b. wozniewicz md phd
TRANSCRIPT

NEW TRENDS IN PARATHYROID ALLOTRANSPLANTATION,
Warsaw 2006
B. Wozniewicz MD PhD
Department of PathologyThe Childrens’ Memorial Health Institute, Warsaw
Biomedical Research Center, Warsaw

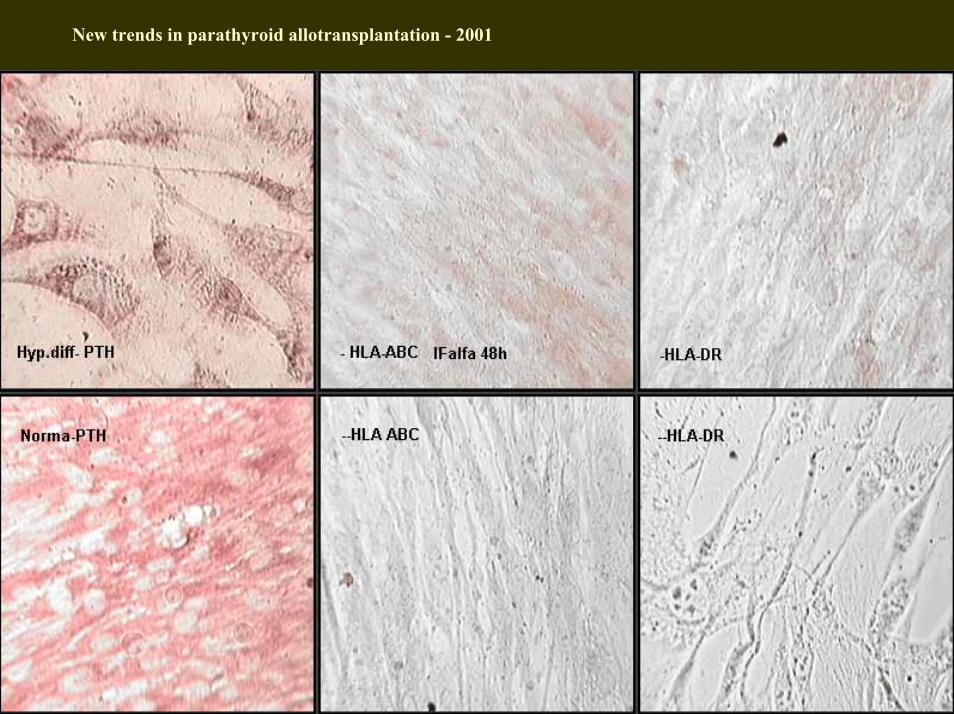
New trends in parathyroid allotransplantation - 2001
LyMac
End Fib
End
PTH
PTH PTH PTHPure PTH
Cell Culture TX
PTH
PTH
Ly
Ly
PTH
PTHPTH
PTH
PTH
PTH
PTH
PTH
No HLA Class II
PTH TX

New trends in parathyroid allotransplantation - 2001
Organ PTx Cell PTx
1. Devoid of immunogens2. Controlled selection3. No Rejection4. No immunosupression
1. Immunogenic epitopes 50%2. Surgical blind selection3. Rejection reaction4. Immunosupresion
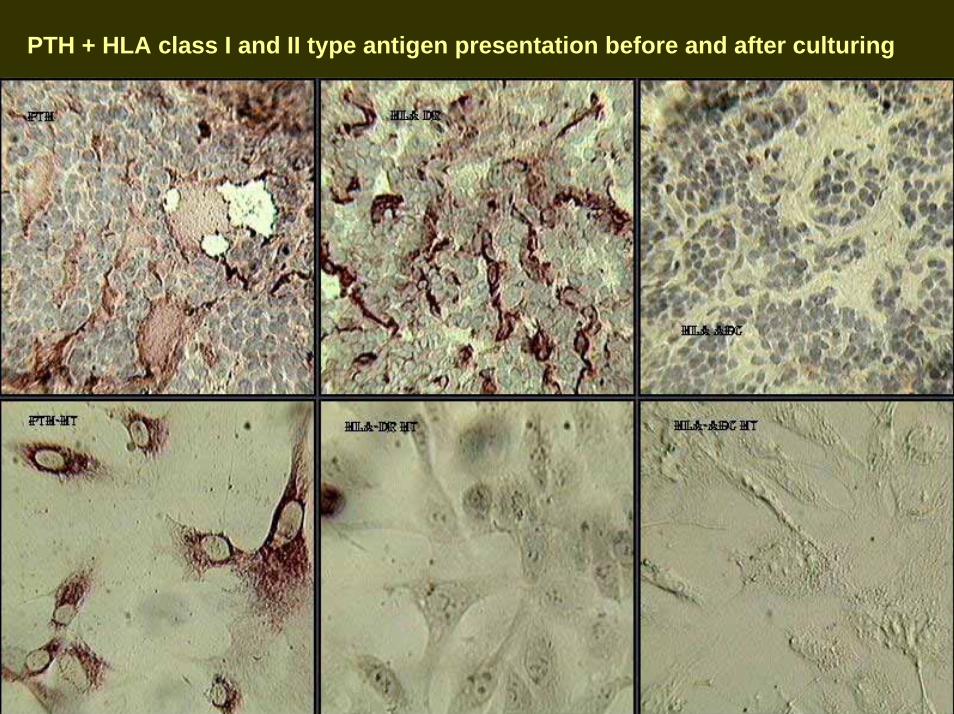
PTH + HLA class I and II type antigen presentation before and after culturing


New trends in parathyroid allotransplantation - 2001
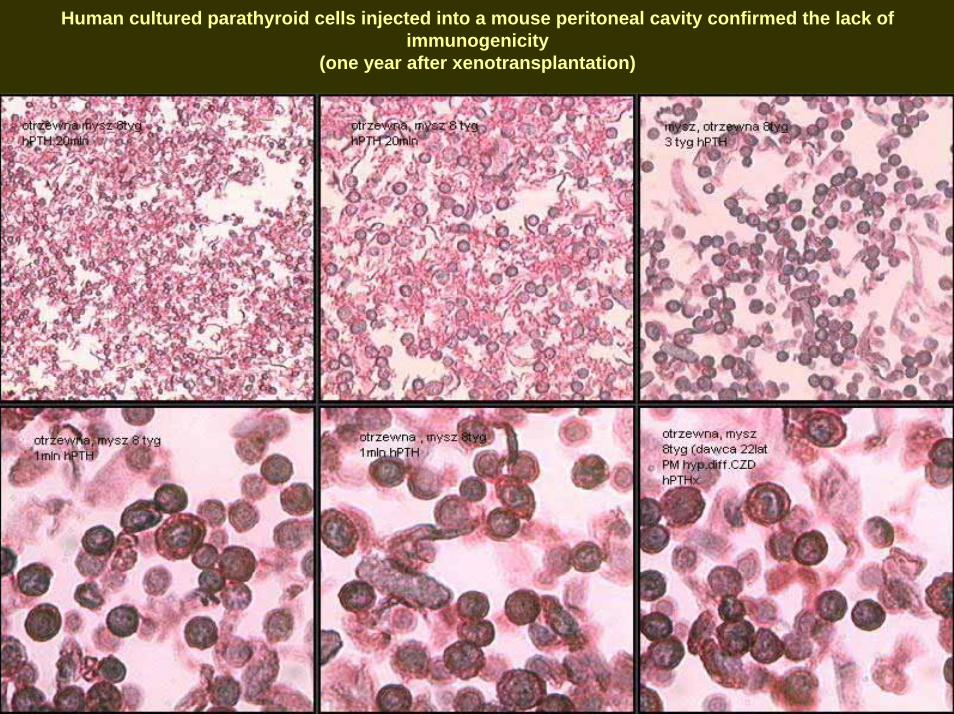
Human cultured parathyroid cells injected into a mouse peritoneal cavity confirmed the lack ofimmunogenicity
(one year after xenotransplantation)

New trends in parathyroid allotransplantation - 2001
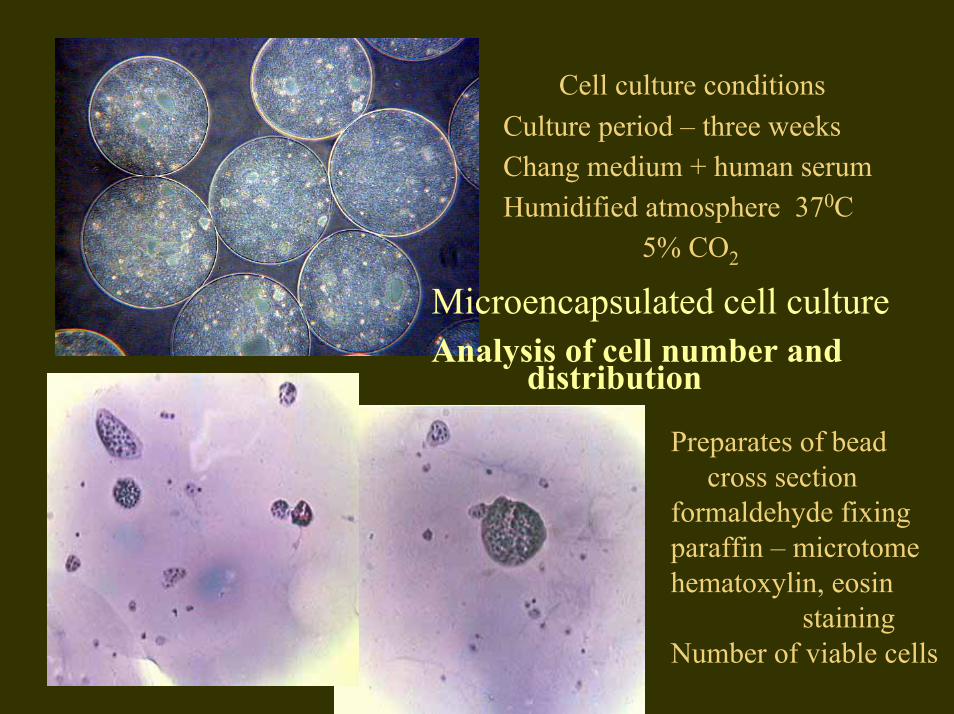
Microencapsulated cell cultureAnalysis of cell number and
distribution
Preparates of beadcross section
formaldehyde fixingparaffin – microtomehematoxylin, eosin
stainingNumber of viable cells
Cell culture conditionsCulture period – three weeksChang medium + human serumHumidified atmosphere 370C
5% CO2

Fixed samples of microencapsulated cell culture
Photos made after cell death
Alginate beads transferredto 0.9%NaCl + EtOH Olympus optical microscope, transmitted light
thanks to dr Korzynska, IBIB

New trends in parathyroid allotransplantation – 2001
Non Rejection Reaction
• 1. Problem of adhesion-failure• 2. Problem with capillary finding• 3. Problem with vasculature interaction• 4. Problem with programmed death• 5. Problem with local ischaemia• 6. Problem with monitoring • 7. Problem with recovery of HLA class-I

New trends in parathyroid allotransplantation - 2001
Supported by
Grant Nr PB 538/PO5/98/15State Committee for Scientific Research
Participants:
Prof.dr. T.Tołłoczko, Prof. dr . J. Szmit & Dr med. I. Nawrot Medical School Warsaw
Prof. Dr med. A. Gorski –Institute of Transplantology, Medical School Warsaw
Prof. Dr med. J.Kawiak & Prof. Dr Eng. A. WerynskiIBiIB Warsaw
Dr n med A. Sawicki Calcium Metabolism Center, Osteomed Warsaw
Prof. Dr hab. B.WozniewiczDep.Pathology, CMHI -Warsaw

Bogdan Woźniewicz
The Children’s Memorial Health Institute
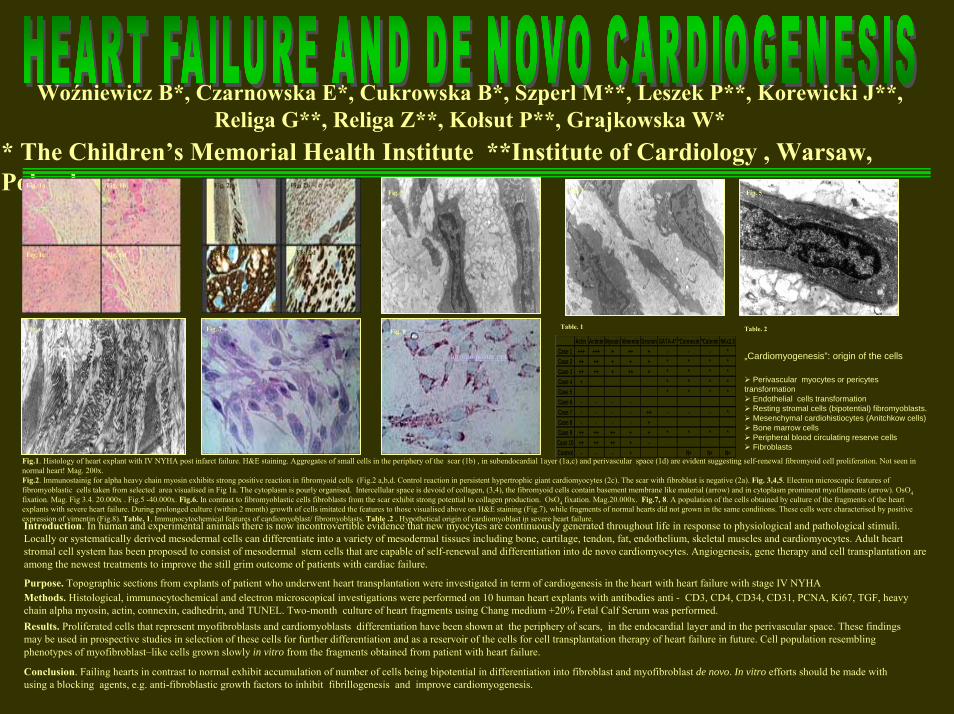
Woźniewicz B*, Czarnowska E*, Cukrowska B*, Szperl M**, Leszek P**, Korewicki J**, Religa G**, Religa Z**, Kołsut P**, Grajkowska W*
* The Children’s Memorial Health Institute **Institute of Cardiology , Warsaw,Poland
Introduction. In human and experimental animals there is now incontrovertible evidence that new myocytes are continuously generated throughout life in response to physiological and pathological stimuli. Locally or systematically derived mesodermal cells can differentiate into a variety of mesodermal tissues including bone, cartilage, tendon, fat, endothelium, skeletal muscles and cardiomyocytes. Adult heart stromal cell system has been proposed to consist of mesodermal stem cells that are capable of self-renewal and differentiation into de novo cardiomyocytes. Angiogenesis, gene therapy and cell transplantation are among the newest treatments to improve the still grim outcome of patients with cardiac failure.
Purpose. Topographic sections from explants of patient who underwent heart transplantation were investigated in term of cardiogenesis in the heart with heart failure with stage IV NYHAMethods. Histological, immunocytochemical and electron microscopical investigations were performed on 10 human heart explants with antibodies anti - CD3, CD4, CD34, CD31, PCNA, Ki67, TGF, heavy chain alpha myosin, actin, connexin, cadhedrin, and TUNEL. Two-month culture of heart fragments using Chang medium +20% Fetal Calf Serum was performed.Results. Proliferated cells that represent myofibroblasts and cardiomyoblasts differentiation have been shown at the periphery of scars, in the endocardial layer and in the perivascular space. These findings may be used in prospective studies in selection of these cells for further differentiation and as a reservoir of the cells for cell transplantation therapy of heart failure in future. Cell population resembling phenotypes of myofibroblast–like cells grown slowly in vitro from the fragments obtained from patient with heart failure.
Conclusion. Failing hearts in contrast to normal exhibit accumulation of number of cells being bipotential in differentiation into fibroblast and myofibroblast de novo. In vitro efforts should be made with using a blocking agents, e.g. anti-fibroblastic growth factors to inhibit fibrillogenesis and improve cardiomyogenesis.
Actin Actinin Myosin Vimentin Desmin GATA-4* *Connexin *Catenin NKx2.5Case 1 +++ +++ + ++ + - - - *Case 2 ++ ++ + + + * * * *Case 3 ++ ++ + ++ + * * * *Case 4 + * * * *Case 5 * * * *Case 6 - - - -Case 7 - - - - ++ - - - *Case 8 - - - - +Case 9 ++ ++ ++ + + * * * *
Case 10 ++ ++ ++ + -Control - - - + N+ N+ N+
„Cardiomyogenesis”: origin of the cells
Perivascular myocytes or pericytes transformation
Endothelial cells transformation Resting stromal cells (bipotential) fibromyoblasts.Mesenchymal cardiohistiocytes (Anitchkow cells)Bone marrow cellsPeripheral blood circulating reserve cellsFibroblasts
Fig. 1a
Fig. 1dFig. 1c
Fig. 1b Fig. 2a Fig. 2b
Fig. 2c Fig. 2d
Fig. 3 Fig. 5
Fig. 7
Fig. 4
Fig. 8Fig. 6 Table. 1 Table. 2
Fig.1. Histology of heart explant with IV NYHA post infarct failure. H&E staining. Aggregates of small cells in the periphery of the scar (1b) , in subendocardial 1ayer (1a,c) and perivascular space (1d) are evident suggesting self-renewal fibromyoid cell proliferation. Not seen in normal heart! Mag. 200x. Fig.2. Immunostainig for alpha heavy chain myosin exhibits strong positive reaction in fibromyoid cells (Fig.2 a,b,d. Control reaction in persistent hypertrophic giant cardiomyocytes (2c). The scar with fibroblast is negative (2a). Fig. 3,4,5. Electron microscopic features of fibromyoblastic cells taken from selected area visualised in Fig 1a. The cytoplasm is pourly organised. Intercellular space is devoid of collagen, (3,4), the fibromyoid cells contain basement membrane like material (arrow) and in cytoplasm prominent myofilaments (arrow). OsO4fixation. Mag. Fig 3.4. 20.000x . Fig.5 -40.000x. Fig.6. In contrast to fibromyoblastic cells fibroblasts from the scar exhibit strong potential to collagen production. OsO4 fixation. Mag.20.000x. Fig.7, 8. A population of the cells obtained by culture of the fragments of the heart explants with severe heart failure. During prolonged culture (within 2 month) growth of cells imitated the features to those visualised above on H&E staining (Fig.7), while fragments of normal hearts did not grown in the same conditions. These cells were characterised by positive expression of vimentin (Fig.8). Table. 1. Immunocytochemical features of cardiomyoblast/ fibromyoblasts. Table .2 . Hypothetical origin of cardiomyoblast in severe heart failure.
toronto poster.ppt

Wozniewicz B**, Czarnowska E**, Cukrowska B**, Szperl M*, Leszek P*, ReligaG*, Kołsut P*, Grajkowska W**, Szymańska-Dębińska T**, Korewicki J*, Religa
Z*.*Institute of Cardiology , Warsaw PL **Children’s Memorial Health
Institute, Warsaw PL
Introduction. In human and experimental animals there is now incontrovertible evidence that new myocytes and angiocytes may be generated throughout life in response to physiological and pathological stimuli. Adult heart stromal cell system has been proposed to consist of mesodermal stem cells that are capable of self-renewal into de novo cardiomyocytes. Similar stimuli e.g. prolonged hypoxy is able to stimulate de novo angiogenesis from endothelial cells. The rate of cell renewal is slow and low. In contrast to normal healthy heart the more severe heart failure the more chance in findings of angiogenesis and cardiogenesis is possible. The problem is haw to differentiate natural vascular system from neo-endotheliogenesis and vasculogenesis could be determined. This findings may be enhancement by application of various method of direct or indirect stimulation e.g. plasmides or autologous blood stem cell transplantation.
Aim. The aim of presentation is to introduce electron microscopic investigation for evaluation normal vessels from self-renewal angiocytes. Material and method. Electron microscopic examination were performed in specimens obtained from seven heart explains in patient with stage IV heart insufficiency (NYHA) undergoing heart transplantation.Material was performed in the routine way to Epon 812 (fixation in 3% glutaraldehyde, dehydration, OsO4 staining ). Semithin section stained with toluidine blue were selected using optic microscopy and ultrathin section were observed in Jeol 100CX EM. Additional staining using monoclonal CD31/PACAM-1 and polyclonal VEGF-1 antibodies were used for visualisation of vessels in paraffin embedded sections.Results. Monoclonal and polyclonal antibodies stain adult opened terminal vessels filled usually with erythrocytes. not aggregates of immature cells. Electron microscopy was useful to determine endothelial/angiocytes precursors from other cells since they present basement membrane and fenestration of the cytoplasm. Histologically in the routine examination angiogenesis was suggested when around the cardiocytes were observed not a single vessel but a plexus of vessels and endothelial cells.
Criteria of de novo vasculogenesis
Marker VEGF-1
CD31/Pecam
Immature cell aggregates - -Maturated cells with openings + +
Immunocytochemical
Adult capillaries + + StructureImmature cellaggregates
BM present
Maturated cellsFenestration presentCytopl. “openings” present
Electron microscopic
Adultcapillaries
Lumen +BM+++Membrana fenestrata +
Table. 1. Ultrastructural and immunocytochemical evidence of neovasculogenesis in heart explands with heart failure.
Fig. 1. Anti CD31/PECAM-1 monoclonal antibodies staining of capillaries in normal heart . Magn. 200x.
Fig. 2. Polyclonal antibodies anti VEGF-1 in heart explant with IV NYFA heart failure. De novo capillaries were stained positive. (arrow).Mag. 220x
Fig. 3. Electron microscopy of immature cells exchibiting presence of basement membrane like structure. OsO4 staining. Magnification 20.000 X
Fig. 4. Electron microscopy of two immature endothelial cells with opening (lumen) formation. OsO4 staining.Magnification 20.000X
Fig. 5. Immature angiocytes not forming de novo vessels becameapoptotic (arrow). OsO4 staining.Magnification 20.000X
Conclusion. Electron microscopy is useful in qualification of self-renewal angiogenesis in the heart with severe failure.

IV Konferencja Otolaryngologów Polskich i Francuskich
Warszawa 18-19 Listopada 2005
HODOWLA KOMHODOWLA KOMÓÓREK REK PROGENITOROWYCH PROGENITOROWYCH Z Z
PRZEWODU PRZEWODU ŚŚLIMAKOWEGO LIMAKOWEGO
CultureCulture ofof progenitorprogenitor cellscells fromfrom thethe
cochleacochleaB. Cukrowska1, K. Niemczyk2, K. Pietrasik2, A. Bruzgielewicz2, K. Morawski2,
B. Biskup2, M. Pronicki1, A. Zajączkowska1, B. Woźniewicz1
1 Instytut „Pomnik - Centrum Zdrowia Dziecka” Zakład Patologii Kierownik Doc. dr hab. M. Pronicki
2 Katedra i Klinika Otolaryngologii Akademii Medycznej w WarszawieKierownik Prof. dr hab. n med. K. Niemczyk

Thymic progenitor cells
Narodowy program regeneracji i transplantacji Grasicy 2007-2009

Transplantacje komórek• Realizacja u człowieka• Przytarczyce od 1993 Warszawa skuteczne• Trzustka wiele ośrodków nieskuteczne• Komórki nerwowe dopamina zwierzęta • Komórki sercowe – w toku• Komórki akustyczne experymenty, zwierzeta• Komórki grasicy – USA skutecznie• Komórki wątrobowe – experymenty zwierzeta• Skóra – skuteczne• Keratinocyty - skuteczne