beckman coulter, inc. - medicine.uci.edu fungal... · bronchiectasis or pulmonary fibrosis that...
TRANSCRIPT

Fungal Infections
Peter Heseltine MB, MA, BCh, FACP, FIDSA, FAACC
Professor of Clinical Medicine UCI
ZOT
2
Conflict of Interest
None for this lecture
Goals & Objectives
Recognize risk factors and presentations of
serious fungal disease:
Candida, Aspergillus, Cryptococcus, Mucor
Histoplasmosis, Blastomycosis, Coccidioidomycosis
Apply fungal diagnostics in clinical practice
Galactomannan, beta-D-glucan
Understand treatment choices for fungemia,
pulmonary & CSF infections
echinocandins vs azoles vs polyenes
3
Current State of Mycology
Overall Mortality
Invasive Aspergillosis: 20-60%
Candidemia: 30-60%
Other Molds: ~80%
Delay in recipt of therapy is asociated with
mortality
Aspergillus (Cordonnier CID 2009)
Candida (Garey CID 2006; Morrell AACC 2005)
Mucormycosis (Chamilos CID 2008)
4
Cordonnnier C Clin Infect Dis 2009 48:1042-51. Garey KW Clin Infect Dis 2006 43:25-31
Morrell Antmicrob Agents Chemother 2005 49:3640-3645
Chamilos G Clin Infect Dis 2008 47:503-9

Populations At Risk / Risk Factors
Non-immunocompromised
Broad spectrum antibiotics
Hemodialysis
Central venous catheter
IV drug use
Total parenteral nutrition
GI perforation or surgery
Colonization
Diabetes
LOS in ICU
Pancreatitis
Sepsis
5
Immunocompromised
Neutropenia
Stem Cell Transplant
Mucositis
GVHD
Chemotherapy
Organ transplant
AIDS
Neonates
Gestational age
H2 blockers
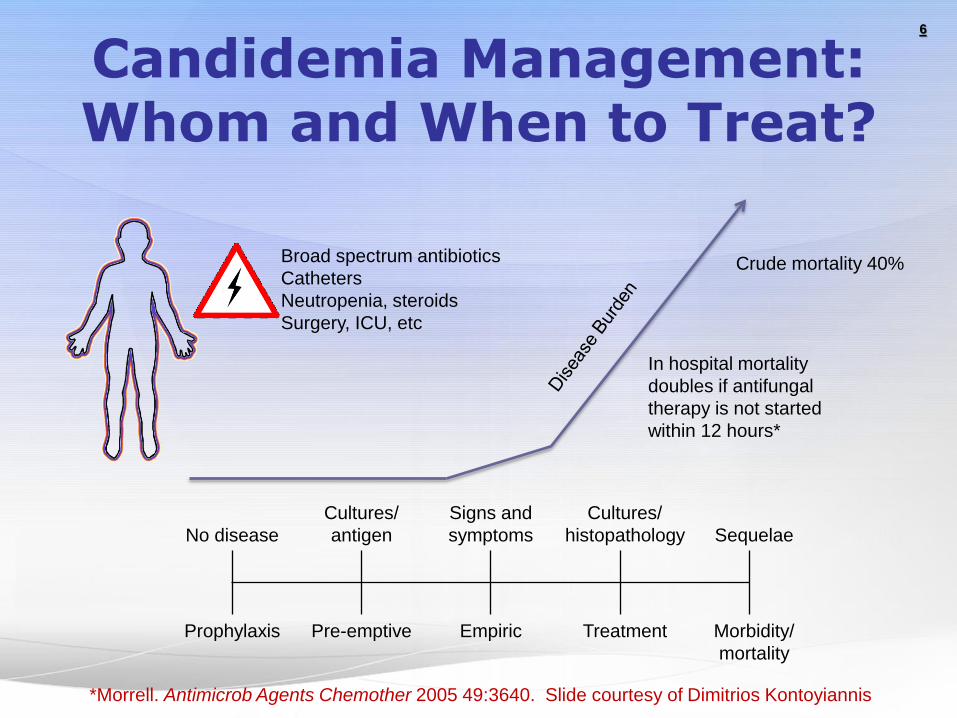
Candidemia Management: Whom and When to Treat?
6
No disease
Cultures/
antigen
Signs and
symptoms
Cultures/
histopathology Sequelae
Prophylaxis Pre-emptive Empiric Treatment Morbidity/
mortality
Broad spectrum antibiotics
Catheters
Neutropenia, steroids
Surgery, ICU, etc
Crude mortality 40%
In hospital mortality
doubles if antifungal
therapy is not started
within 12 hours*
*Morrell. Antimicrob Agents Chemother 2005 49:3640. Slide courtesy of Dimitrios Kontoyiannis
High-risk
neutropenic
patient (chemo,
HSCT)

Candida Infection/Septic Shock Importance of Empiric Therapy and Source Control
7
P < .001 for the comparison of patients receiving both antifungal therapy and
adequate source control within 24 hours of the onset of shock to the other 3 groups.
Kolleff MH CID 2012;54:1739
Rex summary of updated IDSA Candidiasis guidelines.ppt 8
Catheter Exchange? Yes!
Lots of consistent data
Without catheter removal, 82% had persistent
infection
Lecciones, Clin Infect Dis 1992;14:875-883
Shortened duration of fungemia from 5.6 to 2.6 days
P < 0.001 (Rex, Clin Infect Dis 1995;21:994-996)
Reduced mortality: 41% to 21%
P < 0.001 (Nguyen, Arch Intern Med 1995;155:2429-2435)
Especially true for C. parapsilosis
Very strong link with catheters
Kojic, Clin Microbiol Rev 2004;17:255-267
Rex summary of updated IDSA Candidiasis guidelines.ppt 9
Catheter Exchange? Other Sources
~ 15% of candidemia patients have another
obvious source (urine, abscess)
• The gut may
be a cryptic
source
• What does
this imply?
10
Catheter Exchange? Definite Maybe
In non-cancer patients, suspect the catheter
Unless another source is apparent
After cytotoxic chemotherapy, think twice
Gut may be source, effect of removal is less?
C. parapsilosis is the clear exception
More data & better tools needed here
Differential quantitative and time-to-growth central/peripheral BC
Bouza, Clin Infect Dis 2007;44:820-6.
We keep wishing for good serodiagnostic tools
We have several (beta-glucan, PCR) but none have produced
high levels of confidence
Kedzierska, Eur J Clin Microbiol Infect Dis 2007;26:755-766
Nett, J Infec Dis 2007;195:1705-1712.
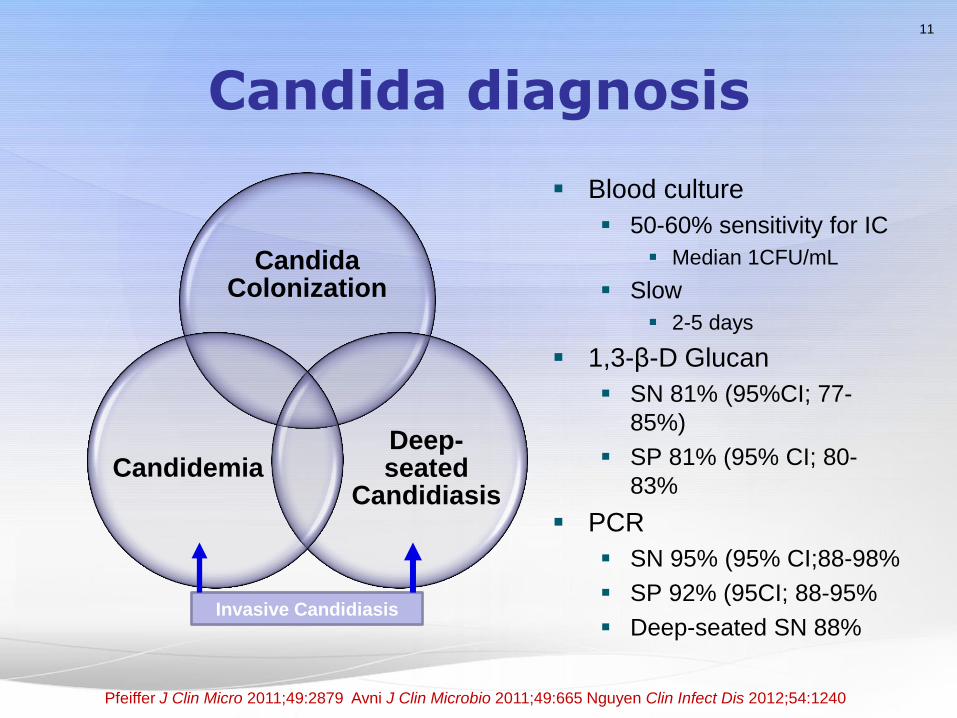
Candida diagnosis
Blood culture
50-60% sensitivity for IC
Median 1CFU/mL
Slow
2-5 days
1,3-β-D Glucan
SN 81% (95%CI; 77-
85%)
SP 81% (95% CI; 80-
83%
PCR
SN 95% (95% CI;88-98%
SP 92% (95CI; 88-95%
Deep-seated SN 88%
11
Candida Colonization
Deep-seated
Candidiasis Candidemia
Invasive Candidiasis
Pfeiffer J Clin Micro 2011;49:2879 Avni J Clin Microbio 2011;49:665 Nguyen Clin Infect Dis 2012;54:1240
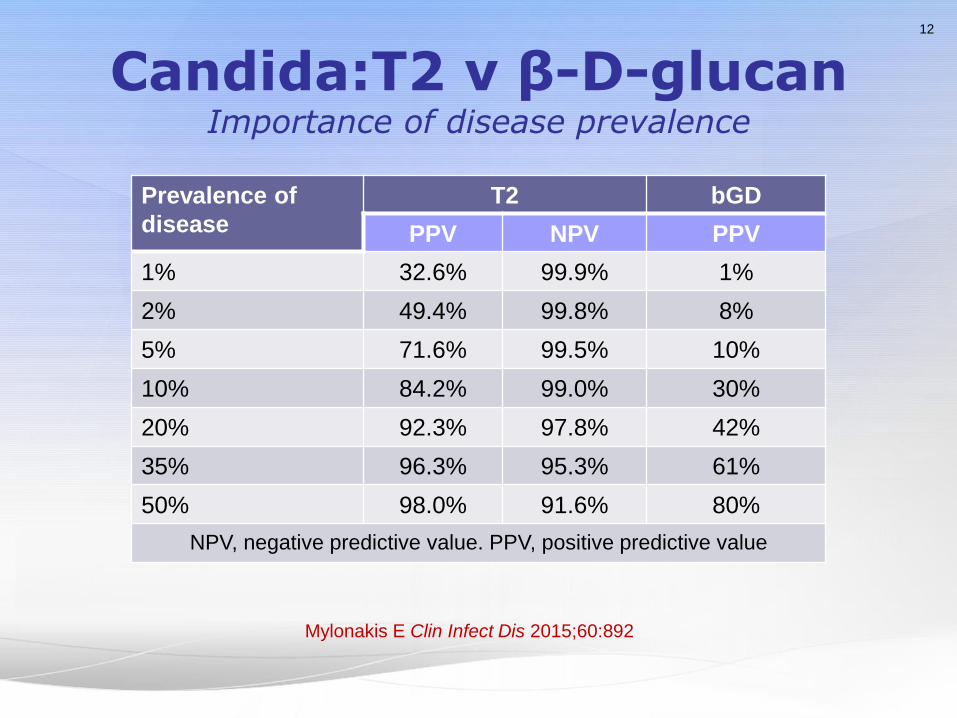
Candida:T2 v β-D-glucan Importance of disease prevalence
Prevalence of
disease
T2 bGD
PPV NPV PPV
1% 32.6% 99.9% 1%
2% 49.4% 99.8% 8%
5% 71.6% 99.5% 10%
10% 84.2% 99.0% 30%
20% 92.3% 97.8% 42%
35% 96.3% 95.3% 61%
50% 98.0% 91.6% 80%
NPV, negative predictive value. PPV, positive predictive value
12
Mylonakis E Clin Infect Dis 2015;60:892

T2 Candida Assay Whole blood sample
(hands on 5 mins)
Results in 3-5 hours
Five species detected
2046 subjects
SN 91.1% & SP 99.4%
12% invalids*
LOD 1 cfu/mL
13
Wilson NM Poster Presentation IDWeek 2016.
Mylonakis E Clin Infect Dis 2015;60:892
14
Other settings
Thinking of non-neutropenia as the start point
The less you know or
The more the patient scares you
The more the guidelines point to
An echinocandin
A (lipid-associated) amphotericin B
But, for resource constrained settings…
The guidelines do note that classic AmB works
15
Empirical Therapy
In the febrile non-neutropenic patient?
Early treatment is theoretically attractive
IDSA Guidelines
“The specific basis for selecting non-neutropenic patients who
should receive empiric antifungal therapy is unclear, but should be
based on at least one of the following: clinical assessment of risk
factors, serologic markers for invasive candidiasis, and/or culture
data from non-sterile sites (BIII).”
My rules
Antibiotics, lines, no other source, and…
Colonized somewhere with Candida
I don’t distinguish sites: anywhere works for me
Prophylaxis? Even hazier
16
Candiduria
Asymptomatic candiduria
No treatment unless high-risk dissemination (AIII).
Focus on elimination of predisposing factors. (BIII).
High risk for dissemination
Urologic manipulations (BIII)
Use short course fluconazole or even amphotericin B
Neutropenic patients and low birth weight infants
Treat as for invasive candidiasis.
Consider imaging kidneys/collecting system (BIII)

17
Key organism principles
Helpful to know tiers of progressive difference
(most virulent, most susceptible): albicans, parapsilosis, tropicalis,
dubliniensis
(intermediate): glabrata - do susceptibility tests!
(least virulent, least susceptible): krusei
You often know quickly if C. albicans
It’s the one that is “germ tube-positive”
Just knowing species is very helpful
P = Plastic = parapsilosis. Look for the device!
Resistance patterns
C. glabrata & C. krusei: Azoles are dicey. Newer azoles are better
C. parapsilosis: Echinocandins sometimes a little weaker than fluconazole
C. lusitaniae: Amphotericin resistance is frequent
C. guilliermondii: higher azole and candin MICs
C. auris: special infection control precautions

18
Key drug principles Voriconazole
Fatty meal reduces absorption
IV form uses cyclodextrin: not well cleared by dialysis
Lots of drug-drug interaction
Echinocandins
Very few convincing differences
Usually cross-resistant – but not always! (emerging data)
Amphotericins
Liposomal amphotericin B = AmBisome
Amphotericin B lipid complex = ABLC = Abelcet
Amphotericin B colloidal dispersion = ABCD = Amphotec
(Classic ampho = Amphotercin B deoxycholate = Fungizone)
19
IDSA Candida guidelines Update 2016
Echinocandins (anidulafungin, caspofungin, micafungin)
preferred choices for proven/suspected invasive disease
There is little distinction made among the echinocandins
Lipid-formulation amphotericin B is alternative
Azole resistant C. glabrata, C. auris
Concept of step-down therapy is strongly encouraged
Fluconazole or Voriconazole (C. krusei) advised as step down
therapy for selected isolates
Fluconazole (oral) for immunocompetent patients
Fluconazole prophylaxis limited to high risk sites
All patients who have candidemia, should undergo an
ophthalmologic examination by an ophthalmologist to
look for evidence of endophthalmitis
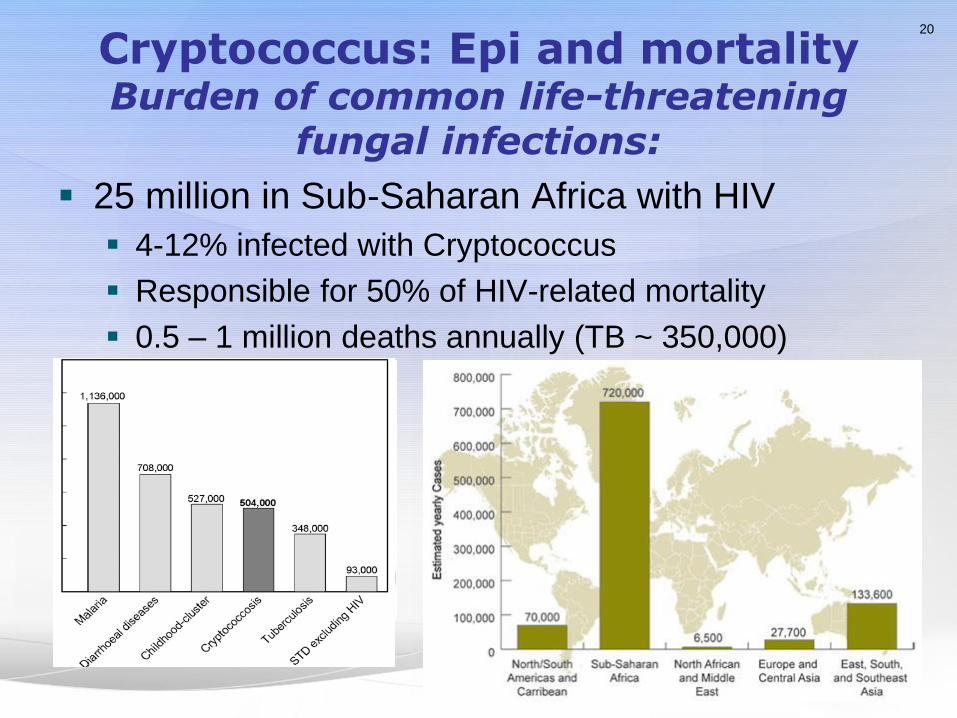
Cryptococcus: Epi and mortality Burden of common life-threatening
fungal infections:
25 million in Sub-Saharan Africa with HIV
4-12% infected with Cryptococcus
Responsible for 50% of HIV-related mortality
0.5 – 1 million deaths annually (TB ~ 350,000)
20

Cryptococcus: Current Diagnostics
CSF India Ink preparation
~80% sensitive
Dependent on fungal burden
Cultures – standard media
CGB media
+ C. gattii v. -C. neoformans
Cryptococcal antigen testing
(CrAg) >90% sensitive
Clear differences between developing world and
elsewhere in type of test & utility
21
Klein K J Clin Micro 2009;47:3669

CrAg (GXM) testing: new method - LFA
Stored at room temperature
No specimen pretreatment
required - 40MuL required
Results in 10 minutes
Qualitative and semi-
quantitative
Serum or CSF
Improved sensitivity for
serotype C
22
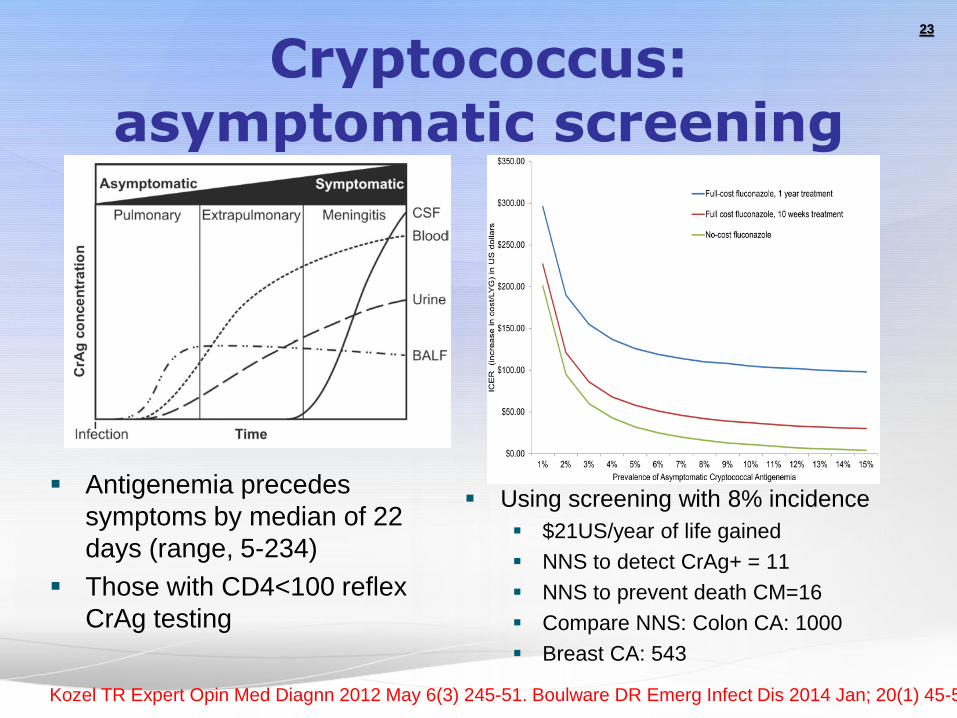
Cryptococcus: asymptomatic screening
Antigenemia precedes
symptoms by median of 22
days (range, 5-234)
Those with CD4<100 reflex
CrAg testing
Using screening with 8% incidence
$21US/year of life gained
NNS to detect CrAg+ = 11
NNS to prevent death CM=16
Compare NNS: Colon CA: 1000
Breast CA: 543
23
Kozel TR Expert Opin Med Diagnn 2012 May 6(3) 245-51. Boulware DR Emerg Infect Dis 2014 Jan; 20(1) 45-53

Cryptococcal screening algorithm
24

Cryptococcal screening algorithm
Smith RM, Nguyen TA, Ha HTT, Thang PH, Thuy C, et al. (2013) Prevalence of Cryptococcal Antigenemia and Cost-Effectiveness
of a Cryptococcal Antigen Screening Program – Vietnam. PLOS ONE 8(4): e62213. doi:10.1371/journal.pone.0062213
http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0062213
25
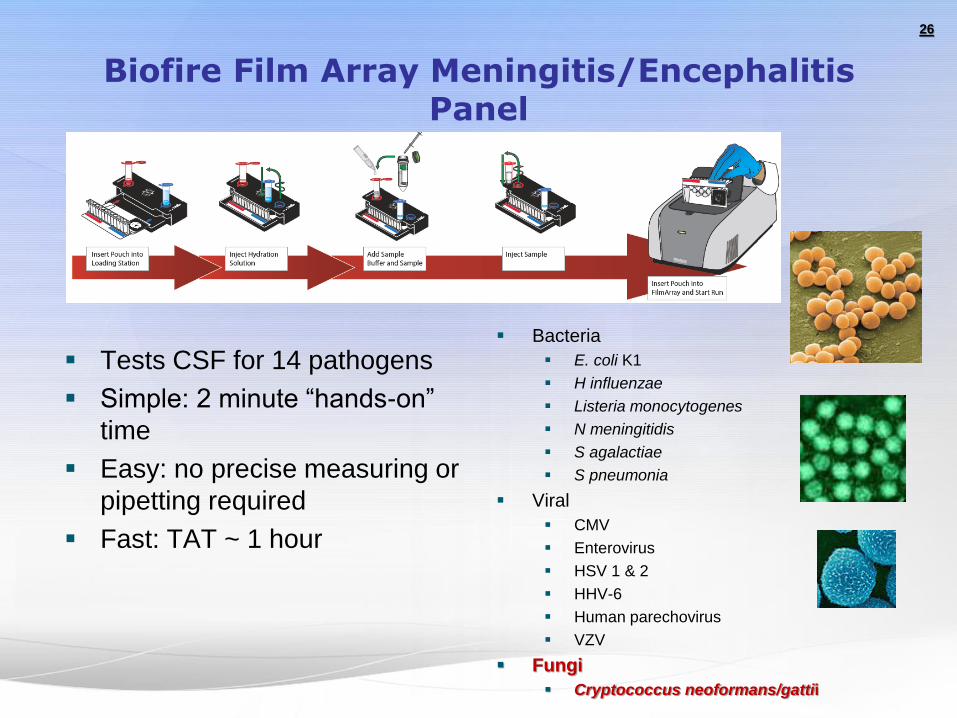
Biofire Film Array Meningitis/Encephalitis Panel
Tests CSF for 14 pathogens
Simple: 2 minute “hands-on”
time
Easy: no precise measuring or
pipetting required
Fast: TAT ~ 1 hour
Bacteria
E. coli K1
H influenzae
Listeria monocytogenes
N meningitidis
S agalactiae
S pneumonia
Viral
CMV
Enterovirus
HSV 1 & 2
HHV-6
Human parechovirus
VZV
Fungi
Cryptococcus neoformans/gattii
26
Hypersensitivity reaction to Aspergillus fumigatus mold that has
colonized bronchi of patients with asthma or cystic fibrosis (genetic
defects).
Exposure of atopic people to fungal spore elements results in the
formation of IgE (50%) and IgG antibodies. Galactomannan is
usually negative, and 1,3-betaD-glucan is often positive
Presents as asthma complicated by bronchial obstruction, fever,
malaise, expectoration of brownish mucus plugs, peripheral blood
eosinophilia, and hemoptysis.
Treatment involves environmental control measures, corticosteroids,
and itraconazole, voriconazole or posaconazole
Early detection and treatment can prevent the development of
bronchiectasis or pulmonary fibrosis that otherwise occurs in the
later stages of the disease.
27
Allergic bronchopulmonary aspergillosis

Allergic bronchopulmonary aspergillosis
28

Aspergillus
Galactomannan Serum
Proven disease: Sens 68-74%; Spec 90-99%
With proven & probable Sens 59-63%; Spec 92-94%
Performs best in hematologic malignancy >> transplant, ICU
BAL – Sens 50-70%; Spec 73%
1,3-β-D-glucan Sens 55-95%; Spec 77-96%
Non-specific – negative in Cryptococcus and Mucormycosis
False positives in heavily filtered products (albumin, IVIG, etc)
gauze, etc
Direct Comparison Higher specificity of GM (97 v 82%) but lower sensitivity (81 v 49%)
29
Erwig LP Nature Rev Micro 2016 14:163. Pfeiffer CD Clin Infect Dis 2006; 42: 1417
Koo Clin Infect Dis 200; 49:1650 Sulahian A J Clin Micro 2014;52:2328
Pip/tazo false
positives greatly
reduced
Galactomannan and 1,3-β-d-Glucan Testing for the Diagnosis of Invasive Aspergillosis
High-risk patients with heme malignancies and
chemotherapy-induced neutropenia or allogeneic HSCT:
both tests have a similar performance with a limited sensitivity
(60%–80%) and a specificity ≥90%.
Two consecutive positive tests results gives high
specificity (95%–99%), with a slight loss of sensitivity.
Insufficient data:
Solid-organ transplant recipients and others at low or moderate
risk of IA. Sensitivity <40% due to limited angio-invasion?
βdG test specificity poor in lung transplant patients.
? GM in pediatric patients ~ adults
Aspergillus-Lateral-Flow Device – POC, BAL
30
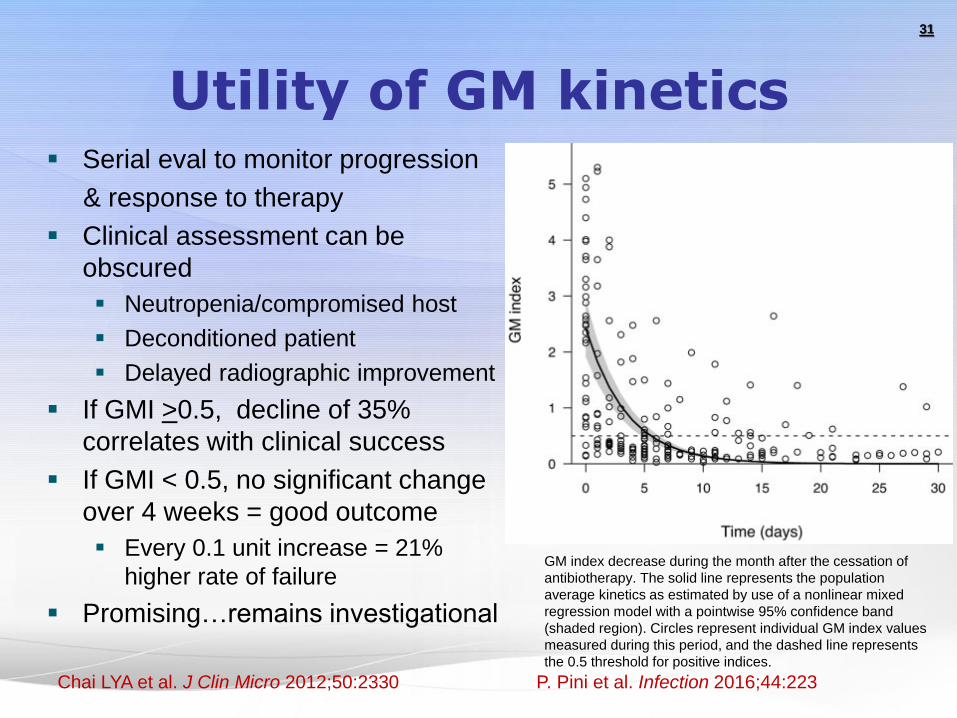
Utility of GM kinetics Serial eval to monitor progression
& response to therapy
Clinical assessment can be
obscured
Neutropenia/compromised host
Deconditioned patient
Delayed radiographic improvement
If GMI >0.5, decline of 35%
correlates with clinical success
If GMI < 0.5, no significant change
over 4 weeks = good outcome
Every 0.1 unit increase = 21%
higher rate of failure
Promising…remains investigational
31
Chai LYA et al. J Clin Micro 2012;50:2330 P. Pini et al. Infection 2016;44:223
GM index decrease during the month after the cessation of
antibiotherapy. The solid line represents the population
average kinetics as estimated by use of a nonlinear mixed
regression model with a pointwise 95% confidence band
(shaded region). Circles represent individual GM index values
measured during this period, and the dashed line represents
the 0.5 threshold for positive indices.
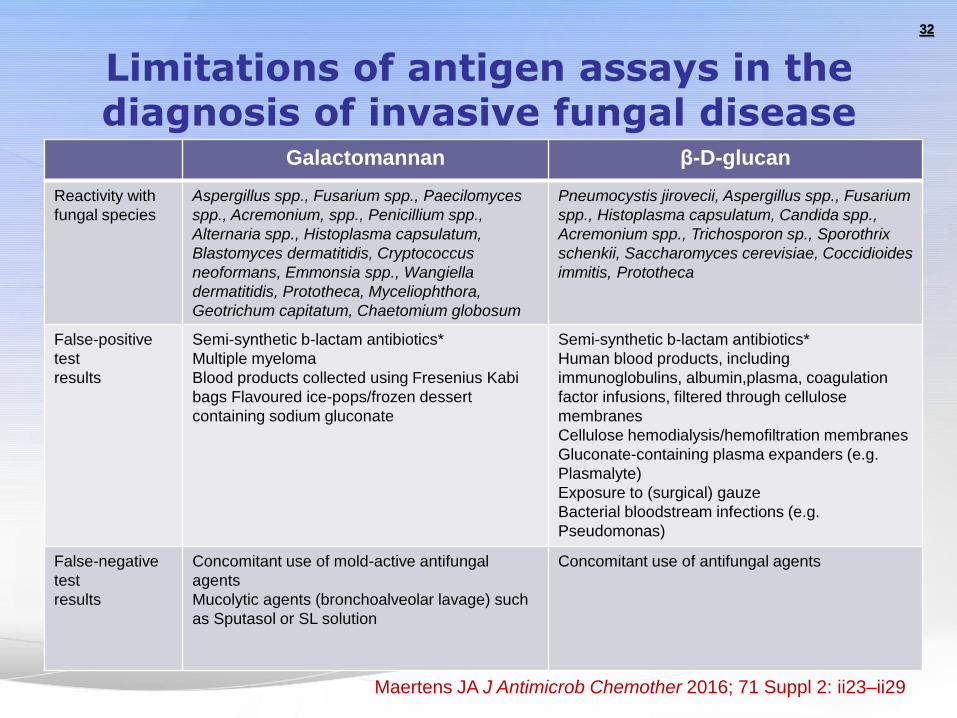
Limitations of antigen assays in the diagnosis of invasive fungal disease
Galactomannan β-D-glucan
Reactivity with
fungal species
Aspergillus spp., Fusarium spp., Paecilomyces
spp., Acremonium, spp., Penicillium spp.,
Alternaria spp., Histoplasma capsulatum,
Blastomyces dermatitidis, Cryptococcus
neoformans, Emmonsia spp., Wangiella
dermatitidis, Prototheca, Myceliophthora,
Geotrichum capitatum, Chaetomium globosum
Pneumocystis jirovecii, Aspergillus spp., Fusarium
spp., Histoplasma capsulatum, Candida spp.,
Acremonium spp., Trichosporon sp., Sporothrix
schenkii, Saccharomyces cerevisiae, Coccidioides
immitis, Prototheca
False-positive
test
results
Semi-synthetic b-lactam antibiotics*
Multiple myeloma
Blood products collected using Fresenius Kabi
bags Flavoured ice-pops/frozen dessert
containing sodium gluconate
Semi-synthetic b-lactam antibiotics*
Human blood products, including
immunoglobulins, albumin,plasma, coagulation
factor infusions, filtered through cellulose
membranes
Cellulose hemodialysis/hemofiltration membranes
Gluconate-containing plasma expanders (e.g.
Plasmalyte)
Exposure to (surgical) gauze
Bacterial bloodstream infections (e.g.
Pseudomonas)
False-negative
test
results
Concomitant use of mold-active antifungal
agents
Mucolytic agents (bronchoalveolar lavage) such
as Sputasol or SL solution
Concomitant use of antifungal agents
32
Maertens JA J Antimicrob Chemother 2016; 71 Suppl 2: ii23–ii29

Aspergillus: Utility of PCR
Emergence of useful test
in diagnosis of IA
Odds ratio comparable to
GM and b-D-glucan
Potential Advanteges
Finds SOME resistance
mutations
Identify to species level
Disadvantages
Validation method in
process
NOT yet available in US
Performance characteristics (DX)
Test Source Sens % Spec %
GM Blood 79 80-86
BAL 83-85 89
b-D-
glucan
Blood 56-77 81-97
PCR Blood 84-88 75-76
BAL 76-80 93-94
Culture Tissue 25-50 100
33
White PL Clin Infect Dis 2015;8:1293. Chong J Antimicrob Chemo 2016 Aug 15

Aspergillus – Resistant Isolates
Triazole resistant isolates
Specific mutations in CYP51A
(azole target)
Global emergence of point
mutations with TR in promoter
region (TR34/L98H &
TR46/Y121F/T289A)
environmental
Specific hotspots: G54, L98,
G138, M220, G448
Overexpression of cyp51B
Efflux pumps: CDR1B, ATRF etc
Cholesterol import: SrbA – import
of cholesterol as ergosterol
substitute
GOF mutation in HapE (P88L)
PCR will catch “some” of these
isolates
New pathways for RES continually
discovered
Genotype v Phenotype misses
some RES isolates
34
Buled A J Anticrob Chemother 2010;65:2116 Fraczek MG J Antimicrob Chemother 2015;68:1486
Buled A J Anticrob Chemother 2013;68:512 Gregson L Antimicrob Agents Chemother 2013;57:5778
Surveillance for Azole-Resistant Aspergillus fumigatus,
United States, 2011–2013
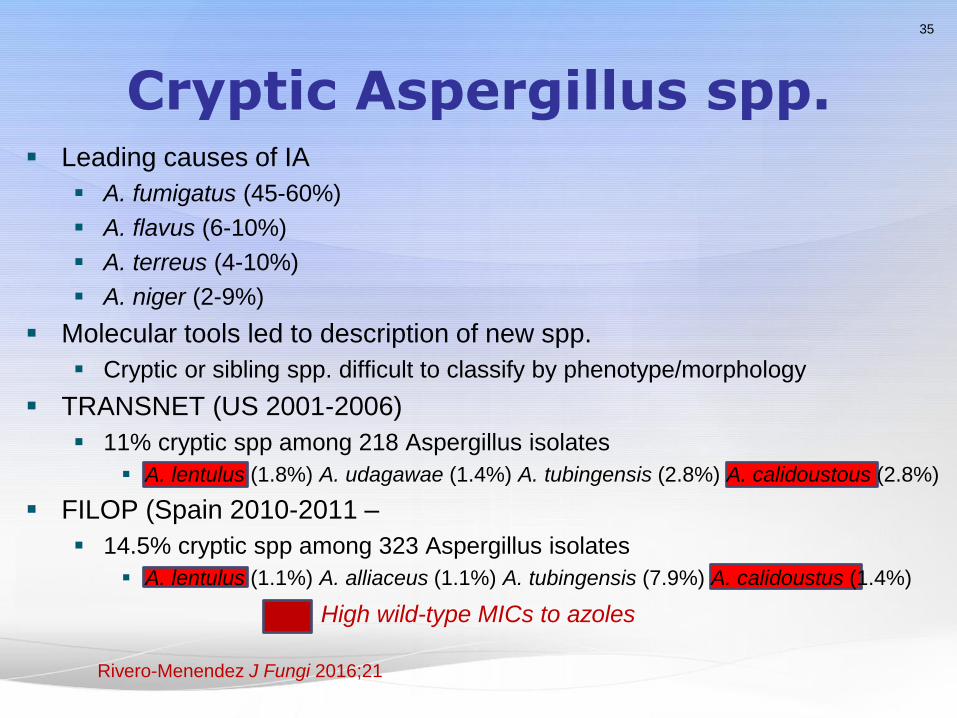
Cryptic Aspergillus spp. Leading causes of IA
A. fumigatus (45-60%)
A. flavus (6-10%)
A. terreus (4-10%)
A. niger (2-9%)
Molecular tools led to description of new spp.
Cryptic or sibling spp. difficult to classify by phenotype/morphology
TRANSNET (US 2001-2006)
11% cryptic spp among 218 Aspergillus isolates
A. lentulus (1.8%) A. udagawae (1.4%) A. tubingensis (2.8%) A. calidoustous (2.8%)
FILOP (Spain 2010-2011 –
14.5% cryptic spp among 323 Aspergillus isolates
A. lentulus (1.1%) A. alliaceus (1.1%) A. tubingensis (7.9%) A. calidoustus (1.4%)
35
High wild-type MICs to azoles
Rivero-Menendez J Fungi 2016;21

Aspergillus Treatment strong recommendations
Primary treatment with voriconazole
? Combination with echinocandin (caspofungin)?
Initiate antifungal therapy when IPA is strongly
suspected, while a diagnostic evaluation is
conducted.
Primary therapy with an echinocandin is not
recommended
Treat IPA for a minimum of 6–12 weeks,
Secondary prophylaxis should be initiated to
prevent recurrence in the immunosuppressed.
36
IDSA Guideline 2016; ATS Guideline 2011
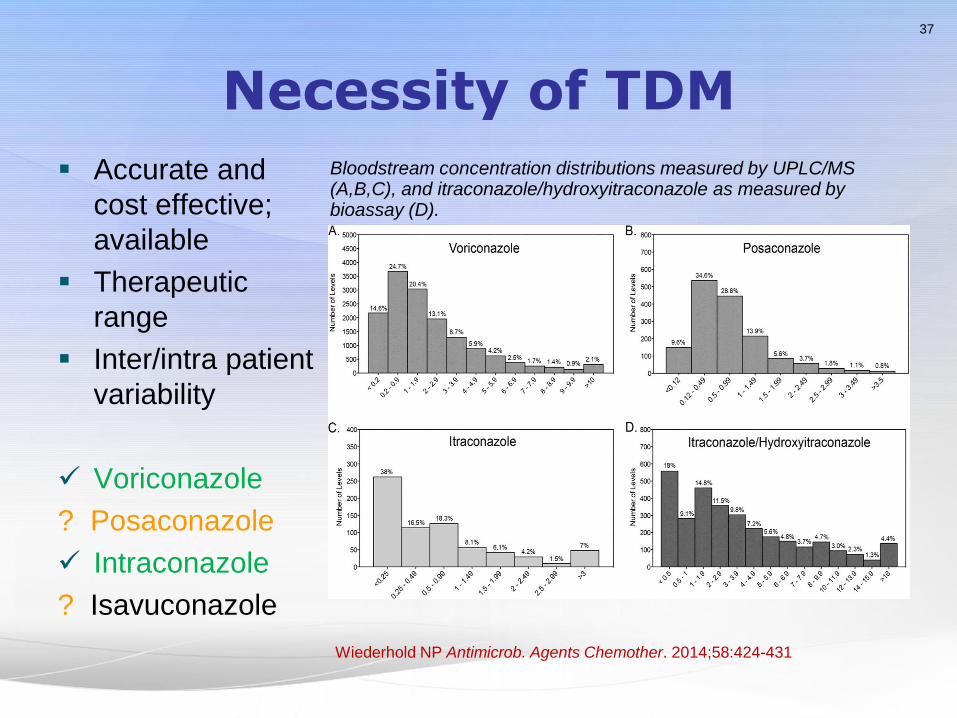
Necessity of TDM
Accurate and
cost effective;
available
Therapeutic
range
Inter/intra patient
variability
Voriconazole
? Posaconazole
Intraconazole
? Isavuconazole
37
Wiederhold NP Antimicrob. Agents Chemother. 2014;58:424-431
Bloodstream concentration distributions measured by UPLC/MS (A,B,C), and itraconazole/hydroxyitraconazole as measured by bioassay (D).
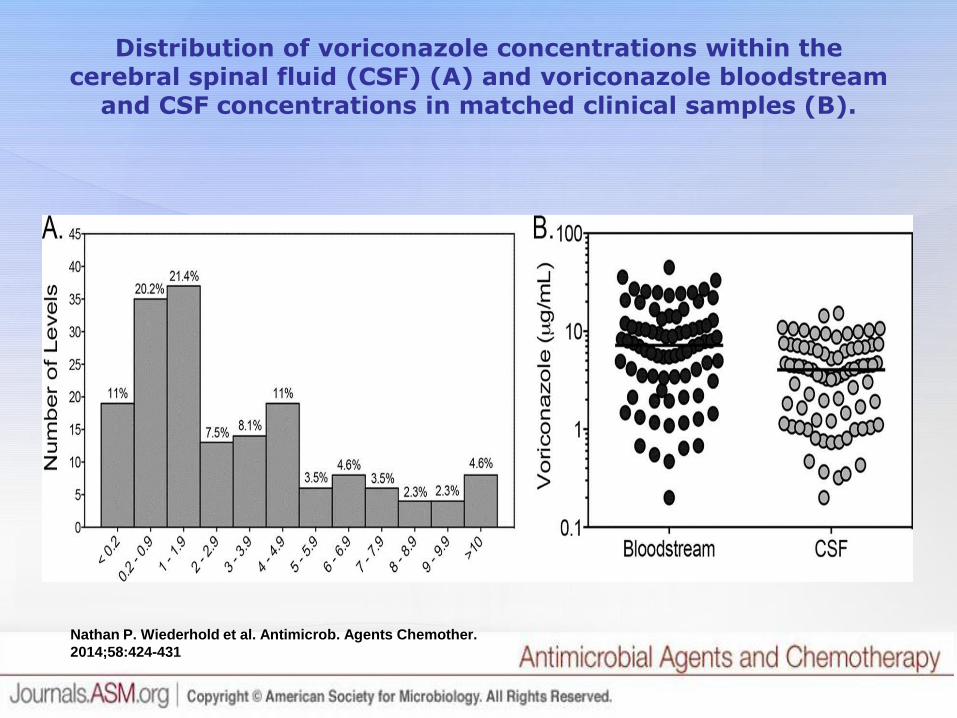
Nathan P. Wiederhold et al. Antimicrob. Agents Chemother.
2014;58:424-431
Distribution of voriconazole concentrations within the cerebral spinal fluid (CSF) (A) and voriconazole bloodstream
and CSF concentrations in matched clinical samples (B).

Molds that cause Mucormycosis Produce Large Ribbon-Like, Irregular Aseptate Hyphae
58 Cx-proven mold
infections – 4 tertiary
centers; blinded
assessment
Aspergillus infections
were misidentified as
MCR in 11%
Concordance between
histopath and culture for
non-mucormycosis
cases: only 68%
39
Haurany N 4th Advances Against Aspergillosis 2010 Rome,
Italy Poster #78
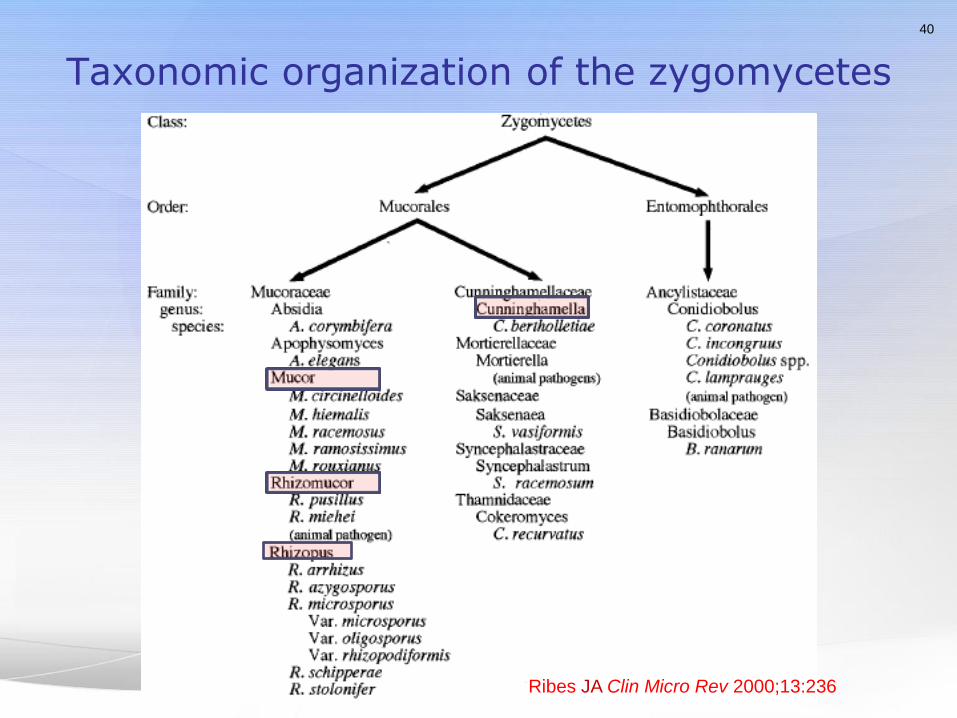
Taxonomic organization of the zygomycetes
40
Ribes JA Clin Micro Rev 2000;13:236
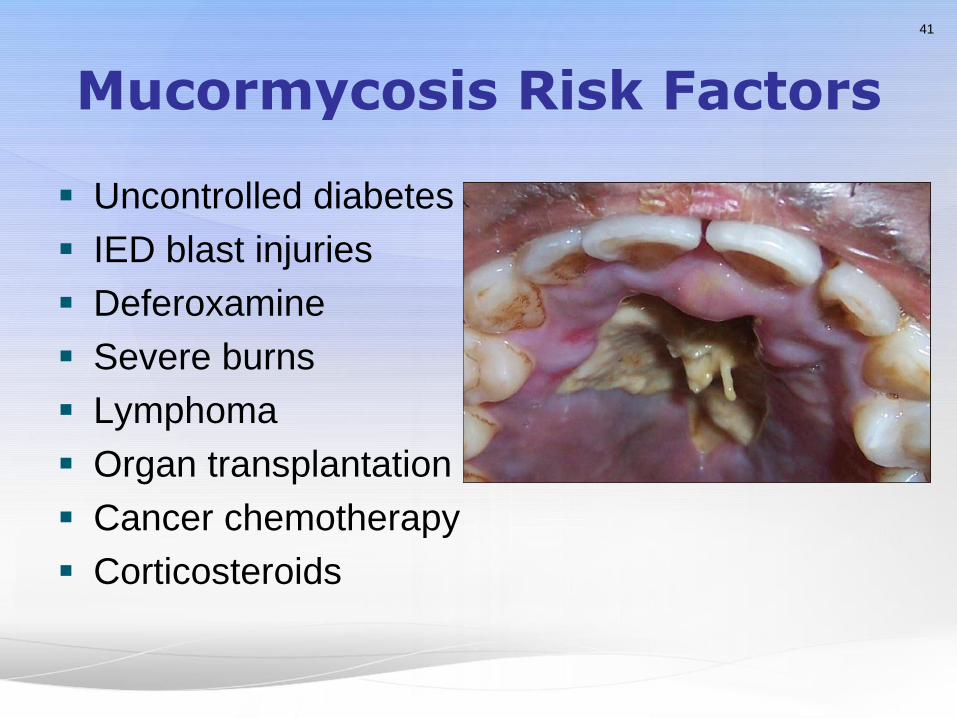
Mucormycosis Risk Factors
Uncontrolled diabetes
IED blast injuries
Deferoxamine
Severe burns
Lymphoma
Organ transplantation
Cancer chemotherapy
Corticosteroids
41
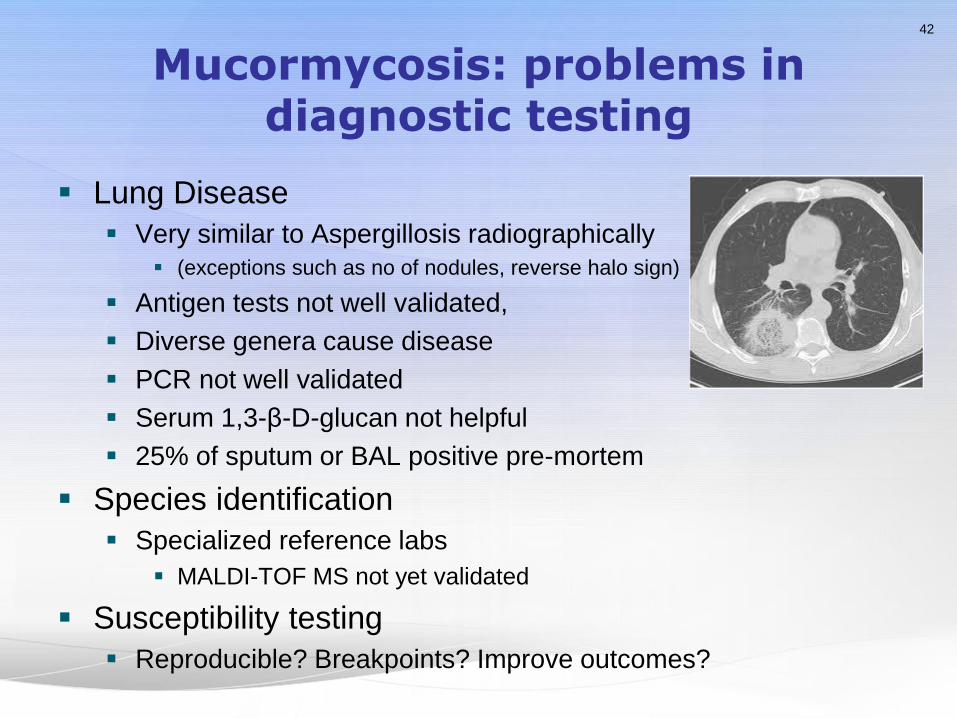
Mucormycosis: problems in diagnostic testing
Lung Disease
Very similar to Aspergillosis radiographically
(exceptions such as no of nodules, reverse halo sign)
Antigen tests not well validated,
Diverse genera cause disease
PCR not well validated
Serum 1,3-β-D-glucan not helpful
25% of sputum or BAL positive pre-mortem
Species identification
Specialized reference labs
MALDI-TOF MS not yet validated
Susceptibility testing
Reproducible? Breakpoints? Improve outcomes?
42

Mucormycosis: Prognostic Factors
Series of 391 patients with
heme malignancy, most die
with 12 weeks
The primary sites of infection
lungs (85%), nose and paranasal
sinus (10%), and other sites (5%).
The diagnosis was made only
at autopsy in 81 patients (21%).
Infection with Cunninghamella
spp – 2.78 fold increase in risk
of death (95% CI, 1.11-6.96;
p=0.029)
High MICs more common in
Rhizopus and Cunninghamella
43
Pagano Haematologica 2001;86:862
Kontoyiannis et al. BMC Infect Diseas 2016;16:730
Roden Clin Infect Dis 2005;41:634
44%
22%
5%
9%
4% 3%
3% 2% 8%
Mucorales infections
Rhizopus oryzae
Rhizopus microsporus
Lichthelmia corymbifera
Mucor circinelloides
Rhizopus pusillus
Cunninghamella bertholletiae
Mucor indicus
Apophycomyces
Other
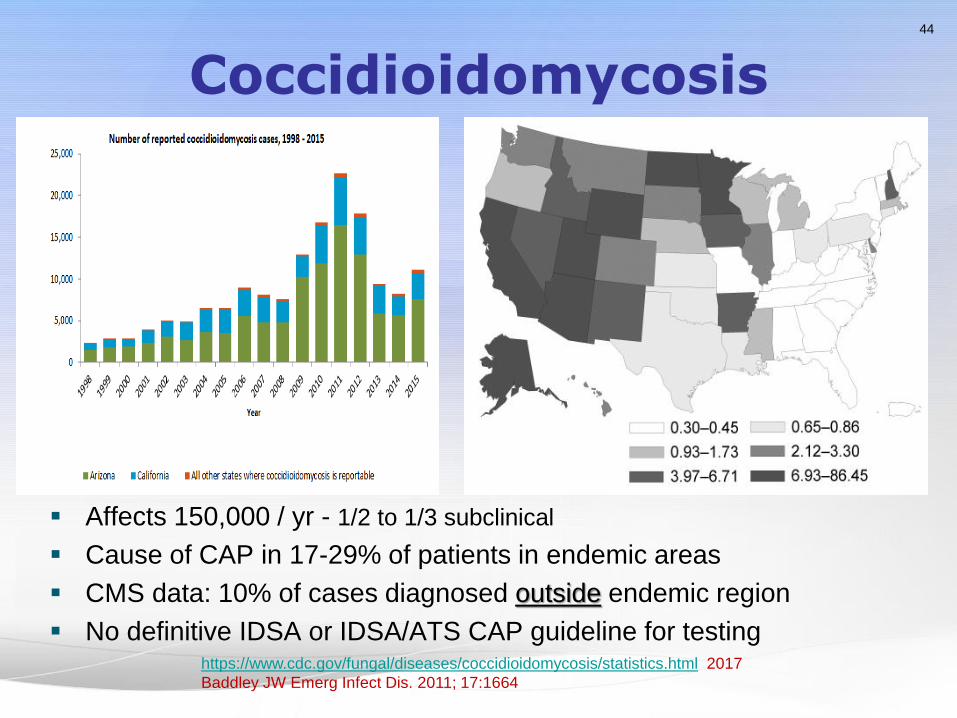
Coccidioidomycosis
Affects 150,000 / yr - 1/2 to 1/3 subclinical
Cause of CAP in 17-29% of patients in endemic areas
CMS data: 10% of cases diagnosed outside endemic region
No definitive IDSA or IDSA/ATS CAP guideline for testing
44
https://www.cdc.gov/fungal/diseases/coccidioidomycosis/statistics.html 2017
Baddley JW Emerg Infect Dis. 2011; 17:1664
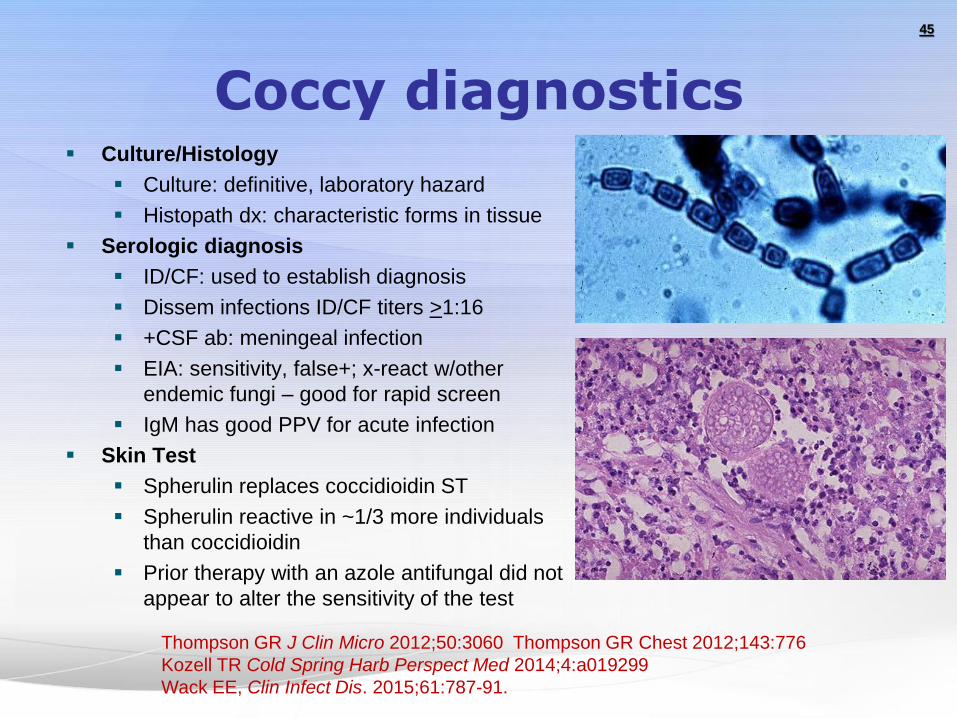
Coccy diagnostics Culture/Histology
Culture: definitive, laboratory hazard
Histopath dx: characteristic forms in tissue
Serologic diagnosis
ID/CF: used to establish diagnosis
Dissem infections ID/CF titers >1:16
+CSF ab: meningeal infection
EIA: sensitivity, false+; x-react w/other
endemic fungi – good for rapid screen
IgM has good PPV for acute infection
Skin Test
Spherulin replaces coccidioidin ST
Spherulin reactive in ~1/3 more individuals
than coccidioidin
Prior therapy with an azole antifungal did not
appear to alter the sensitivity of the test
45
Thompson GR J Clin Micro 2012;50:3060 Thompson GR Chest 2012;143:776
Kozell TR Cold Spring Harb Perspect Med 2014;4:a019299
Wack EE, Clin Infect Dis. 2015;61:787-91.

Emerging Diagnostics
Lateral Flow Assay
Developed specifically to
improve TAT
Simple to use
Yes/No answer in Urgent
Care/Clinic/ER
IgM and IgG
Semi-quantitative
MVista® Coccidioides
Antigen Quant EIA
CSF, Serum
Lab developed test
Also Blastomyces,
Histoplasma AG
46
Histoplamosis: cases/100,000 person-years
Blastomycosis: cases/100,000 person-years
MVista® Antigen Quant EIA

Histoplasmosis
Consider for “culture-negative” TB syndromes
Consider in differential for sarcoid
Galactomannan: test both blood and urine
Treatment: itraconazole or amphotericin
Measure itraconazole levels (1-3 mcg/mL)
Posaconazole for salvage therapy
Fluconazole NOT recommended
Echincandins NOT effective in animal models
47
2007 update by the Infectious Diseases Society of America.
Blastomycosis
All patients with disseminated
blastomycosis need a bone scan
to detect occult osteoarticular dx
Genitourinary infection may be
asymptomatic or associated with
symptoms of prostatism – urine culture!
Extrapulmonary blastomycosis can occur in the absence of
lung disease.
Most patients require therapy: Itraconazole
“Current serologic assays serve no role” (MKSAP)
48
2008 update by the Infectious Diseases Society of America.

Sporotrichosis
49
Exposure
Roses etc.
Cats!
Diagnosis
Culture, histopath
Treatment
Itraconazole
SSKI

Exserohilum rostratum
Exposure
Contaminated lots of methylprednisolone acetate
from a single compounding pharmacy
Treament:
Voriconazole + liposomal Amphoterecin B
50
CBS/AP October 25, 2012, 5:02 PM
323 infected in meningitis outbreak as experts study fungal culprit
Barry J. Cadden, the onetime president of a booming drug
compounding company, is on trial on charges of racketeering
and 25 counts of second-degree murder. Cadden's now defunct
company, the New England Compounding Center, produced the
fungus-riddled drugs that sickened ..more than 700. It killed 76.
USA Today Feb. 2, 2017
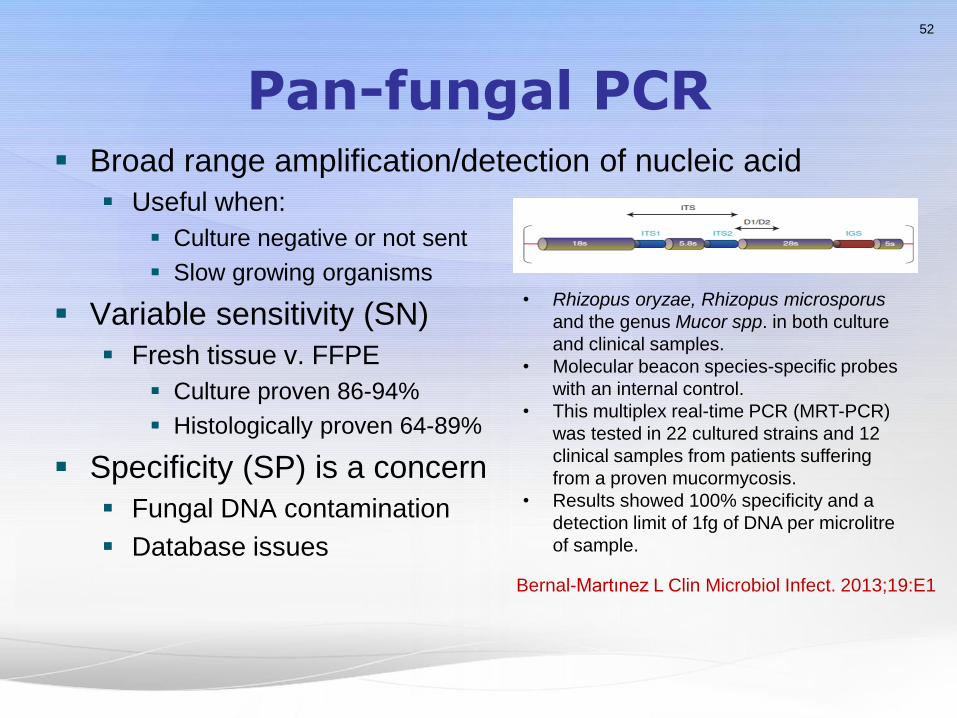
Pan-fungal PCR Broad range amplification/detection of nucleic acid
Useful when:
Culture negative or not sent
Slow growing organisms
Variable sensitivity (SN)
Fresh tissue v. FFPE
Culture proven 86-94%
Histologically proven 64-89%
Specificity (SP) is a concern
Fungal DNA contamination
Database issues
52
• Rhizopus oryzae, Rhizopus microsporus
and the genus Mucor spp. in both culture
and clinical samples.
• Molecular beacon species-specific probes
with an internal control.
• This multiplex real-time PCR (MRT-PCR)
was tested in 22 cultured strains and 12
clinical samples from patients suffering
from a proven mucormycosis.
• Results showed 100% specificity and a
detection limit of 1fg of DNA per microlitre
of sample.
Bernal-Martınez L Clin Microbiol Infect. 2013;19:E1

Alternative methods Not hypothesis driven
Proteomics
Profiling/Fingerprinting
MALDI/TOF
Patterns of antibodies
Pan-Fungal Detection of b-
Glucan
favorable NPV
Able to detect multiple pathogens
PCR fungal ribosomal targets
53
The variable regions can provide information that discriminate to the
species level, depending on genus, include ITS1, ITS2, and D1/D2.
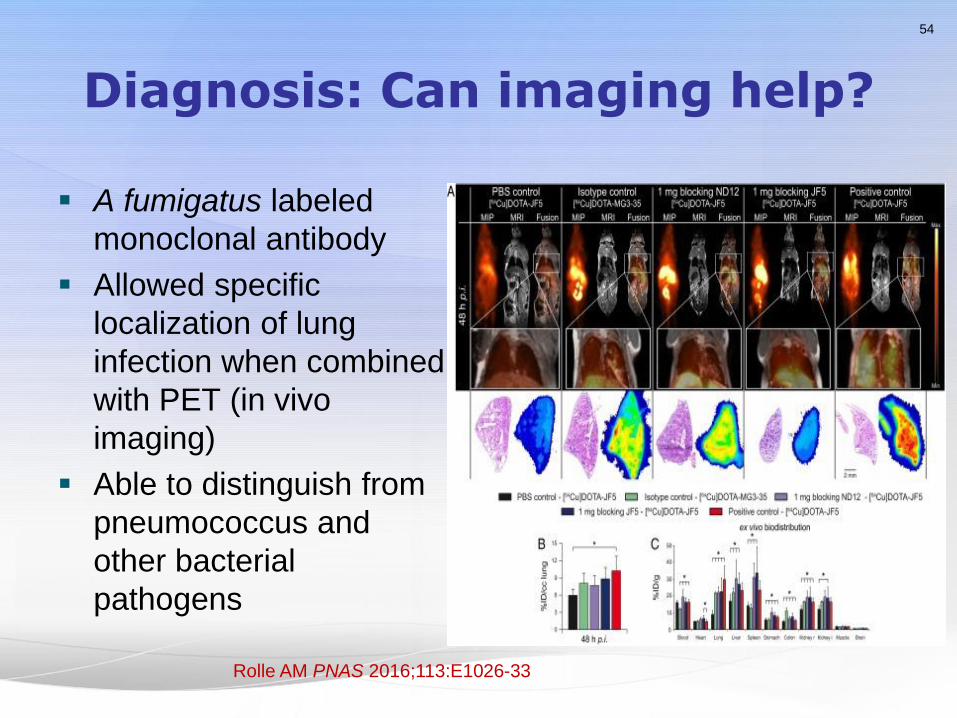
Diagnosis: Can imaging help?
A fumigatus labeled
monoclonal antibody
Allowed specific
localization of lung
infection when combined
with PET (in vivo
imaging)
Able to distinguish from
pneumococcus and
other bacterial
pathogens
54
Rolle AM PNAS 2016;113:E1026-33

Current Diagnostics Infection
Culture
/histopath
Biomarker for Diagnosis Response
To Therapy
Antibody
Antigen/marker
Aspergillosis Yes –
invasive
No-invasive
disease
Galatomannan/β
-D-glucan/PCR
Increasing
evidence
Candidiasis Routine Investigational
(anti-mannan)
PCR mannan/β-
D-glucan/PCR
No
Cryptococcus Routine No Yes/PCR Yes (CSF
antigen)
Histoplasmosis Culture-
delay
Limited Yes Yes
(Antigen)
Coccidioidomycosis Culture-
delay
Yes Antigen in CSF Yes
(Antibody)
Paracoccidioidomycosis Culture-
delay
Yes Yes Unknown
Mucormycosis Yes-
invasive
No Investigational No
Other molds Yes-
invasive
No Investigational No
55

56
What’s Learned?
Diagnosis: Targeted populations
New monitoring tests
Prognosis: Variability
Treatment: New agents