benign rectal, anal, and perineal problems
DESCRIPTION
Dr Ali Abuseini FRCS Ed. Benign Rectal, Anal, and Perineal Problems. Benign Rectal, Anal, and Perineal Problems. Anatomy - PowerPoint PPT PresentationTRANSCRIPT
Dr Ali Abuseini FRCS Ed
Benign Rectal, Anal, and Perineal Problems
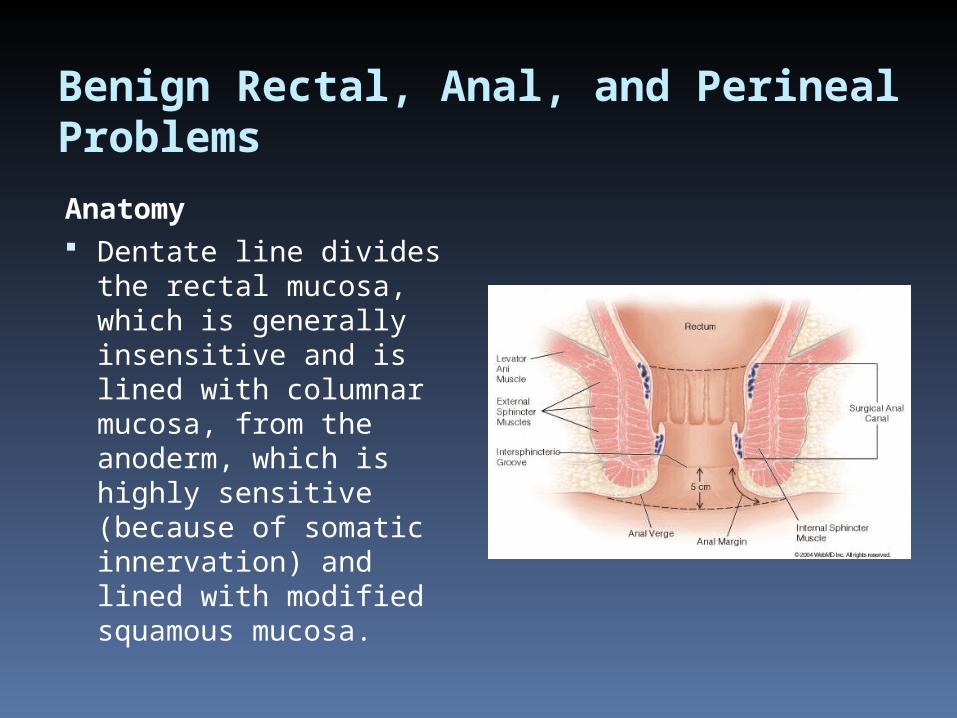
Anatomy Dentate line divides
the rectal mucosa, which is generally insensitive and is lined with columnar mucosa, from the anoderm, which is highly sensitive (because of somatic innervation) and lined with modified squamous mucosa.

Benign Rectal, Anal, and Perineal Problems
Anatomy (continue) The anal canal is surrounded by two
muscles - Internal sphincter innervated by
autonomic nervous system, maintaining resting anal tone and under involuntary control
- External sphincter innervated by somatic nerve fibers, generates the voluntary anal squeeze and plays the key role in maintaining anal continence
Benign Rectal, Anal, and Perineal Problems
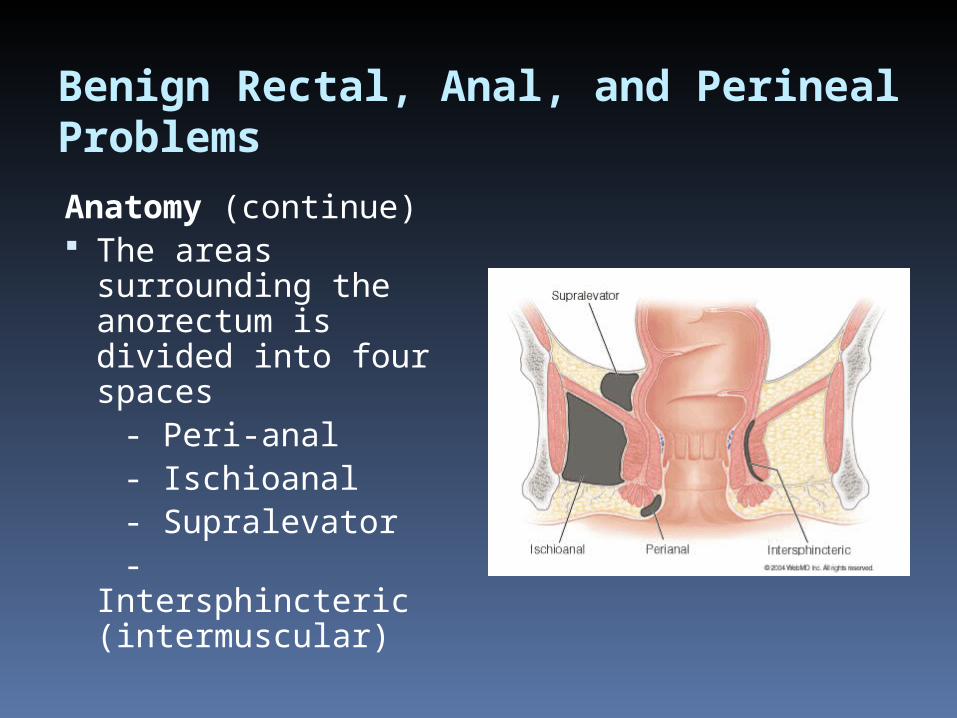
Anatomy (continue) The areas
surrounding the anorectum is divided into four spaces
- Peri-anal - Ischioanal - Supralevator - Intersphincteric
(intermuscular)

Hemorrhoids
Fibro-muscular cushions that line the anal canal
Classically found in three locations - Right anterior - Right posterior - Left lateral - Small secondary cushions may be
found lying between the main cushions
Hemorrhoids
They are part of normal anal anatomy
Play role in normal mechanism of fecal continence, they get engorged during straining or performance of Valsalva maneuver, which completes the occlusion of the anal canal and prevents stool loss with none defecatory straining
Hemorrhoids
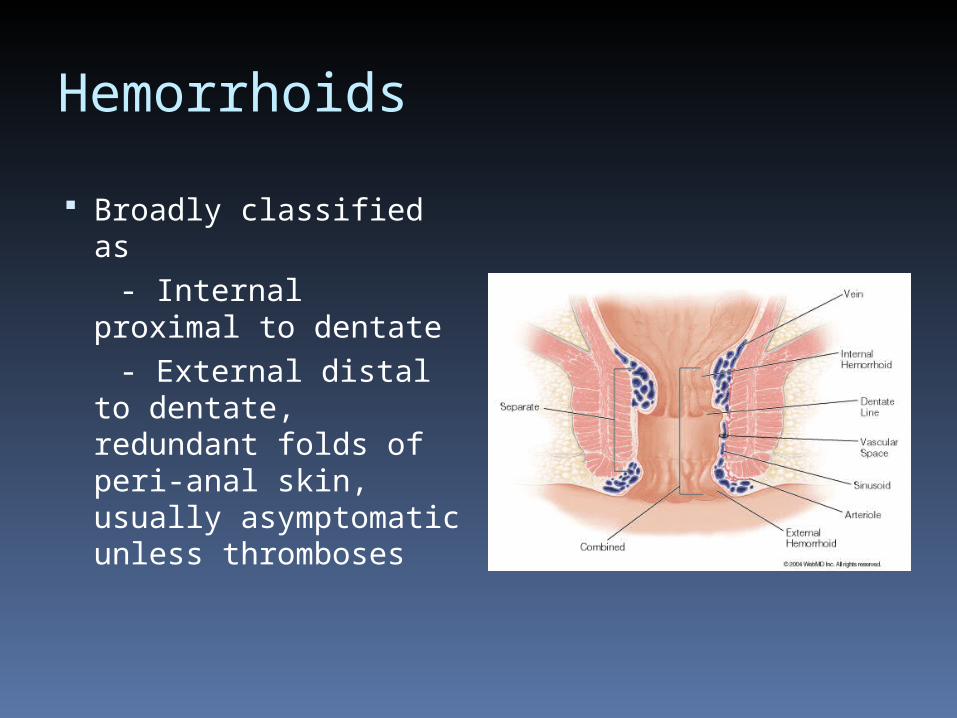
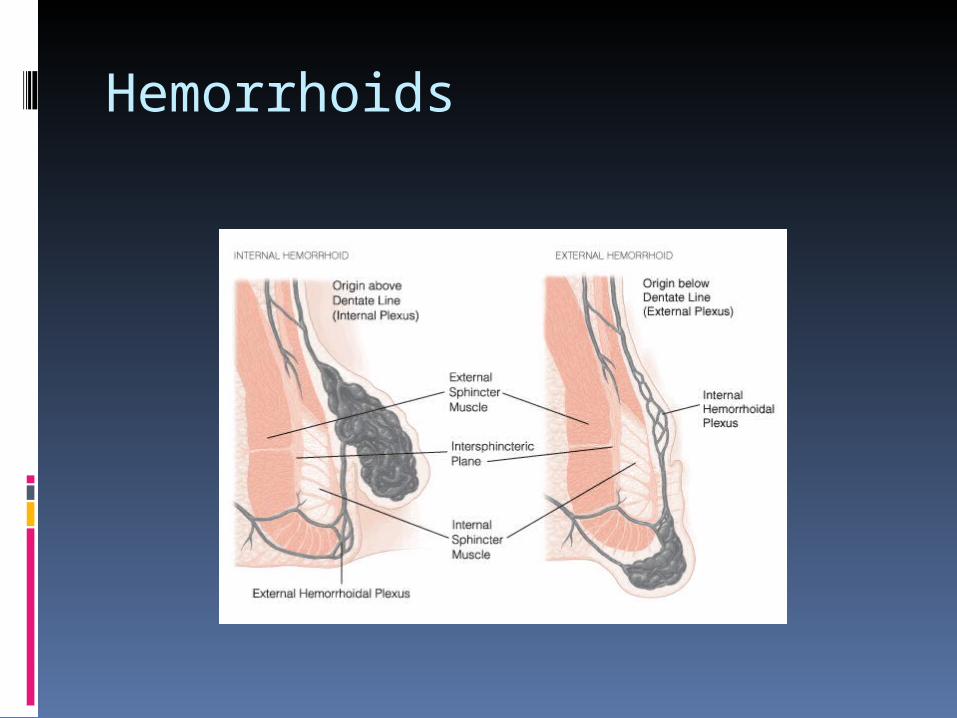
Broadly classified as - Internal proximal
to dentate - External distal to
dentate, redundant folds of peri-anal skin, usually asymptomatic unless thromboses
Hemorrhoids
Hemorrhoids
Internal Hemorrhoids Disease Manifested by two main symptoms - Painless Bleeding - Protrusion (Pain is rare as they originate above
dentate line) Most popular etiologic theory states
that Hemorrhoids result from chronic straining at defecation
Continued straining causes engorgement and bleeding, as well as hemorrhoidal prolapse
Hemorrhoids
Internal Hemorrhoids Disease (continue)
Grades - Grade 1 Bleeding without prolapse
- Grade 2 prolapse that spontaneously reduce
- Grade 3 prolapse necessitating manual reduction
- Grade 4 irreducible prolapse
Hemorrhoids
Internal Hemorrhoids Disease History - Bleeding - Protrusion - Chronic Constipation (extensive bathroom
readers) Physical examination - Visual inspection may reveal prolapsing
hemorrhoidal tissue appearing as rosette of three distinct pink-purple hemorrhoidal groups
- If no prolapse, anoscopy reveals redundant anorectal mucosa proximal to dentate line in the classic locations
Hemorrhoids
Internal Hemorrhoids DiseaseManagement Ranges from (depending on hemorrhoid
grade)
Reassurance to operative hemorrhoidal
excision
Hemorrhoids
Internal Hemorrhoids Disease / Management
Therapies classified into three categories
Diet and lifestyle modification None operative and office procedures Operative hemorroidectomies
Hemorrhoids
Internal Hemorrhoids Disease / Management
(1)Diet and life style modification All patients grade 1 or 2 and most patients with
grade 3 Correct constipation High fiber diet Liberal water intake Fiber supplement Sitz bath (soothing effect ability to relax anal
sphincter) Topical creams
Hemorrhoids
Internal Hemorrhoids Disease / Management(2)None operative and office procedures If diet and life style modification are not effective
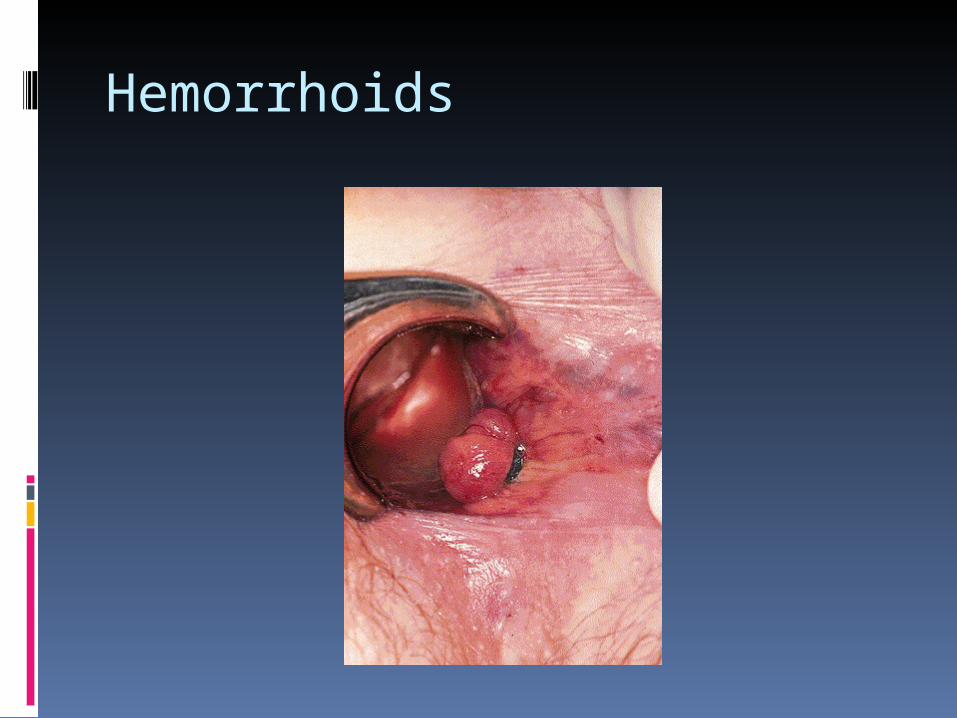
Rubber band ligation Ligation of hemorrhoid with elastic bands Successful in 2/3 to 3/4 in patients with grade 1 or 2 - Complications - Bleeding - Pain - Thromboses - Perianal sepsis (pain, fever, difficult urination)
Hemorrhoids
Hemorrhoids
Internal Hemorrhoids Disease / Management
(2)None operative and office procedures
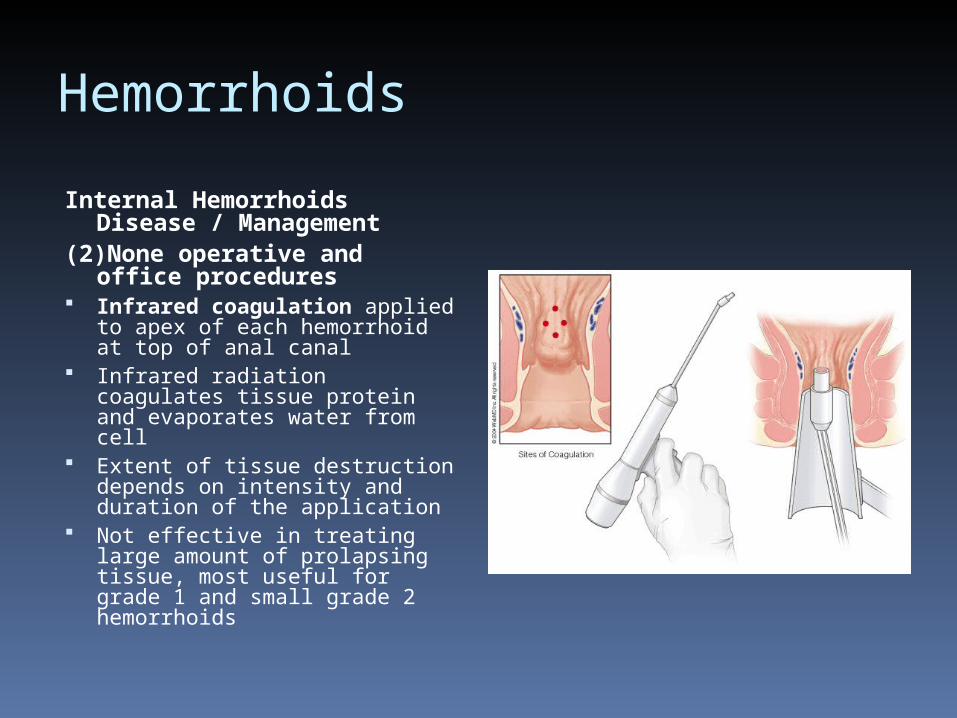
Infrared coagulation applied to apex of each hemorrhoid at top of anal canal
Infrared radiation coagulates tissue protein and evaporates water from cell
Extent of tissue destruction depends on intensity and duration of the application
Not effective in treating large amount of prolapsing tissue, most useful for grade 1 and small grade 2 hemorrhoids
hemorrhoids
Internal Hemorrhoids Disease / Management
(2)None operative and office procedures Sclerotherapy Less popular nowadays Injection of sclerosant into anorectal
submucosa to decrease vascularity and increase fibrosis (injection at apex of hemorrhoids at anorectal ring)
Agents used (phenol in oil, sodium morrhuate, and quinine urea)
Hemorrhoids
Internal Hemorrhoids Disease / Management
(3) Operative Hemorrhoidectomies Reduction of blood flow to anorectal ring Removal of redundant hemorrhoidal tissue Fixation of redundant mucosa
Procedures Hemorrhoidectomy Stapled Hemorrhoidectomy
Hemorrhoids
External Hemorrhoids Asymptomatic except when secondary thrombosed Thrombosis may result from defecatory straining or
extreme physical activity or may be random event Patient presents with constant anal pain of acute onset Physical examination identifies external thrombosis as
purple mass at anal verge Management - Depends on patients symptoms - In the first 24 – 72 hours after onset, pain increase
and excision is warranted - After 72 hours, pain generally diminishes
Hemorrhoids
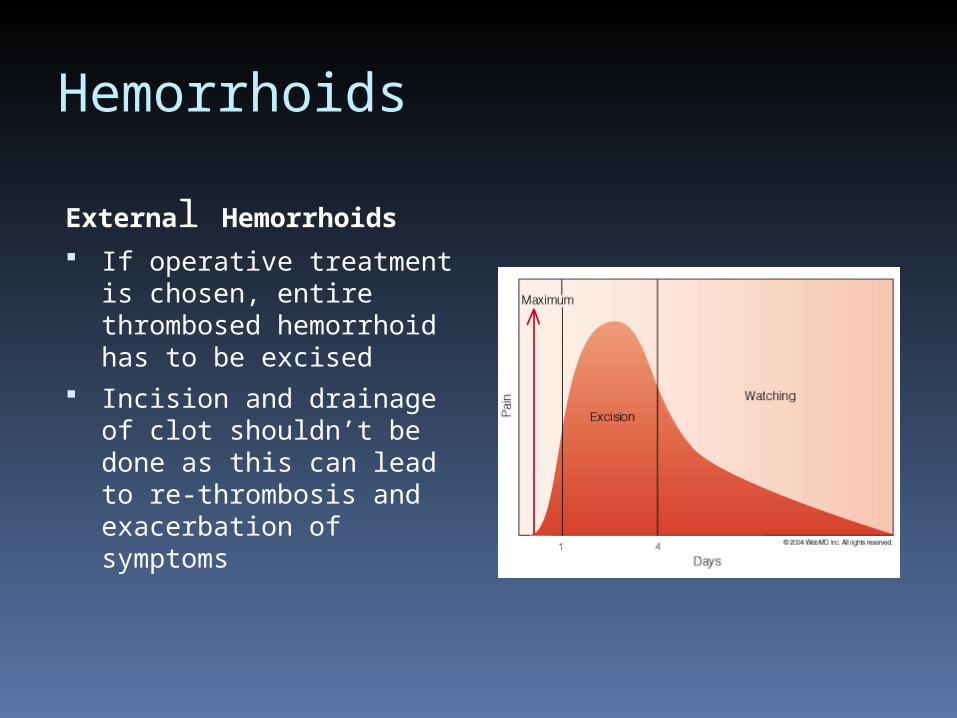
External Hemorrhoids
If operative treatment is chosen, entire thrombosed hemorrhoid has to be excised
Incision and drainage of clot shouldn’t be done as this can lead to re-thrombosis and exacerbation of symptoms
Anal Fissure
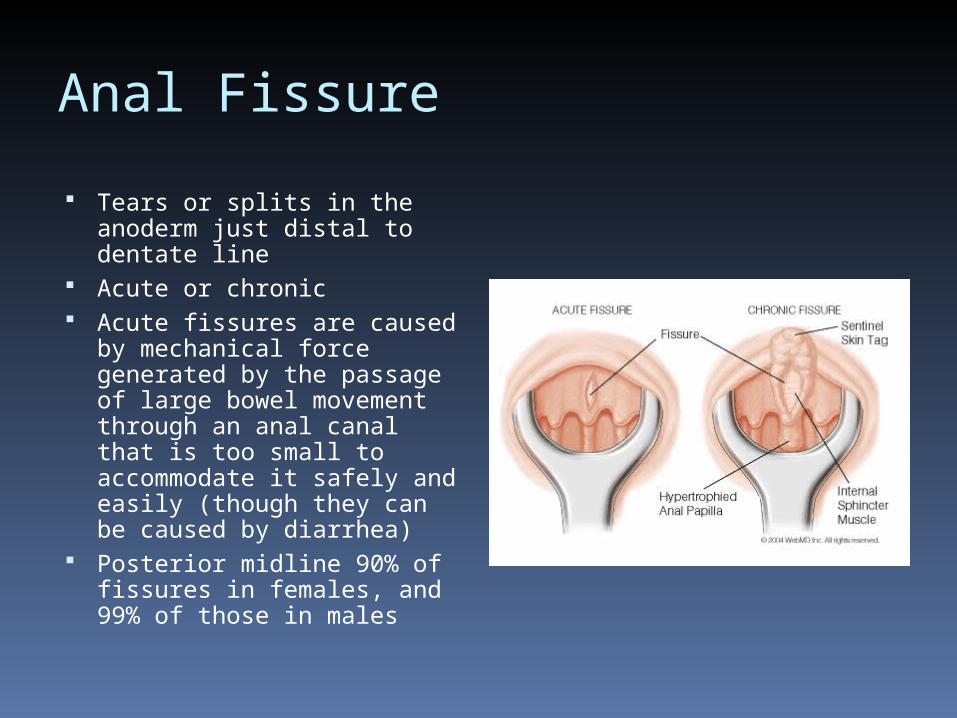
Tears or splits in the anoderm just distal to dentate line
Acute or chronic Acute fissures are caused
by mechanical force generated by the passage of large bowel movement through an anal canal that is too small to accommodate it safely and easily (though they can be caused by diarrhea)
Posterior midline 90% of fissures in females, and 99% of those in males
Anal Fissure
Decreased blood flow or increased mechanical stress may account for the propensity of these fissures to occur at this location
Repeated injury (hard or watery bowel movement ) may result in development of chronic fissure
Anal Fissure
Clinical Evaluation
Symptoms Pain (knife like or tearing sensation) Bright red rectal bleeding after bowel
movement, minor and seen on toilet paper Associated with anal spasm that persist for
several hours after each bowel movement
Anal Fissure
Clinical EvaluationPhysical Examination Difficult , extremely tender anus Split in anoderm, about 1 cm long, in posterior
midline just distal to dentate line In chronic fissure Classic triad - Hypertrophy of anal papilla - Anal fissure - Sentinel skin tag (with exposed internal anal sphincter muscle
at base of fissure)
Anal Fissure
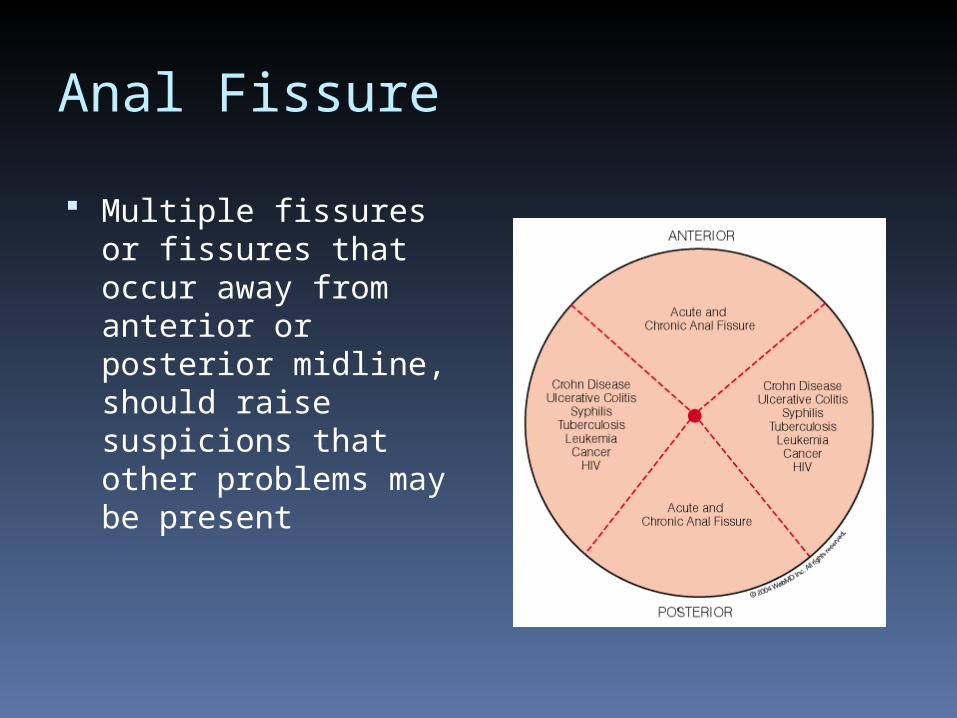
Multiple fissures or fissures that occur away from anterior or posterior midline, should raise suspicions that other problems may be present
Anal Fissure
ManagementAcute anal fissure History less than 4 – 6 weeks None operative - Fiber supplement - Stool softeners - Generous water intake - Sitz bath - Local anesthetic ointment Rapidly alleviate symptoms and bring about
complete healing
Anal Fissure
ManagementChronic anal fissure Longer than 4 – 6 weeks Respond less to none-operative measures Surgical procedure of choice lateral internal
anal sphintrotomy Cure in 95 -98% Complications - Incontinence to flatus 0 – 18% - Soiling 0 – 7% - Fecal incontinence 0 – 0.17%
Anal Fissure
Management
Therapeutic alternatives Topical Nitroglycerin (cause neurogenic
relaxation of internal sphincter( Nifedipine gel or ointment (reduce local
demand for O2 and mechanical contraction of the muscle
Topical Diltiazem Botulinum Toxins (from clostridium botulinum)
eliminate spasm and contraction of sphincter
Anorectal Abscess
Pathophysiology Most anorectal abscesses are of cryptogenic They begin as infections in the anal glands
that surrounds the anal canal and empty in the anal crypts at the dentate line
The ducts leading to and from glands become obstructed by feces or traumatized tissue, the secondary infection develops and follow the path of least resistance
Anorectal Abscess
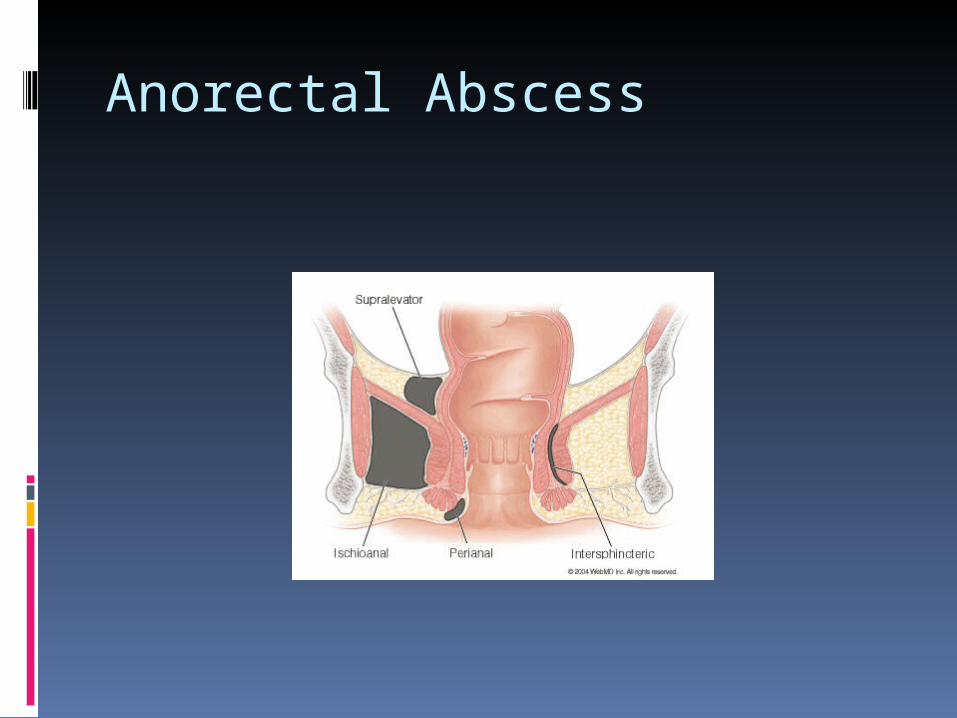
Clinical Evaluation Categorized according to space in which they
occur Peri-anal, Ischioanal, Supralevator, Intersphincteric (intermuscular)
Perianal abscesses are the most common, together with ischioanal abscesses account for 90% of perianal infections
Presentation (Pain, fever, chills, malaise, s/t systemic toxicity)
Anorectal Abscess
Anorectal Abscess
Clinical EvaluationExamination Fluctuant, erythematous, tender area in the
perineum or perianal area In case of supralevater or intersphenteric
abscesses, there may be no external manifestations, however, digital rectal examination may reveal tender mass above anal canal
Management Adequate Drainage
Fistula in Ano
Communication between anal canal and anal skin Usually begins in a crypt at the dentate line and
follows a course either between the internal and external sphincters (the most common location) resulting in ischioanal abscess, or above sphincter leading to supralevator abscess
After abscess drainage (one of three possibilities) - Fistula heals spontaneously OR - Abscess heals to recur in the future OR - Abscess heals but chronic draining fistula
remains
Fistula in Ano
Clinical Evaluation After drainage of Abscess, fistula is usually
associated with chronic serosanguinous to seropurulent discharge
As long as fistula remains open and draining, patient report little pain
If fistula close externally, abscess may develop Physical Examination reveals 2 – 3 mm opening
in the perianal skin, with surrounding induration Fistula tract can be palpated as firm cord
between external opening and anal canal
Fistula in Ano
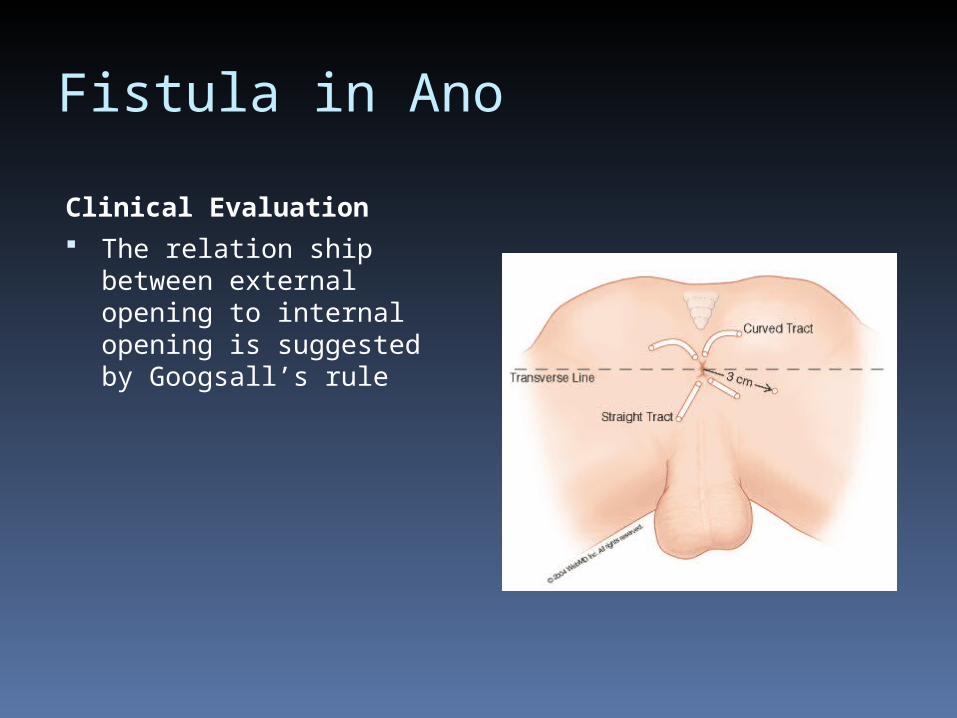
Clinical Evaluation The relation ship between
external opening to internal opening is suggested by Googsall’s rule
Fistula In Ano
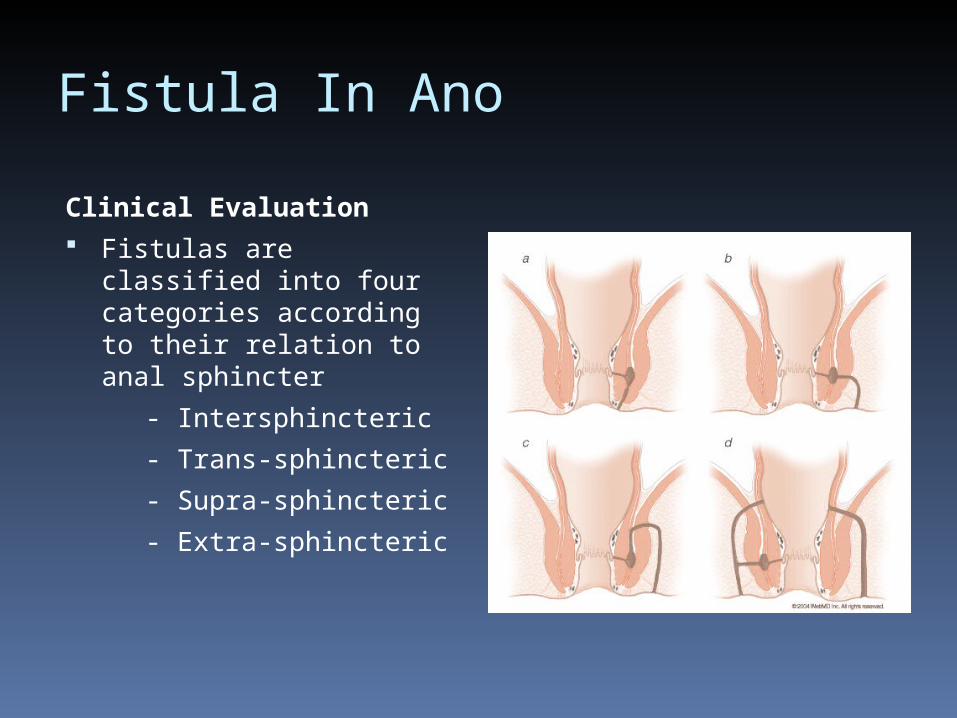
Clinical Evaluation Fistulas are classified into
four categories according to their relation to anal sphincter
- Intersphincteric
- Trans-sphincteric
- Supra-sphincteric
- Extra-sphincteric
Fistula In Ano
Management Chronic fistulas call for surgical treatment Unroofing entire fistula tract (fistulotomy) and
leaving wound open to heal secondarily Fistula that course through significant amount
of sphincter muscle, can’t be opened entirely because incontinence will result. In this condition the fistula is partially open with the musculature left intact and encircled with seton (tight (cutting seton) or un-tight)
OR close internal opening with advancement flap
Pilonidal Sinus Disease
Derived from Latin words pilus (hair) and nidus (nest) It denotes a chronic subcutaneous infection and foreign
body reaction to hairs imbedded in the skin or to abnormalities of follicles in the natal cleft
Most common in men between the onset of puberty and 40 years of age, and in obese persons
Clinical evaluation
- most patient experience an episode of acute abscess formation
- After abscess resolves, sinus tract develops
- Later in most cases sinus tract resolve, however, in the minority chronic disease or recurrent disease develops
Pilonidal Sinus Disease
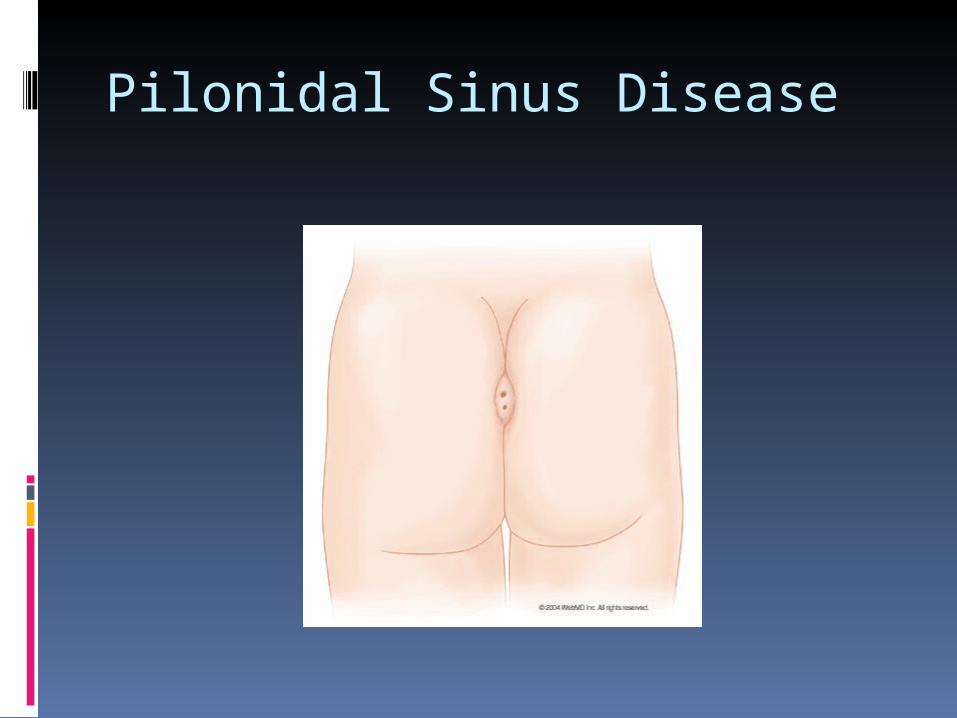
Physical examination One or more small dermal pits at the base of
intergluteal cleft Tracking from the pits (usually proceeding in a
cranial and lateral direction) appears as areas of induration
If there is abscess, the area will be erythematous, tender and draining pus may be evident
Pilonidal Sinus Disease
Pilonidal Sinus Disease Management Abscess must be drained (incision & drainage) 40% of acute pilonidal abscesses treated with incision and
drainage develop into chronic sinuses Operations for sinus tract - Closed techniques (coring out follicles and brushing the tracts),
very high recurrence rate - Laying open (un-roofing) the tract with healing by granulation,
healing time 48 days, recurrence rate 13% - Wide and deep excision of the sinus alone, healing time 72
days, recurrence rate 13% - Excision and primary closure, healing time two weeks,
recurrence rate 15%
Pilonidal Sinus Disease
Management None operative conservative approach
- Meticulous hair control (natal cleft shaving)
- improved perineal hygiene
- Limited lateral incision and drainage for treatment of abscess
Hydradenitis Suppurativa
Chronic recurrent inflammatory process involving the apocrine glands of the axilla, the groin, and peri-anal region
Occlusion of follicles and abnormalities of apocrine ducts are believed to be the causative factors
Disease can result in chronically draining wounds and sinus tracts and can become quite painful and debilitating
Hydradenitis Suppurativa
Management Medical may afford temporary relief of
symptoms Most patients eventually require surgical
therapy Incision and drainage or un-roofing of sinus
reserved for early and acute disease Local excision provides adequate control of
symptoms, recurrence rate higher than 50% Wedge excision with secondary granulation
Pruritus Ani
Dermatologic condition of the perianal skin characterized by uneasiness or itching in the area around anus
Predisposing factors - Poor peri-anal hygiene (related to incontinence,
diarrhea, or excessive hair) - Over hygiene - Excessive moisture - Irregularities of peri-anal skin (from hemorrhoids,
fistulas, or previous surgery) - Skin hypersensitivity - Diet - Decreased resistance to infection - Injury to peri-anal skin
Pruritus Ani
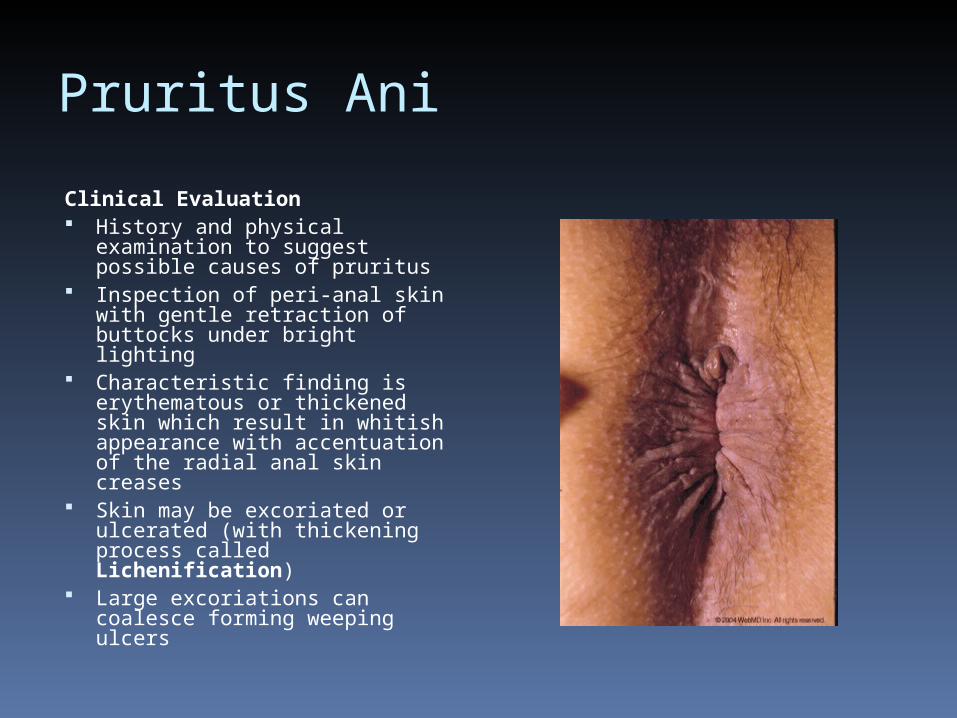
Clinical Evaluation History and physical
examination to suggest possible causes of pruritus
Inspection of peri-anal skin with gentle retraction of buttocks under bright lighting
Characteristic finding is erythematous or thickened skin which result in whitish appearance with accentuation of the radial anal skin creases
Skin may be excoriated or ulcerated (with thickening process called Lichenification)
Large excoriations can coalesce forming weeping ulcers
Pruritus Ani
Clinical Evaluation Digital rectal examination to assess competence of anal
sphincter at rest and at maximal squeeze Anoscopy and proctoscopy should be performed
Management Cause has to be eliminated Keep peri-anal area dry Avoid trauma to area Peri-anal area should be gently washed, never scrubbed Avoid irritating foods (tomatoes, pepper, citrus fruits and
juices, coffee, colas, beer, milk , nuts and any food stuff found to be associated with increased gas, indigestion and diarrhea
Maintain regular bowel habbits
Pruritus Ani
Management (continue) Avoid creams, lotions and emollients Hydrocortisone cream may be applied for one
week If candidal yeast infection is found, try
antifungal lotion, solution or powder If standard measures fail to elicit
improvement, fungal and viral cultures and even biopsy may be necessary to exclude an infectious or neoplastic cause
Solitary Rectal Ulcer Syndrome Clinical condition characterized by rectal bleeding,
copious mucous discharge, anorectal pain and difficult evacuation
SRUS can have single rectal ulcer, multiple ulcers or even no ulcers
When present, ulcers usually occur on the anterior rectal wall just above the anorectal ring
Ulcers usually appear as shallow lesions with punched out gray-white base that is surrounded by hyperemia
Cause unclear, associated with chronic inflammation or trauma (internal intussception or prolapse of the rectum, direct digital trauma, or forces to evacuate hard stool)
Solitary Rectal Ulcer SyndromeManagement Treatment is directed at alleviating symptoms or
interfering with some of the proposed etiologic mechanisms
Conservative therapy (e.g. high fiber diet, lifestyle changes etc) should be tried first
Pharmacologic therapy (e.g. anti-inflammatory enemas and suppositories), limited success but worth trying
If symptoms persists, localized resection may be considered
Patients with prolapse, prolapse need to be treated either with perineal procedures or abdominal procedures
Questions
Which is true regarding anal sphincter function
a. when the rectum is distended, the external sphincter relax and the
internal sphincter contract. B. when the rectum is distended. The internal sphincter contract and
the external sphincter relax.
C. The External sphincter is responsible for resting anal pressure
D. The internal sphincter is responsible for resting anal pressure.
E. The external sphincter has an autonomic nerve sensation
The most common complication after hemorroidectomy is which of the following?
A. Urine retention B. Rectal bleeding C. Incontinence D. wound infection E. Anal stricture.
The fistula in ano traversing the external anal sphincter and intersphincteric plane is categorized as:
A. Intersphincteric B. Transsphincteric C. Suprasphincteric D. Extrasphincteric E. Subsphincteric
Which is not true regarding perianal abscess.
A. cryptoglandulr theory explain its pathology B. clinically presented as severe perianal pain C. once diagnosed ,the initial treatment is IV
antibiotics D. if it is not treated can be complicated by
fistula in ano E. can be treated by catheter drainage.
Pilonidal Sinus Disease which false A. the commonest site is natal cleft B. conservative treatment is effective in
some cases. C. can be complicated by abscess
formation D. If an abscess is found it should be
drain E. Recurrence rate is very low after
surgery