bcfs hhs emergency management division
TRANSCRIPT
BCFS HHS Emergency Management Division

• Founded in 1944, BCFS is a system of non‐profit health and human service corporations
• Programs and services are offered domestically and internationally, serving more than 4,700,000 persons annually
• BCFS administers over 60 separate programs
• Funding is derived from fees for service, contracts, grants, philanthropic and endowment revenue
BCFS; System of Nonprofit Corporations

Rooted in Texas. Branches Worldwide.
Arizona • California • Colorado • Florida • Illinois • New YorkOhio • Oregon • Tennessee • Texas • Washington, D.C. Africa • Eastern Europe • Latin America • Southeast Asia

Partner and Contractor

BCFS Health and Human Services• One of five corporate entities within the BCFS system of non‐profit companies providing a full array of services and programs including:– Emergency management planning and response– Medical and mental health services– Services for adults with mild to moderate disabilities– Residential services – Community development – Social services– International humanitarian aid and medical teams– Management and support services to other non‐profit organizations.

BCFS HHS Emergency Management Division• A non‐profit partner of federal, state and local government and
private industry specializing in – Emergency management– Incident management– Disaster response– Consultation and training– Policy and plan development– Turnkey logistics– Public health & medical emergency response– Mass care– Mass fatality planning– Medical sheltering and alternate care site planning and
operations– Base camp operations– Planning for vulnerable populations
• Alternate Care Facility Planning• The Shelter Continuum; from Gen Pop to Medical • Mass Fatality Management• ICS and HICS• Whole Community Planning• Planning for People With Disabilities and Others with
Access and Functional Needs• Disaster Medical Care Courses• Medical Surge and Disaster Triage• Crisis Standards of Care• Standards and Regulatory Compliance for Environment
of Care/Emergency Management• Medical and Ambulance Strike Team Training• Developing ESF 8 and ESF 6 Emergency Management
Programs and Emergency Operations Plans
Consultation, Training & Exercise Program
Large Incident Reponses• Branch Davidian Incident• Southeast Asia Tsunami• Hurricane Emily• Hurricane Katrina• Hurricane Rita• Eagle Pass Tornado• Hurricane Dean• FLDS Event• Hurricane Dolly• Hurricane Gustav• Hurricane Ike• H1N1 Flu• Haiti Earthquake• Hurricane Alex• Texas Wildfires 2011• USHHS ORR Influx 2012
A Force Multiplier

Expansion of Incident Management Capability • 200 Members
– ICS, All Hazards, Position Specific Training
– Most have specialized licensing or credentials
– Multi‐disciplinary senior level experience to include: Emergency Management, Public Health, EMS, Fire, Law Enforcement, Logistics, Personnel, Finance, Public Relations, Social Services, Mental Health, Medical, Legal, DMAT, DMORT, Information Technology and Communications
– Unique expertise and experience in complex international, large scale and major responses

Increased Visibility & Documentation
• Consistent and thorough utilization of web based emergency management tool; WebEOC
• Operational Period Incident Action Plans
• Daily Situation Reports
INCIDENT OBJECTIVES 1. Incident Name 2.Date Prepared 3.Time Prepared
ORR Surge 2012 15Apr2012 1600 4. Operational Period 16Apr-17Apr2012, 0700-0700
Management Objectives 1. Ensure the dignity, safety, and well being of all residents and staff in calm and comforming atmosphere. 2. Ensure effective coordination, command and control for ORR Surge 2012. 3. Provide for comprehensive force protection for all personnel assigned to include access to medical
services,
Operational Objectives 1. Complete knowledge of and adherence to all Protocols, Evacuation and Safety Plans. 2. Implement complex IMT organization 0700. 3. Implement use of consolidated WebEOC. 4. Support the Operations new site ECHO and continue to prepare for operations at FOXTROT. 5. Provide orientation and training to all new oncoming staff. 6. Conduct “Avoiding Allegations” training at all locations immediately following briefing for all staff. 7. Develop long term transportation plan by 1500 hours. 8. Solidify Parking Plan for Fiesta. 9. Evaluate plan for meeting temporary CFO building requirements. 10. Train on and implement medical protocol at all locations to provide consistency at all sites.
San Antonio: high of 84°, low of 61°, wind from ENE at 12 mph, chance of precipitation is 10%. Harlingen: high of 87°, low of 71°, wind from ESE at 16 mph, chance of precipitation is 40%.
7. General Safety Message 1. Maintain situational awareness regarding weather fluctuations. Ensure proper hydration and rest to remain. 2. Report any symptoms of colds or flu immediately to medical staff; to determine fitness for duty. 3. Use best practices with frequent hand sanitization and personal sanitary measures. 4. Watch for “out of place” scenarios, including people. Remediate and/or report.
8. ATTACHMENTS (X) IF ATTACHED) [ x ] Org. Assignment List ICS 203 [ x ] Alpha Med. Plan ICS 206 [ x ] Entry Security Procedure [ x ] Alpha Div. Assignment s ICS 204s [ x ] CHARLIE Med. Plan ICS
206 [ x ]
Incident Safety Plans
[ x ] CHARLIE Div. Assignment Lists ICS 204s [ x ] Safety Plans – ICS 208 [ ] [ x ] Communications Plan – ICS 205 [ X ] Evacuation/Relo. Plans [ ]
9. Prepared By (Planning Section Chief) 10. Approved By (Incident Commander)
S. Hardy RESL K. Dinnin, IC

Supplementing Medical Staff
• Maintain continuity of operations– Decrease impact on day to day operations
• Trained BCFS disaster medical staff team• Rapid Deployment
• Physicians• Nurse Practitioners• Physician Assistants• RNs• LVNs• Paramedics• EMTs

Increased Communications & Logistics
• MCP‐Communications– Satellite (fixed and mobile)– Cellular (all carriers)– VoIP Telephones– Radios: VHF, UHF, 700, 800 and SAT– GIS– VTC
• Caches– Verizon, Nextel, AT&T, VHF, Laptops
• Fleet– MCP‐1 (Large Command Platform)– MCP‐2 (Small Command
Platform/IT/Commo for hard structure)– SSUs (Shelter Support Units for 1,000
people at alternate care sites)– Mobile shower and laundry units

• Multiple M‐SAT Kits (portable satellite radio/VHF) w/ additional handheld SAT phones
• 900+ VHF handheld radios• Portable VHF repeaters• 60+ Verizon cell phones with Push‐
To‐Talk (PTT) capability• 100 AT&T cell phones with Push‐To‐
Talk (PTT) capability• 80+ DELL laptops• 50 portable Wi‐Fi hot spots• 4 DHS‐PIV‐I certified credentialing
kits
Field Deployable Assets

• Warehouse‒ Medical resources
owned and staged for deployment
• National Redundant Contracts‒ Redundant regional
and national vendors‒ Medical Staffing‒ Equipment
(generators, tent structures, trucks, shower and toilet units, HVAC, food service)
• Procurement capabilities‒ Spending authority
and capacity with tasking
Expanded National Logistics & Procurement

Operational Experience

BCFS Operations; Hurricane Katrina
• 1700 persons sheltered in 12 shelters
• 260 BCFS staff• 1,500 volunteers • 2,500 medical man
hours utilized during the peak 48 hour period
• Duration 7 weeks
BCFS Operations: Hurricanes Gustav & Ike
• 32 Shelters / 3 Cities• 2,784 Shelter Guests• 542 Medical Staff• 245 IMT/Shelter Management
Staff• 370 Volunteers• 5,839 Prescriptions • 40% O2 Dependent• 430 Hospital Beds• 59 Bariatric Beds• Youngest Guest‐newborn• Oldest Guest – 98• Duration 4 Months

H1N1 Response ‐2009
• Texas ‐ Ground Zero for initial outbreak
• Issues of cross border disease spread
• BCFS IMT supported Public Health response for Health Services Region 8

USHHS ORR Influx 2012
• Operations– 116 Days of 24‐hour operations– 184 Incident Management Staff– 2,400+ total UACs received care – 19,200+ immunizations administered– Over one‐half million meals and
snacks served – 20,100+ articles of clothing
distributed – 15,300 bags of laundry cleaned – Over 10,000 international calls to
family facilitated– At the peak of activity in late April,
over 1,000 UACs were in the care of BCFS HHS at the same time at 8 different locations, including a United States Air Force base, which housed over 350 UACs
USHHS ORR Influx 2012
• Turnkey services– Food service– Portable power generation– Portable shower equipment– Portable restroom equipment– Mobile laundry units– On‐site educational services– On‐site recreational services– 24‐hour law enforcement support– IT and communication support– Enhanced waste removal services– Clothing supplies– Case management staff– Direct care staff to maintain a
minimum 1:8 (caregiver‐to‐UAC) ratio – Nationwide transportation services
utilizing air and ground resources
International Responses
Sri Lanka Tsunami• Established foster program for orphaned children
• Provided medical services
Haiti Earthquake• IMT support of local hospital
• Medical providers• Vaccination of local orphanages

Katrina and Rita Identified Significant Gaps; Irene and Sandy Confirmed We Still Have a Long Way To Go
Lack of…– Sheltering preparedness
• Medical personnel• Durable Medical Equipment and Consumable Medical Supplies
• Coordination of resources• Communication• Sustaining services
– Some shelters unable to support individuals with medical needs and/or disabilities; resulting in individuals being turned away

Disaster Lessons Learned
• Inadequate evacuation planning to evacuate individuals with medical needs– People had to evacuate in inclement conditions– People with disabilities remained in their homes for fear of not being accommodated
– People were evacuated without their equipment– People had to be transported in assets that did not meet their medical needs
– People missed the window of opportunity to evacuate because of road closures; forcing them to stay in their homes
– Major impact on transportation systems and on EMS and First Responders

Disaster Lessons learned
• Major power outages create a strain on persons with medical conditions living at home– Lack of refrigeration– Lack of ability to power life sustaining DME resulting in loss of life
– Lack of ability to heat or cool; affecting persons with the inability to self regulate body temperature
– Major impact on health care system
Disaster Lessons Learned
• Lack of medical shelter capacity– People had to remain in transportation resources while a bed is located
– People were inappropriately placed in facilities; who were previously living independently at home with support services
– People evacuated to Emergency Departments at health care facilities impacting the ability for the health care infrastructure to support those with acute medical needs

Disaster Lessons Learned
• Lack of planning = Lack of appropriate resources– People placed in facilities that were not equipped to meet their medical needs
– Lack of DME and CMS– Lack of medical staff– Lack of ADA accommodations

National Initiatives and Concerns
• Functional Needs Support Services• Whole Community Planning• Alternate Care Site and Medical Sheltering

BCFS Response to National Initiatives
• BCFS contracted to develop Federal guidance on sheltering people with disabilities and others with access and functional needs
• BCFS contracted to develop and deliver FEMA’s Whole Community Training Curriculum
• BCFS develops and maintains 5000 fixed bed capacity and 750 mobile bed capacity
• BCFS develops copyrighted medical sheltering manual and training

Public Health Preparedness Capabilities
• Medical Surge• Community Recovery• Emergency Operations• Mass Care• Fatality Management• Crisis Standards• Responder Safety

Medical Surge – Its Not Just About Hospitals
• “Hospital surge capacity” - the ability of a hospital in a mass casualty incident to augment bed availability by maximizing resources and utilizing alternate forms of delivering care.
• “Community surge capacity” refers to local or regional-level activities undertaken to bolster the response of a community’s healthcare facilities to mass casualties.
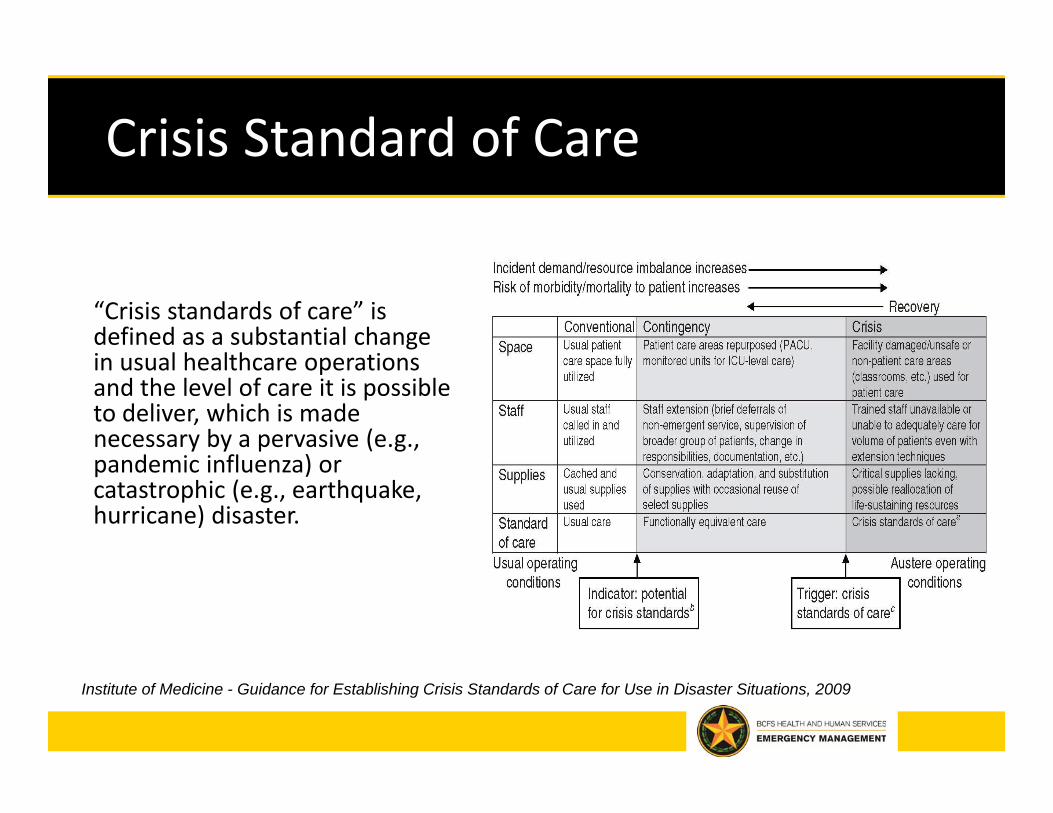
Crisis Standard of Care
“Crisis standards of care” is defined as a substantial change in usual healthcare operations and the level of care it is possible to deliver, which is made necessary by a pervasive (e.g., pandemic influenza) or catastrophic (e.g., earthquake, hurricane) disaster.
Institute of Medicine - Guidance for Establishing Crisis Standards of Care for Use in Disaster Situations, 2009

Mass Fatality Management
• Medical-legal authority• Storage of bodies issues related to pandemics• Forensics and Identification issues• Public Health will be involved• Emotional toll on bereaved• Emotional toll on staff• Media attention
Disaster Medical Training
• Health care providers unprepared for disaster response
• Health care administration not sufficiently trained in ICS
• Crisis stress management for health providers is critical
• Staff tracking and oversight• Lack of resource management• Lack of understanding of crisis standards of care
• Collateral duties

Summary • Multidisciplinary Senior‐Level Experience:
• Readily Available Rolling Resources Fully Dedicated to the State of Texas• Spending Authority – Contractual and Philanthropic• Core Competencies
• National Alternate Care Site Planning• National Mass Fatalities Planning• National Vulnerable Populations Planning
– FNSS– Whole Community– Medical
Emergency Management Logistics Mental Health Public Health Personnel Management Medical EMS Finance Legal Fire Public Relations DMORT Law Enforcement Social Services IT/Comm

Contact
Kari TatroExecutive Vice President
Emergency Management OperationsBCFS Health and Human Services
210‐832‐[email protected]