benefits guide 2016-17 - wdmcs.org · wdmcs benefits guide — 3 wellmark bcbs of iowa benefit...
TRANSCRIPT

Benefits Guide 2016-17
Inside this Guide
Enrollment ...........................................................................................................................................................................1
Benefits Comparison .............................................................................................................................................................2
Your Health Plan Options .......................................................................................................................................................4
Prescription Drug Benefits .....................................................................................................................................................4
Plan Grandfathered Status.....................................................................................................................................................4
Dental Benefits .....................................................................................................................................................................5
Voluntary Vision Benefits .......................................................................................................................................................6
Life Benefits ..........................................................................................................................................................................7
Long-Term Disability Benefits ................................................................................................................................................8
Employee Assistance & Wellness Program Benefits .................................................................................................................8
Flexible Spending Account .....................................................................................................................................................9
FSA—Premium-Only Plan ......................................................................................................................................................9
Retirement Plans ................................................................................................................................................................10
Retirement Investors’ Club ..................................................................................................................................................10
Early Retirement & Planning ................................................................................................................................................10
Special Points of Interest
The information in this Benefits Guide is presented for illustrative purposes and is based on information provided by the employer. The text contained in this guide was taken from various summary plan descriptions and benefit information. While every effort was taken to accurately report your benefits, discrepancies or errors are always possible. In case of discrepancy between the guide and the actual plan documents, the actual plan documents will prevail.
All information is confidential, pursuant to the Health Insurance Portability and Accountability Act of 1996.
If you have any questions about this guide, contact the benefits adviser at 515-633-5076.


WDMCS Benefits Guide — 1
You may enroll for benefits when you are hired or during a qualifying life event. West Des Moines Community Schools (WDMCS) provides all eligible employees with single medical and dental coverage. However, all eligible employees are required to enroll online or fill out an enrollment form to secure coverage.
Upon timely enrollment, your coverage will be effective the first day of the month following your start date. If your start date is on the first day of the month, insurance coverage will begin that day.
Under Section 125 of the Internal Revenue Service (IRS) code, you are allowed to pay for certain group insurance premiums with tax-free dollars. This means your premium deductions are taken before federal and state income and Social Security taxes are calculated, saving you up to 23 percent or more, depending on your tax bracket.
However, you must make your benefit elections carefully, including the choice to waive coverage for any Volunteer Benefits including Flexible Spending. Your pretax elections will remain in effect until the next annual enrollment period unless you experience an IRS-approved qualifying event change in status.
Qualifying change in status events include, but are not limited to:• Marriage, divorce, or legal separation• Death of spouse or other dependent• Birth or adoption of a child (60 days)• A spouse’s employment begins or ends• A dependent’s eligibility status changes due to age, student status, marital status,
or employment• You or your spouse experience a change in work hours that affect benefits
eligibility• Relocation into or outside of your plan’s service area• Loss of eligibility under Medicaid or CHIP (60 days)• Eligibility for premium assistance under Medicaid or CHIP (60 days)
If you experience one of the above changes to your qualified status, please contact the Benefits Office within 30 days of the event.
Annual EnrollmentAnnual enrollment is held in late April or early May. It is a two-week period of time in which you can go into BCEnroll and sign up for your flex benefits. Remember, you need to do this every year.
You may also change your medical plan (from Plan 1 to Plan 2 or Plan 3, or vice versa), or you may choose to add or drop a dependent from any of your plans. You may also choose to apply to or change your supplemental life, spouse life and child life accounts.
The exact dates and further information for Annual Enrollment for the 2017-18 year will be sent via the staff e-newsletter. Please watch for this information to come by email in spring.
InformationInformation on benefits and wellness will be provided in the staff e-newsletter.
Enrollment

WDMCS Benefits Guide — 2
2016-17 Medical and Prescription Drug Benefit Comparison
Wellmark BCBS of IowaAlliance Select — Plan 1 Alliance Select — Plan 2 Alliance Select — Plan 3
PPO Benefit Overview In-Network Out-of-Network In-Network Out-of-Network In-Network Out-of-Network
Deductible - Calendar Year Single $300 $300 $600 $600 $1,000 $1,000 Family $600 $600 $1,200 $1,200 $2,000 $2,000 Coinsurance 10% 20% 10% 20% 10% 20%Out-of-Pocket Max — Calendar Year Single $750 $750 $1,500 $1,500 $2,500 $2,500 Family $1,500 $1,500 $3,000 $3,000 $5,000 $5,000 Lifetime Maximum Unlimited Unlimited Unlimited Unlimited Unlimited Unlimited
Benefit Highlights for Plans 1, 2, & 3BENEFIT HIGHLIGHTS In-Network Out-of-NetworkPhysician Visit-Office Visits
Routine: Physicals, Gynecological Exam, Pap smears, and mammograms
$15 Copay Waived, 100% paid by Wellmark
$25 Copay
Non-Routine: Physicals, Gynecological Exam, Pap smears, and mammograms
$15 Copay $25 Copay
Routine Eye Exam (Includes Refraction) $15 Copay Waived, 100% paid by Wellmark
$25 Copay
Well Child Care & Immunizations $15 Copay Waived, 100% paid by Wellmark
$25 Copay
Office Visit—Other than routine noted above $15 Copay $25 Copay
Chiropractic Care $15 Copay $25 Copay
Maternity Services
Prenatal & Postnatal Physician Services $15 Copay $25 Copay
Delivery & Surgery Charges (If doctor includes prenatal care with delivery charges, they will be screened with delivery charges.)
Deductible, 10% Coinsurance Deductible, 20% Coinsurance
Inpatient Hospital Care Deductible, 10% Coinsurance Deductible, 20% Coinsurance
Outpatient X-Ray & Laboratory Deductible, 10% Coinsurance Deductible, 20% Coinsurance
Hospital Services
Inpatient Deductible, 10% Coinsurance Deductible, 20% Coinsurance
Unlimited Hospital Days (Semi-Private), Private Room-Medically Necessary, Medications/Drugs, Nursing Care, Professional Services, X-Ray & Lab, Intensive/Coronary Care, Radiation Therapy, Administration of Blood
Outpatient
X-Rays & Laboratory, Ambulatory Surgery Deductible, 10% Coinsurance Deductible, 20% Coinsurance
X-Ray & Laboratories that are related to Routine Physicals (Mammograms, Colonoscopies, etc.)
Deductible waived, 10% Coinsurance
Deductible, 20% Coinsurance
WDMCS Benefits Guide — 3
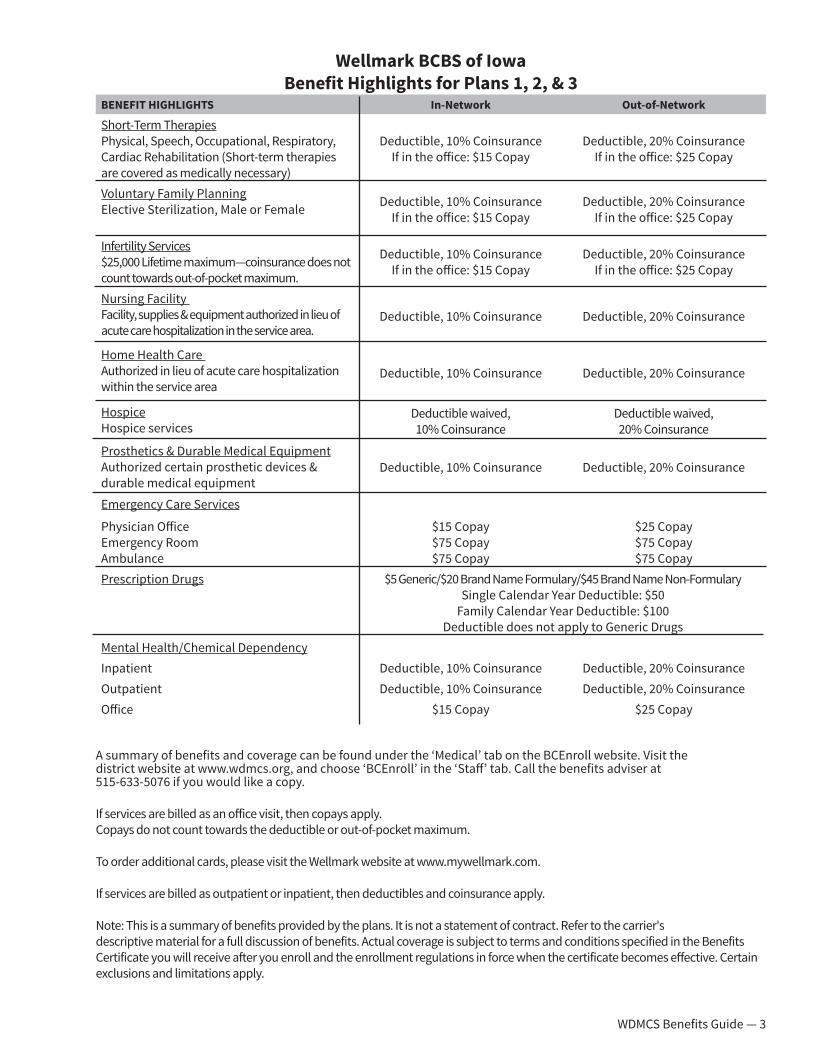
Wellmark BCBS of Iowa Benefit Highlights for Plans 1, 2, & 3
BENEFIT HIGHLIGHTS In-Network Out-of-Network
Short-Term Therapies Physical, Speech, Occupational, Respiratory, Cardiac Rehabilitation (Short-term therapies are covered as medically necessary)
Deductible, 10% Coinsurance If in the office: $15 Copay
Deductible, 20% Coinsurance If in the office: $25 Copay
Voluntary Family PlanningElective Sterilization, Male or Female Deductible, 10% Coinsurance
If in the office: $15 CopayDeductible, 20% Coinsurance
If in the office: $25 Copay
Infertility Services $25,000 Lifetime maximum—coinsurance does not count towards out-of-pocket maximum.
Deductible, 10% Coinsurance If in the office: $15 Copay
Deductible, 20% Coinsurance If in the office: $25 Copay
Nursing Facility Facility, supplies & equipment authorized in lieu of acute care hospitalization in the service area.
Deductible, 10% Coinsurance Deductible, 20% Coinsurance
Home Health Care Authorized in lieu of acute care hospitalization within the service area
Deductible, 10% Coinsurance Deductible, 20% Coinsurance
Hospice Hospice services
Deductible waived, 10% Coinsurance
Deductible waived, 20% Coinsurance
Prosthetics & Durable Medical EquipmentAuthorized certain prosthetic devices & durable medical equipment
Deductible, 10% Coinsurance Deductible, 20% Coinsurance
Emergency Care Services
Physician OfficeEmergency Room Ambulance
$15 Copay$75 Copay$75 Copay
$25 Copay$75 Copay$75 Copay
Prescription Drugs $5 Generic/$20 Brand Name Formulary/$45 Brand Name Non-Formulary Single Calendar Year Deductible: $50
Family Calendar Year Deductible: $100 Deductible does not apply to Generic Drugs
Mental Health/Chemical DependencyInpatient Deductible, 10% Coinsurance Deductible, 20% CoinsuranceOutpatient Deductible, 10% Coinsurance Deductible, 20% CoinsuranceOffice $15 Copay $25 Copay
A summary of benefits and coverage can be found under the ‘Medical’ tab on the BCEnroll website. Visit the district website at www.wdmcs.org, and choose ‘BCEnroll’ in the ‘Staff’ tab. Call the benefits adviser at 515-633-5076 if you would like a copy.
If services are billed as an office visit, then copays apply. Copays do not count towards the deductible or out-of-pocket maximum.
To order additional cards, please visit the Wellmark website at www.mywellmark.com. If services are billed as outpatient or inpatient, then deductibles and coinsurance apply. Note: This is a summary of benefits provided by the plans. It is not a statement of contract. Refer to the carrier's descriptive material for a full discussion of benefits. Actual coverage is subject to terms and conditions specified in the Benefits Certificate you will receive after you enroll and the enrollment regulations in force when the certificate becomes effective. Certain exclusions and limitations apply.

WDMCS Benefits Guide — 4
Plans 1, 2, and 3 have all of the same benefit options. The only differences are the deductible and out-of-pocket expenses. These plans use Wellmark’s Alliance Select PPO network, which consist of providers that participate directly with Alliance Select and providers that participate with other Blue Cross and/or Blue Shield preferred provider organizations (PPOs). These PPO providers offer services to members of contracting medical benefits plans at a reduced cost, which usually result in the least expense for you.
Non-PPO providers are either participating or nonparticipating. If you are unable to utilize a PPO provider, it is usually to your advantage to visit what we call a participating provider. Participating providers participate with a Blue Cross and/or Blue Shield Plan, but not with a PPO.
Other providers are considered nonparticipating, and you will usually pay the most for services you receive from them. To determine if a provider participates with this medical benefits plan, ask your provider. To find a participating provider:
• Go to www.wellmark.com. • Select ‘Find a Doctor or Hospital’• Click ‘Iowa and South Dakota Providers’• Select the appropriate network from the drop-down menu.
The deductible is $50 per person or $100 (maximum) per family. Copayment is $5 for Tier 1 medications, $20 for Tier 2 medications, and $45 for Tier 3 medications. The deductible is waived for Tier 1 drugs and well-child care immunizations.
The mail-order pharmaceutical service is available for certain prescriptions packaged in doses exceeding the maximum days’ supply covered under this Blue Rx Complete drug plan. A 30-day mail order prescription will be charged one copayment, and a 90-day supply will be charged two copayments.
Specialty pharmaceuticals are high-cost injectable, infused, oral, or inhaled drugs typically used for treating or managing chronic illnesses. These drugs often require special handling (e.g., refrigeration) and administration. They are not available through the mail-order drug program.
Specialty drugs may be covered under this medical benefit plan or under your Blue Rx Complete prescription drug plan. To determine whether a particular specialty drug is covered under this medical benefits plan or under your Blue Rx Complete prescription drug plan, consult the Wellmark Blue Rx Complete Drug list at www.wellmark.com, or call the Customer Service number at 1-800-800-5122.
The West Des Moines Community Schools believes the West Des Moines Community Schools’ Medical Plan is a “grandfathered health plan” under the Patient Protections and Affordable Care Act (the “Affordable Care Act”).
As permitted under the Affordable Care Act, a grandfathered health plan can preserve certain basic health coverage that was already in effect when the law was enacted. As a grandfathered health plan, we may not include certain consumer protections of the Affordable Care Act that apply to other plans. However, grandfathered health plans must comply with certain other consumer protections in the Affordable Care Act, like the elimination of lifetime limits on benefits.
Questions regarding which protections do and do not apply to a grandfathered plan and what might cause a plan to change from grandfathered health plan status can be directed to the benefits adviser.
Your Health Plan Options
Prescription Drug Benefits
Medical Plan Grandfathered Status
WDMCS Benefits Guide — 5
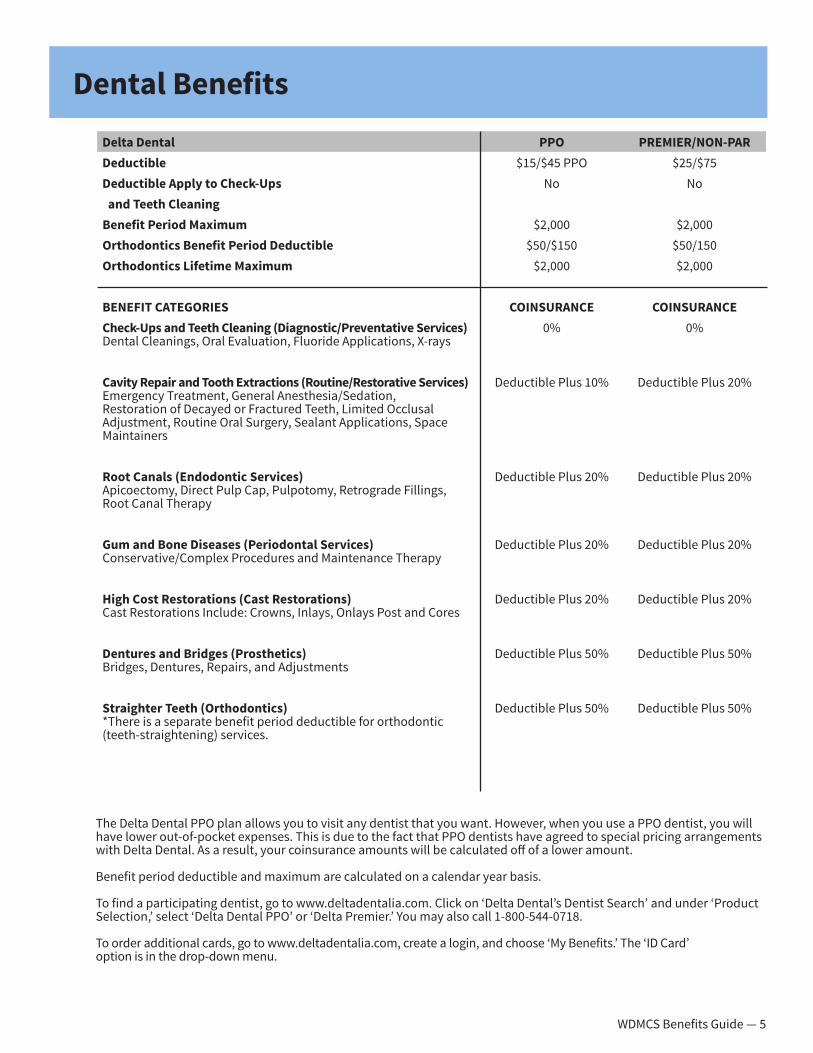
Delta Dental PPO PREMIER/NON-PARDeductible $15/$45 PPO $25/$75Deductible Apply to Check-Ups No No and Teeth CleaningBenefit Period Maximum $2,000 $2,000 Orthodontics Benefit Period Deductible $50/$150 $50/150Orthodontics Lifetime Maximum $2,000 $2,000
BENEFIT CATEGORIES COINSURANCE COINSURANCECheck-Ups and Teeth Cleaning (Diagnostic/Preventative Services) Dental Cleanings, Oral Evaluation, Fluoride Applications, X-rays
0% 0%
Cavity Repair and Tooth Extractions (Routine/Restorative Services) Emergency Treatment, General Anesthesia/Sedation, Restoration of Decayed or Fractured Teeth, Limited Occlusal Adjustment, Routine Oral Surgery, Sealant Applications, Space Maintainers
Deductible Plus 10% Deductible Plus 20%
Root Canals (Endodontic Services) Apicoectomy, Direct Pulp Cap, Pulpotomy, Retrograde Fillings, Root Canal Therapy
Deductible Plus 20% Deductible Plus 20%
Gum and Bone Diseases (Periodontal Services) Conservative/Complex Procedures and Maintenance Therapy
Deductible Plus 20% Deductible Plus 20%
High Cost Restorations (Cast Restorations) Cast Restorations Include: Crowns, Inlays, Onlays Post and Cores
Deductible Plus 20% Deductible Plus 20%
Dentures and Bridges (Prosthetics) Bridges, Dentures, Repairs, and Adjustments
Deductible Plus 50% Deductible Plus 50%
Straighter Teeth (Orthodontics)*There is a separate benefit period deductible for orthodontic (teeth-straightening) services.
Deductible Plus 50% Deductible Plus 50%
The Delta Dental PPO plan allows you to visit any dentist that you want. However, when you use a PPO dentist, you will have lower out-of-pocket expenses. This is due to the fact that PPO dentists have agreed to special pricing arrangements with Delta Dental. As a result, your coinsurance amounts will be calculated off of a lower amount.
Benefit period deductible and maximum are calculated on a calendar year basis.
To find a participating dentist, go to www.deltadentalia.com. Click on ‘Delta Dental’s Dentist Search’ and under ‘Product Selection,’ select ‘Delta Dental PPO’ or ‘Delta Premier.’ You may also call 1-800-544-0718.
To order additional cards, go to www.deltadentalia.com, create a login, and choose ‘My Benefits.’ The ‘ID Card’ option is in the drop-down menu.
Dental Benefits
WDMCS Benefits Guide — 6
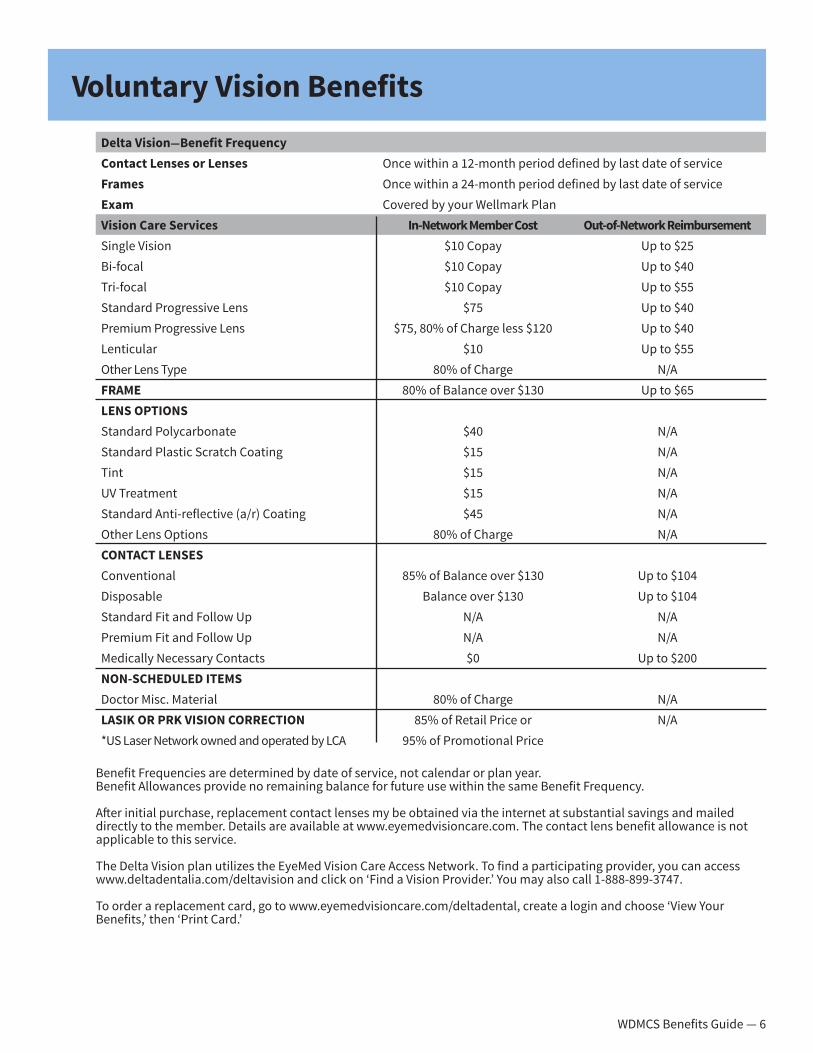
Delta Vision—Benefit FrequencyContact Lenses or Lenses Once within a 12-month period defined by last date of serviceFrames Once within a 24-month period defined by last date of serviceExam Covered by your Wellmark PlanVision Care Services In-Network Member Cost Out-of-Network ReimbursementSingle Vision $10 Copay Up to $25Bi-focal $10 Copay Up to $40Tri-focal $10 Copay Up to $55Standard Progressive Lens $75 Up to $40Premium Progressive Lens $75, 80% of Charge less $120 Up to $40Lenticular $10 Up to $55Other Lens Type 80% of Charge N/AFRAME 80% of Balance over $130 Up to $65LENS OPTIONSStandard Polycarbonate $40 N/AStandard Plastic Scratch Coating $15 N/ATint $15 N/AUV Treatment $15 N/AStandard Anti-reflective (a/r) Coating $45 N/AOther Lens Options 80% of Charge N/ACONTACT LENSESConventional 85% of Balance over $130 Up to $104Disposable Balance over $130 Up to $104Standard Fit and Follow Up N/A N/APremium Fit and Follow Up N/A N/AMedically Necessary Contacts $0 Up to $200NON-SCHEDULED ITEMSDoctor Misc. Material 80% of Charge N/ALASIK OR PRK VISION CORRECTION 85% of Retail Price or N/A*US Laser Network owned and operated by LCA 95% of Promotional Price
Benefit Frequencies are determined by date of service, not calendar or plan year.Benefit Allowances provide no remaining balance for future use within the same Benefit Frequency.
After initial purchase, replacement contact lenses my be obtained via the internet at substantial savings and mailed directly to the member. Details are available at www.eyemedvisioncare.com. The contact lens benefit allowance is not applicable to this service.
The Delta Vision plan utilizes the EyeMed Vision Care Access Network. To find a participating provider, you can access www.deltadentalia.com/deltavision and click on ‘Find a Vision Provider.’ You may also call 1-888-899-3747.
To order a replacement card, go to www.eyemedvisioncare.com/deltadental, create a login and choose ‘View Your Benefits,’ then ‘Print Card.’
Voluntary Vision Benefits

WDMCS Benefits Guide — 7
Madison National Life Insurance Company Basic Life with Accidental Death & Dismemeberment Insurance
9-10 Month (16 Pays) Employees
Spv. Non Unit & Certified 11-12 Month (24 Pays)
EmployeesAdministrators
Benefit Amount 1 x Annual Salary Rounded to Next Highest
$1,000
1 x Annual Salary Rounded to Next Highest
$1,000
2 x Annual SalaryRounded to Next Highest
$1,000Benefit Maximum $500,000 $500,000 $500,000 Age Reduction Schedule None None NoneMonthly Cost Paid in Full by WDMCS Paid in Full by WDMCS Paid in Full by WDMCSAccidental Death & Dismemberment
Mirrors Basic Life Insurance BenefitIncludes Additional Seat Belt, Airbag, Spouse Tuition Expenses, Child Care Benefit and
Child Higher Education Benefit SUPPLEMENTAL LIFE/AD&DEmployee Benefit Amount $10,000 increments up to $500,000Guarantee Issue $100,000 Spouse Benefit Amount* $5,000 increments up to $250,000Spouse Guarantee Issue $20,000 Child Benefit Amount* $2,000 increments up to $10,000Child Guarantee Issue $10,000
*Maximum of 50% of the employees amount of Supplemental Life
Monthly Cost Based on Age of Employee Amount Per $1,000 AD&D Rate<30 0.04 .015 per $1,00030-34 0.059 .015 per $1,00035-39 0.079 .015 per $1,00040-44 0.098 .015 per $1,00045-49 0.147 .015 per $1,00050-54 0.226 .015 per $1,00055-59 0.422 .015 per $1,00060-64 0.579 .015 per $1,00065-69 6.82 .015 per $1,00070-74 .848 .015 per $1,00075-99 .0594 .015 per $1,000Child Rates: Monthly premium rate for this coverage is 30 cents per $2,000, regardless of the number of eligible children covered. Age Reductions: Reduced to 65 percent at age 65, to 50 percent at age 70, and to 35 percent at age 75. Please note: Life insurance coverage of more than $50,000 is considered taxable income. Amounts over $50,000 will be taxed.
Identity theft assistance services are available through Madison National. Please call us toll-free, 24/7, at 855-860-3727.
If you are currently enrolled in voluntary employee life, you can elect an additional $10,000 at each renewal, up to the $100,000 guarantee issue, without providing evidence of insurability. Amounts over the Guarantee Issue require completion of an Underwriting Form. Please download this from BCEnroll or contact the benefits adviser at 515-633-5076. If you do not enroll when initially eligible and later decide to enroll, you will be required to complete the Underwriting Form for any amount applied for. Please note that if both spouses are employed by WDMCS, only one employee can elect Dependent Supplemental Life. Unmarried dependent children qualify up to age 26.
Life Benefits

WDMCS Benefits Guide — 8
Monthly Benefit Amount 66 2/3% of Annual SalaryMonthly Maximum Covered Salary
$20,000/month ($240,000 annual)
Monthly Benefit Maximum $13,333/monthMonthly Benefit Minimum $100
Elimination Period 90 Days
Disability Benefit Provisions — disabled from your own occupation for two years; from any occupation after the initial two-year period— 3/12 pre-existing condition limitation— benefit payments to age 65— 24-month limitation on mental/nervous and substance abuse claims
Additional Benefits Includes survivor benefit, waiver of premium, voluntary rehabilitation, 12-month return to work incentive, partial disability, reasonable accommodation expense benefit.
Monthly Cost Employee pays tax on the equivalent premium amount and then the district pays the premium through payroll deduction. Paid in full by WDMCS.
Please note that eligibility for Long Term Disability benefits require that each Active Regular Full Time Employee who works an average of 30 hours per week for a minimum of nine months during the 12 months, just before the date of disability.
Part time certified employees working 50 percent time are also eligible.
Employee Assistance Program (EAP)The EAP is your 24/7 direct line to free, confidential, and professional help when you need it. Eligible participants include you, family members living in your home, and legal dependents who may live elsewhere. Family members may contact the EAP on their own and receive the same confidential services including Telephone Consultation, In-Person Appointments with Counselors, Life Coaching, Legal Services, Financial Consultation, and Eldercare Resources. Better Living Web Resource is available through the EPA website at www.efr.org/myeap.
Employee WellnessThe WDMCS is committed to our employee wellness program. The program incentives are determined annually. This year, the program will start on Oct. 1, 2016, and end April 30, 2017. To log in to our beBetter site, visit the district site at www.wdmcs.org, and choose ‘beBetter’ in the ‘Staff’ tab. Further instructions are on the site.
Long Term Disability Benefits
Employee Assistance and Wellness Program Benefits

WDMCS Benefits Guide — 9
Flexible Spending Accounts are the tax-smart way to pay for qualifying expenses, such as child care and unreimbursed medical expenses. Participation reduces your taxable income, resulting in fewer taxes and more take-home pay. There are two main components to the FSA:
1) Healthcare Reimbursement PlanThe Healthcare Reimbursement Plan allows you to set aside money, on a pre-tax basis, to pay for qualified out-of-pocket medical expenses that are not covered by your insurance plan. By doing so, you reduce your taxable income. You can set a maximum of $2,550 per calendar year. Eligible expenses include more than just your deductible and copayments. Some examples include:
• Vision services, including glasses, contact lenses, frames, and contact lens solution• Dental services, including orthodontia• Chiropractic services• Over-the-counter medications will require a doctor’s order for certain OTC items
For more information about eligible expenses, please refer to IRS Publication 502, Medical and Dental Expenses available at http://www.irs.gov/publications/p502/index.html.
2) Dependent Care PlanThe Dependent Care Plan allows you to set aside money, on a pre-tax basis, to pay for qualified dependent care expenses. This reduces your taxable income. The maximum amount that you can contribute per calendar year is $5,000 (or $2,500 if married and filing separately).
Dependent Care expenses include:• Care for your children, through age 12, who qualify as dependents on your federal income tax return.• Care for a disabled dependent age 13 or older, spouse, or elderly parent who is physically incapable of self-care
and claimed as a dependent on your federal tax return.
Eligible expenses include the direct supervision of dependents as defined above. This care must be provided by an individual other than your spouse or child (unless no longer a tax-claimed dependent) and can include care in your home, a preschool, or a dependent care center.
Plan Year and Grace PeriodThere is no cost to participate in the Medical Reimbursement or Dependent Care Plans. However, you must be on district insurance coverage to participate. The plan year is one full year (365 days) and generally begins on the first of a month. Many employers design their flexible spending plan to run on the same plan year as their insurance program.
This plan year runs from July 1, 2016, through June 30, 2017, with a 2.5-month grace period until Sept. 15, 2017. The grace period is a timeframe up to 75 days after the end of the official plan year, during which employees may use up any funds remaining at the end of the plan year.
You may submit claims until Oct. 31, 2017, for this plan year. All funds not used by Sept. 15, 2017, will be forfeited to the district.
The Premium Only Plan allows you to have your premium contribution for medical and/or dental insurance taken from your paycheck on a pre-tax basis. This reduces your taxable income.
Your share of the premiums for medical and/or dental insurance (child, spouse, or family coverage) will be automatically paid with pre-tax dollars. If you do not want your premiums to be paid with pre-tax dollars, you will need to fill out a form in the Payroll Department.
Flexible Spending Account (FSA)
FSA—Premium-Only Plan

WDMCS Benefits Guide — 10
Participation in IPERS (Iowa Public Employees Retirement System) is mandatory for all full and part-time employees who are no longer high school aged.
Contribution Rates (percent of Your Pre-Tax Pay)
Your Share WDMCS’ Share Total Contribution July 1, 2016 5.95% 8.93% 14.88%
In addition to the above mentioned retirement plan all regular WDMCS employees participate in, you have the opportunity to shelter additional retirement funds through the State’s 403(b) TSA plan.
To start your contributions, complete and return a salary reduction agreement to Linda Rippentrop in the Business Services Department at the Learning Resource Center (515-633-5084). In addition to completing and returning a salary reduction agreement, you must also establish an account with one of the RIC’s investment providers. Contact information is on RIC’s website at ric.iowa.gov/403b/providers/active.html. A provider can send you enrollment information and, at your request, will schedule an appointment with a financial adviser.
Horace Mann, VOYA, MassMutual, or VALIC are the companies with whom we are licensed to do business.
The district contributes $100/month to a 403(b) Tax Sheltered Annuity to all certified staff who are contracted to work 70 percent or more time. Certified staff contracted between 50 percent and 69 percent will receive a monthly 403(b) Tax Sheltered Annuity contribution prorated.
The district contributes $70/month to a 403(b) Tax Sheltered Annuity for supervisors/specialists.
The maximum contribution is $18,000, or $21,000 for 15-year catch up, or $24,000 if age 50 or older by the end of the year. If qualified for both the 15-year catch up and age 50 contributions, the maximum contribution is $27,000.
The WDMCS Board of Education approves the Early Retirement Plan each year. Plans are in place for 2016-17. Employees planning to retire must notify the district by the end of November.
A session about IPERS, Social Security, and retiree health options is held for employees thinking about retirement each fall.
Employer-Sponsored Retirement Plans
Retirement Investors’ Club (RIC) 403(b)
Early Retirement Plan and Retirement Planning

WDMCS Benefits Guide — 11

Contact Information
Kris CraigWDMCS Benefits Adviser 515-633-5076 [email protected] Linda RippentropWDMCS Payroll Coordinator 515-633-5084 [email protected]
Wellmark BC/BSMedical 1-800-800-5122 www.wellmark.com
Delta DentalDental 1-800-544-0718 www.deltadentalia.com
DeltaVision/EyeMedVision 1-888-899-3747 www.deltadentalia.com/deltavision or www.eyemedvisioncare.com
West Des Moines Community SchoolsSchool/Community Relations Office
515-633-5023 or 515-633-5022 | www.wdmcs.orgwww.facebook.com/wdmcs | www.twitter.com/wdmcs
The West Des Moines Community School District does not discriminate on the basis of race, color, national origin, gender, disability, religion, creed, age (for employment), marital status (for programs), sexual orientation, gender identity and socioeconomic status (for programs) in its educational programs and
its employment practices. There is a grievance procedure for processing complaints of discrimination.
If you have questions or a grievance related to this policy, please contact the district’s Equity Coordinator Carol Seid, Associate Superintendent of Human Resources, 3550 Mills Civic Parkway, West Des Moines, IA 50265; Phone: 515-633-5037; Email: [email protected].