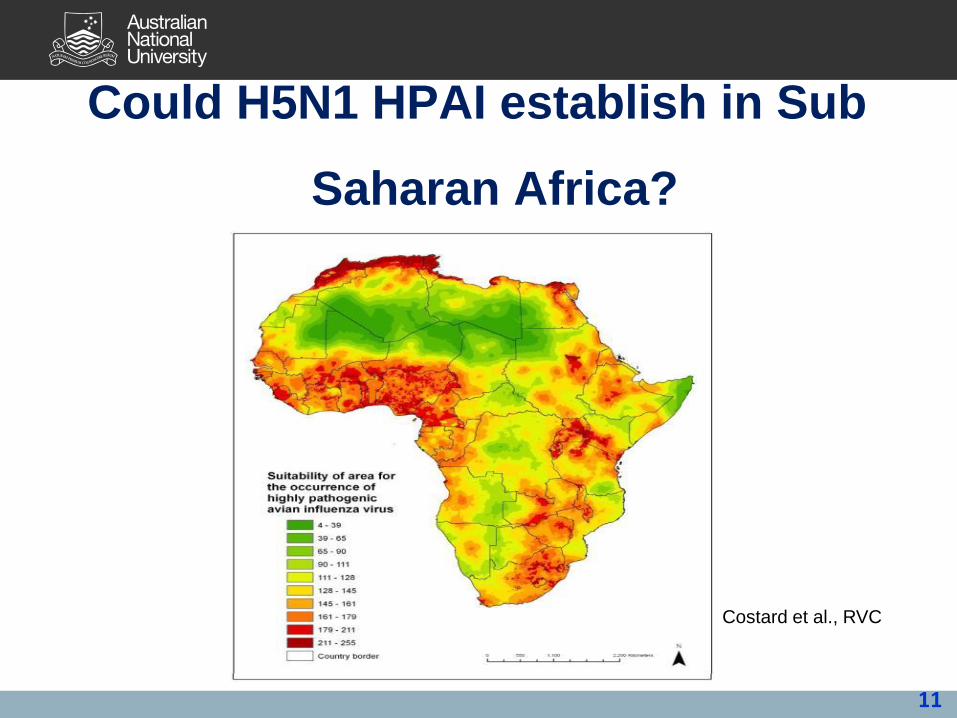
Could H5N1 HPAI establish in Sub
Saharan Africa?
11
Costard et al., RVC
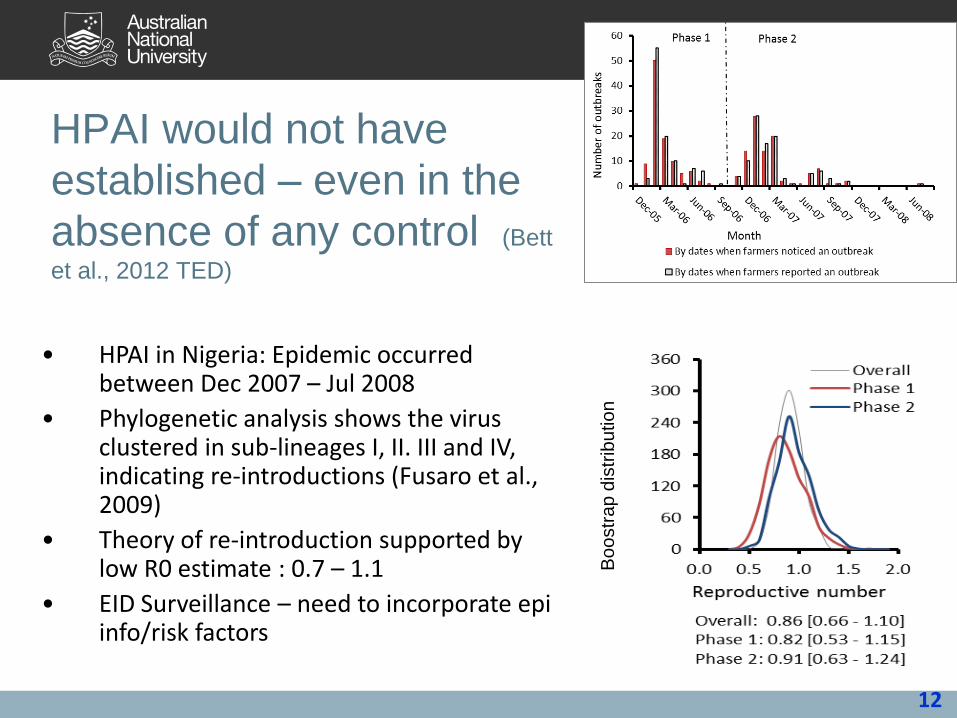
HPAI would not have
established – even in the
absence of any control (Bett
et al., 2012 TED)
12
• HPAI in Nigeria: Epidemic occurred between Dec 2007 – Jul 2008
• Phylogenetic analysis shows the virus clustered in sub-lineages I, II. III and IV, indicating re-introductions (Fusaro et al., 2009)
• Theory of re-introduction supported by low R0 estimate : 0.7 – 1.1
• EID Surveillance – need to incorporate epi info/risk factors
Bo
ostr
ap
dis
trib
utio
n
Most costs associated with control, not
disease
13
Nigeria
•140 million people
•150 million poultry – 25% intensive systems
HPAI
•I.3 million chicken died or culled One person died
•80% people stopped eating chicken for up to 4 mths
•41% of farm workers lost jobs
•Most compensation went to larger farms
•Dead chickens widely consumed, Sick chickens widely
consumed, Vaccination probably used
•Around 100 million USD lost or spent
From emerging microbe to pathogenic milieu
14
15
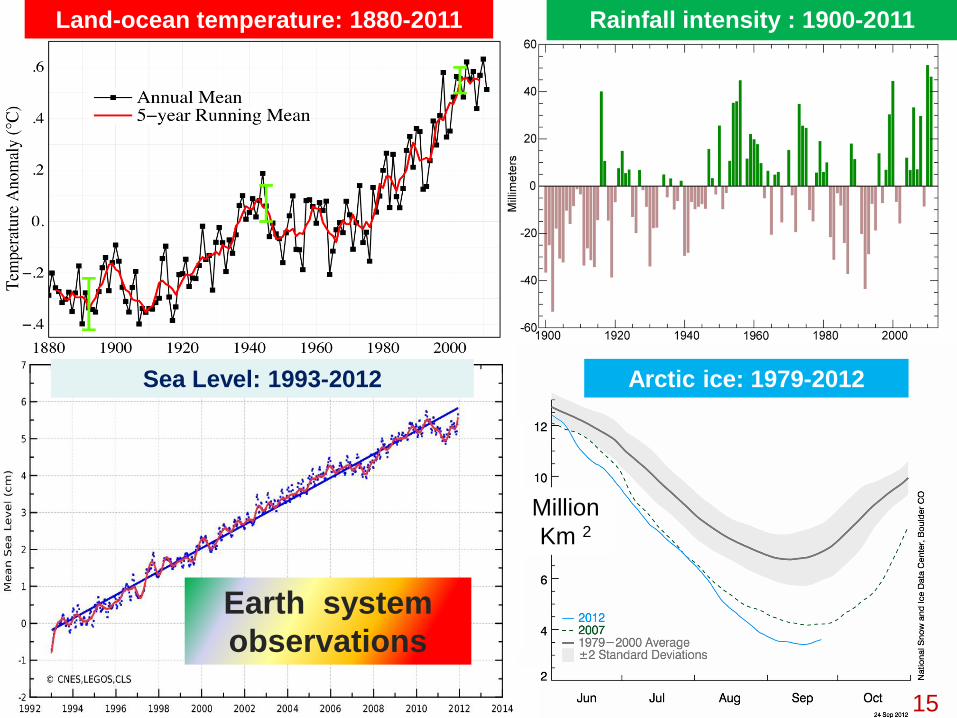
Sea Level: 1993-2012
Rainfall intensity : 1900-2011 Land-ocean temperature: 1880-2011
Earth system
observations
Arctic ice: 1979-2012
Million
Km 2

1998 2000 2004 2008 2011
Adapted from Murray & King, Nature. 2012; 481: 433-5.
Apparent production cap
2005: Plateau Oil
Production
(million barrels/day)
Oil price (US$ per
barrel)
16

17
“IMF assessment of world recovery bleak”
October 9, 2012
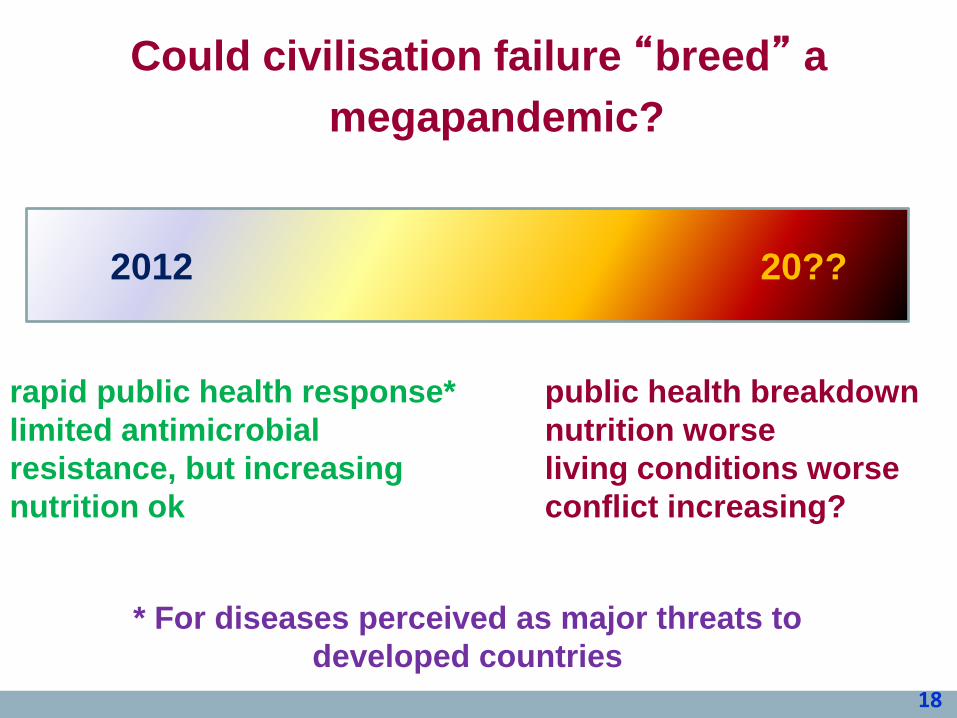
18
rapid public health response*
limited antimicrobial
resistance, but increasing
nutrition ok
public health breakdown
nutrition worse
living conditions worse
conflict increasing?
2012 20??
Could civilisation failure “breed” a
megapandemic?
* For diseases perceived as major threats to
developed countries
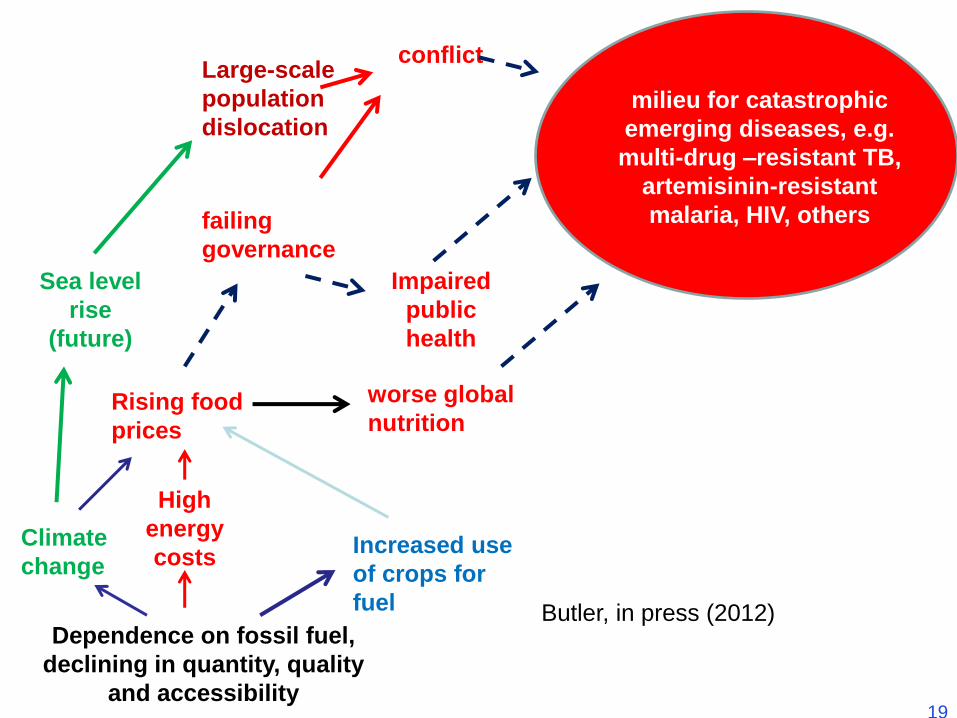
Sea level
rise
(future)
worse global
nutrition
failing
governance
Impaired
public
health
milieu for catastrophic
emerging diseases, e.g.
multi-drug –resistant TB,
artemisinin-resistant
malaria, HIV, others
Large-scale
population
dislocation
Climate
change
Rising food
prices
High
energy
costs
Dependence on fossil fuel,
declining in quantity, quality
and accessibility
Increased use
of crops for
fuel
conflict
Butler, in press (2012)
19
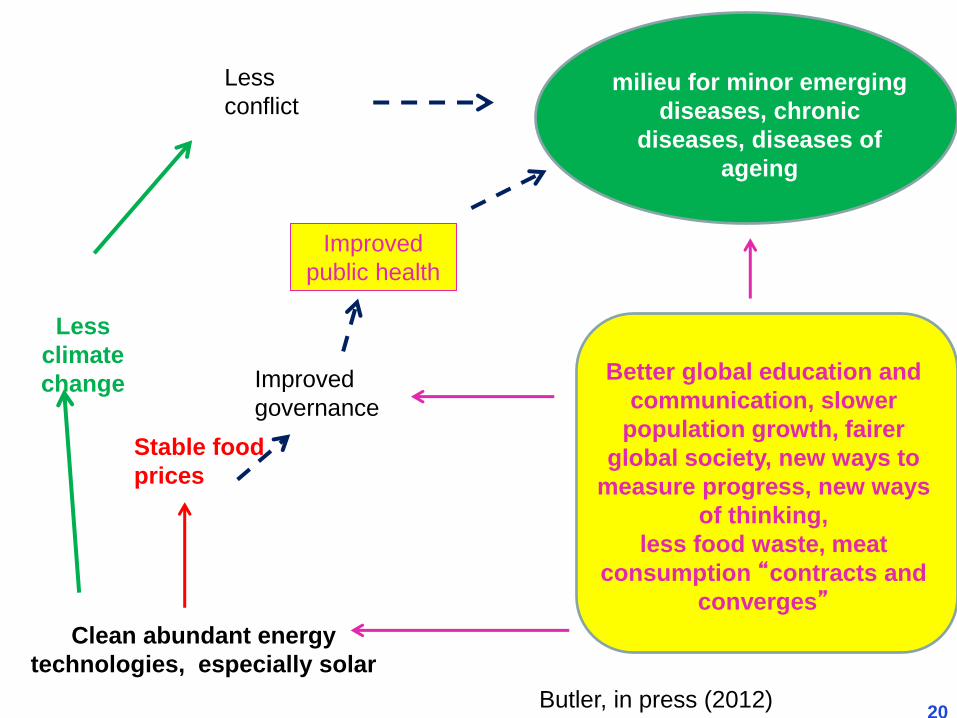
Less
climate
change Improved
governance
milieu for minor emerging
diseases, chronic
diseases, diseases of
ageing
Stable food
prices
Clean abundant energy
technologies, especially solar
Less
conflict
Better global education and
communication, slower
population growth, fairer
global society, new ways to
measure progress, new ways
of thinking,
less food waste, meat
consumption “contracts and
converges”
Improved
public health
Butler, in press (2012) 20

21
Acknowledgements
6 “Di TRGIV: “Environment, agriculture and infectious
diseases of poverty”
Prof AJ McMichael (ANU)
Prof Xiao-Nong Zhou (China CDC)
WHO Technical Report
Also Bianca Brijnath, Adrian Sleigh
Special Programme for Tropical
Diseases Research
WORLD BANK
Summary
• H5N1 very unlikely to become a global
pandemic
• H5N1 very unlikely to establish in SSA
• Current EH side-stepping problems crucial
to our health and future
– Creation of continental-wide pathogenic milieus
– Difficult problems of equity and justice
22

23
http://www.bodhi.net.au/html/forumforthefuture.html
23