back to the bedside: internal medicine bedside ultrasound program
TRANSCRIPT

BACK TO THE BEDSIDEThe Internal Medicine Bedside UltraSound Program
!!!
IMBUS#David Tierney, MD FACP
Abbott Northwestern Hospital - Dept.Director - IMBUS Program
Assoc.


POINT OF CARE ULTRASOUND: POCUS
Clinician: Focused Question in Focused Timing/Situation

POCUS
Clinician: Obtain images to answer that question

POCUS
Clinician: Interpretation of Adequate Image

POCUS
Clinician: Integration of interpretation into the rest of the clinical picture IN REAL TIME

POCUS
Clinician: Come back and check again after a treatment/intervention

• A few cases
• Why did we start it?
• What does it take?• Training & Resources
• What do we get out of it• AKA “Why are we still doing it”
• What don’t we know yet?

BACK TO THE BEDSIDE
• CASE #1: 78 yo female
•ANGMA at Center for Outpatient Care
•“I have a sinus infection and need some antibiotics”

1
2
3

BACK TO THE BEDSIDE
• CASE #2: 38 yo female
•ANGMA resident clinic
•New patient establishing care post cholecystectomy
•Doing well, but some sob increasing since prior to surgery, getting much worse now. Legs a little swollen.
•Pulse 110, BP 92/70
ANGMA Resident Clinic


BACK TO THE BEDSIDE
• CASE #3: 48 yo female
•ANGMA resident clinic
•bit by a bug while camping last week, got Augmentin without improvement in cellulitis

BACK TO THE BEDSIDE
• CASE #4: 82 yo male
• In hospital with acute on chronic renal insufficiency. Minimal urine output and abdominal pain. Foley draining some urine but tapering off last 48hrs. Bladder scanner = 60cc


BACK TO THE BEDSIDE• CASE #5: 59 yo male, establishing care at ANGMA COC clinic
•no medical problems
•“sick as a dog” for 3mo
•fevers off/on, sweats, exhausted
•multiple urgent care and allergist visits
•extensive lab w/u, trials empiric abx
•allergist concerned for possible lymphoma
•BP 92/50, pluse 80, temp 99.4F
•systolic murmur throughout

BACK TO THE BEDSIDE• CASE #5: 59 yo male, establishing care at ANGMA COC clinic
•no medical problems
•“sick as a dog” for 3mo
•fevers off/on, sweats, exhausted
•multiple urgent care and allergist visits
•extensive lab w/u, trials empiric abx
•allergist concerned for possible lymphoma
•BP 92/50, pluse 80, temp 99.4F
•systolic murmur throughout

BACK TO THE BEDSIDE
• CASE #6: 60 yo male
•HD# 16: Sepsis, ARDS, On/Off Ventilator
•2:15AM in ICU:
•Acute Hypotension, hypoxia

BACK TO THE BEDSIDE
• CASE #6: 60 yo male
•HD# 16: Sepsis, ARDS, On/Off Ventilator
•2:15AM in ICU:
•Acute Hypotension, hypoxia
• PEA Arrest
Hypovolemia Hypoxia
Hydrogen ion (acidosis) Hypoglycemia Hypo/Hyperkalemia Hypothermia Tension Ptx Tamponade Toxins
Thrombosis
PEA
ObstructionVolume Pump
Ptx Tamponade PE

BACK TO THE BEDSIDE30”
30”
15”

BACK TO THE BEDSIDE
• Case #s 7-182: Short of Breath Patient

“B-LINES”

PNEUMONIA

• A few cases
• Why did we start it?
• What does it take?• Training & Resources
• What do we get out of it• AKA “Why are we still doing it”
• What don’t we know yet?

WHY DID IT START HERE?one of the national leaders in IM POCUS
!!!
IMBUS#

WHY HERE, WHY NOW?
• Procedural Safety & Standard of Care
• Medical Students, Residents, Fellows
• Global Health & Limited Resource Locations
• Patient Communication, Understanding & Satisfaction
• Better Patient Care

Central lines Less complica,ons OR 0.43 (0.22-‐0.87) Less failed inser,ons OR 0.14 (0.06-‐0.33) AHRQ 1 of 12 most highly rated pa,ent safety prac,ces to reduce medical errors
Thoracentesis Ptx: 4% vs. 9% (OR 0.3 [0.2-‐0.7]) Training ins,tu,on ptx rates
(10% vs. 5%) & (18% vs. 3%) 10% underlying solid organ with clinically selected site Easily obtained ultrasound skill by house staff and intensivists 1hr training session
Paracentesis Success rate 95% vs. 65% (P = .0003)
Emerg Med Residents & Staff <1% bleed or bowel perf complica,on rate with blind & ultrasound
Lumbar Puncture Successful LP: OR 1.32 US vs. Tradi,onal landmark Iden,fica,on of landmarks in obese pts. BMI>30 = 75%
BMI >30: OR 2.3 US vs. Tradi,onal landmark
Hind, et al. BMJ. 2003; 327(7411): 361-‐368. Agency for Healthcare Research and Quality. (AHRQ publica,on no. 01-‐E058.)
Gordon, et al. Arch Intern Med. 2010; 170 (4): 332-‐339. Daniels, C, Ryu, J. Current Opinion in Pulmonary Medicine 2011, 17:000–000.
Diacon AH, et al. Chest 2003; 123:436–441. Mayo, et al. Chest 2004;125;1059-‐1062.
Nazeer Am J Emer Med 2005; 23(3):363 -‐367. McGibbon. Dig Dis Sci 2007; 52:3307–3315.
Wong, et al. JAMA. 2008; 299(10):1166-‐1178. Nomura J, et al. J Ultrasound Med 2007;26;1341-‐8.
It is easily learned, evidence-‐based, and “best prac<ce”

• Procedural Safety & Standard of Care
• Medical Students, Residents, Fellows….A.K.A “the future”
• Global Health & Limited Resource Locations
• Patient Communication, Understanding & Satisfaction
• Better Patient Care
WHY HERE, WHY NOW?

MEDICAL SCHOOL PUSH

• Procedural Safety & Standard of Care
• Medical Students, Residents, Fellows
• Global Health & Limited Resource Locations
• Patient Communication, Understanding & Satisfaction
• Improved Diagnostic Ability as Internists
WHY HERE, WHY NOW?

• Procedural Safety & Standard of Care
• Medical Students, Residents, Fellows
• Global Health & Limited Resource Locations
• Patient Communication, Understanding & Satisfaction
• Improved Diagnostic Ability as Internists
WHY HERE, WHY NOW?

The Physician-Patient RelationshipIMBUS#

• Procedural Safety & Standard of Care
• Medical Students, Residents, Fellows
• Global Health & Limited Resource Locations
• Patient Communication, Understanding & Satisfaction
• Improved Diagnostic Ability as Internists = Better, more efficient patient care
WHY HERE, WHY NOW?

Physical Finding ExamSens% (LR-) Spec% (LR+)
AAA 22-68 (0.6) 75-99 (7.6)Ascites Flank Dullness 80-94 (0.3) 29-69 (NS) Shifting Dullness 60-87 (0.4) 56-90 (2.3) Fluid Wave 50-80 (0.5) 82-92 (5.0)Splenomegaly 18-69 (0.6) 89-99 (9.6)Hepatomegaly 50-71 (0.5) 56-77 (1.7)Hypovolemia Dry Axilla 50 (NS) 82 (2.8) Dry MM 85 (0.3) 58 (NS)Volume overload 3rd Heart Sound 13 (0.8) 99 (11) JVD 39 (0.6) 92 (5.1) Abd Jugular Reflux
24 (0.8) 96 (6.4) (*CT Scan as Gold Standard) Lichtenstein. Anesthesiology 2004; 100:9 –15

• A few cases
• Why did we start it?
• What does it take?
• Training & Resources
• What do we get out of it• AKA “Why are we still doing it”
• What don’t we know yet?

THE NUTS & BOLTS!!!
IMBUS#

IMBUS SPECTRUM OF CARE

Basics of Ultrasound Physics, Ar,facts, Bio effects Portable ultrasound machine mechanics and knobology Bedside ultrasound mechanics in a pa,ent room Pa,ent discussion & consent Draping of male/female pa,ents Image annota,on Integra,ve approach to clinical decision making at the bedside
Pulmonary Ultrasound Pleural ultrasound – A-‐Lines, lung sliding, Pneumothorax, pleural effusion Inters,,al syndromes – B-‐Lines Alveolar syndromes – consolida,on, atelectasis
Cardiovascular Ultrasound Windows: Parasternal long/short Axis, Apical 4/5, LA & 2 chamber, Subxyphoid 4-‐chamber and short axis
Pericardial assessment Assessment of LV and RV func,on Semi-‐quan,ta,ve assessment of clinically significant valvular dysfunc,on Assessment of diastology & dysfunc,on* Qualita,ve assessment of chamber size and overload Semi-‐quan,ta,ve assessment of volume status and fluid responsiveness -‐ E/e’, Cardiac Output, Passive Leg Raise, etc.
Assessment of aorta for aneurysm * Vascular 2-‐point DVT screening *
Abdominal Ultrasound Urinary
Renal evalua,on for hydronephrosis Kidney findings in chronic kidney disease Bladder assessment
Hepatobiliary Assessment for hepatomegaly Findings in cirrhosis Assessment of the gallbladder and CBD *
Assessment for splenomegaly Peritoneal free fluid evalua,on Bowel
Assessment for ileus and small bowel obstruc,on Assessment of inflammatory bowel states *
SoC Tissue Ultrasound Lymphadenopathy * Celluli,s and Abscess
HEENT Ultrasound Thyroid ultrasound * Ocular ultrasound * Sinus ultrasound ICP assessment with op,c nerve sheath * Real-‐,me intuba,on guidance and confirma,on
Musculoskeletal Ultrasound Assessment of the symptoma,c joint, bursa, tendon/ligament *
Procedural Ultrasound Central and peripheral venous and arterial line placement Thoracentesis Lumbar puncture Paracentesis Abscess I&D Endotracheal tube placement verifica,on Central venous line placement verifica,on Joint, sos ,ssue, and bursa injec,ons

IMBUS TRAINING
1 12 13 16 16 12 11 10
Core Faculty
Resident G1/2s
Resident G1/3s Staff Physicians Hospitalists
ClinicIntensivists
ED
2011 2012 2012 20132006
Resident G1s and staff
2013 2014
Resident G1s Intensivists
Telecardiology NPs
2014
2
1
2013
Outpatient IM Staff
CLINICAL WORKFLOW

!!!
IMBUS#

ANW Center for Outpatient Care
ANGMA Resident Clinic



Pulmonary Cardiac & Fluid Abdominal MSKL Soft Tissue HEENT Vasc
!!!
IMBUS#

TimeCompensation Models
Politics & Turf
All vs. Core Group
Bottom Up
Trainer Bottleneck
!!!
IMBUS#
Personal Skill & Motivation
Machines

• A few cases
• Why did we start it?
• What does it take?• Training & Resources
• What do we get out of it
• AKA “Why are we still doing it”
• What don’t we know yet?

TEACHING PHYSICAL EXAM
!!!
IMBUS#

S1
LA
LV
Ao
S1 S2 S1Systole
A2,P2M1,T1 M1,T1
Diastole
S2

PATIENT SATISFACTION & UNDERSTANDING

BIG IMPACTS

LITTLE IMPACTS

change management confirm management avoid additional resources
!!!
IMBUS#

BETTER INTERNISTS & SUBSPECIALISTS
!!!
IMBUS#

RECRUITING & CAREERS

• A few cases
• Why did we start it?
• What does it take?• Training & Resources
• What do we get out of it• AKA “Why are we still doing it”
• What don’t we know yet?

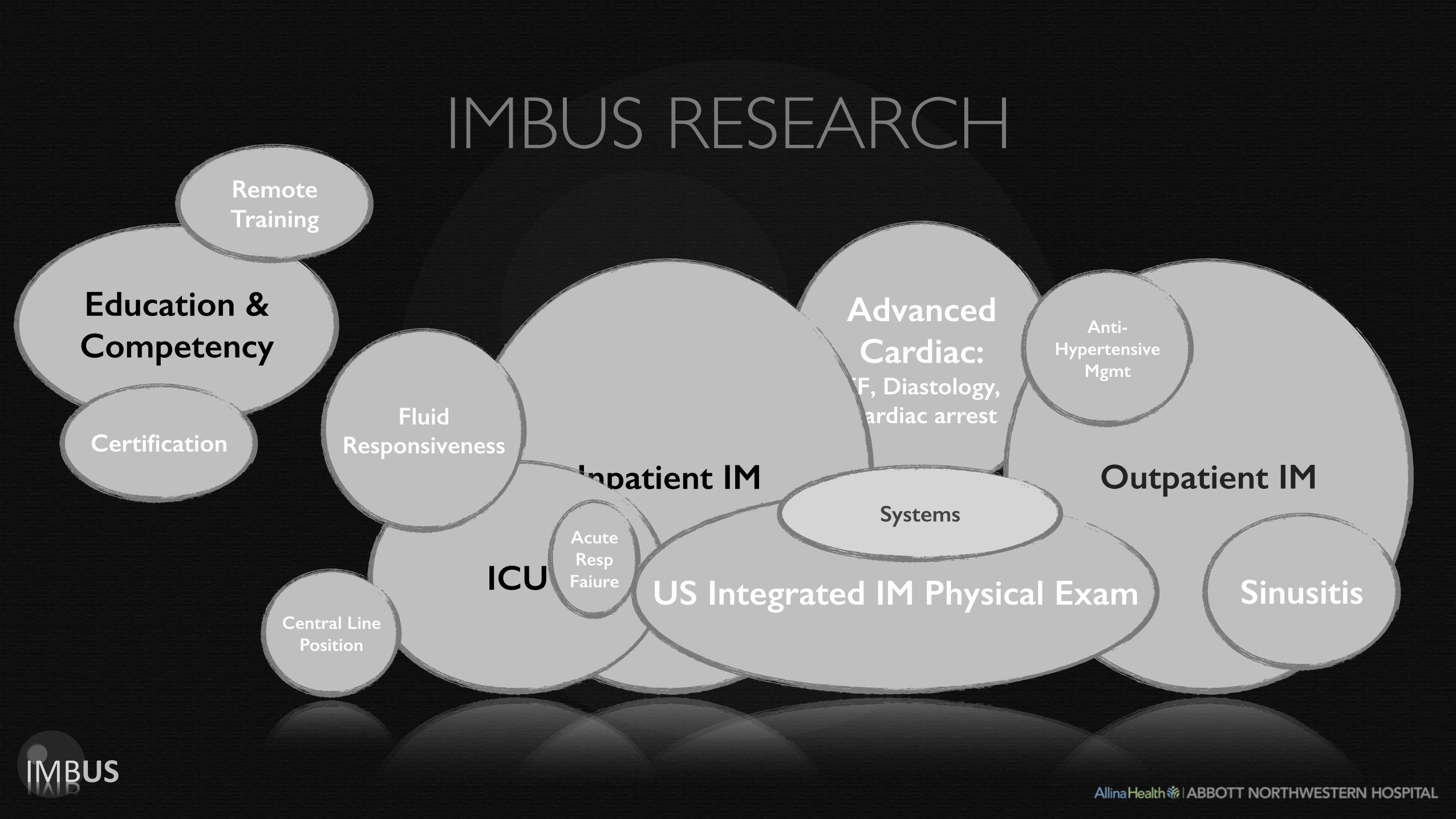
Advanced Cardiac:
EF, Diastology, Cardiac arrest
IMBUS RESEARCH
Outpatient IMInpatient IM
ICU US Integrated IM Physical Exam
Fluid Responsiveness
Anti-Hypertensive
Mgmt
Central Line Position
Sinusitis
Acute Resp
Faiure
Systems
!!!
IMBUS#
Education & Competency
Remote Training
Certification

Advanced Cardiac:
EF, Diastology, Cardiac arrest
IMBUS RESEARCH
Inpatient IM
ICU
Fluid Responsiveness
Anti-Hypertensive
Mgmt
Central Line Position
Sinusitis
Acute Resp
Faiure
Systems
!!!
IMBUS#
Education & Competency
Remote Training
CertificationOutpatient IM
US Integrated IM Physical Exam

HYBRID PRIMARY CARE PHYSICAL EXAM
ANW Center for Outpatient CareANGMA Resident Clinic
Advanced Cardiac:
EF, Diastology, Cardiac arrest
IMBUS RESEARCH
Outpatient IMInpatient IM
ICU US Integrated IM Physical Exam
Fluid Responsiveness
Anti-Hypertensive
Mgmt
Central Line Position
Sinusitis
Acute Resp
Faiure
Systems
!!!
IMBUS#
Education & Competency
Remote Training
Certification

Advanced Cardiac:
EF, Diastology, Cardiac arrest
IMBUS RESEARCH
Outpatient IM
US Integrated IM Physical Exam
Fluid Responsiveness
Anti-Hypertensive
Mgmt
Central Line Position
Sinusitis
Acute Resp
Faiure
!!!
IMBUS#
Education & Competency
Remote Training
Certification
ICU
Inpatient IMSystems

Terry Rosborough, MD FACP!David Tierney, MD FACP!
!Department of Medical Education!Abbott Northwestern Hospital!
!
The IMBUS-PCI Study:!Internal Medicine Bedside UltraSound !
Patient Care Improvement Study!
To#be#Top#10%…#
Cost#Reduc2on#
Length#of#stay#&#ICU#days#
Diagnos2c#Efficiency#
Reduc2on#in#costly#imaging#
Reduc2on#in#unnecessary#
medica2on#use#
Pa2ent#Care#
Safety#
Time#to#Dx/Tx#
Length#of#stay#
Less#Radia2on#(XJray/CT#Scan)#
Pa2ent#Experience#
Physician#Communica2on#
Pt.#Understanding#
Pt/Physician#Rela2onship#
Leader#
Recruit#
Top#Decile#
To#be#Top#10%…#
Cost#Reduc2on#
Length#of#stay#&#ICU#days#
Diagnos2c#Efficiency#
Reduc2on#in#costly#imaging#
Reduc2on#in#unnecessary#
medica2on#use#
Pa2ent#Care#
Safety#
Time#to#Dx/Tx#
Length#of#stay#
Less#Radia2on#(XJray/CT#Scan)#
Pa2ent#Experience#
Physician#Communica2on#
Pt.#Understanding#
Pt/Physician#Rela2onship#
Leader#
Recruit#
Top#Decile#
To#be#Top#10%…#
Cost#Reduc2on#
Length#of#stay#&#ICU#days#
Diagnos2c#Efficiency#
Reduc2on#in#costly#imaging#
Reduc2on#in#unnecessary#
medica2on#use#
Pa2ent#Care#
Safety#
Time#to#Dx/Tx#
Length#of#stay#
Less#Radia2on#(XJray/CT#Scan)#
Pa2ent#Experience#
Physician#Communica2on#
Pt.#Understanding#
Pt/Physician#Rela2onship#
Leader#
Recruit#
Top#Decile#
13,000 Patients

Advanced Cardiac:
EF, Diastology, Cardiac arrest
IMBUS RESEARCH
Outpatient IMInpatient IM
ICU US Integrated IM Physical Exam
Fluid Responsiveness
Anti-Hypertensive
Mgmt
Central Line Position
Sinusitis
Acute Resp
Faiure
Systems
!!!
IMBUS#
Education & Competency
Remote Training
Certification

Advanced Cardiac:
EF, Diastology, Cardiac arrest
IMBUS RESEARCH
Outpatient IMInpatient IM
ICU US Integrated IM Physical Exam
Fluid Responsiveness
Anti-Hypertensive
Mgmt
Central Line Position
Sinusitis
Acute Resp
Faiure
Systems
!!!
IMBUS#
Education & Competency
Remote Training
Certification

EDUCATION & COMPETENCY

Advanced Cardiac:
EF, Diastology, Cardiac arrest
IMBUS RESEARCH
Outpatient IMInpatient IM
ICU US Integrated IM Physical Exam
Fluid Responsiveness
Anti-Hypertensive
Mgmt
Central Line Position
Sinusitis
Acute Resp
Faiure
Systems
!!!
IMBUS#
Education & Competency
Remote Training
Certification

As internists, we orchestrate some of medicine’s most complex hunts.
The tools we search with are one half of the equation.
The ability to recognize & integrate what we find is the other half.
However, neither gets us anywhere without a patient relationship.
!!!
IMBUS#

Thank you
David Tierney, MD FACPAbbott Northwestern Hospital - Dept of Med Ed
Director - IMBUS ProgramAssoc. Prog. Dir. - IM Residency Program
Email: [email protected]
!!!
IMBUS#