behavior group powerpoint
TRANSCRIPT

BEHAVIORAL ASSESSMENT: BASC II AND
ACHENBACH
Nikole Coleson
Jordan Morrison
Megan Lambert
Lauren Riley

BEHAVIOR ASSESSMENT
SYSTEM FOR CHILDREN,
SECOND EDITION
(BASC II)
Basics of the BASC II
Authors are Cecil R. Reynolds and Randy W. Kamphaus,
PhD
Published by Pearson
Administered by those who have appropriate graduate
coursework, as well as supervised experience with
administration.
Multimethod (different components) and
Multidimensional (different aspects of behavior are
measured).

Components to the BASC II Teacher Rating Scale (TRS)
Parent Rating Scale (PRS)
TRS and PRS measure OBSERVABLE BEHAVIORS from OUTSIDE
PERSPECTIVES, not the student his/ her self.
Structured Developmental History form (SDH)
Parent(s) can fill out on own or through interview
Student Observation System (SOS)
Self-Report of Personality (SRP)
Assessment which the student fills out as a self-assessment

Aspects of Behavior Measured
Hyperactivity
Aggression
Conduct Problems
Anxiety
Depression
Somatization (“tendency to be overly sensitive […] to minor physical problems[…]”)
Attention Problems
Learning Problems
Atypicality
Withdrawal
Adaptability
Social Skills
Leadership
Study Skills
Functional Communication
Clinical Scale Measures Adaptive Behavior Scale

Aspects of Behavior Measured (Cont.)
Externalizing Problems
Composite
Internalizing Problems
Composite
School Problems
Behavioral Symptoms
Some aspects are on TRS/ PRS only, OR
on SRP only:
Alcohol Abuse, Negative Emotionality,
Resiliency, etc.
Composite Scales
Clinical and Adaptive Scales
Clinical Scale: Measures maladaptive behaviors. An average or below-
average score on this scale means that the student’s behaviors are
“normal” (NOT clinically significant).
Adaptive Scale: Measures adaptive skills. An average or above-
average score on this scale means that the student’s behaviors are
“normal” (NOT clinically significant).

With ASSIST software, other, optional scales may
be added:
Anger Control
Ego Strength
Mania, Test Anxiety
Bullying
Developmental Social Disorders
Emotional Self-Control
Executive Functioning
Negative Emotionality
Resiliency

Component Information
Different components of BASC II may be used in different instances.
Components can be used in isolation, OR combination
SRP may be used from age 8-25, other components may be used
from age 2-21 under different forms.
Questioning
Some similarity between TRS and PRS, though some questions are
unique to one or the other only.
Each question in the SRP, TRS an PRS have 4 multiple choice
answers, denoting how often the behavior in question occurs
N (Never)
S (Sometimes)
O (Often)
A (Almost Always)
Participants are encouraged to put an answer down for every question-
no more than 2 may be mis-marked for accurate scoring.

Administration/ Scoring Methods Administration seems to be exclusively paper-and-pencil for the current
version of the BASC
Scoring may be completed by hand
Test that student, parent, or teacher fills out is on carbon-free paper, with the
scoring system underneath. Responses are assigned numerical point values
and go into boxes to be added up and interpreted by the scorer.
Scoring can also be completed via Q-Local software, ASSIST/ ASSIST
Plus Software, or Q-Global web-based scoring

Uses of the BASC
Aide in clinical diagnoses of behavior problems
Assessing/ developing IEP’s for students with emotional and behavioral
disorders (EBD)
Program evaluation (how is Head Start helping Johnny with his anger
issues?)
Forensic Evaluation
For further research on behavior problems

Reliability and Validity Measures Both reliability and validity measures are given in the BASC II manual
for the TRS, PRS, and SRP scales
Within each component, reliability is given for all composite scales
(Externalizing Problems, Internalizing Problems, School Problems, and
Behavioral Symptoms), Clinical Behavior Scales, Adaptive Behavior
Scales, and all aspects of behavior within each scale.
Within most scale/ behavior aspect, reliability and validity are separated
by age range, sex, and LD/ADHD status

A Brief Glimpse…R
elia
bili
ty/ V
alid
ity
TRS
Composite Scales
Externalizing, Internalizing, etc.
Clinical ScaleDepression,
Hyperactivity, etc.
PRS Adaptive ScaleAdaptability,
Social Skills, etc.
SRP

Adaptive
Behavio
r Adaptability
Adolescent
Male
Nondisabled
LD
ADHDFemale
Child
PreschoolStudy Skills
Func. Comm.
Social Skills
Leadership

Compone
nt
Coefficien
t Alpha
(Median
Range)
Test-Retest
(Median Range)
Student Pop. With Lower
Reliability
Behavioral
Aspects with
Lower
Reliability
TRS .84- .89
.83 (Preschoolers) .88
(Children) .79
(Adolescents)
2-3 year olds, Preschoolers,
Males 15-18, Students with
LD/ ADHD
Functional
Communication
, Leadership,
Adaptability,
Withdrawal,
Learning
Problems,
Somatization,
Anxiety
PRS 80- .87
.76 (Preschoolers), .84
(Children) and .82
(Adolescents)
No sig. lag in pop.
Upward trend with age
Activities of
Daily Living
SRP.75- .83
71 (children) .75
(adolescents) .83 (College-
Age)
Children/ Adolescents with
LD, Males with LD/ Males
with ADHD
No aspects
significantly
behind

POSITIVES We Discussed
High reliability coefficients overall
Time-tested, well-recognized
Short administration times (10-30 minutes per component)
Good norm selection and reconsiderations in the second version
of the assessment
NEGATIVES We Noticed
Low(er) reliability coefficients for the SRP
Low(er) interpreter reliability coefficients for the TRS
Possibly cost-prohibitive

ACHENBACH SYSTEM OF
EMPIRICALLY BASED
ASSESSMENT (ASEBA)

Basics of the Achenbach
Dr. Thomas Achenbach- publisher
Published by its own company (ASEBA)
The ASEBA has assessment forms appropriate for virtually all ages:
Preschool Assessments (Ages 1.5- 5 years)
School-Age Assessments (Ages 6-18 years)
Adults (18-59) and Older Adults (Ages 60- 90 +)
(For the purposes of this presentation, we will be focusing on the Pre-School
and School-Age forms)
Preschool Age Assessments
Child Behavior Checklist for Ages 1.5- 5 (CBCL/11/2-5)
Parent portion
Caregiver-Teacher Report Form for Ages 1.5- 5 (C-TRF)
Teacher portion

Preschool Assessments
Child Behavior Checklist for Ages 1.5- 5 (CBCL/11/2-5)
Mother, Father, or Guardian views a list of 99 behaviors, and rates their
occurrences on the student in question on a short, Likert-type scale (0= Not
True, 1= Somewhat or Sometimes True, 2= Very True or Often True).
Open-ended questions included as well (“What concerns you most about
the child?,” etc.)
Language Development Survey (LDS) included. Asks parents for health/
language history, as well as what words know.
Preschool Assessments (Cont.) Caregiver-Teacher Report Form for Ages 1.5- 5 (C-TRF)
Caregiver or teacher fills out a list of several behaviors, similar to the CBCL/11/2-5
Open-ended questions included as well (“What concerns you most about the child?,” etc.)
BOTH the CBCL/11/2-5 and the C-TRF score rate students according to the following scales: Internalizing Problems
Externalizing Problems
Total Problems
Stress Problems
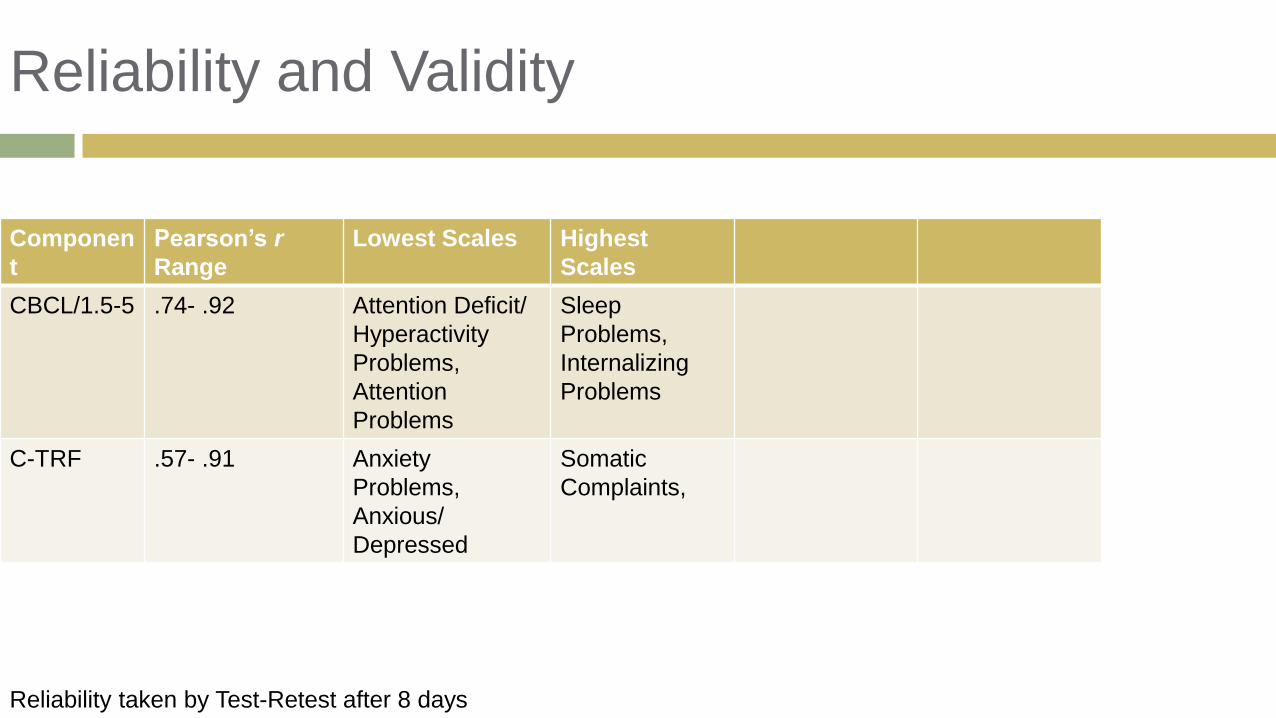
Reliability and Validity
Componen
t
Pearson’s r
Range
Lowest Scales Highest
Scales
CBCL/1.5-5 .74- .92 Attention Deficit/
Hyperactivity
Problems,
Attention
Problems
Sleep
Problems,
Internalizing
Problems
C-TRF .57- .91 Anxiety
Problems,
Anxious/
Depressed
Somatic
Complaints,
Reliability taken by Test-Retest after 8 days
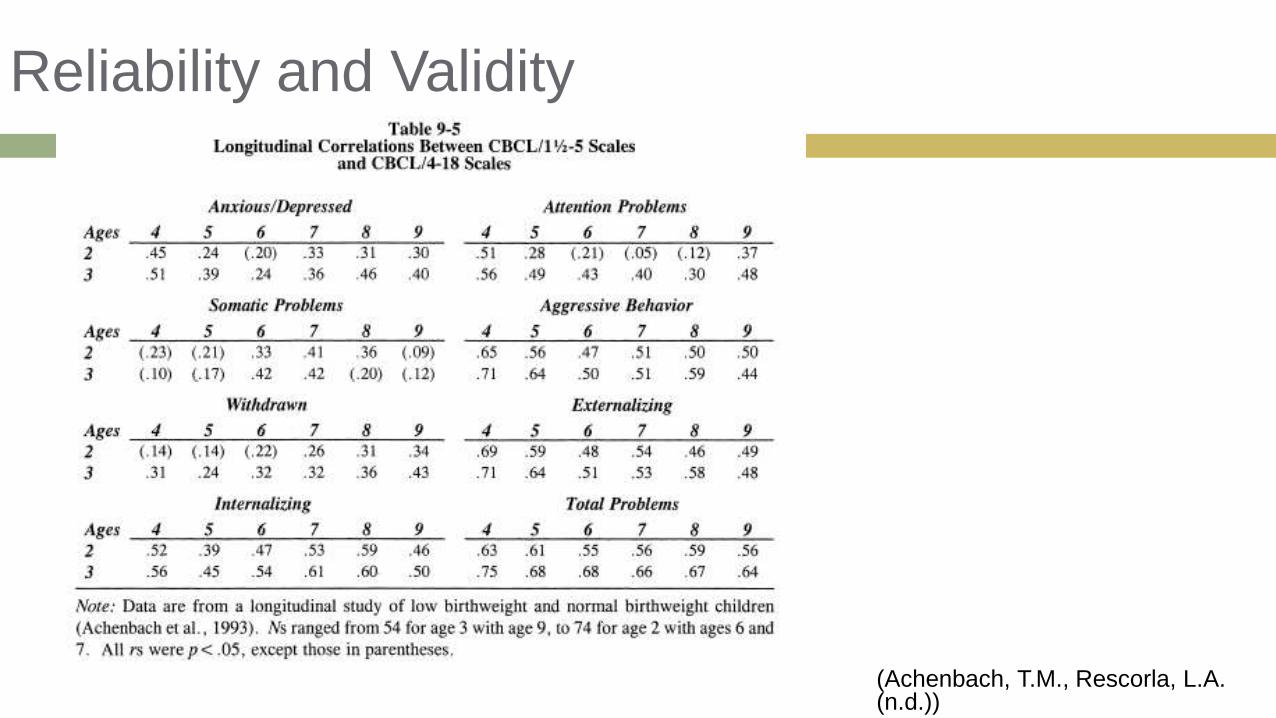
Reliability and Validity
(Achenbach, T.M., Rescorla, L.A. (n.d.))

School-Age Assessments
Child Behavior Checklist for Ages 6-18 (CBCL/ 6-18)
Teacher’s Report Form for Ages 6-18 (TRF/6-18)
Youth Self-Report for Ages 11-18 (YSR/11-18)
Semistructured Clinical interview for Children & Adolescents (SCICA/
Ages 6-18)
Test Observation Form (TOF)
Direct Observation Form (DOF)
Brief Problem Monitor (BPM)
School-Age Assessments
CBCL/6-18
Completed by parents or guardians of the student
Begins with listing of different hobbies/ favorite activities of the student, as
well as time engaged in these activities and how well they are completed
compared to others of his/her age.
Open-ended questions included
List of behaviors are presented with a 0-2 Likert-type scale
School-Age Assessments TRF/6-18
Completed by teachers/ school staff
Teachers evaluate how well they know the student in question, as well as
their academic performances (to include recent achievement tests).
List of behaviors are presented with a 0-2 Likert-type scale

School-Age Assessments
YSR/11-18
Completed by the student themselves
Students complete assessment of their favorite hobbies, sports,
etc. They also evaluate their performances, as well as time spent
on each (much like the CBCL/6-18)
Evaluate their close friendships
List of behaviors are presented with a 0-2 Likert-type scale

School-Age Assessments
Empirically-based scales assessed on these 3 school-age assessments
are:
Anxious/Depressed
Withdrawn/Depressed
Somatic Complaints
Social Problem
Thought Problems
Attention Problems
Rule-Breaking Behavior
Aggressive Behavior

School-Age Assessments
DSM-5 oriented scales assessed are:
Affective Problems
Anxiety Problems
Somatic Problems
Attention Deficit/ Hyperactivity Problems
Oppositional Defiant Problems
Conduct Problems

School-Age Assessments
Test Observation Form (TOF) for Ages 2-18
Filled out by a test examiner or other observer.
Examiner administers an IQ or other test and fills out the TOF while the student is taking the other exam. The examiner is evaluating the child’s behavior while he or she is taking the IQ assessment.
Test examiner gives background on any disability or disabilities that the student is currently diagnosed with. There are blank sheets available for free-form notes, and then the examiner is to fill out a behavioral scale.
125 items for rating children’s problems during achievement testing on a 4-point scale 0= No occurance
1= Very slight or ambiguous occurrence
2= Definite occurrence with mild to moderate intensity/ frequency and less than 3 months total duration
3= Definite occurrence with severe intensity, high-frequency, or 3 or more minutes total duration.

School-Age Assessments Semistructured Clinical interview for Children & Adolescents (SCICA/
Ages 6-18)
One form for children 6-11 and another for children 12-18.
Open-ended questions covering academic performance, preferred activities,
self-perceptions, and others.
School-Age Assessments
Direct Observation Form (DOF)/ Ages 6-11
“Observer” who has familiarity with behavioral assessment and child
behavior, such as a paraprofessional, university student, research
assistant, or other professional in a closely related field, typically
administers this assessment.
Observer will write a description of the student’s behavior during a
10-minute period in a group setting, as well as rate on-task behavior at 1-
minute intervals.
After 10 minutes, the observer is given a list of 88 behaviors, and
they are asked to evaluate the student on each one.
This assessment is recommended to be completed 3-6 times over a
2 day period.

School-Age Assessments Brief Problem Monitor (BPM)
Three assessments: Parent Form (BPM-P) Ages 6-18
Teacher Form (BPM-T) Ages 6-18
Youth Form (BPM-Y) Ages 11-18
Forms are completed in 1-2 minute intervals
There are parallel items and scales between the BPM and the: CBCL
TRF
YSR
These parallel items enable comprehensive behavioral assessment.
Items are to be ranked on a 0-2, Likert-type scale.
18-19 items, with room for additional items to also be ranked.
Included in the Achenbach as a means of frequent, brief assessment for students with suspected behavioral difficulties.
Multiple forms of the BPM allow data to be compared from multiple sources

Reliability and ValidityRange (r): .80- .93
Highs: Social (Working), Somatic
Complaints, Attention Problems
Lows: Anxiety Problems,
Activities (Academic), Anxious/
Depressed
Range (Coefficient Alpha): .63-
.94
Highs: Aggressive Behavior,
Externalizing.
Lows: School (Behaving), Social
(Working), Activities (Academic)
Range (r): .67- .91
Highs: School (Behaving),
Lows: Withdrawn/
Depressed, Anxiety
Problems, Somatic
Problems
Range (Coefficient Alpha):
.55- .90
Highs: Externalizing,
Internalizing
Lows: Social (Working),
Anxiety Problems
Range (r): .60- .96
Highs: ADH Problems,
Inattention, Social Problems
Lows: Withdrawn/
Depressed, Affective
Problems,
Range (Coefficient Alpha):
.72- .95
Highs: Attention Problems,
Aggressive Behavior,
Externalizing
Lows: Somatic Complaints,
Thought Problems


Purposes and Uses Mental Health Services
Schools
Medical Settings
Child and Family Services
Multicultural Assessment
HMOs
Public Health Agencies
Child Guidance
Training
Research
“Develop a more differentiated picture of child and adolescent psychopathology than was provided by the prevailing diagnostic system”.

Positives Discussed
Open-ended responses available on most scales
Several scales available for school-age children
Multiple people involved in student’s life assess different ways.
TOF= Unique assessment we have not heard of in research for other
classes
Qualitative Components

Negatives Discussed
Overall, low reliability and validity coefficients
Significant time needed to complete entire battery of assessments
Variability may exist between qualitative components of the answers-
more difficult to score and provide reliability coefficients for.
What Questions Can We Answer?