basic hypertension. jnc-7 is the best guideline! national committee on prevention, detection,...
TRANSCRIPT

Basic Hypertension
JNC-7 is the best guideline!
• National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure. The JNC 7 Report. JAMA 2003; 289:2560-72.
• JNC-8 is in development; anticipated release in spring 2011, though delayed 2 years already.

Classifications• DX: Sustained bp elevation over time (3 in at
least 2 weeks)• Normotensive: <=120mm Hg systolic AND <=80
mm Hg diastolic• Prehypertension: 121-139 systolic OR 81-89
diastolic• Stage I HTN: 140-159 systolic or 90-99 diastolic• Stage 2 HTN: 160+ systolic or 100+ diastolic
– Choose the highest category applicable– Dr. Dodd’s first HTN commandment: Thou shall not
let stage 2 HTN leave clinic without doing something!

Why Treat Hypertension?
• Major cause of cardiovascular morbidity and mortality– Stroke, Congestive Heart Failure, MI
• Major cause of ESRD requiring dialysis
• Treat to GOAL (not “almost to goal”)– <=140 AND <=90 for all patients (possibly not
extreme elderly)– <130/80 for pts with DM or renal dz

Lifestyle Modifications
• 3-6 months of this for stage 1 HTN (1)
1. National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure. The JNC 7 Report. JAMA 2003; 289:2560-72.
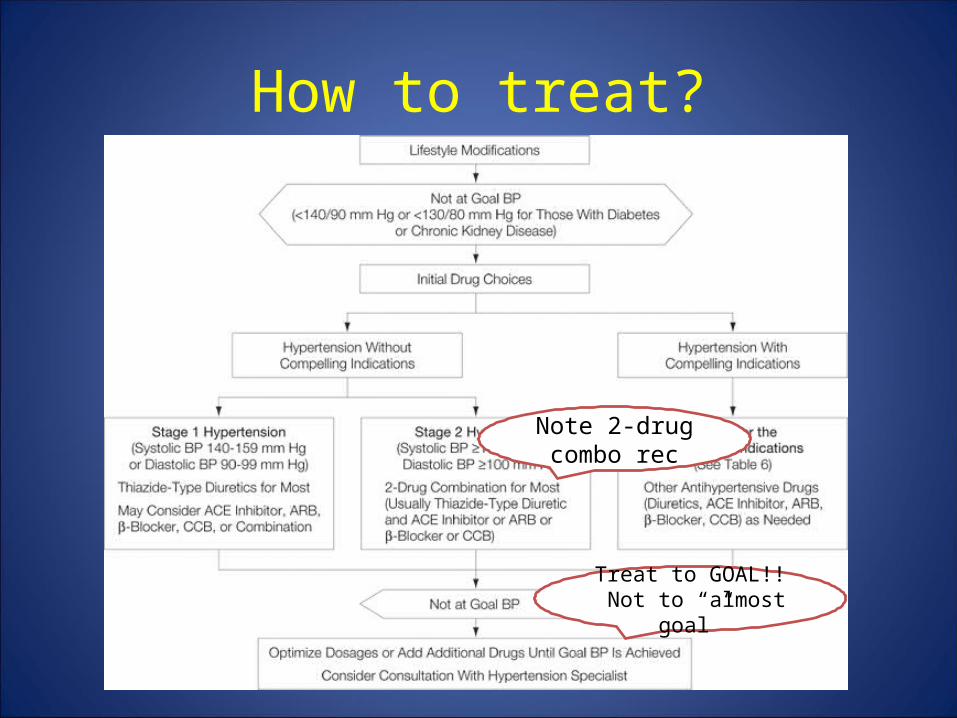
How to treat?
Note 2-drug combo rec
Treat to GOAL!! Not to “almost goal”

Compelling Indications
Indication Recommended Drugs Comments
Heart Failure Diuretic, BBlocker, ace-inhibitor, arb
Loop diuretics preferred; ARB only if ace not tolerated
Post MI BBlocker, ACE-I ACE-I for low EF post MI
Diabetes mellitus Diuretic, BBlockers, ACE-I, ARB, CAB
Diuretics reduce CV risk; ACE-I reduce ESRD risk
CKD ACE-I, ARB
Stroke Prevention Diuretic, ACE-I

Without Compelling Indications, Which Drug should I Use?
• Several trials inform this decision:– ALLHAT– ASCOT– ANBP-2– ACCOMPLISH
• Brief reviews of each:

ALLHAT 2002 (2)
• Randomized, double-blinded trial• 33,357 participants >=age 55 with HTN
and one other CHD risk factor; large AA contingent
• Randomized to chlorthalidone, amlodipine, lisinopril, doxazosin; followed for 4.9 years
• Achieved similar BP in all groups
• Alpha blocker inferior (more CHF)
2. The ALLHAT Collaborative Research Group. Major Outcomes in High-Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic. JAMA. 2002; 288:2981-2997.

ALLHAT• No difference in primary outcome comparing
thiazide to ACE and thiazide to CCB (combined fatal CHD or nonfatal MI).– All cause mortality no different
• Subgroup analysis:– Higher heart failure rate with CCB– Stroke 15% higher with ACE-I (principally AA enrollees)– Combined CV disease: 10% higher rate in ACE-I arm
(driven by stroke rate)• CHF 19% higher (all subsets)• Angina 11% higher (all subsets)• Revascularization 10% higher (all subsets)

ASCOT – BPLA 2005 (3)
• Multi-center, randomized controlled European trial in 19,257 hypertensive pts aged 40-79 with at least three other CV risk factors
• Randomized to amlodipine 5-10mg plus perindopril 4-8mg or atenolol 50-100mg plus bendroflumethiazide 1.25-2.5 mg
• Stopped early after 5.5 years – Lower stroke; fewer total CV events; lower all
cause mortality in cab/ace arm!3. Dahlof B, et al. Prevention of cardiovascular events with an antihypertensive regimen of amlodipine adding perindopril as required versus atenolol adding bendroflumethiazide as required, in the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA): a multicentre randomised controlled trial. Lancet 2005; 366: 895-906

ASCOT – BPLA
• Mean BP’s were 137.7/79.2 in the bb/thiazide group; and were 136.1/77.4 in the cab/ace group
• 2.7/1.9 mm Hg difference over 5.5 years is a lot of BP load
• Thiazide dose equivalent to 6.25-12.5mg of HCTZ– Dose really low!
ANBP-2 2003 (4)
• Prospective, randomized OPEN LABEL Australian study of 6083 subjects with HTN aged 65-84; f/u of 4.1 years
• Randomized to enalapril vs HCTZ, but rx determined individually by providers– 58-62% on assigned rx by end of study.
• Achieved BP were the same in each group• ACE-I group had lower CV event rate or death
from any cause. 4. Lindon MH, et al. A Comparison of Outcomes with Angiotensin-Converting–Enzyme Inhibitors and Diuretics for Hypertension in the Elderly. NEJM 2003; 348:583-92.

ACCOMPLISH 2008 (5)• Randomized double-blind trial of 11506 US
patients; 36 month f/u.• Benazepril plus amlodipine or benazepril plus
HCTZ• Slightly different BP achieved (131.6/73.3 vs
132.5/74.4).• Improved composite outcome in the ACE/CAB
group– CV death, nonfatal MI, nonfatal stroke, hospitalization
for angina, sudden cardiac arrest and coronary revascularization
Jamerson K, Weber MA, et al. Benazepril plus Amlodipine or Hydrochlorothiazide for Hypertension in High-Risk Patients . NEJM 2008; 359; 2417-28.

Bottom line
• Biggest goal in HTN treatment is to get the patient to his/her BP goal
• Choice of agent really doesn’t matter inside the “big 5” classes (thiazide, bb, cab, ace, arb)
What to talk about next?
• Let’s talk more more about these medication classes
• My inpatient’s BP is too high
Thiazide Diuretics
• HCTZ and Chlorthalidone available• Thiazides generally not useful if GFR <30
ml/min (Cr>2.5)• Side Effects:
– volume depletion– metabolic abnormalities (K+, Mg+, Na+, glucose,
lipids, alkalosis)– hyperuricemia and gout– Increased risk of diabetes mellitus

Which Thiazide?
• Half-life of Chlorthalidone longer than HCTZ (24 -55 vs 2.5 hours)
• More night-time dipping with chlorthalidone (6)– More night-time dipping associated with better CV
outcomes• ALLHAT, SHEP used chlorthalidone and found
improved or similar outcomes to other drug regimens
• ANBP2, ACCOMPLISH used hctz and found hctz inferior to other drug regimens
6. Ernst ME, Carter BL, Goerdt CJ, et al: Comparativeantihypertensive effects of hydrochlorothiazide and chlorthalidone on ambulatory and office blood pressure. Hypertension 47. (3): 352-358.2006
Beta Blockers
• Also First Line Agent per JNC-7; however expected to move lower on list with JNC-8
• Primary indication: post-MI or with angina• Lipid soluble, liver metabolized - propranolol,
metoprolol• Water soluble, renal excretion - nadolol,
atenolol

Beta Blockers - adverse effects
• RAD, COPD - increased bronchospasm• Worsen decompensated CHF• SSS, first degree heart block are
contraindications• Mask symptoms of hypoglycemia; prolonged
recovery from hypoglycemia• Rebound hypertension

ACE-Inhibitors
• Block AT-I to AT-II conversion– AT-II: potent vasoconstrictor, releases
aldosterone, stimulates smooth muscle hypertrophy
• Many, many drugs available in this class!! Structurally heterogenous; functionally the same.
• Not as effective in AA, Asian Pacific Islanders• Ramipril is the most potent of these

ACE-Inhibitors
• Compelling indications in DM, low EF - “more is better”
• High renin states - more responsive. Low renin, salt sensitive AA’s may be less responsive.
• Neutral to lipids, glucose• Fosinopril, lisinopril, trandolapril do not
require bid admin at higher doses.• Max dose lisinopril is 40! (not 80)
ACE-Inhibitors - Side Effects
• Bilat renal artery stenosis - renal insufficiency, hyperkalemia
• Low flow states (chf, dehydration) - renal insufficiency and orthostasis
• Dry cough - up to 20%• Angioedema - <1%• Birth defects - don’t use in pregnant women
or women of childbearing age not on birth control

Angiotensin II Receptor Blockers
• Well tolerated, but generally not as potent as other classes– Same compelling indications as ACE, but second line
• Add diuretic if low dose doesn’t work• Virtually free of SE’s - rare angioedema,
teratogenic, ARF as with ACE-I• Multiple drugs available; valsartan, telmisartan,
candesartan, irbesartan, losartan…

Dihydropyridine Calcium Antagonists
• Amlodipine, felodipine, many, many more• Good antianginal effects• Second choice for systolic htn in elderly
– More effective than ACE-I in AA, Asian Pacific Islanders
• Some safety questions in diabetics; perhaps increased mortality with short acting agents
• SE’s: HA, tachycardia, edema• ACE-I addition may reduce edema
Non-dihydropyridine Calcium Antagonists
• Verapamil and diltiazem• Useful for SVT’s, Variant Angina• SE’s: constipation, heart block, negative
inotropy, flushing.• Generally reserved for second or third line
treatment.
• back
Mr. Smithers
• You are the night float called to see a 62 yo man admitted to yellow team for treatment of MSSA epidural abcess with nafcillin 2g q4h. Currently on lisinopril 40, and bp was controlled as an outpatient. Nurse tells you that BP is 178/94.
– What do you want to know?

Several Questions• Is the patient stable?
– HTN Urgency– HTN Emergency
• Is the BP elevated and if so, why is his BP elevated?– Take the BP yourself. – Consider wide differential: pain, anxiety, measurement error,
medication effects, kidney disease• Should I treat it?
– Is there a dx present that will worsen with uncontrolled BP?• If so, how should I treat it?
– Oral vs IV– Which oral and which IV?

Mr. Flanders
• You are rounding outside the room of Ned Flanders, a 75 yo man transferred out of the unit yesterday after a LGI bleed secondary to diverticulitis. He also has a hx of HTN, HLP, and renal cell CA in the distant past. The med student presents a BP of 162/88, and tells you that his BP had been 150-178/78-88 overnight. He’s taking lisinopril 40, amlodipine 10 and hctz 12.5. The ICU team had increased the amlodipine 24 hours before, and the patient had received the second dose.
• What do you want to know?

Several Questions
• Why is his BP elevated?– Consider wide differential: pain, anxiety, measurement
error, medication effects, kidney disease• Should I treat it?
– Remember my first commandment• If so, how should I treat it?
– Don’t overtreat!• What’s the half-life of the drug?• What’s the time to achieve max effect of the drug?• Was the chosen drug correct?• back

Questions?