barnsteiner - university of vermontkappatau/images/2015orals/barnsteiner_keynote.pdf · 11/3/2015 1...
TRANSCRIPT

11/3/2015
1
Jane Barnsteiner, PhD, RN, FAANProfessor Emerita, University of Pennsylvania School of Nursing
Editor, Translational Research and QI, AJNNovember 6, 2015
Health Professions Education
6 Core Competencies:1. Provide patient‐centered care
2. Work in interdisciplinary teams
3. Employ evidence‐based practice
4 Safety as a system property4. Safety as a system property
5. Apply quality improvement
6. Utilize informatics
11/3/2015
2
IOM Competencies
PCC
Teamwork
EBPTeamwork
&
Collaboration
Quality Improvement
Safety
Informatics
Evidence-Based Practice Old – Adhere to internal
policies and procedures. New - Integrate best
d h current evidence with clinical expertise and patient/family preferences and values for delivery of optimal health care.
Why the focus on EBP?• Leads to higher quality of care, improved patient outcomes, decreased costs, and greater nursing satisfaction.
• Significant gaps in care:
30 40% d t i t t t• 30 – 40% do not receive treatments proven effective,
Antibiotics before and after surgery
Hand hygiene 100% of the time
• 20 – 25% receive treatments that are not needed or are potentially harmful
Indwelling catheters post‐op or in ICU
11/3/2015
3
Locating and Retrieving the Evidence
The World of Evidence
PublishedEvidence
Indexed and Indexed and Locatable
Accessible and Reviewable
Use
EBP ‐ Staff nurse use of research( Yoder, AJN, 9/14)
Where do you get your evidence?
Personal Experience – 75%
Policies and Procedures 58%
Peers 55%
Intuition – 32%
Use of journals, internet – 25%
36% avoid using research as they perceive they do not have authority to use even if useful.
Do I hear myself saying… We’ve always done it this way That’s not our way As soon as this change is over, we can do it I’m just not comfortable with change It’s just not the way it used to be I’m just not a creative person

11/3/2015
4
2015 National Survey‐ Sacred CowsPractice True False
Shock ‐
Trendelenburg
51% 49%
Scrub the hub 81% 19%
Instill NSS NTT 35% 65%
Auscultate G‐
tube
31% 69%
Ph testing G‐
tube
51 49%
Aspirate
subglottic
secretions to
prevent VAP
29% 71%
Willful Blindness Conscious avoidance, not challenging the status quo
12 hour shifts lead to increased safety errors
Increased staffing leads to decreased adverse events, LOS, and is cost neutral
Faculty adding their name to junior faculty and student papers when not met criteria for authorship
Incivility and bullying
Patient/Family Centered Care Old – Listen to patient and
demonstrate compassion and respect.
American Association of Colleges of Nursing. © 2010 - All Rights Reserved.
New - Recognize the patient or designee as the source of control and full partner in providing compassionate and coordinated care based on respect for patient’s preferences, values and needs
11/3/2015
5
New Focus “Knowledge is power.”Angelina Jolie Pitt:, Diary of a Surgery, NYT 3.24.15
Patient‐Centered Care“‐ is providing care that is respectful of and responsive to individual patient preferences, needs, and values and ensuring that patient values guide all clinical decisions” (Institute of Medicine)
Orthopedist goal – uneventful hip replacement surgery
Nursing goal – discharge with no complications
Patient goal – be back on golf course
(Need to begin to measure patient goal outcomes)
“It’s all about the patient”Not true
It’s about cost
It’s about completing the checklist It s about completing the checklist
It’s about physician schedule
It’s about us being in charge as we are the most knowledgeable

11/3/2015
6
Benefits of PFCCPerson Outcomes Patients more involved in their care are better able to
Manage complex chronic conditions
Seek appropriate assistance
Have reduced lengths of stay and avoidable readmissions and emergency department visits
Experience increased patient satisfaction and employee engagement(Jarousse, 2011)
Barriers Attitudes
When physicians and nurses perceive that family members are “policing” them, or that unrestricted visiting by family members is “not possible” it speaks to a culture ‐ but not amembers is not possible it speaks to a culture but not a culture of P&FCC.
AJCC, 2014
Knowledge – studies for past 40 years
Skill – HC professionals often novices with the new definition. Reason for push‐back on handoffs and rounds in patient rooms.
Patient Engagement and Activation – not anymore about handing out instructions and doing discharge teaching.
Engagement
Activation
Patient Activation Measure (PAM)(Hibbard, et al, 2005)
Plan interventions based on level of activation

11/3/2015
7
Patient EngagementEvidence-based approaches that lead to patient engagement, activation and improved clinical outcomes:
Medical literacy Shared decision making Goal settingSelf-care skills Motivation/confidence Plans of care
Patient Activation Measure (Hibbard)
Lucille‐Packard Children’s Hospital
11/3/2015
8
EB Benefits of PFCC ‐ Financial Outcomes
100 Planetree healthcare institutions
Increased patient satisfaction
Increased staff retention
Enhanced staff recruitment Enhanced staff recruitment
Decreased length of stay
Decreased emergency department return visits
Decreased adverse events including fewer medication errors
Reduced operating costs’ and a lower cost per case
Increased market share
Improved liability claims experience
Collaboration and Teamwork
Old – Work side by side with other HC professionals while performing nursing skills.
American Association of Colleges of Nursing. © 2010 - All Rights Reserved.
New - Function effectively within nursing and inter-professional teams, fostering open communication, mutual respect, and shared decision-making to achieve quality patient care
EB Benefits of Interprofessional Teamwork and Collaboration
• Improved mortality outcomes and quality of life after adjustment for patient severity
• Increased patient and family satisfaction with care
I d i f i fli• Improved team perception of micro‐system conflict management, collaboration, job satisfaction and quality of care
11/3/2015
9
Integrate TW&C
Team STEPPS, Crucial Conversations – communication
Interprofessional experiences in orientation and regular discussion on work area
i b f li d lf Patient as member of team – literacy and self‐management
Incivility not tolerated
Care Coordination – integrator role
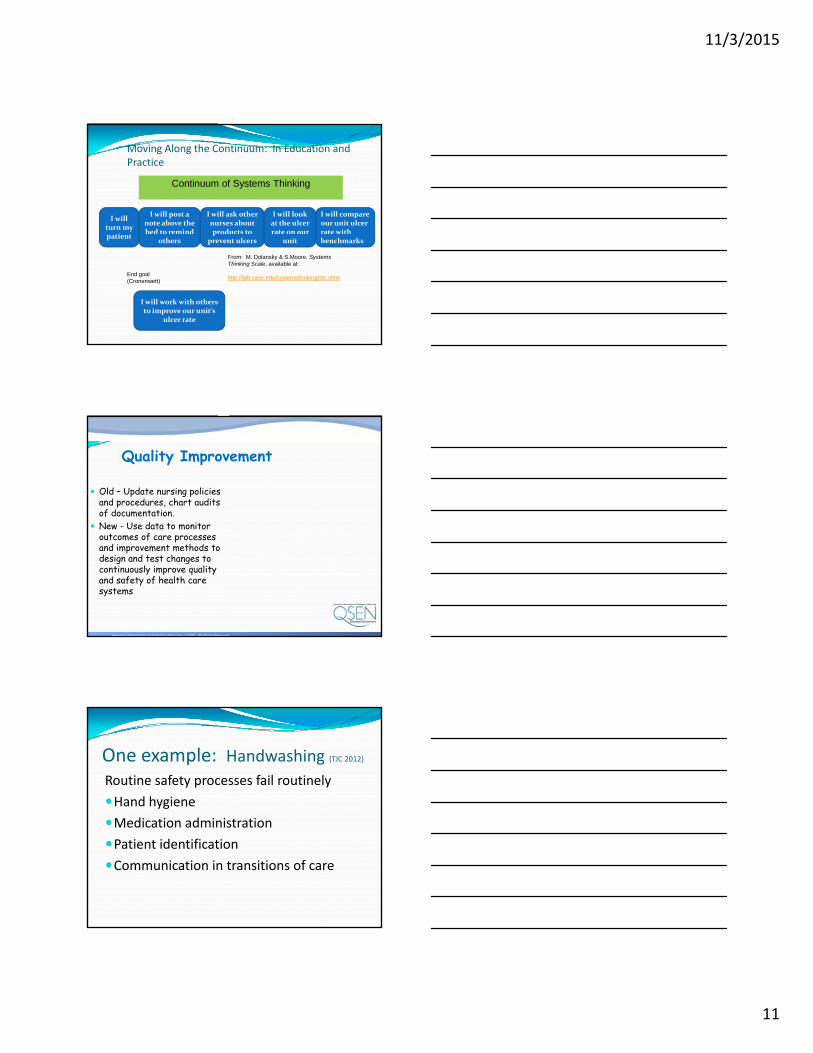
Safety
Old – focus on individual performance, vigilance to keep patients safe.
k f
American Association of Colleges of Nursing. © 2010 - All Rights Reserved.
New - Minimize risk of harm to patients and providers through both system effectiveness and individual performance
van der Schaaf‐ modified for healthcare
Technical
Organi-zational
Adequatedefenses
Return to Normal
Close Call
Dangerous Situation
Dangerous Situation
HumanFactors
defenses
DevelopingErrors
ERRORERROR(Inadequate Defenses)
PatientFactors

11/3/2015
10
Quality and Safety:Two Forms of Vigilance
Optimal Patient Care
Vigilant Individual
Care (Traditional)
Vigilant Systems of
Care( ad t o a )
• Patient Centered Care• Teamwork & Collaboration• Evidenced Based Practice• Safety • Quality Improvement• Informatics
QSEN
Mary Dolansky2012 QSEN National Forum
11/3/2015
11
I will turn my
ti t
I will post a note above the bed to remind
I will ask other nurses about products to
I will look at the ulcer rate on our
I will compare our unit ulcer rate with
Continuum of Systems Thinking
Moving Along the Continuum: In Education and Practice
patientothers
pprevent ulcers unit benchmarks
From: M. Dolansky & S.Moore. Systems Thinking Scale, available at:
http://fpb.case.edu/systemsthinking/sts.shtm
I will work with others to improve our unit’s
ulcer rate
End goal (Cronenwett)
Quality Improvement
Old – Update nursing policies and procedures, chart audits of documentation.
New Use data to monitor
American Association of Colleges of Nursing. © 2010 - All Rights Reserved.
New - Use data to monitor outcomes of care processes and improvement methods to design and test changes to continuously improve quality and safety of health care systems
One example: Handwashing (TJC 2012)
Routine safety processes fail routinely
Hand hygiene
d dMedication administration
Patient identification
Communication in transitions of care

11/3/2015
12
Informatics - HIT
Old – timely and accurate documentation
American Association of Colleges of Nursing. © 2010 - All Rights Reserved.
New - Use information and technology to communicate, manage knowledge, mitigate error, and support decision-making
Decision Support Aids "What clinicians need is decision support tools that fit into their workflow and remind them of evidence‐based practices” S. Baacken, Columbia School of Nursing
With electronic decision support aids clinicians:
7 times more likely to diagnose obesity
5 times more likely to spot issues in tobacco use
44 times more likely to identify depression in adults
4 times more likely to identify depression in children and adolescents
11/3/2015
13
Headache Diary
What It Is: Tracks every detail (including triggers and remedies) with recurring headaches.Why It's Cool: By keeping detailed notes of headache symptoms—right down to the location, duration, and foods you snacked on before the headache flared—you can help your health provider diagnose you more easily and begin treating you quickly.Cost: Free. Available for Android
Health Patch MDAbout the size of a Band‐Aid
and tracks heart rate, heart rate variability, respiratory rate, ECG and skin temperature continuously.p y
Can be worn constantly for three days before it needs to be replaced. The stats it collects can be sent to physician in real time via the cloud.
Nutrition ‐ ShopwellWhat It Is: With a quick scan of a barcode, this app can determine which foods meet your dietary needs.Why It's Cool: Shopwellpersonally scores each product personally scores each product just for you based on your age, gender, health goals, diet needs, and ingredient and nutrition preferences. Scores range from 0‐100; the higher the number, the better the product is for you.Cost: Free. Available for iOS

11/3/2015
14
Evidence to Action
40
Institutional Barriers to EBPLack of budget for information resources
Lack of budget for training in resource use
CNO belief that EBP not achievable in “real world”
Individual Barriers to Use of Evidence Lack of time Lack of value for research in practice Lack of knowledge about research Lack of computer skillsL k f d t di f l t i d t b Lack of understanding of electronic databases
Lack of access to computer and library Lack of search skills Lack of skills to critique or synthesize the literature Difficulty accessing research materials Difficulty understanding research articles
Funk et al, 1995; Kajermo et al, 1998; Omery et al, 1999; Parahoo, 1998; Rodgers, 2000 Provikoff, 2005

11/3/2015
15
EBP Culture change necessary among health care providers to understand that life‐long learning has an equal priority as delivering care.
Health care providers are incentivized for staying t d tup to date.
Greater efforts are needed to provide (commercial free) synthesized knowledge that is easily translated into practice briefs, guidelines and policies. These need to be regularly updated as new knowledge is generated. All too often guidelines are published but not kept current.
Creating a Culture of EBPAccelerate uptake
Awaken the spirit of inquiry
Patients and Families Expect CompetencePatients and Families Expect Competence
They don’t say “I prefer you care for me by the standards and guidelines, policies and procedures of 10 years ago”.
Formal Methods of Dissemination • Standards of Practice
• Practice Guidelines and Protocols
• Decision support systems
• Improved technology ‐ Smart pumps
11/3/2015
16
Informal Methods of Dissemination• Brown Bags
• Journal Clubs
• NewslettersNewsletters
• Professional Meetings/Conferences
Choosing Wisely Campaign(ABIM & AAN, 2014)Don’t
1. Automatically initiate continuous electronic FHR
2. Let oldsters lay in bed or be in chair during hospitalization
3. Use physical restraints for oldsters
4. Wake for routine care
5. Place or maintain UC without specific indication
The Choosing Wisely®, “Things Nurses and Patients Should Question,” identified by ONS include (4.23.15):
Don’t neglect to advise patients with cancer to get physical activity and exercise during and after treatment to manage fatigue and other symptoms.
Don’t use L‐carnitine/acetyl‐L‐carnitine supplements to prevent or treat symptoms of peripheral neuropathy in to prevent or treat symptoms of peripheral neuropathy in patients receiving chemotherapy for treatment of cancer.
Don’t use mixed medication mouthwash, commonly termed “magic mouthwash,” to prevent or manage cancer treatment‐induced oral mucositis.
Don’t administer supplemental oxygen to relieve dyspnea in patients with cancer who do not have hypoxia.
Don’t use aloe vera on skin to prevent or treat radiodermatitis.

11/3/2015
17
Leadership – EB Practice
Set the vision
Secure resources
Create environment
Establishing a Culture: Institutional Level CNO and Senior Leadership Support
Budget allocations
Technology, staff time, education
Leverage Existing Programs
Professional Development
Practice and Quality Improvement Committees
Advanced Practice Nurses
Partner with School of Nursing
Secure the ResourcesUnlimited access to online sources of evidence at all work areas
Search engines, elearning such as MosbySearch engines, elearning such as Mosby Nursing Skills, paper and electronic journals
Staffing and scheduling for release time to participate in education and practice development activities
11/3/2015
18
Create the EnvironmentShared Governance – research, practice, education counsels/committees
Faculty mentors as nurse scientistsFaculty mentors as nurse scientists
Tie into Compensation, Benefits and Incentives
Nursing sensitive quality outcomes
Establishing a Culture: Institutional Level Research behaviors in clinical advancement levels
EBP/Research Champions
Demonstrate use of electronic databases
Journal clubs, brown bags, case reviews, poster sessions, Nursing Grand Rounds
Research/EBP Committee
Research Fellowships
Establishing a Culture: Institutional Level EBP Toolkit
What is a clinical question
How to search – tip sheet
Resources – librarian, champions
How to do a synthesis – Table of Evidence
How to critique
How to lead a journal club
How to develop EB policies/procedures/ CPG
11/3/2015
19
Integrate EBP at the POC Resources to easily access knowledge
Position descriptions/performance appraisals –incorporate requirement of EBP use
i i Orientation
Evaluate Guidelines, Cochrane, JBI,
Web eval of consumer content using CARS (credible, accurate, reasonable, supported)
Annual competency for EBP
Work area – unit council discussions on practice evidence
Next Steps
P&FCC
Teamwork
EBPTeamwork
&
Collaboration
InformaticsQuality Improvement
Safety
Overcoming Barriers to Use of Evidence Knowledge
About research process Electronic databases Accessing research materials Understanding research articles
Skills Computer skills Search skills Skills to critique or synthesize the literature
Attitudes Value for research in practice If this is important I will find the time
11/3/2015
20
Lesson on Leadership and Followers
http://www.youtube.com/watch?v=hO8MwBZl‐&f l dVc&feature=related
CHANGE THE WORLD OF HEALTH CARE
Start where you areUse what you haveUse what you haveDo what you can
A. Ashe
??????
Questions, Comments and Questions, Comments and
???? ??
Q ,Q ,DiscussionDiscussion