aviation accident risk for airmen with aphakia and d.c ...for aphakia and artificial lens implants...
TRANSCRIPT

AD-A268 389
DOT/FAA/AM-93/11 Aviation Accident Risk for
Airmen with Aphakia andOffice of Aviation MedicineWashington, D.C. 20591 Artificial Lens Implants
Van B. Nakagawara
Kathryn J. Wood
Civil Aeromedical InstituteFederal Aviation AdministrationOklahoma City, Oklahoma 73125
July 1993 . A
Final Report
This document is availab!e to the publicthrough the National Technical Information
(V) Service, Springfield, Virginia 22161.
a).L-~
___ U.S. Departmentof TransportationFederal AviationAdministration
93823 086

NOTICE
This document is disseminated under the sponsorship ofthe U.S. Department of Transportation in the interest of
information exchange. The United States Governmentassumes no liability for the contents or use thereof.

Technical Report Documentation Page
1. Report No. 2. Government Accession No. 3. Recipient's Catalog No.
DOT/FAA/AM-93/11
4. Title and Subtitle 5. Report Date
AVIATION ACCIDENT RISK FOR AIRMEN WITH July 1993APHAKIA AND ARTIFICIAL LENS IMPLANTS 6. Performing Organization Code
7. Author(s) 8. Performing Organization Report No.
Van B. Nakagawara, O.D.; Kathryn J. Wood
9. Performing Organization Name and Address 10. Work Unit No. (TRAIS)
FAA Civil Aeromedical InstituteP.O. Box 25082Oklahoma City, OK 73125 11. Contract or Grant No.
1 2. Sponsoring Agency name and Address 13. Type of Report and Period Covered
Office of Aviation MedicineFederal Aviation Administration800 Independence Avenue, S.W.Washington, D.C. 20591 14. Sponsoring Agency Code
15. Supptementel Notes
This work was performed under task AM-A-91-PHY-144
16. Abstract
Airmen with aphakia and intraocular (IOL) implants who, on a case-by-casebasis, may obtain a waiver for a medical certificate, have been previouslyassociated with higher aviation accident rates when compared to the totalcivil airman population. This study analyzes the accident frequencies ofthese civil airmen for a 4-year period (1982-95). Medical records wereevaluated for all certified airmen who carried FAA-specific pathology codesfor aphakia and artificial lens implants during the study period. Aviationaccident and active airman population frequencies were obtained from FAAdatabases. The entire population of aphakia and IOL airmen and those < 50years of age had significantly higher (p < .50) accident rates than thecorresponding non-aphakic airman population. Aeromedical certificationconsiderations of the study findings are discussed. Further investigationsinto additional confounding factors between the aphakic and non-aphakicpopulations are recommended.
17. Key Words 18. Distribution StatementVision; Aphakia; Lens, Intraocular; Document is available to the publicMedical Certification; Accidents. through the National Technical
Information Service,Springfield, Virginia 22161
19. Security lassic. (of this report) 20. Securfty aessaf. (of this page) 21. No. of Pages 22. Price
Unclassified Unclassified 16Form DOT F 1700.7 (8-72) Reproduction of completed page authorized
• m m I |

ACKNOWLEDGMENTS
The authors gratefully acknowledge the assistance provided by FaredoonK. Loochan and Ronald Montgomery of the Vision Research Section,Aeromedical Research Division, who provided statistical and computersupport; Shirley Dark of the Program Support Branch, AeromedicalCertification Division, who provided consultation and technical support;and Shawn Seiter of the Application Systems Branch, Data ServicesDivision, and Jack Price and Loretta June Allen of the OperationalSystems Branch, Regulatory Support Division, who supplied informationfrom the various FAA databases.
DTIC QUALITY ITTSPECTLFl 4
Aooesslon For
NT IS GRA&IDTI' rLB
UL*.V ' "".L .In
ds El l
or C1
*111.

AVIATION ACCIDENT RISK FOR AIRMEN WITH APHAKIAAND ARTIFICIAL LENS IMPLANTS
INTRODUCTION
Vision changes as one ages. Changes in Aphakic spectacles have many opticalrefraction and ocular light transmission deficiencies and are not recommended fortypically appear in the age range 34-45 flight operations (8). Although superior toyears, while those changes in the retinal spectacles, contact lenses used to correctand neural system usually become more aphakia have their own deficiencies. Poorevident about age 55-65 (1). Presbyopia, compliance is a problem with rigid (hard)macular degeneration, and glaucoma are lenses (9). Soft contact lenses are diffi-examples of vision conditions that become cult for the patient to see, poorly handledmore common with aging (2). by older aphakics, and their wearers are
more prone to infections and more suscep-Elderly pilots are becoming a larger tible to the development of contact lens
percentage of the total civil airman popu- solution sensitivities.lation. In 1966, pilots over 50 years of agemade up only 9.5% of the civil airman In the last decade, IOL implantation haspopulation. Twenty years later, in 1986, become the primary therapeutic modalitythis age group comprised 22% of that for the correction of aphakia In the Unitedpopulation (3). As the frequency of elderly States. In 1980, approximately 396,000pilots has increased, the prevalence of cataract procedures were performed invisual impairment in the civil airman popu- the United States and 30% of these surger-lation has also increased (4)(5). ies included the implantation of an IOL
(10). In 1988, nearly one million cataractCataract, a condition in which there is a operations were performed in the United
loss of transparency of the crystalline States and 90% of these surgeries in-lens or its capsule, is the third leading cluded the implantation of an IOL (6). Incause of blindness in the United States (6) 1990, approximately 1.385 million cata-and is often associated with the aged. ract surgeries were done in this countryAphakia. a condition in which the crystal- and 98% of these included the implanta-line lens has been extracted, is usually a tion of an IOL (11). Cataract surgery ac-result of the removal of a cataractous counts for about 40% of all eye operationslens. The relationship of age to aphakia is in the United States (12) with a successwell established, and was again verified rate for contemporary cataract surgery ofin a recent study on aphakia prevalence in better than 98% (13). During this period.the civil airman population (7). There are there have been notable advances in cata-three ophthalmic devices normally em- ract surgical procedures and in designsployed to correct aphakia: spectacles, con- and materials used by ophthalm4c sur-tact lenses, and artificial or intraocular geons for IOL implantation which havelens (IOL) implants. provided the impetus for early medical
intervention. A recent Federal AviationAdministration (FAA) study confirmed the
I

increased prevalence of IOL use in the civil The Federal Air Surgeon's request for con-airman population during the period 1982- tinuing research on vision disorders related85 (14). to aging, surgical intervention or other treat-
ment as they affect airman performance.
In the FAA's Guide for Aviation Medical prompted the Vision Research Section, CivilExaminers (AME), the examining physician Aeromedical Institute, in collaboration withmay issue a medical certificate to a third- the Aeromedical Certification Division, toclass (private pilot) aphakic applicant who perform a follow-up epidemiologic study onmeets designated visual criteria and is aphakia and IOL in civillan airmen and theirotherwise healthy. However, first- (air association with aviation accidents duringtransport pilot) and second-class (com- the study period 1982-85. The objective ofmercial pilot) airman applicants who have this report is to present the results of ourhad cataract surgery are deferred issu- analysis of relative risk of accidents forance of a certificate and their applica- pilots with and without the defined de-tions are submitted for further consideration fects (aphakia and IOL) for the study pe-by the FAA. A waiver can be issued for such riod, 1982-85.applicants (15), on a case-by-case basis,after review of a complete ophthalmological METHODSevaluation.
1. A list was generated identifying civilAviation accidents associated with de- airmen who were issued airman medi-
fective vision in civil airmen have been cal certificates between January 1,the subject of numerous studies by the 1980, and December 31, 1985, andFAA (16, 17, 18, 19, 20, 21, 22, 23). Two who carried one or both of the FAA-of these studies by Dille and Booze ad- specific pathology codes 134dressed aphakia and artificial lens im- (aphakia) and 160 (artificial lens im-plants (21,22). While one of the studies plant) in FAA computer files.found a statistically significant eleva-tion in the accident rates for these pilots 2. The medical records of these airmenin relation to that of the total airman were reviewed and a Vision Defectpopulation (21), the other study reported Database, of known demographic andonly that the accident rates for the aphakia medical data on these aphakic air-and artificial lens implant groups were men, was constructed from the medi-higher than the rate for the total airman cal examination records and FAApopulation (22). Due to the small accident computer files.population in relation to the large overallairman population, this later study did not 3. The Aviation Standards National Fieldhave enough power to test whether these Office, Operations Systems Branchdifferences were statistically signifi- (AVN-124), generated a list from thecant. The authors recommended that a Accident/Incident Data Systems forlonger term study be performed in the the period of January 1. 1982, tohopes of determining whether accident December 31, 1985, of all airmen whorates for pilots having these medical con- were involved in civil aviation air-ditions were significantly higher than craft accidents (i.e., Accident Data-those of a normal pilot population, base).
2
4. A list of known aphakic airmen (n = b) Stratified all airmen with accidents by3460) during the study period was pro- effective class of medical certificatevided to AVN- 124. This list was matched and age as of the end of each studyagainst the Accident/ Incident Data Sys- year.tems database for the time period of c) Stratified all aphakic airmen fromJanuary 1, 1982, to December 31, 1985, the Vision Defect Database by pa-which identified those aphakic airmen thology (aphakia and IOL), by effec-involved in civil aviation aircraft acci- tive class of medical certificatedents (i.e., Aphakic Accident Database), and age as of the end of each studywhich included fatal accidents. year.
5. The Aphakic Accident Database was 8. Accident rates per 1,000 airmen werecompared with the Vision Defect Data- calculated for three major populations,base to ensure all the identified aphakic total airman (aphakic and non-aphakic),airmen with accidents were aphakic, aphakic airman (aphakia with and with-with or without an IOL, at the time of out IOL), and IOL airman (aphakia withtheir accident and active at the end of IOL). These populations were thenthe accident year. (Note: Active refers to stratified by age and class. These ratesthe current status of the airman's medi- were calculated for each calendar yearcal certificate. Airmen are considered and for the composite 4-year studyactive until their certificate expires. FAA period. Significance was determined byaeromedical certification guidelines con- using the Chi-Square statistic (X2c), or
sider an airman to be active for a period the Fisher Exact 2-Tailed Test, whenof 24 months after the month in which appropriate.the certificate is issued. A certificateremains active even with the death of RESULTSthe airman from aviation-related ornonaviation-related causes.) There were 12,883 aviation accidents that
occurred during the study period. When6. The aphakic accident reports were re- these accidents were cross-referenced to
viewed to determine the ascribed causal the CAIS database, 1,889 (14.7%) wererole in the accident, and the likelihood deleted due to non-readable informationof vision or eye pathology being a factor. in the pilot certificate number field,
incorrect pilot certificate or social7. The Data Services Division (AAC-300): security numbers, and changes in the
a) Stratifled all active airmen in the Con- control data, for a total of 10,994solidated Airman Information System identifiable accidents. When the airmen(CAIS) database by effective class of involved in these 10,994 accidents weremedical certificate (Note: FAA aero- stratified by effective class of medicalmedical regulations stipulate that an certificate held at the end of each year ofairman maybe first- or second-class the study, 1,832 (14.2%) airmen weremedically certified and the time lapse deleted for the following reasons: notsince examination would reduce the active at the time of the accident or at the end"effective status" to a lesser class.) of the year; active at the time of the accidentand age (< 50 or z 50 years) as of the but not at the end of the year; not active at theend of each study year. time of the accident but active at the end of
3

TABLE 1. TOTAL ACTIVE AIRMEN BY AGE GROUP AND YEAR
CUMMULATIVEFREQUENCIES
CATEGORY 1982 1983 1984 1985 1982-85
APHAKIA:
< AGE 50 465 488 516 516 1,985
_ AGE 50 1,284 1,457 1,620 1,775 6,136
TOTAL 1,749 1,945 2,136 2,291 8,121
IOL:
< AGE 50 106 135 179 217 637
> AGE 50 558 785 996 1,206 3,545
TOTAL 664 920 1,175 1,423 4,182
TOTAL AIRMEN:
< AGE 50 608,960 586,289 573,746 551,161 2,320,156
2 AGE 50 159,382 162,016 165,554 165,316 652,268
TOTAL 768,342 748,305 739,300 716,477 2,972,424
the year; and doubtful determination of Aphakic airmen with accidents duringeffective class of medical certificate and age, the study period were cross-referenced toleaving a total of 9,162 (71.1%) airmen with the CAIS database. One airman was de-aviation accidents. leted from the study (active at the time of
accident, but was not active at the end ofAirmen from the Vision Defect Database the year), leavingatotalof41 aphakic airmen
(n = 3460) were cross-referenced to the involved in accidents and active at the end ofCAIS database. A total of 43 airmen were the accident year.deleted due to error messages in one of theidentification fields (e.g., social security num- The frequency of the total, and aphakiaber, pilot certification number, etc.), leaving and IOL airmen by age groups (< 50 and - 50)a total of 3,417 known aphakia and IOL and by year is presented in Table 1. Asairmen during the study period. expected, in the aphakia and IOL airman
4
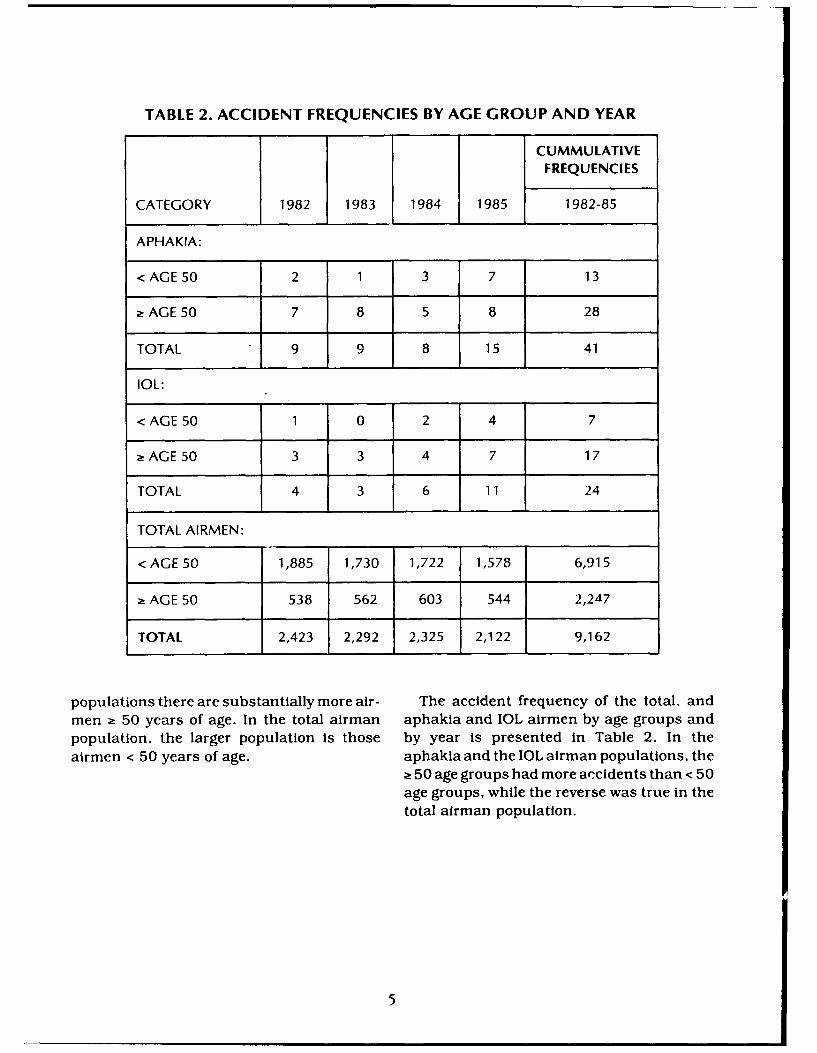
TABLE 2. ACCIDENT FREQUENCIES BY AGE GROUP AND YEAR
CUMMULATIVEFREQUENCIES
CATEGORY 1982 1983 1984 1985 1982-85
APHAKIA:
< AGE 50 2 1 3 7 13
a AGE 50 7 8 5 8 28
TOTAL 9 9 8 15 41
IOL:
< AGE 50 1 0 2 4 7
aAGE50 3 3 4 7 17
TOTAL 4 3 6 11 24
TOTAL AIRMEN:
< AGE 50 1,885 1,730 1,722 1,578 6,915
2 AGE 50 538 562 603 544 2,247
TOTAL 2,423 2,292 2,325 2,122 9,162
populations there are substantially more air- The accident frequency of the total, andmen ; 50 years of age. In the total airman aphakia and IOL airmen by age groups andpopulation, the larger population is those by year is presented in Table 2. In theairmen < 50 years of age. aphakia and the IOL airman populations, the
! 50 age groups had more accidents than < 50
age groups, while the reverse was true in thetotal airman population.
5
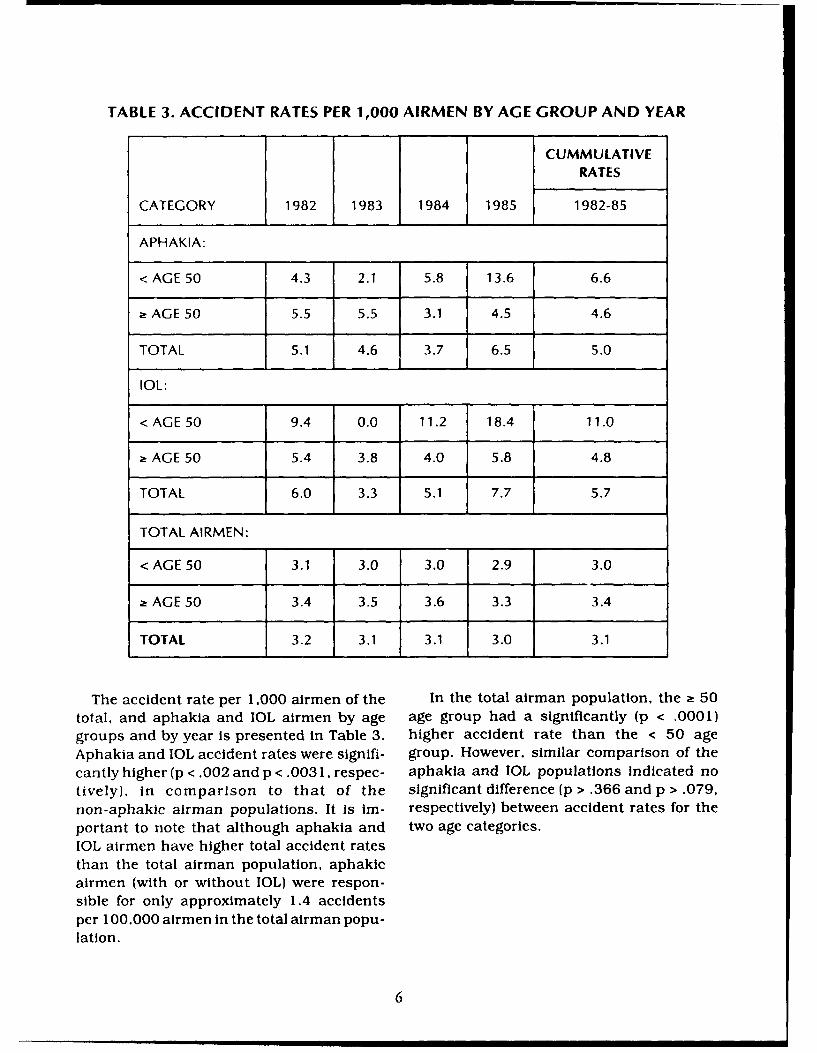
TABLE 3. ACCIDENT RATES PER 1,000 AIRMEN BY AGE GROUP AND YEAR
CUMMULATIVERATES
CATEGORY 1982 1983 1984 1985 1982-85
APHAKIA:
< AGE 50 4.3 2.1 5.8 13.6 6.6
SAGE 50 5.5 5.5 3.1 4.5 4.6
TOTAL 5.1 4.6 3.7 6.5 5.0
IOL:F
< AGE 50 9.4 0.0 11.2 18.4 11.0
SAG E 50 5.4 3.8 4.0 5.8 4.8
TOTAL 6.0 3.3 5.1 7.7 5.7
TOTAL AIRMEN:
< AGE 50 3.1 3.0 3.0 2.9 3.0
SAG E 50 3.4 3.5 3.6 3.3 3.4
TOTAL 3.2 3.1 3.1 3.0 3.1
The accident rate per 1,000 airmen of the In the total airman population, the a 50total, and aphakia and IOL airmen by age age group had a significantly (p < .0001)groups and by year is presented in Table 3. higher accident rate than the < 50 ageAphakia and IOL accident rates were signifi- group. However, similar comparison of thecantly higher (p < .002 and p < .0031, respec- aphakia and 1OL populations indicated notively). in comparison to that of the significant difference (p > .366 and p > .079,non-aphakic airman populations. It is Im- respectively) between accident rates for theportant to note that although aphakia and two age categories.IOL airmen have higher total accident ratesthan the total airman population, aphakicairmen (with or without IOW were respon-sible for only approximately 1.4 accidentsper 100,000 airmen in the total airman popu-lation.
6

TABLE 4. SUMMARY OF STATISTICAL TESTS FOR PATHOLOGY AND AGE
FISHERODDS 95% CONFIDENCE CHI-SQ 2 -TAIL
CATEGORY RATIO INTERVAL (Yates) P-VALUE TEST
Total Aphakia 1.64 (1.19 < OR < 2.26) 9.61 0.00193
Total IOL 1.87 (1.22 < OR < 2.83) 8.79 0.00303
"< Age 50 Aphakic 2.21 (1.22 < OR < 3.89) 7.36 0.00669
"< Age 50 IOL 3.72 (N/A) N/A 0.00336
Note: Above populations are compared with like non-aphakic populations.
* Age 50 Total Airmanvs 1.16 (1.10 < OR < 1.21) 35.60 0.00000
< Age 50 Total Airman
2! Age 50 Aphakiavs 0.70 (0.35 < OR < 1.42) 0.82 0.36654
< Age 50 Aphakia
* Age 50 IOLvs 0.43 (N/A) N/A 0.07950
< Age 50 IOL
Although both the < 50 and ;50 age groups in The statistical test results are summarizedboth the aphakia and IOL populations had in Table 4.higher accident rates than similar age cat-egories in the total airman population, only the Upon review of the FAA accident reports of< 50 aphakic and IOL populations had signifi- airmen with aphakia or IOL, neither the pres-cantly (p < .007 and p < .004, respectively) ence of aphakia or 1OL was ascribed a causalhigher accident rates than their counterparts in role, nor was any association to vision problemsthe non-aphakic airman population. ascribed during any accident.
7

DISCUSSION differences between the non-aphakic airmanpopulation versus the aphakia and IOL air-
In our study, aphakia and IOL airmen have man populations were significant in airmen <significantly higher accident rates/ 1,000 50 years of age and non-significant for theairmen than the rates for the non-aphakic older age category. In other words, althoughairman population. For the defined defects, there are substantially fewer aphakia andour accident rates are lower than those IOL airmen < 50 years of age, these youngerreported in Dille & Booze's 1979 and 1980-81 airmen were involved in significantly moresthdies. However, direct comparison should accidents than non-aphakic airmen of thebe viewed with caution as the populations same age category. We postulate that youngerused to determine accident rates for the two airmen may be "physiologically" impaired bystudies are different. While we determined aphakia, but do not have the "psychological"aphakia and TOL pep'uLatW -s bydirect review impairment that the aged often accept. Asof the airman n;, iical iecords, Dille and various sensory-motor functions, includingBooze determined th•ir populations by vision, begin to deteriorate, the aged maypathology codes medically assigned by the exercise greater caution .-.nd reduced expo-FAA. several of which were found to be sure to hazards. This finding may be signifi-miscoded during our review process. In cant since medical intervention for cataractsaddition, we reviewed individual medical and the implantation of IOLs in the Unitedrecords to ensure all airmen involved in States are being done on progressivelyaccidents had aphakia or an IOL at the time younger patients. Additionally, the lack ofof the accident, and were active both at the significant differences in the accident rates oftime of the accident and at the end of the the 2 50 aphakia and IOL airmen comoaredcalendar year. to those of the < 50 aphakia and IOL airmen
suggest that medical impairment rather thanAge is considered significant in air carrier age may be a more important factor to avia-
operations (e.g., in the U.S. the retirement tion accident risk. These findings supportage for air carrier pilots is 60 years). however Dougherty and Harper's (17) conclusion thatthere is no mandatory upper age limit for the increased risk of accidents associatedgeneral aviation pilots. When analyzed by age with age was actually associated with fre-categories, total civil airmen ; 50 years of age quency of physical defects accumulating withhad significantly higher accident rates than age, rather than age itself.those airmen < 50 years of age. This supportsthe association of age with increased acci- An aircraft accident is defined as an occur-dent risk that has been previously observed rence associated with the operation of an(16, 24, 25). Booze found that age-specific aircraft which takes place between the timeaccident rates for older airmen increased any person boards an aircraft with the inten-approximately four times that of younger tion of flight until such time as all suchairman (24). Others have reported a linear persons disembarked, in which any personincrease in accident rate with increasing age suffers death or serious injury, or in which(16, 25). the aircraft receives substantial damage (26).
Such events are rare, and the use of acci-Aphakia and IOL airmen < 50 and 2 50 dents as a performance measurement asso-
years of agt, had higher accident rates per 1000 elated with a medical conditior is limited byairmen than that for the same age categories the low frequency of reported occurrences.in the total airman population. However, the Aircraft incidents, defined as occurrences
8

involving the operation of one or more air- lations and were not directly supported bycraft in which the hazard or potential hazard the accident investigation team reports. Rou-to safety is involved, but are not classified as tine aircraft accident investigation, whichan accident due to degree of injury and/or seeks to determine the presence of physicalextent of damage (27), may be a better perfor- problems and any association of the defectmance measurement. However, many cases with the accident cause, may need to focusare not reported and other incidents are not more closely on vision problems associateda direct result of piloting an aircraft. with aircraft accidents in order to truly iden-
tify causal relationships.The rarity of aviation accidents is again
demonstrated in our study. In the total air- There are several aeromedical certifi-man population there were approximately cation considerations indicated from our3.1 accidents per 1,000 airmen during the study, including:study period. The number of accidents con-tributed by either aphakia or TOL airmen to 1. The higher accident rates of the aphakiathese accidents was minimal (about 0.014 and IOL airmen suggest that epidemio-per 1,000 airmen). The small number of logical accident studies and clinical re-aviation accidents makes statistical evalua- search on aviation stressor effects oftion of association of stratified medical con- these visually compromised airmen beditions to such events questionable. A continued. This research may be im-coordinated airman health information and proved by a closer assessment of acci-accident database system could greatly as- dent records to determine possiblesist in any future correlation studies of avia- factors contributing to the accidentstion accidents to medical conditions by (e.g., time of day, phase of flight), whichreducing the amount of lost data. can be the foundation for considering
various recommendations for reducingHuman error has been found to cause or such accidents. The Vision Research
contribute to over half of all aviation acci- Section plans to perform such an analy-dents. Attempts to investigate human perfor- sis of accidents involving aphakic air-mance error, and vision performance in men during our study period.particular, in aircraft accidents face three Additionally, a system may be imple-major obstacles: such vision related acci- mented that identifies aphakic airmendents are rare events and difficult to identify; involved in accidents so that the evalu-post-accident database Information is often ation by the accident investigator canfragmentary or faulty; and potential liability focus on vision factors that may con-associated with an accident can hinder the tribute to the accident.Investigatory process (28). Neither aphakianor IOL was ascribed a causal role upon 2. Aphakia and IOL airmen in our studyreview of the FAA accident reports, nor was are not necessarily characteristic ofany association with vision problems as- airmen at any future time. Surgical tech-cribed to any accident. Although upon close niques and ophthalmic materials areexamination of these records some associa- being constantly improved, as aretion of the accident with possible vision prob- changes In corrective device applica-lems could be extrapolated either from tions. which may improve the visualenvironmental conditions present or the pri- capabilities and safety of such pilots.mary cause of the mishap, these are specu-
9
3. New medical applications to correct system, a gauge of poor piloting skillsaphakia in the airman population should (aircraft accident) can be used to validatecontinue to be monitored. such a performance test.
4. No relaxation in the current aeromedlcal 3) Aircraft design and maintenance needs tocertification standards and review pro- accommodate the capabilities and limita-cess is recommended at this time. tions of the older and medically Impaired
airmen.5. Future recommendations may consider
the reiative flight safety of airmen with 4) Improved training and education of medi-multiple medical impairments. cally impaired airmen, whose conditions
may adversely affect their ability to fly an
6. Although no measurement of information aircraft, are needed.processing skills, such as visual attentionor cognitive function which the pilot pos- CONCLUSIONSsessed prior to the aircraft accident, iscurrently available, we have the capability The major findings of our study include:to measure two functional variables (eyehealth and visual function) that contrib- 1) Civil airmen > 50 years of age had signifi-ute to the quality of visual information cantly higher accident rates than thoseavailable to the pilot. These two variables, airmen < 50 years of age.influenced by physiologic and environ-mental conditions, and the use of oph- 2) Aphakia and IOL airmen had significantlythalmic devices, can be monitored and higher accident rates than non-aphakicoptimized to improve visual efficiency and airmen.aviation safety.
3) Aphakia and IOL airmen < 50 years of ageIn order to improve aviation performance and had significantly higher accident rates
safety of the aged and the visually Impaired, than non-aphakic airmen < 50 years ofseveral programs are recommended for consid- age.eration and implementation:
Significant associations found with aphakia1) The research community needs to develop and IOL populations and aviation accidents
basic Information necessary for effective should be cautiously interpreted. Our analysisevaluation of the elderly and visually com- could not directly attribute the causation of theproisled airmen. observed higher frequency of aviation accidents
to either aphakia and/or the use of an IOL.2) A medical or performance appraisal sys- Therefore, it would be premature to suggest any
tern should be developed to identify pilots change in current FAA aeromedical certiflca-considered to be at risk due to early or tion standards for airmen with aphakia andimpending deterioration in health or per- 1OL. Further investigations into confoundingformance. An appropriate measurement factors between the aphakic and non-aphakicof piloting behavior (performance on a populations (e.g., flight hours, class of medicalsimulator) needs to be developed to evalu- certificate held, type of aphakia) may provideate pilot performance. And, as a result of further insight into possible visual problems inan improved aircraft accident reporting the cockpit.
10

RIEFERNE
1. Fozard JL, Wolf E, et al. Visual perception 8. Dhenin G. Ophthalmological conditionsand communication. In: Birren JE, and eye examination. In: Aviation Medi-Schale KW, eds. Handbook of the Psy- cine: Health and Clinical Aspects. Lon-chology ofAging. New York:Van Nostrand don: Tri-Med Books Limited, 1978:264-Rheinhold Company, 1977:497-534. 302.
2. National Academy of Science, Institute of 9. Boyd BF. Highlights of Ophthalmology.Medicine. Airline pilot age, health, and 1974-1975 Series; 3:1-6.performance. Washington DC:National 10. Boyd BF. Highlights of Ophthalmology.Academy Press, 1981. 1980 Series 8:1-3.
3. Nakagawara VB. The relevance of vision 11. Carr M. Cataract, intraocular lens, anddefects in the medical certification of refractive surgery in 1987 with a fore-civilian airman. In: Goss DA, Edmondson cast to 1995. J Cataract Refract Surg.LL, eds. Proceedings of the 1988 North- 1988; 14:664-7.eastern State University Symposium onTheoretical and Clinical Optometry. 12. Alexander LJ. Aphakia and pseudophakia.March 25, 1988. Tahlequah, OK. In: Amos JF, ed. Diagnosis and Manage-1988:59-71. ment in Vision Care. Boston: Butter-
4. Booze CF Jr. Prevalence of selected pathol- worths, 1987:639-69.
ogy among currently certified active air- 13. Frank A, Werfel N. ECCE with phacoe-men. Washington, DC: Department of mulsification. J Ophthalmic Nurs &Transportation /Federal Aviation Admin- Technol. 1988; 7:62-7.istration; 1981; FAA Report No. FAA- 14. Nakagawara VB, Loochan FK, Wood KJ.AM-81-9. Available from: National Tech- The prevalence of artificial lens implantnical Information Service. Springfield, in the civil airman population. Wash-VA 22161. Order #ADA103397/6. ington, DC: Department of Transporta-
5. Booze CF Jr. Prevalence of disease among tion/Federal Aviation Administration;active airmen. Washington, DC: De- 1992; FAA Report No. DOT/FAA/AM-partment of Transportation /Federal 92 / 14. Available from: National Techni-Aviation Administration; 1988; FAA cal Information Service, Springfield, VAReport No. DOT/FAA/AM-89/2. Avail- 22161. Order #ADA 249126.able from: National Technical Infor- 15. Department of Transportation/Federalmation Service, Springfield, VA 2216 1. Aviation Administration. Guide for avia-Order #ADA206050. tion medical examiners. Washington,
6. Goodman DF, Stark WJ, Gottsch JD. Com- DC: 1981; FAA Office of Aviation Medi-plications of cataract extraction with cine.intraocular lens implantation. Oph- 16. Harper CR. Physical defects of civilianthalmic Surgery. 1989; 20:132-40. pilots related to aircraft accidents. Aero-
7. Nakagawara VB, Loochan FK, Wood KJ. space Med. 1964; 35:851-6.The prevalence of aphakia in the civil 17. Dougherty JD, Harper CR. Physical de-airman population. Washington, DC: fets of c a rp e d to aicaftDepartment of Transportation/Federal fects of civilian pilots related to aircraftAviation Administration; 1991; FAA Re- accidents: a new look at an old problem.port No. DOT/FAA/AM-91/14. Avail- Aerospace Med. 1968; 39:521-7.able from: National Technical Informa-tion Service, Springfield, VA 22161. Or-der #ADA241032.
II
18. Dille JR. Booze CF Jr. Accident experience 23. Ryan LC, Gerathewohl SJ, Mohler SR,of civilian pilots with static physical Booze CF Jr. To see or not to see: visualdefects. Washington, DC: Department acuity of pilots involved in midair colli-of Transportation/Federal Aviation Ad- sions. Washington, DC: Department ofministration; 1976; FAA Report No. FAA- Transportation/ Federal Aviation Ad-AM-76-7. Available from: National Tech- ministration; 1975: FAA Report No. FAA-nical Information Service, Springfield, AM-75-5. Available from: National Tech-VA 22161. Order #ADA029431/4GI. nical Information Service, Springfield,
19. Dille JR, Booze CF Jr. The 1975 acci- VA 22161. Order #ADA016277.
dent experience of civilian pilots with 24. Booze CF Jr. An epidemiologic investiga-static physical defects. Washington, tion of occupation, age, and exposure inDC: Department of Transportation/ general aviation accidents. Washington,Federal Aviation Administration; 1977; DC: Department of Transportation/ Fed-FAA Report No. FAA-AM-77-20. Avail- eral Aviation Administration; 1977; FAAable from: National Technical Infor- Report No. FAA-AM-77-10. Availablemation Service, Springfield, VA 2216 1. from: National Technical InformationOrder #ADA045429/8GI. Service, Springfield, VA 22161. Order
20. Dille JR, Booze CF Jr. The 1976 acci- #ADA-040978/9G1.
dent experience of civilian pilots with 25. Lategola MT, Fiorica V, Booze CF Jr, Folkstatic physical defects. Washington, ED. Comparison of status variablesDC: Department of Transportation/ among accident and non-accident air-Federal Aviation Administration; 1979: men from the active airman population.FAA Report No. FAA-AM-79-19. Avail- Washington, DC: Department of Trans-able from: National Technical Infor- portation/Federal Aviation Administra-mation Service, Springfield, VA 22161. tion; 1970; FAA Report No. FAA-AM-70-Order #ADA07718919. 18. Available from: National Technical
21. Dille JR, Booze CF Jr. The prevalence of Information Service, Springfield, VA21. ileJR.Booz CFJr.The22161I. Order #AD722 148.
visual deficiencies among 1979 general
aviation accident airmen. Washington, 26. International Civil Aviation Organization.DC: Department of Transportation / Fed- International standards and recom-eral Aviation Administration; 1981; FAA mended practices: aircraft accident in-Report No. FAA-AM-81-14. Available vestigation. March 1981.from: National Technical Information 27. Department of Transportation/FederalService, Springfield. VA 22161. Order Aviation Administration. Aircraft acci-#ADA106489/8. dent and incident notification, investi-
22. Dille JR, Booze CF Jr. The 1980 and 1981 gation, and reporting. FAA Orderaccident experiences of civil airmen with 8020.11.selected visual pathology. Washington, 28. Billings CE, Reynard WD. Human factorsDC: Department of Transportation/Fed- in aircraft incidents; result of a 7-yeareral Aviation Administration; 1983; FAA study. Aviat Space Environ Med. 1984;Report No. FAA-AM-83-18. Available study.from: National Technical Information 55:960-5.Service, Springfield, VA 22161. Order#ADA134898.
12 *U.S. GOVERNMENT r" mNG omN tIC-: . ,e